
Much Ado about Sleep: Current Concepts on Mechanisms and Predisposition to Pediatric Obstructive Sleep Apnea


Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
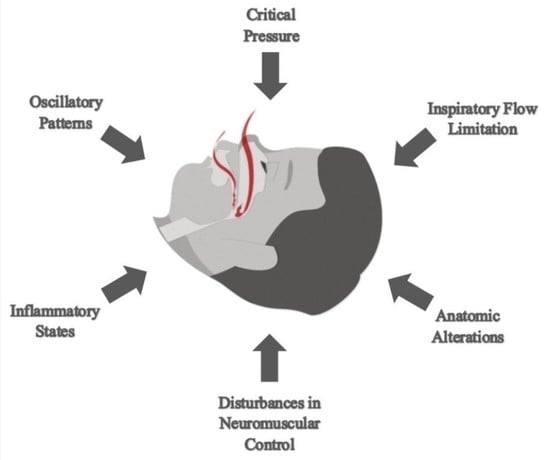
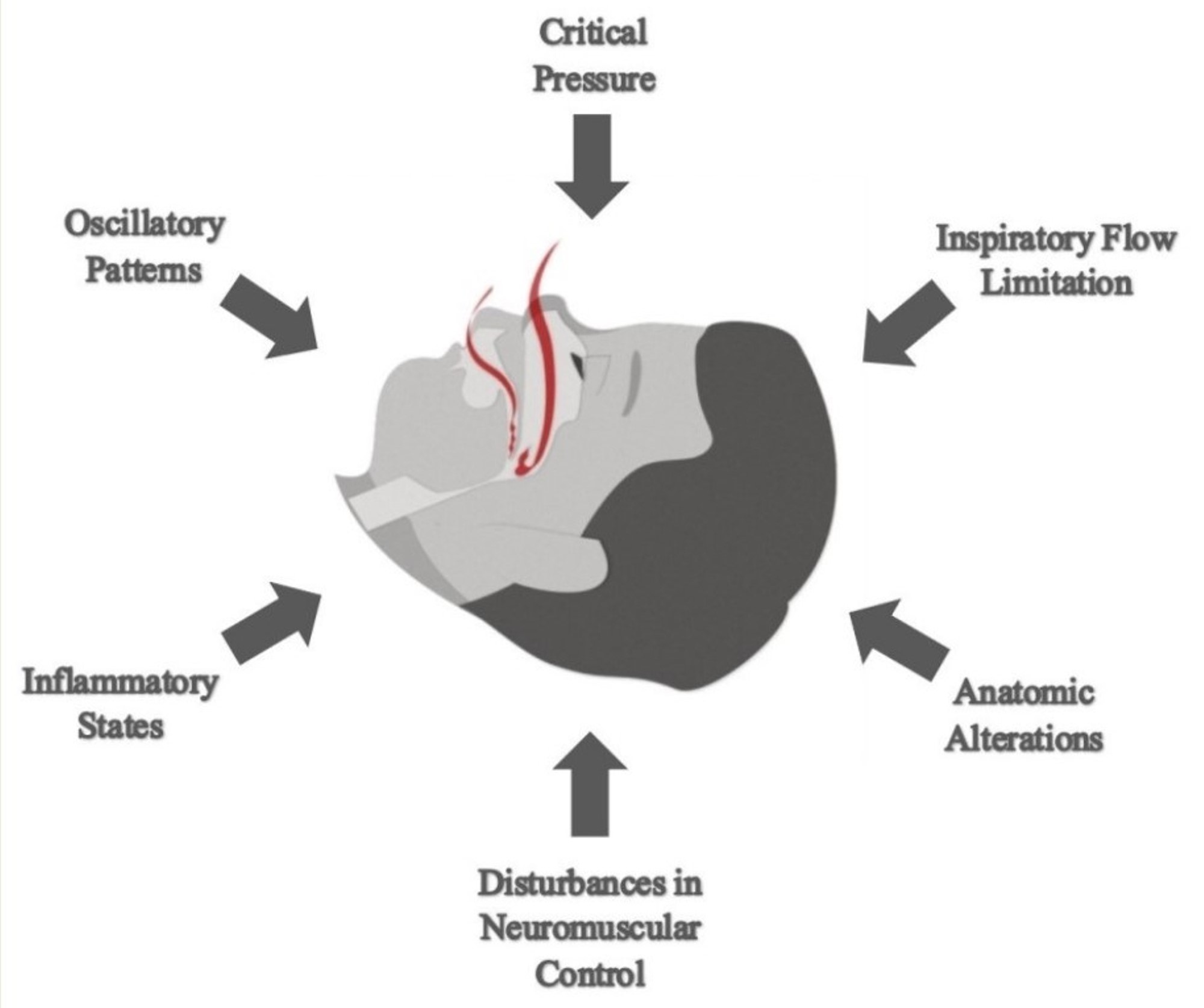
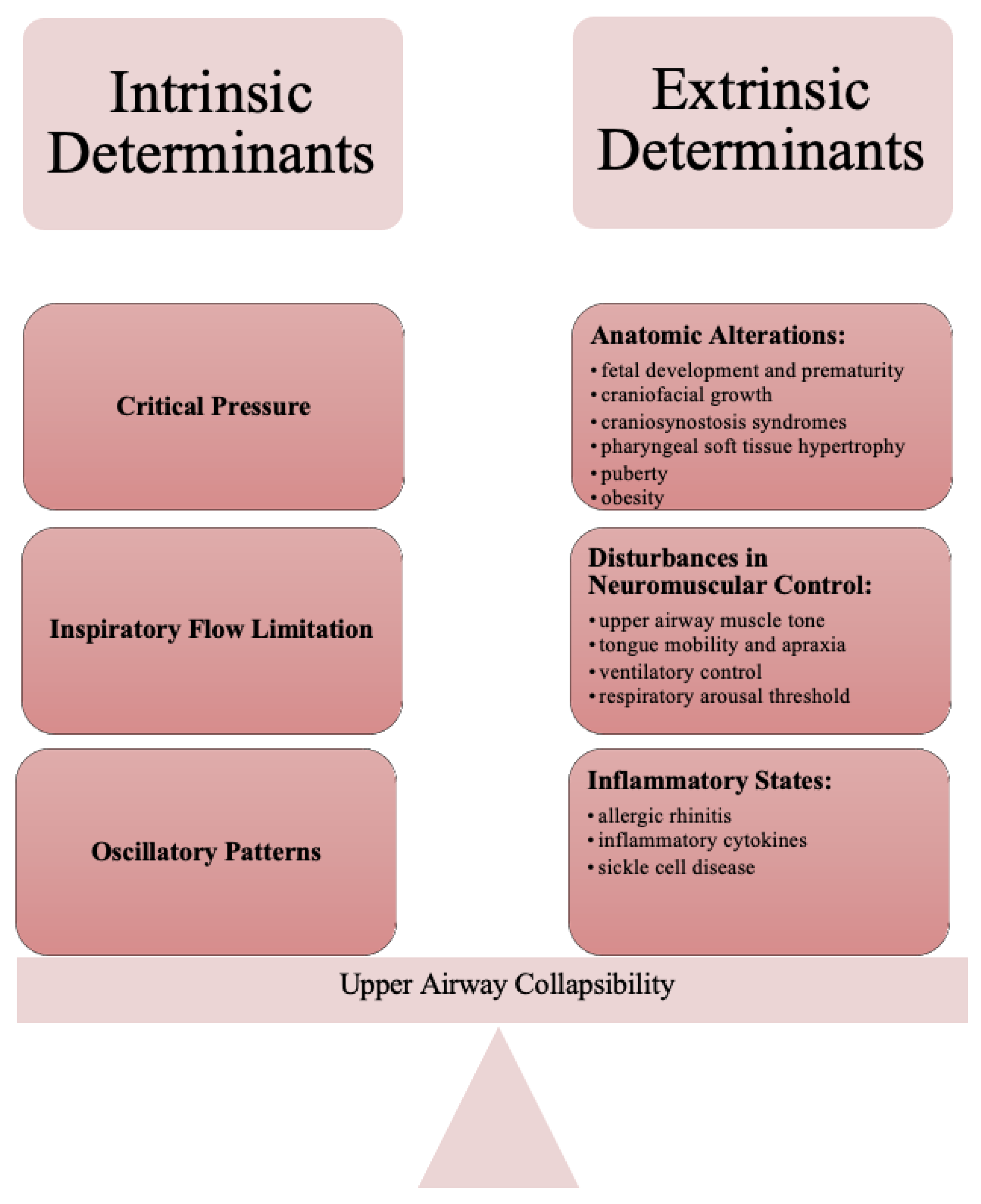
2. Intrinsic Determinants of Upper Airway Collapsibility
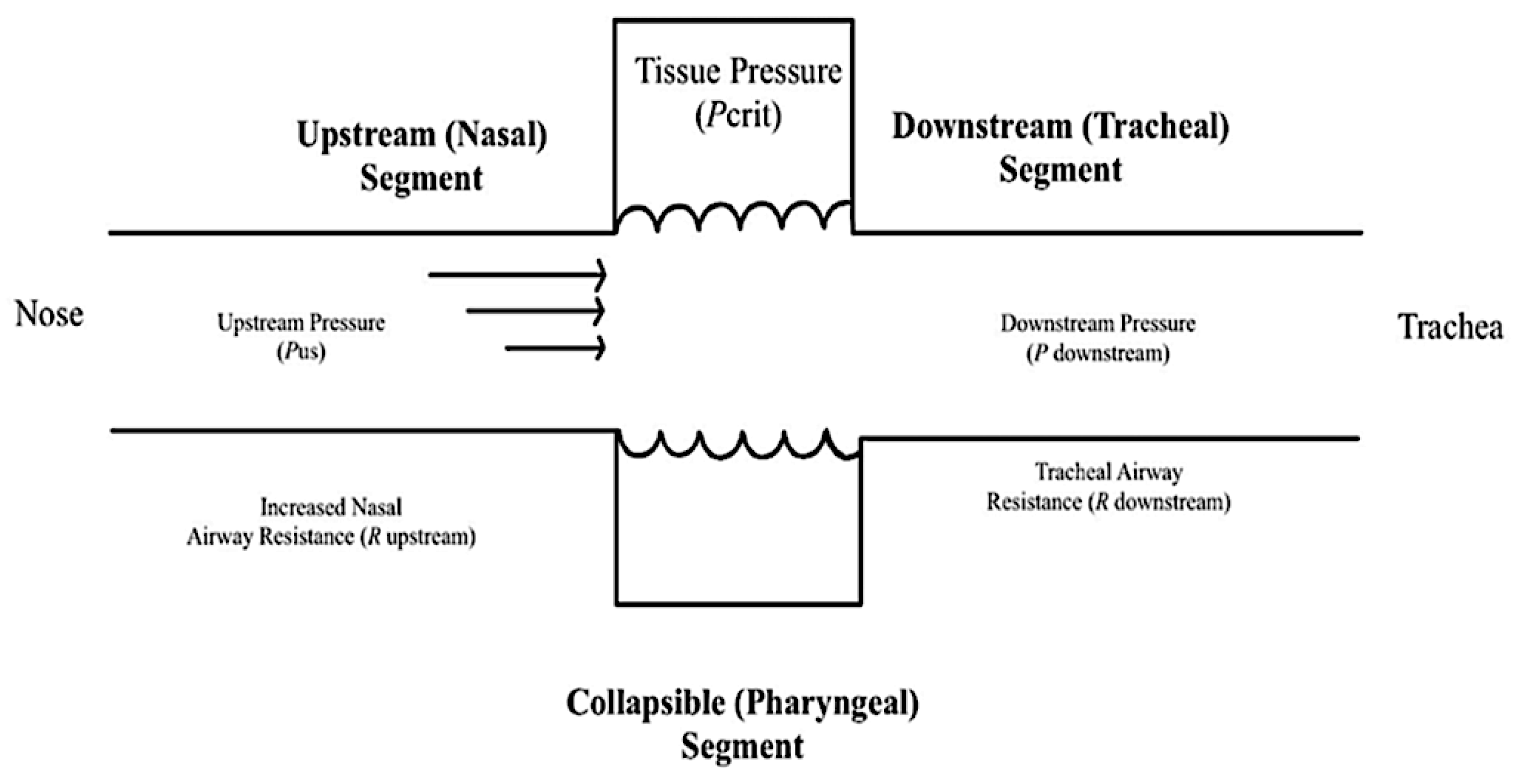
2.1. Critical Pressure
2.2. Oscillatory Patterns
3. Extrinsic Determinants of Upper Airway Collapsibility
3.1. Anatomic Alterations
3.1.1. Craniofacial Growth during Fetal Life
3.1.2. Craniofacial Dysmorphism
3.1.3. Craniosynostosis Syndromes
3.1.4. Pharyngeal Soft Tissue
3.1.5. Puberty-Related Changes
3.1.6. Obesity
3.2. Disturbances in Neuromuscular Control and Inflammatory States
3.2.1. Ineffective Upper-Airway Dilator Muscles
3.2.2. Reduced Tongue Mobility
3.2.3. Unstable Ventilatory Control and Low Respiratory Arousal Threshold
3.2.4. Local Inflammation and Allergic Rhinitis
3.2.5. Diffuse Inflammation
3.2.6. Sickle Cell Disease
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garg, R.K.; Afifi, A.M.; Garland, C.B.; Sanchez, R.; Mount, D.L. Pediatric Obstructive Sleep Apnea: Consensus, Controversy, and Craniofacial Considerations. Plast. Reconstr. Surg. 2017, 140, 987–997. [Google Scholar] [CrossRef]
- Pham, L.V.; Schwartz, A.R. The pathogenesis of obstructive sleep apnea. J. Thorac. Dis. 2015, 7, 1358–1372. [Google Scholar] [CrossRef]
- Savini, S.; Ciorba, A.; Bianchini, C.; Stomeo, F.; Corazzi, V.; Vicini, C.; Pelucchi, S. Assessment of obstructive sleep apnoea (OSA) in children: An update. Acta Otorhinolaryngol. Ital. 2019, 39, 289–297. [Google Scholar] [CrossRef]
- Bitners, A.C.; Arens, R. Evaluation and Management of Children with Obstructive Sleep Apnea Syndrome. Lung 2020, 198, 257–270. [Google Scholar] [CrossRef] [PubMed]
- Rundo, J.V. Obstructive sleep apnea basics. Clevel. Clin. J. Med. 2019, 86, 2–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capdevila, O.S.; Kheirandish-Gozal, L.; Dayyat, E.; Gozal, D. Pediatric obstructive sleep apnea: Complications, management, and long-term outcomes. Proc. Am. Thorac. Soc. 2008, 5, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Quinlan, C.M.; Otero, H.; Tapia, I.E. Upper airway visualization in pediatric obstructive sleep apnea. Paediatr. Respir. Rev. 2019, 32, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Gulotta, G.; Iannella, G.; Vicini, C.; Polimeni, A.; Greco, A.; de Vincentiis, M.; Visconti, I.C.; Meccariello, G.; Cammaroto, G.; De Vito, A.; et al. Risk Factors for Obstructive Sleep Apnea Syndrome in Children: State of the Art. Int. J. Environ. Res. Public Health 2019, 16, 3235. [Google Scholar] [CrossRef] [Green Version]
- Guilleminault, C.; Sullivan, S.S.; Huang, Y.S. Sleep-Disordered Breathing, Orofacial Growth, and Prevention of Obstructive Sleep Apnea. Sleep Med. Clin. 2019, 14, 13–20. [Google Scholar] [CrossRef]
