
Effects of Dynamic Suit Orthoses on the Spatio-Temporal Gait Parameters in Children with Cerebral Palsy: A Systematic Review

 , ,
, ,  and
and
Abstract
:1. Introduction
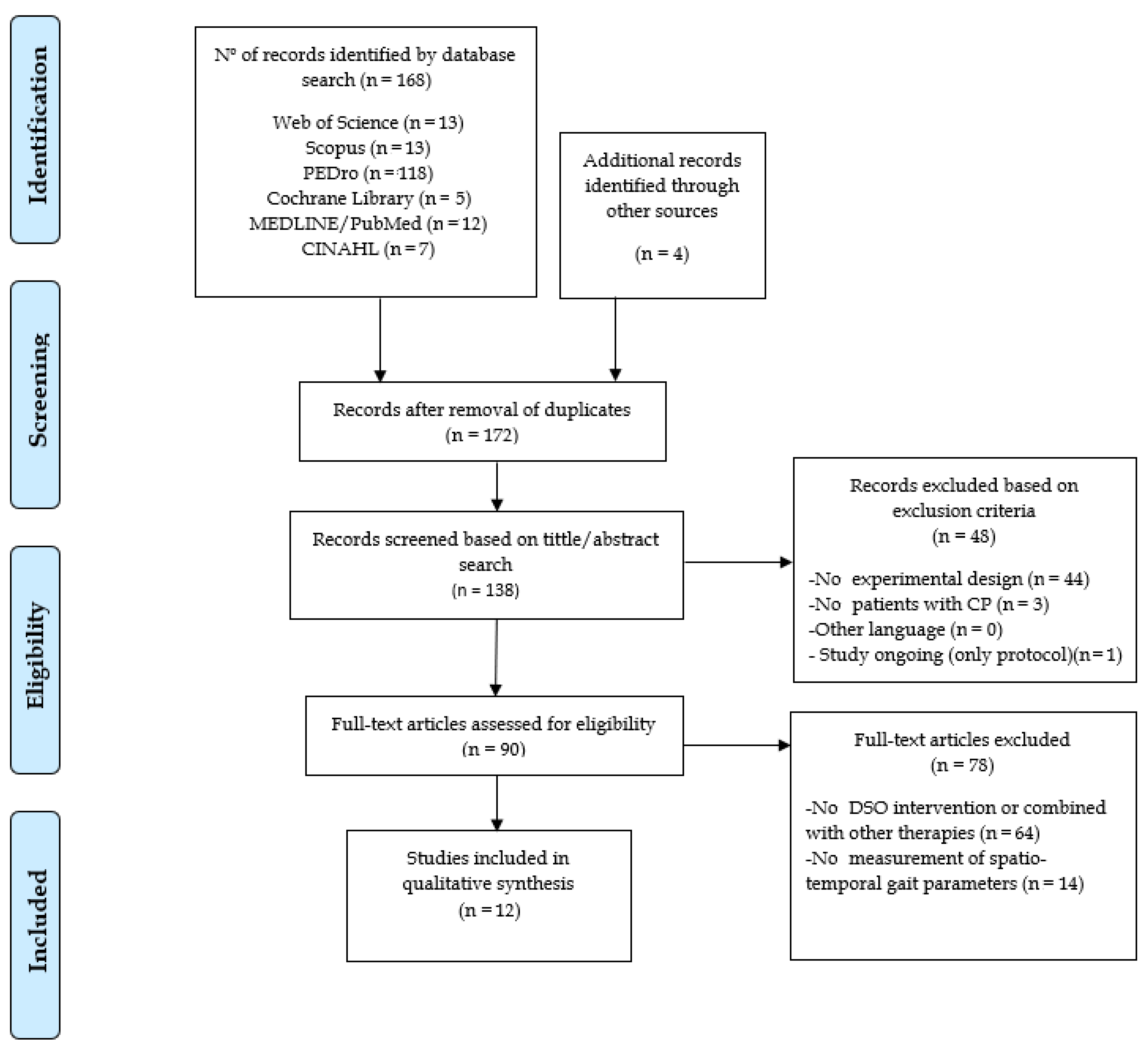
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
- P (Patients): cwCP with Gross Motor Function Classification System (GMFCS) level I–III.
- I (Intervention): Use of full body DSO. Interventions were included if they consisted in wearing the suit in isolation or using the suit in combination with conventional physical therapy (Neuro-Development Treatment, exercise programme). Theratogs, Dynamic Elastomeric Fabric Orthosis (DEFO) trousers, and external strap orthoses were included for their impact on pelvic biomechanics and axial control.