- Guilleminault, C.; Huang, Y.S. From oral facial dysfunction to dysmorphism and the onset of pediatric OSA. Sleep Med. Rev. 2018, 40, 203–214. [Google Scholar] [CrossRef]
- Tan, H.L.; Gozal, D.; Kheirandish-Gozal, L. Obstructive sleep apnea in children: A critical update. Nat. Sci. Sleep 2013, 5, 109–123. [Google Scholar] [CrossRef] [Green Version]
- Katz, E.S.; D’Ambrosio, C.M. Pathophysiology of pediatric obstructive sleep apnea. Proc. Am. Thorac. Soc. 2008, 5, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Subramani, Y.; Singh, M.; Wong, J.; Kushida, C.A.; Malhotra, A.; Chung, F. Understanding Phenotypes of Obstructive Sleep Apnea: Applications in Anesthesia, Surgery, and Perioperative Medicine. Anesth. Analg. 2017, 124, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Sforza, E.; Petiau, C.; Weiss, T.; Thibault, A.; Krieger, J. Pharyngeal critical pressure in patients with obstructive sleep apnea syndrome. Clinical implications. Am. J. Respir. Crit. Care Med. 1999, 159, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Gold, A.R.; Schwartz, A.R. The pharyngeal critical pressure. The whys and hows of using nasal continuous positive airway pressure diagnostically. Chest 1996, 110, 1077–1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, A.R.; Smith, P.L. CrossTalk proposal: The human upper airway does behave like a Starling resistor during sleep. J. Physiol. 2013, 591, 2229–2232. [Google Scholar] [CrossRef]
- Wellman, A.; Genta, P.R.; Owens, R.L.; Edwards, B.A.; Sands, S.A.; Loring, S.H.; White, D.P.; Jackson, A.C.; Pedersen, O.F.; Butler, J.P. Test of the Starling resistor model in the human upper airway during sleep. J. Appl. Physiol. 2014, 117, 1478–1485. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, A.R.; Smith, P.L.; Wise, R.A.; Gold, A.R.; Permutt, S. Induction of upper airway occlusion in sleeping individuals with subatmospheric nasal pressure. J. Appl. Physiol. 1988, 64, 535–542. [Google Scholar] [CrossRef]
- Brockbank, J.C. Update on pathophysiology and treatment of childhood obstructive sleep apnea syndrome. Paediatr. Respir. Rev. 2017, 24, 21–23. [Google Scholar] [CrossRef]
- Marcus, C.L.; McColley, S.A.; Carroll, J.L.; Loughlin, G.M.; Smith, P.L.; Schwartz, A.R. Upper airway collapsibility in children with obstructive sleep apnea syndrome. J. Appl. Physiol. 1994, 77, 918–924. [Google Scholar] [CrossRef]
- Gold, A.R.; Marcus, C.L.; Dipalo, F.; Gold, M.S. Upper airway collapsibility during sleep in upper airway resistance syndrome. Chest 2002, 121, 1531–1540. [Google Scholar] [CrossRef]
- Marcus, C.L.; Katz, E.S.; Lutz, J.; Black, C.A.; Galster, P.; Carson, K.A. Upper airway dynamic responses in children with the obstructive sleep apnea syndrome. Pediatr. Res. 2005, 57, 99–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carberry, J.C.; Jordan, A.S.; White, D.P.; Wellman, A.; Eckert, D.J. Upper Airway Collapsibility (Pcrit) and Pharyngeal Dilator Muscle Activity are Sleep Stage Dependent. Sleep 2016, 39, 511–521. [Google Scholar] [CrossRef] [PubMed]
- Zhi, Y.X.; Vena, D.; Popovic, M.R.; Bradley, T.D.; Yadollahi, A. Detecting inspiratory flow limitation with temporal features of nasal airflow. Sleep Med. 2018, 48, 70–78. [Google Scholar] [CrossRef]
- Guevarra, J.T.; Castillo, B.; Joshi, H.; Parekh, A.; Ayappa, I.; Rapoport, D.M. Immediate Physiological Responses to Inspiratory Flow Limited Events in Mild Obstructive Sleep Apnea. Ann. Am. Thorac. Soc. 2021, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Spina, G.; Spruit, M.A.; Alison, J.; Benzo, R.P.; Calverley, P.M.A.; Clarenbach, C.F.; Costello, R.W.; Donaire-Gonzalez, D.; Dürr, S.; Garcia-Aymerich, J.; et al. Analysis of nocturnal actigraphic sleep measures in patients with COPD and their association with daytime physical activity. Thorax 2017, 72, 694–701. [Google Scholar] [CrossRef]
- Lin, C.; Lo, M.T.; Guilleminault, C. Exploring the Abnormal Modulation of the Autonomic Systems during Nasal Flow Limitation in Upper Airway Resistance Syndrome by Hilbert-Huang Transform. Front. Med. 2017, 4, 161. [Google Scholar] [CrossRef] [Green Version]
- Khoo, M.C.K. Physiological Control Systems: Analysis, Simulation, and Estimation, 2nd ed.; IEEE Press: Piscataway, NJ, USA; Wiley: Hoboken, NJ, USA, 2018; p. xvii. 429p. [Google Scholar]
- Remmers, J.E.; deGroot, W.J.; Sauerland, E.K.; Anch, A.M. Pathogenesis of upper airway occlusion during sleep. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1978, 44, 931–938. [Google Scholar] [CrossRef]
- Javaheri, S.; Barbe, F.; Campos-Rodriguez, F.; Dempsey, J.A.; Khayat, R.; Javaheri, S.; Malhotra, A.; Martinez-Garcia, M.A.; Mehra, R.; Pack, A.I.; et al. Sleep Apnea: Types, Mechanisms, and Clinical Cardiovascular Consequences. J. Am. Coll. Cardiol. 2017, 69, 841–858. [Google Scholar] [CrossRef]
- Kirkness, J.P.; Peterson, L.A.; Squier, S.B.; McGinley, B.M.; Schneider, H.; Meyer, A.; Schwartz, A.R.; Smith, P.L.; Patil, S.P. Performance characteristics of upper airway critical collapsing pressure measurements during sleep. Sleep 2011, 34, 459–467. [Google Scholar] [CrossRef] [Green Version]
- Clark, C.; Ulualp, S.O. Multimodality assessment of upper airway obstruction in children with persistent obstructive sleep apnea after adenotonsillectomy. Laryngoscope 2017, 127, 1224–1230. [Google Scholar] [CrossRef] [PubMed]
- ElMallah, M.; Bailey, E.; Trivedi, M.; Kremer, T.; Rhein, L.M. Pediatric Obstructive Sleep Apnea in High-Risk Populations: Clinical Implications. Pediatr. Ann. 2017, 46, e336–e339. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.S.; Guilleminault, C. Pediatric Obstructive Sleep Apnea: Where Do We Stand? Adv. Otorhinolaryngol. 2017, 80, 136–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stark, T.R.; Pozo-Alonso, M.; Daniels, R.; Camacho, M. Pediatric Considerations for Dental Sleep Medicine. Sleep Med. Clin. 2018, 13, 531–548. [Google Scholar] [CrossRef] [PubMed]