- C (Comparison): no intervention, other interventions, no comparison, and additional effect of DSO with conventional physical therapy.
- O (Outcomes): Spatio-temporal gait parameters.
- Use of subjective tools for measuring results (observational analysis, etc.).
- DSO intervention combined with other non-conventional therapies (i.e., virtual reality or use of robotic devices), except for those performed with the use of the suit.
2.4. Assessment of the Methodological Quality, Level of Evidence, and Grade of Recommendation
3. Results
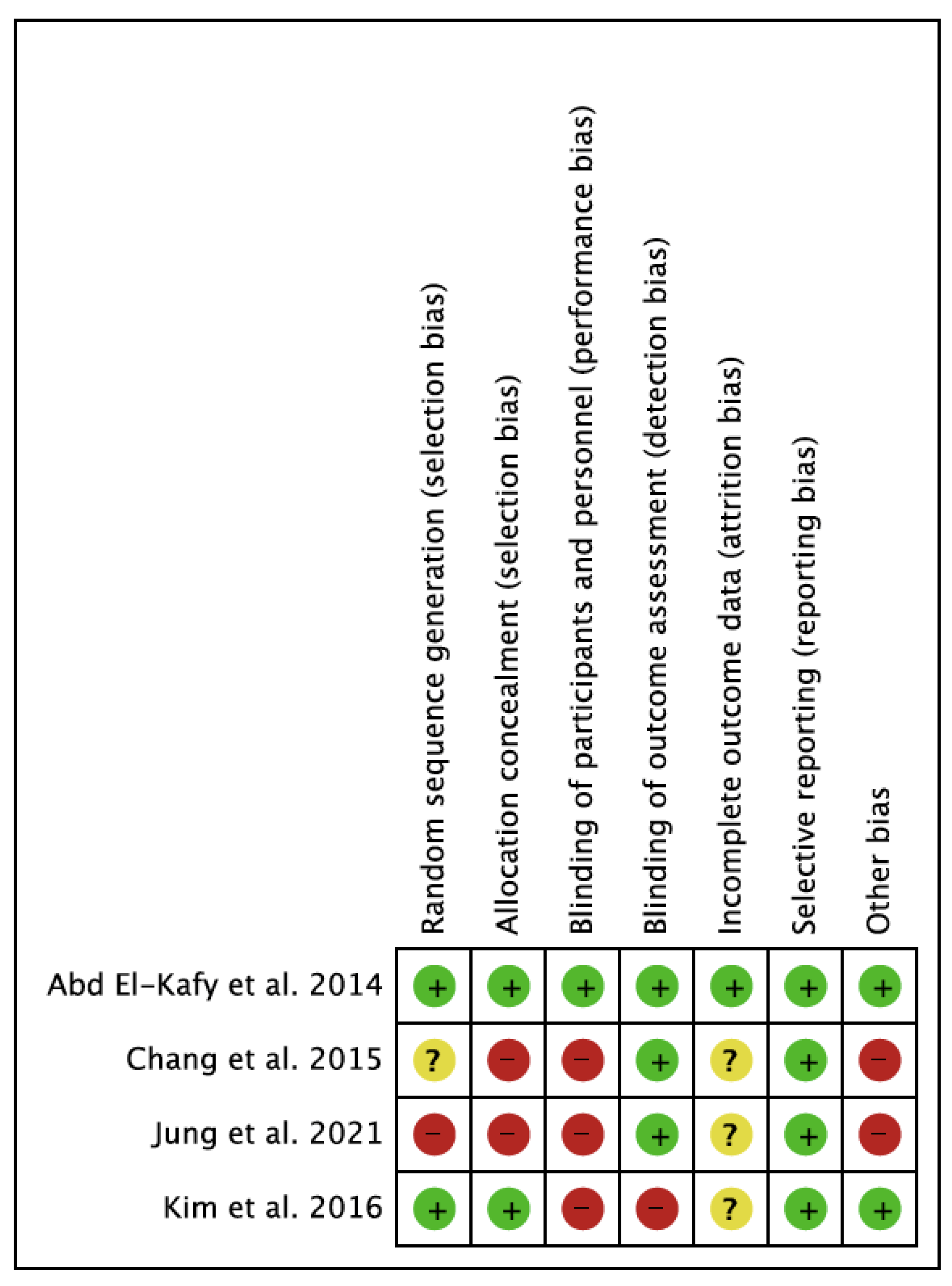
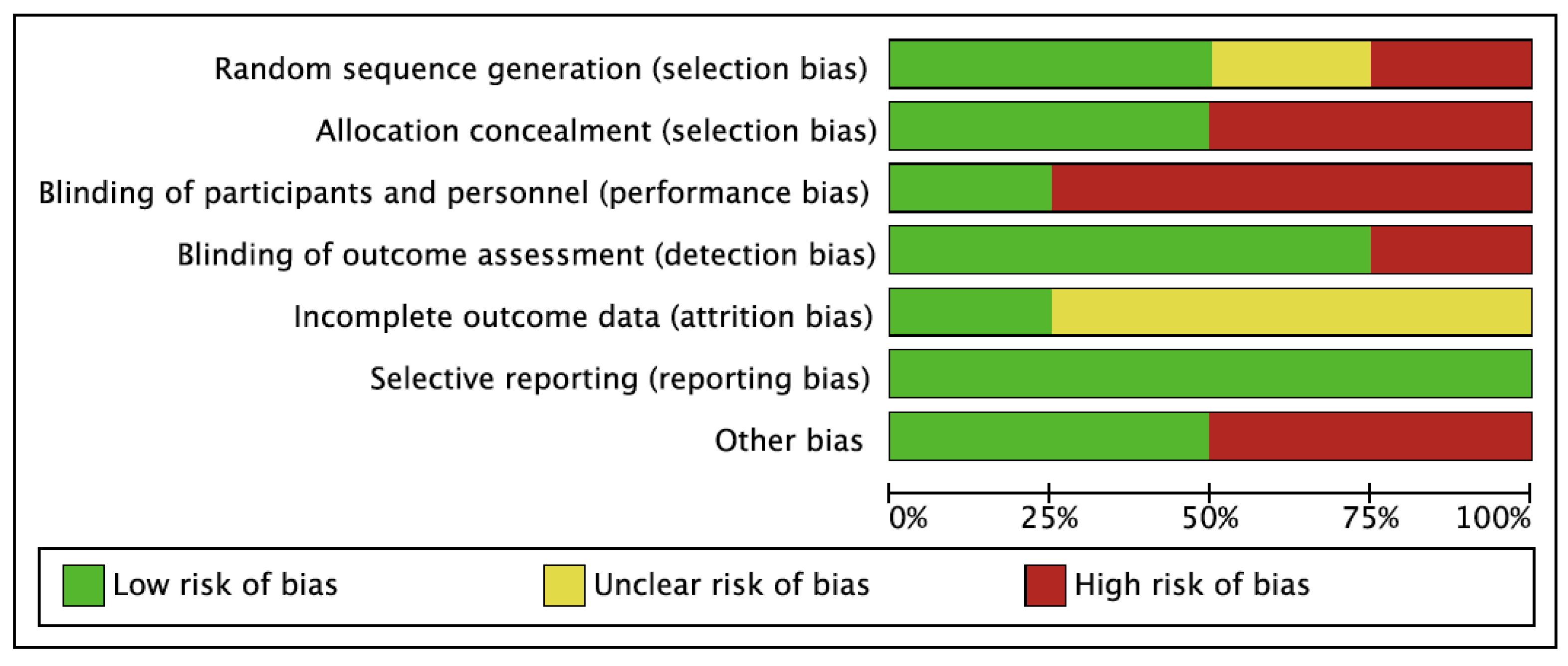
3.1. Methodological Quality, Level of Evidence, Grade of Recommendation, and Risk of Bias
3.2. Participant Characteristics
3.3. Intervention Characteristics
3.4. Outcomes Measures
4. Discussion
4.1. Outcome Measures, Intensity, and Type of Intervention
4.2. Functional Implications
4.3. Methodological Quality
4.4. Limits and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M. A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child. Neurol. 2007, 49, 8–14. [Google Scholar]
- Reddihough, D.S.; Collins, K.J. The epidemiology and causes of cerebral palsy. Aust. J. Physiother. 2003, 49, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Pascual, J.M.; Koenigsberger, M.R. Cerebral palsy: Prenatal risk factors. Rev. Neurol. 2003, 37, 275–280. [Google Scholar] [CrossRef]
- Bugler, K.E.; Gaston, M.S.; Robb, J.E. Distribution and motor ability of children with cerebral palsy in Scotland: A registry analysis. Scott. Med. J. 2019, 64, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Oskoui, M.; Coutinho, F.; Dykeman, J.; Jetté, N.; Pringsheim, T. An update on the prevalence of cerebral palsy: A systematic review and meta-analysis. Dev. Med. Child. Neurol. 2013, 55, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Granild-Jensen, J.B.; Rackauskaite, G.; Flachs, E.M.; Uldall, P. Predictors for early diagnosis of cerebral palsy from national registry data. Dev. Med. Child. Neurol. 2015, 57, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Smithers-Sheedy, H.; Badawi, N.; Blair, E.; Cans, C.; Himmelmann, K.; Krägeloh-Mann, I.; McIntyre, S.; Slee, J.; Uldall, P.; Watson, L.; et al. What constitutes cerebral palsy in the twenty-first century? Dev. Med. Child. Neurol. 2014, 56, 323–328. [Google Scholar] [CrossRef]
- Sadowska, M.; Sarecka-Hujar, B.; Kopyta, I. Cerebral palsy: Current opinions on definition, epidemiology, risk factors, classification and treatment options. Neuropsychiatr. Dis. Treat. 2020, 16, 1505–1518. [Google Scholar] [CrossRef]
- Dimakopoulos, R.; Syrogiannopoulos, G.; Grivea, I.; Dailiana, Z.; Youroukos, S.; Spinou, A. Kinematic and temporospatial changes in children with cerebral palsy during the initial stages of gait development. Dev. Neurorehabil. 2021, 1–9. [Google Scholar] [CrossRef]
- Chakraborty, S.; Nandy, A.; Kesar, T.M. Gait deficits and dynamic stability in children and adolescents with cerebral palsy: A systematic review and meta-analysis. Clin. Biomech. 2020, 71, 11–23. [Google Scholar] [CrossRef]
- Rethwilm, R.; Böhm, H.; Haase, M.; Perchthaler, D.; Dussa, C.U.; Federolf, P. Dynamic stability in cerebral palsy during walking and running: Predictors and regulation strategies. Gait Posture 2021, 84, 329–334. [Google Scholar] [CrossRef]
- Kurz, M.J.; Arpin, D.J.; Corr, B. Differences in the dynamic gait stability of children with cerebral palsy and typically developing children. Gait Posture 2012, 36, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Santorelli, F.M.; Maris, S.; Cioni, G.; Merete Braendvik, S.; Goihl, T.; Braaten, R.S.; Vereijken, B. The effect of increased gait speed on asymmetry and variability in children with cerebral palsy. Front. Neurol. 2020, 1, 1399. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Bulea, T.C.; Damiano, D.L. Greater reliance on cerebral palsy-specific muscle synergies during gait relates to poorer temporal-spatial performance measures. Front. Physiol. 2021, 12, 630627. [Google Scholar] [CrossRef] [PubMed]
- Kimoto, M.; Okada, K.; Sakamoto, H.; Kondou, T. The association between the maximum step length test and the walking efficiency in children with cerebral palsy. J. Phys. Ther. Sci. 2017, 29, 822–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.J.; Son, S.M. Comparison of spatiotemporal gait parameters between children with normal development and children with diplegic cerebral palsy. J. Phys. Ther. Sci. 2014, 26, 1317. [Google Scholar] [CrossRef] [Green Version]
- Õunpuu, S.; Gorton, G.; Bagley, A.; Sison-Williamson, M.; Hassani, S.; Johnson, B.; Oeffinger, D. Variation in kinematic and spatiotemporal gait parameters by Gross Motor Function Classification System level in children and adolescents with cerebral palsy. Dev. Med. Child. Neurol. 2015, 57, 955–962. [Google Scholar] [CrossRef] [Green Version]