- Vos, W.G.; De Backer, W.A.; Verhulst, S.L. Correlation between the severity of sleep apnea and upper airway morphology in pediatric and adult patients. Curr. Opin. Allergy Clin. Immunol. 2010, 10, 26–33. [Google Scholar] [CrossRef]
- Huynh, N.T.; Desplats, E.; Almeida, F.R. Orthodontics treatments for managing obstructive sleep apnea syndrome in children: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 84–94. [Google Scholar] [CrossRef]
- Guilleminault, C.; Lee, J.H.; Chan, A. Pediatric obstructive sleep apnea syndrome. Arch. Pediatr. Adolesc. Med. 2005, 159, 775–785. [Google Scholar] [CrossRef]
- Galeotti, A.; Festa, P.; Viarani, V.; Pavone, M.; Sitzia, E.; Piga, S.; Cutrera, R.; De Vincentiis, G.C.; D’Antò, V. Correlation between cephalometric variables and obstructive sleep apnoea severity in children. Eur. J. Paediatr. Dent. 2019, 20, 43–47. [Google Scholar] [CrossRef]
- Luzzi, V.; Ierardo, G.; Di Carlo, G.; Saccucci, M.; Polimeni, A. Obstructive sleep apnea syndrome in the pediatric age: The role of the dentist. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 9–14. [Google Scholar] [CrossRef]
- Lee, Y.H.; Huang, Y.S.; Chen, I.C.; Lin, P.Y.; Chuang, L.C. Craniofacial, dental arch morphology, and characteristics in preschool children with mild obstructive sleep apnea. J. Dent. Sci. 2020, 15, 193–199. [Google Scholar] [CrossRef]
- Yap, B.; Kontos, A.; Pamula, Y.; Martin, J.; Kennedy, D.; Sampson, W.; Dreyer, C. Differences in dentofacial morphology in children with sleep disordered breathing are detected with routine orthodontic records. Sleep Med. 2019, 55, 109–114. [Google Scholar] [CrossRef]
- Wenger, T.L.; Hing, A.V.; Evans, K.N. Apert Syndrome. In GeneReviews((R)); Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Mirzaa, G., Amemiya, A., Eds.; U.S. National Library of Medicine: Seattle, WA, USA, 1993. [Google Scholar]
- Hill, C.M.; Evans, H.J.; Elphick, H.; Farquhar, M.; Pickering, R.M.; Kingshott, R.; Martin, J.; Reynolds, J.; Joyce, A.; Rush, C.; et al. Prevalence and predictors of obstructive sleep apnoea in young children with Down syndrome. Sleep Med. 2016, 27–28, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, E.O.; Haddad, F.L.M.; Stefanini, R.; Moreira, G.A.; Rapoport, P.B.; Gregorio, L.C.; Tufik, S.; Bittencourt, L.R.A. Clinicals And Upper Airway Characteristics in Obese Children with Obstructive Sleep Apnea. Sleep Sci. 2017, 10, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Xu, Z.; Wu, Y.; Tai, J.; Feng, G.; Ge, W.; Zheng, L.; Zhou, Z.; Ni, X. Risk factors of obstructive sleep apnea syndrome in children. J. Otolaryngol. Head Neck Surg. 2020, 49, 11. [Google Scholar] [CrossRef] [PubMed]