- Morgan, P.; Murphy, A.; Opheim, A.; McGinley, J. Gait characteristics, balance performance and falls in ambulant adults with cerebral palsy: An observational study. Gait Posture 2016, 48, 243–248. [Google Scholar] [CrossRef]
- Iosa, M.; Marro, T.; Paolucci, S.; Morelli, D. Stability and harmony of gait in children with cerebral palsy. Res. Dev. Disabil. 2012, 33, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Calderón González, R.; Calderón Sepúlveda, R.F. Tratamiento de la espasticidad en parálisis cerebral con toxina botulínica. Rev. Neurol. 2002, 34, 52. [Google Scholar] [CrossRef]
- Booth, A.T.C.; Buizer, A.I.; Meyns, P.; Oude Lansink, I.L.B.; Steenbrink, F.; van der Krogt, M.M. The efficacy of functional gait training in children and young adults with cerebral palsy: A systematic review and meta-analysis. Dev. Med. Child. Neurol. 2018, 60, 866–883. [Google Scholar] [CrossRef] [PubMed]
- Ryan, J.M.; Cassidy, E.E.; Noorduyn, S.G.; O’Connell, N.E. Exercise interventions for cerebral palsy. Cochrane Database Syst. Rev. 2017, 6, CD011660. [Google Scholar] [CrossRef] [Green Version]
- Moreau, N.G.; Bodkin, A.W.; Bjornson, K.; Hobbs, A.; Soileau, M.; Lahasky, K. Effectiveness of rehabilitation interventions to improve gait speed in children with cerebral palsy: Systematic review and meta-analysis. Phys. Ther. 2016, 96, 1938–1954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corsi, C.; Santos, M.M.; Moreira, R.F.C.; Dos Santos, A.N.; de Campos, A.C.; Galli, M.; Rocha, N.A.C.F. Effect of physical therapy interventions on spatiotemporal gait parameters in children with cerebral palsy: A systematic review. Disabil. Rehabil. 2021, 43, 1507–1516. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Tan, Z.; Yun, G.; Cao, J.; Wang, J.; Liu, Q.; Chen, T. Effectiveness of exercise interventions for children with cerebral palsy: A systematic review and meta-analysis of randomized controlled trials. J. Rehabil. Med. 2021, 53, jrm00176. [Google Scholar] [CrossRef]
- Carvalho, I.; Pinto, S.M.; das Virgens Chagas, D.; Praxedes Dos Santos, J.L.; de Sousa Oliveira, T.; Batista, L.A. Robotic gait training for individuals with cerebral palsy: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2017, 98, 2332–2344. [Google Scholar] [CrossRef]
- Bahrami, F.; Noorizadeh Dehkordi, S.; Dadgoo, M. The efficacy of treadmill training on walking and quality of life of adults with spastic cerebral palsy: A randomized controlled trial. Iran. J. Child Neurol. 2019, 13, 121–133. [Google Scholar]
- Han, Y.-G.; Yun, C.-K. Effectiveness of treadmill training on gait function in children with cerebral palsy: Meta-analysis. J. Exerc. Rehabil. 2020, 16, 10–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómez-Pérez, C.; Font-Llagunes, J.M.; Martori, J.C.; Vidal Samsó, J. Gait parameters in children with bilateral spastic cerebral palsy: A systematic review of randomized controlled trials. Dev. Med. Child. Neurol. 2019, 61, 770–782. [Google Scholar] [CrossRef] [Green Version]
- Flett, P.J. Rehabilitation of spasticity and related problems in childhood cerebral palsy. J. Paediatr. Child. Health 2003, 39, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, A.; Krzak, J.; Peer, M.; Johnson, P.; Urban, M. Evaluation of short-term intensive orthotic garment use in children who have cerebral palsy. Pediatr. Phys. Ther. 2009, 21, 201–204. [Google Scholar] [CrossRef] [Green Version]
- Matthews, M.J.; Watson, M.; Richardson, B. Effects of dynamic elastomeric fabric orthoses on children with cerebral palsy. Prosthet. Orthot. Int. 2009, 33, 339–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Degelaen, M.; De Borre, L.; Buyl, R.; Kerckhofs, E.; De Meirleir, L.; Dan, B. Effect of supporting 3D-garment on gait postural stability in children with bilateral spastic cerebral palsy. NeuroRehabilitation 2016, 39, 175–181. [Google Scholar] [CrossRef]
- Bailes, A.F.; Greve, K.; Schmitt, L.C. Changes in two children with cerebral palsy after intensive suit therapy: A case report. Pediatr. Phys. Ther. 2010, 22, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Christy, J.B.; Chapman, C.G.; Murphy, P. The effect of intense physical therapy for children with cerebral palsy. J. Pediatr. Rehabil. Med. 2012, 5, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Karadağ-Saygı, E. The clinical aspects and effectiveness of suit therapies for cerebral palsy: A systematic review. Turk. J. Phys. Med. Rehabil. 2019, 65, 93–110. [Google Scholar] [CrossRef]
- Glowinski, S.; Blazejewski, A. Spider as a rehabilitation tool for patients with neurological disabilities: The preliminary research. J. Pers. Med. 2020, 10, 33. [Google Scholar] [CrossRef]
- World Health Organization International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001.