- Feng, G.; Gong, X.; Yu, M.; Huang, X.; Gao, X. Differences of Craniofacial Characteristics in Oral Breathing and Pediatric Obstructive Sleep Apnea. J. Craniofac. Surg. 2021, 32, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Friedman, M.; Salapatas, A.M.; Bonzelaar, L.B. Updated Friedman Staging System for Obstructive Sleep Apnea. Adv. Otorhinolaryngol. 2017, 80, 41–48. [Google Scholar] [CrossRef]
- Patini, R.; Arrica, M.; Di Stasio, E.; Gallenzi, P.; Cordaro, M. The use of magnetic resonance imaging in the evaluation of upper airway structures in paediatric obstructive sleep apnoea syndrome: A systematic review and meta-analysis. Dentomaxillofac. Radiol. 2016, 45, 20160136. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.Y.; Guilleminault, C.; Chiu, H.Y.; Sullivan, S.S. Mouth breathing, “nasal disuse”, and pediatric sleep-disordered breathing. Sleep Breath. 2015, 19, 1257–1264. [Google Scholar] [CrossRef]
- Arens, R.; Sin, S.; Nandalike, K.; Rieder, J.; Khan, U.I.; Freeman, K.; Wylie-Rosett, J.; Lipton, M.L.; Wootton, D.M.; McDonough, J.M.; et al. Upper airway structure and body fat composition in obese children with obstructive sleep apnea syndrome. Am. J. Respir. Crit. Care Med. 2011, 183, 782–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isono, S.; Shimada, A.; Utsugi, M.; Konno, A.; Nishino, T. Comparison of static mechanical properties of the passive pharynx between normal children and children with sleep-disordered breathing. Am. J. Respir. Crit. Care Med. 1998, 157, 1204–1212. [Google Scholar] [CrossRef]
- Kaditis, A.G.; Alonso Alvarez, M.L.; Boudewyns, A.; Alexopoulos, E.I.; Ersu, R.; Joosten, K.; Larramona, H.; Miano, S.; Narang, I.; Trang, H.; et al. Obstructive sleep disordered breathing in 2- to 18-year-old children: Diagnosis and management. Eur. Respir. J. 2016, 47, 69–94. [Google Scholar] [CrossRef] [PubMed]
- Carter, K.A.; Hathaway, N.E.; Lettieri, C.F. Common sleep disorders in children. Am. Fam. Physician 2014, 89, 368–377. [Google Scholar] [PubMed]
- Marcus, C.L.; Brooks, L.J.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Schechter, M.S.; Ward, S.D.; Sheldon, S.H.; Shiffman, R.N.; et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012, 130, e714–e755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vicini, C.; De Vito, A.; Iannella, G.; Gobbi, R.; Corso, R.M.; Montevecchi, F.; Polimeni, A.; De Vincentiis, M.; Meccariello, G.; D’Agostino, G.; et al. The aging effect on upper airways collapse of patients with obstructive sleep apnea syndrome. Eur. Arch. Otorhinolaryngol. 2018, 275, 2983–2990. [Google Scholar] [CrossRef] [PubMed]
- Ronen, O.; Malhotra, A.; Pillar, G. Influence of gender and age on upper-airway length during development. Pediatrics 2007, 120, e1028–e1034. [Google Scholar] [CrossRef] [Green Version]
- Xu, Z.; Jiaqing, A.; Yuchuan, L.; Shen, K. A case-control study of obstructive sleep apnea-hypopnea syndrome in obese and nonobese chinese children. Chest 2008, 133, 684–689. [Google Scholar] [CrossRef]