- World Health Organization. International Classification of Functioning, Disabiity and Health. Children & Youth Version (ICF-CY); World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Novak, I.; Mcintyre, S.; Morgan, C.; Campbell, L.; Dark, L.; Morton, N.; Stumbles, E.; Wilson, S.A.; Goldsmith, S. A systematic review of interventions for children with cerebral palsy: State of the evidence. Dev. Med. Child. Neurol. 2013, 55, 885–910. [Google Scholar] [CrossRef]
- Novak, I.; Morgan, C.; Fahey, M.; Finch-Edmondson, M.; Galea, C.; Hines, A.; Langdon, K.; Namara, M.; Paton, M.; Popat, H.; et al. State of the evidence traffic lights 2019: Systematic review of interventions for preventing and treating children with cerebral palsy. Curr. Neurol. Neurosci. Rep. 2020, 20, 3. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.; Park, J.; Lee, H.; Nam, K.; Park, T.; Kim, H.; Kwon, B. Efficacy of intensive neurodevelopmental treatment for children with developmental delay, with or without cerebral palsy. Ann. Rehabil. Med. 2017, 41, 90–96. [Google Scholar] [CrossRef] [Green Version]
- Yalcinkaya, E.Y.; Caglar, N.S.; Tugcu, B.; Tonbaklar, A. Rehabilitation outcomes of children with cerebral palsy. J. Phys. Ther. Sci. 2014, 26, 285–289. [Google Scholar] [CrossRef] [Green Version]
- Jackman, M.; Lannin, N.; Galea, C.; Sakzewski, L.; Miller, L.; Novak, I. What is the threshold dose of upper limb training for children with cerebral palsy to improve function? A systematic review. Aust. Occup. Ther. J. 2020, 67, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Almeida, K.M.; Fonseca, S.T.; Figueiredo, P.R.P.; Aquino, A.A.; Mancini, M.C. Effects of interventions with therapeutic suits (clothing) on impairments and functional limitations of children with cerebral palsy: A systematic review. Braz. J. Phys. Ther. 2017, 21, 307–320. [Google Scholar] [CrossRef]
- Martins, E.; Cordovil, R.; Oliveira, R.; Letras, S.; Lourenço, S.; Pereira, I.; Ferro, A.; Lopes, I.; Silva, C.R.; Marques, M. Efficacy of suit therapy on functioning in children and adolescents with cerebral palsy: A systematic review and meta-analysis. Dev. Med. Child. Neurol. 2016, 58, 348–360. [Google Scholar] [CrossRef]
- Wells, H.; Marquez, J.; Wakely, L. Garment therapy does not improve function in children with cerebral palsy: A Systematic review. Phys. Occup. Ther. Pediatr. 2018, 38, 395–416. [Google Scholar] [CrossRef]
- Zhou, J.Y.; Lowe, E.; Cahill-Rowley, K.; Mahtani, G.B.; Young, J.L.; Rose, J. Influence of impaired selective motor control on gait in children with cerebral palsy. J. Child. Orthop. 2019, 13, 73–81. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- da Costa Santos, C.M.; de Mattos Pimenta, C.A.; Cuce Nobre, M.R. The PICO strategy for the research question construction and evidence search. Rev. Lat. Am. Enferm. 2007, 15, 508–511. [Google Scholar] [CrossRef] [Green Version]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, P.A.; Harniss, M.K.; Schomer, K.G.; Feinberg, M.; Cullen, N.K.; Johnson, K.L. Conducting systematic evidence reviews: Core concepts and lessons learned. Arch. Phys. Med. Rehabil. 2012, 93, S177–S184. [Google Scholar] [CrossRef]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H.; Goddard, O.; et al. OCEBM Levels of Evidence Working Group: The Oxford 2011 Levels of Evidence. Oxford Centre for Evidence-Based Medicine. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 10 October 2021).
- Manterola, C.; Asenjo-Lobos, C.; Otzen, T. Hierarchy of evidence. Levels of evidence and grades of recommendation from current use. Rev. Chil. Infectol. 2014, 31, 705–718. [Google Scholar] [CrossRef] [Green Version]
- Mella Sousa, M.; Zamora Navas, P.; Mella Laborde, M.; Ballester Alfaro, J.J.; Uceda Carrascosa, P. Niveles de evidencia clínica y grados de recomendación Niveles de Evidencia Clínica y Grados de Recomendación. Rev. S And. Traum. Ort. 2012, 29, 59–72. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Jung, J.; Cho, H.; Lee, G. Immediate effects of orthotic garment and strapping system on balance and gait in children with spastic diplegia. Neurol. Asia 2021, 26, 355–360. [Google Scholar]