- Guilleminault, C.; Partinen, M.; Praud, J.P.; Quera-Salva, M.A.; Powell, N.; Riley, R. Morphometric facial changes and obstructive sleep apnea in adolescents. J. Pediatr. 1989, 114, 997–999. [Google Scholar] [CrossRef]
- Oliven, R.; Cohen, G.; Somri, M.; Schwartz, A.R.; Oliven, A. Relationship between the activity of the genioglossus, other peri-pharyngeal muscles and flow mechanics during wakefulness and sleep in patients with OSA and healthy subjects. Respir. Physiol. Neurobiol. 2020, 274, 103362. [Google Scholar] [CrossRef]
- Osman, A.M.; Carter, S.G.; Carberry, J.C.; Eckert, D.J. Obstructive sleep apnea: Current perspectives. Nat. Sci. Sleep 2018, 10, 21–34. [Google Scholar] [CrossRef] [Green Version]
- Eckert, D.J. Phenotypic approaches to obstructive sleep apnoea—New pathways for targeted therapy. Sleep Med. Rev. 2018, 37, 45–59. [Google Scholar] [CrossRef]
- Patel, J.A.; Ray, B.J.; Fernandez-Salvador, C.; Gouveia, C.; Zaghi, S.; Camacho, M. Neuromuscular function of the soft palate and uvula in snoring and obstructive sleep apnea: A systematic review. Am. J. Otolaryngol. 2018, 39, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Bassiouny, A.; Nasr, S.; Mashaly, M.; Ayad, E.; Qotb, M.; Atef, A. Electron microscopy study of peripheral nerves in the uvulae of snorers and obstructive sleep apnoea patients. J. Laryngol. Otol. 2009, 123, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Yuen, H.M.; Au, C.T.; Chu, W.C.W.; Li, A.M.; Chan, K.C. Reduced Tongue Mobility: An Unrecognised Risk Factor of Childhood Obstructive Sleep Apnoea. Sleep 2021. [Google Scholar] [CrossRef] [PubMed]
- Guilleminault, C.; Huang, Y.S.; Quo, S. Apraxia in children and adults with obstructive sleep apnea syndrome. Sleep 2019, 42, zsz168. [Google Scholar] [CrossRef]
- Huang, Y.S.; Hsu, S.C.; Guilleminault, C.; Chuang, L.C. Myofunctional Therapy: Role in Pediatric OSA. Sleep Med. Clin. 2019, 14, 135–142. [Google Scholar] [CrossRef] [PubMed]
- De Felício, C.M.; da Silva Dias, F.V.; Folha, G.A.; de Almeida, L.A.; de Souza, J.F.; Anselmo-Lima, W.T.; Trawitzki, L.V.; Valera, F.C. Orofacial motor functions in pediatric obstructive sleep apnea and implications for myofunctional therapy. Int. J. Pediatr. Otorhinolaryngol. 2016, 90, 5–11. [Google Scholar] [CrossRef] [PubMed]
- De Felício, C.M.; da Silva Dias, F.V.; Trawitzki, L.V.V. Obstructive sleep apnea: Focus on myofunctional therapy. Nat. Sci. Sleep 2018, 10, 271–286. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Orr, J.; Jen, R.; Sands, S.A.; DeYoung, P.; Smales, E.; Edwards, B.; Owens, R.L.; Malhotra, A. Is there a threshold that triggers cortical arousals in obstructive sleep apnea. Sleep 2019, 42, zsz047. [Google Scholar] [CrossRef]
- Sands, S.A.; Terrill, P.I.; Edwards, B.A.; Taranto Montemurro, L.; Azarbarzin, A.; Marques, M.; de Melo, C.M.; Loring, S.H.; Butler, J.P.; White, D.P.; et al. Quantifying the Arousal Threshold Using Polysomnography in Obstructive Sleep Apnea. Sleep 2018, 41, zsx183. [Google Scholar] [CrossRef] [Green Version]