- Skublewska-Paszkowska, M.; Lukasik, E.; Milosz, M.; Smolka, J.; Napiorkowski, J.; Taczala, J.; Zdzienicka-Chyla, A.; Napiorkowski, J.; Kosiecz, A. Motion capture technology as a tool for quantitative assessment of the rehabilitation progress of gait by using soft orthoses. In Proceedings of the 11th International Conference on Human System Ineteraction, HIS, Gdansk, Poland, 4–6 July 2018; pp. 384–390. [Google Scholar]
- Kim, M.-R.; Lee, B.-H.; Park, D.-S. Effects of combined Adeli suit and neurodevelopmental treatment in children with spastic cerebral palsy with gross motor function classification system levels I and II. Hong Kong Physiother. J. Off. Publ. Hong Kong Physiother. Assoc. Ltd. 2016, 34, 10–18. [Google Scholar] [CrossRef] [Green Version]
- Lee, B.-H. Clinical usefulness of Adeli suit therapy for improving gait function in children with spastic cerebral palsy: A case study. J. Phys. Ther. Sci. 2016, 28, 1949–1952. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.D.; Chang, N.J.; Lin, H.Y.; Lai, P.T. Changes of plantar pressure and gait parameters in children with mild cerebral palsy who used a customized external strap orthosis: A crossover study. Biomed. Res. Int. 2015, 2015, 813942. [Google Scholar] [CrossRef] [Green Version]
- Abd El-Kafy, E.M. The clinical impact of orthotic correction of lower limb rotational deformities in children with cerebral palsy: A randomized controlled trial. Clin. Rehabil. 2014, 28, 1004–1014. [Google Scholar] [CrossRef]
- Ko, M.-S.; Lee, J.-A.; Kang, S.-Y.; Jeon, H.-S. Effect of Adeli suit treatment on gait in a child with cerebral palsy: A single-subject report. Physiother. Theory Pract. 2015, 31, 275–282. [Google Scholar] [CrossRef]
- Cámara Tobalina, J. Gait analysis: Phases and spatio-temporal variables. Entramado 2011, 7, 160–173. [Google Scholar]
- Grieve, D.W.; Gear, R.J. The relationships between length of stride, step frequency, time of swing and speed of walking for children and adults. Ergonomics 1966, 9, 379–399. [Google Scholar] [CrossRef]
- Wert, D.M.; Brach, J.; Perera, S.; VanSwearingen, J.M. Gait biomechanics, spatial and temporal characteristics, and the energy cost of walking in older adults with impaired mobility. Phys. Ther. 2010, 90, 977–985. [Google Scholar] [CrossRef]
- Saether, R.; Helbostad, J.L.; Adde, L.; Brændvik, S.; Lydersen, S.; Vik, T. Gait characteristics in children and adolescents with cerebral palsy assessed with a trunk-worn accelerometer. Res. Dev. Disabil. 2014, 35, 1773–1781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Park, I.; On, L. Reliability and Validity of Gait Speed Test. J. Exerc. Nutr. Biochem. 2016, 20, 46–50. [Google Scholar] [CrossRef] [PubMed]
- De Mattos, C.; Patrick Do, K.; Pierce, R.; Feng, J.; Aiona, M.; Sussman, M. Comparison of hamstring transfer with hamstring lengthening in ambulatory children with cerebral palsy: Further follow-up. J. Child. Orthop. 2014, 8, 513–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Databases | Search Equation | Results |
|---|---|---|
| Web of Science | TS = (“suit wear” OR “space suits” OR lycra OR Adeli OR therasuit OR “strapping system” OR theratog* OR “suit therapy”) AND TS = (“cerebral palsy” AND gait) | 13 |
| Scopus | TITLE-ABS-KEY ((“suit wear” OR “space suits” OR lycra OR Adeli OR therasuit OR “strapping system” OR theratog* OR “suit therapy”) AND (“cerebral palsy” AND gait)) | 13 |
| PEDro | Therapy: orthoses, taping, splinting Subdiscipline: neurology Topic: cerebral palsy | 118 |
| Cochrane Library | TITLE-ABS-KEY (“suit wear” OR “space suits” OR lycra OR Adeli OR therasuit OR “strapping system” OR theratog* OR “suit therapy”) AND “cerebral palsy” AND gait | 5 |
| CINAHL | (“suit wear” OR “space suits” OR lycra OR Adeli OR therasuit OR “strapping system” OR theratog* OR “suit therapy”) AND “cerebral palsy” AND gait | 7 |
| MEDLINE/PubMed | (“suit wear” OR “space suits” OR lycra OR Adeli OR therasuit OR “strapping system” OR theratog* OR “suit therapy”) AND “cerebral palsy” AND gait | 12 |
| TOTAL | 168 |
| Authors Year GR, LoE | Design | Sample | Age (Aver) | Type of CP/GMFCS | Measurement/Tools | Performance of Evaluation | N Sessions, Temporality | Results |
|---|---|---|---|---|---|---|---|---|