- Al-Shawwa, B.; Cruz, J.; Ehsan, Z.; Ingram, D.G. The challenges in scoring hypopneas in children: Is pulse wave amplitude drop the answer? Sleep Med. 2021, 81, 336–340. [Google Scholar] [CrossRef]
- Lopes, M.C.; Marcus, C.L. The significance of ASDA arousals in children. Sleep Med. 2007, 9, 3–8. [Google Scholar] [CrossRef]
- Rizzi, M.; Onorato, J.; Andreoli, A.; Colombo, S.; Pecis, M.; Marchisio, P.; Morelli, M.; Principi, N.; Esposito, S.; Sergi, M. Nasal resistances are useful in identifying children with severe obstructive sleep apnea before polysomnography. Int. J. Pediatr. Otorhinolaryngol. 2002, 65, 7–13. [Google Scholar] [CrossRef]
- Young, T.; Finn, L.; Kim, H. Nasal obstruction as a risk factor for sleep-disordered breathing. The University of Wisconsin Sleep and Respiratory Research Group. J. Allergy Clin. Immunol. 1997, 99, S757–S762. [Google Scholar] [CrossRef]
- Gozal, D.; Capdevila, O.S.; Kheirandish-Gozal, L.; Crabtree, V.M. APOE epsilon 4 allele, cognitive dysfunction, and obstructive sleep apnea in children. Neurology 2007, 69, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.S.; Guilleminault, C.; Hwang, F.M.; Cheng, C.; Lin, C.H.; Li, H.Y.; Lee, L.A. Inflammatory cytokines in pediatric obstructive sleep apnea. Medicine 2016, 95, e4944. [Google Scholar] [CrossRef] [PubMed]
- Khalyfa, A.; Serpero, L.D.; Kheirandish-Gozal, L.; Capdevila, O.S.; Gozal, D. TNF-alpha gene polymorphisms and excessive daytime sleepiness in pediatric obstructive sleep apnea. J. Pediatr. 2011, 158, 77–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, C.S.; Guilleminault, C.; Park, H.J.; Cho, J.H.; Lee, H.K.; Son, H.L.; Hwang, S.H. Correlation of salivary alpha amylase level and adenotonsillar hypertrophy with sleep disordered breathing in pediatric subjects. J. Clin. Sleep Med. 2014, 10, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Tauman, R.; Ivanenko, A.; O’Brien, L.M.; Gozal, D. Plasma C-reactive protein levels among children with sleep-disordered breathing. Pediatrics 2004, 113, e564–e569. [Google Scholar] [CrossRef] [Green Version]
- Kheirandish-Gozal, L.; Gozal, D. Pediatric OSA Syndrome Morbidity Biomarkers: The Hunt Is Finally On! Chest 2017, 151, 500–506. [Google Scholar] [CrossRef] [Green Version]
- Kassim, R.; Harris, M.A.; Leong, G.M.; Heussler, H. Obstructive sleep apnoea in children with obesity. J. Paediatr. Child Health 2016, 52, 284–290. [Google Scholar] [CrossRef]
- Mutlu, M.; Vuralkan, E.; Yardim Akaydin, S.; Akin, I.; Miser, E. Effects of adenoid/tonsillectomy on inflammatory response in snoring children with witnessed apnoea. Clin. Otolaryngol. 2014, 39, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Nachalon, Y.; Lowenthal, N.; Greenberg-Dotan, S.; Goldbart, A.D. Inflammation and growth in young children with obstructive sleep apnea syndrome before and after adenotonsillectomy. Mediat. Inflamm. 2014, 2014, 146893. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.S.; Chin, W.C.; Guilleminault, C.; Chu, K.C.; Lin, C.H.; Li, H.Y. Inflammatory Factors: Nonobese Pediatric Obstructive Sleep Apnea and Adenotonsillectomy. J. Clin. Med. 2020, 9, 1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gileles-Hillel, A.; Alonso-Alvarez, M.L.; Kheirandish-Gozal, L.; Peris, E.; Cordero-Guevara, J.A.; Teran-Santos, J.; Martinez, M.G.; Jurado-Luque, M.J.; Corral-Penafiel, J.; Duran-Cantolla, J.; et al. Inflammatory markers and obstructive sleep apnea in obese children: The NANOS study. Mediat. Inflamm. 2014, 2014, 605280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tam, C.S.; Wong, M.; McBain, R.; Bailey, S.; Waters, K.A. Inflammatory measures in children with obstructive sleep apnoea. J. Paediatr. Child Health 2006, 42, 277–282. [Google Scholar] [CrossRef] [Green Version]
- Gozal, D.; Serpero, L.D.; Sans Capdevila, O.; Kheirandish-Gozal, L. Systemic inflammation in non-obese children with obstructive sleep apnea. Sleep Med. 2008, 9, 254–259. [Google Scholar] [CrossRef] [Green Version]
- Lu, D.; Li, N.; Yao, X.; Zhou, L. Potential inflammatory markers in obstructive sleep apnea-hypopnea syndrome. Bosn. J. Basic Med. Sci. 2017, 17, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Tsou, P.Y.; Cielo, C.M.; Xanthopoulos, M.S.; Wang, Y.H.; Kuo, P.L.; Tapia, I.E. The burden of obstructive sleep apnea in pediatric sickle cell disease: A Kids’ inpatient database study. Sleep 2021, 44, zsaa157. [Google Scholar] [CrossRef]
- Maroda, A.J.; Spence, M.N.; Larson, S.R.; Estepp, J.H.; Gillespie, M.B.; Harris, A.J.; Mamidala, M.P.; Sheyn, A.M. Screening for Obstructive Sleep Apnea in Children with Sickle Cell Disease: A Pilot Study. Laryngoscope 2021, 131, E1022–E1028. [Google Scholar] [CrossRef]
- Arnaud, C.; Bochaton, T.; Pepin, J.L.; Belaidi, E. Obstructive sleep apnoea and cardiovascular consequences: Pathophysiological mechanisms. Arch. Cardiovasc. Dis. 2020, 113, 350–358. [Google Scholar] [CrossRef]
- Perez, C. Obstructive sleep apnea syndrome in children. Gen. Dent. 2018, 66, 46–50. [Google Scholar] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saint-Fleur, A.L.; Christophides, A.; Gummalla, P.; Kier, C. Much Ado about Sleep: Current Concepts on Mechanisms and Predisposition to Pediatric Obstructive Sleep Apnea. Children 2021, 8, 1032. https://doi.org/10.3390/children8111032
Saint-Fleur AL, Christophides A, Gummalla P, Kier C. Much Ado about Sleep: Current Concepts on Mechanisms and Predisposition to Pediatric Obstructive Sleep Apnea. Children. 2021; 8(11):1032. https://doi.org/10.3390/children8111032
Chicago/Turabian StyleSaint-Fleur, Ashley L., Alexa Christophides, Prabhavathi Gummalla, and Catherine Kier. 2021. "Much Ado about Sleep: Current Concepts on Mechanisms and Predisposition to Pediatric Obstructive Sleep Apnea" Children 8, no. 11: 1032. https://doi.org/10.3390/children8111032