| Jung et al. 2021 [57] A, 1b | RCT Cross-over | n = 24 TFB1 = 24 TFB2 = 24 | 6.17 | Spastic diplegia (I–II) | STV: walking speed, cadence, step length, stride length, single support time, double support time MT: 3D-MAS | Pre/Post-intervention | 1 ses (30 m | Post-TFB intervention, showed significant improvements in walking speed, cadence, step length, stride length, single support time, and double support time |
| Skublewska-Paszkowska et al. 2018 [58] C,4 | EDS | n = 1 TTO = 1 | 5 | Spastic diplegia (II) | STV: walking speed, cadence, step time, step length MT:3D-MAS | Pre/Post-intervention (w-wh TTO in both cases) | 60 ses, 12 week | Significant improvement measured post-intervention without TTO in walking speed. Significant improvement measured post-intervention with TTO in stabilisation of step length |
| Degelaen et al. 2016 [33] B,3b | QED | n = 31 CP = 15 TDC = 16 | 7.27 | Spastic diplegia (I–II) | STV: walking speed, cadence, step length MT:3D-MAS | Own clothes/ wearing FBS | 1 ses | CP group wearing FBS, showed significant improvements in walking speed (p < 0.003) and cadence (p < 0.001), but not in step length |
| Kim et al. 2016 [59] A, 1b | RCT | n = 17 AST/NDT = 8 NDT = 9 | 5.64 | Spastic diplegia, cuadriplegia (I–II) | STV: walking speed, cadence, step length, stride length, step length, and stride length symmetry MT:3D-MAS | Pre/Post-intervention | AST/NDT: 60 ses AST: 30 m/ses,1 ses/day, 5 days/week, 6 weeks NDT: 30 m/ses, 2 ses/day, 5 day/week, 6 weeks NDT: 60 ses 30 m/ses, 2 ses/day, 5 day/week, 6 weeks | AST + NDT group showed significant increase in walking speed, cadence, and step length symmetry (p < 0.001, 0.003, 0.027) NDT group improved step length and stride length symmetry (p = 0.006, 0.018) None of the groups showed improvement in stride length |
| Lee 2016 [60] C,4 | CS | n = 2 AST = 2 | 4.5 | Spastic diplegia (II) | STV: walking speed, cadence, step length, stride length MT: 3D-MAS | Pre/Post-intervention | 20 ses (60 m), 5 day/week, 4 weeks | Both cases showed improvement in cadence, only one showed improvement in step length symmetry and walking speed. Results for step length and stride length were variable in each case. |
| Chang et al. 2015 [61] A, 1b | RCT Cross-over | n = 9 ESO 1 = 9 ESO 2 = 9 | 8.73 | Spastic diplegia (I–II) | STV: walking speed, cadence, stride length MT: 3D-MAS | Own clothes/ wearing ESO | 1 ses (10 m) | Significant changes between ESO control, showed an increase in walking speed (p = 0.036), cadence (p = 0.005), and stride length (p = 0.011), wearing ESO |
| Abd El-Kafy 2014 [62] A, 1b | RCT | n = 57 NO = 18 TTG = 16 TTG + AFO = 17 | 7.3 | Spastic diplegia (I–II) | STV: walking speed, cadence, stride length MT: 3D-MAS | Pre/Post-intervention | 60 ses (2 h), 1 ses/day, 5 days/week, 12 weeks | Significant post-intervention differences among three groups in walking speed, stride length, and cadence (p = 0.03, 0.001, 0.011). Best improvements of all gait parameters were shown in group C |
| Ko et al. 2014 [63] C,4 | EDS | n = 1 AST = 1 | 8 | Spastic diplegia (III) | STV: walking speed, stride time, stride length, stride width MT: 3D-MAS, 10-MWT | Pre/Post-intervention (1–25 ses) 10-MWT: each ses | 18 ses (50 m), 1 ses/day, 1 day/week, 18 weeks | Significant improvement post-treatment in walking speed, stride length, stride width, and step time. 10-MWT improved after each session and growing up until the end of intervention. |
| Christy et al. 2012 [35] C,4 | QED Follow up | n = 17 TST = 17 | 7.6 | Spastic, hypotonic, athetoid, ataxic diplegia cuadriplegia triplegia (I–III) | STV: cadence MT: step activity monitor | Pre/Post-intervention (I. effects, 3 months/later) | 15 ses (4 h), 1 ses/day, 5 day/week, 3 weeks | Immediate post-intervention and follow-up showed trends of improvements in cadence, but there was no significant improvement immediately after or at 3 months compared to pre-intervention |
| Bailes et al. 2010 [34] C,4 | CS | n = 2 TST = 2 | 7.5 | Spastic diplegia (III) | STV: walking speed, cadence, single support time, double support time, step length, stride length MT: 3D-MAS | Pre/Post-intervention (4 d/later) | 15 ses (4 h), 1 ses/day, 5 days/week, 3 weeks | Both subjects showed post-intervention improvement in walking speed and cadence. Only one had changes in double support time and single support time. No significant changes were reported in stride length or step length in any case |
| Matthews et al. 2009 [32] C,4 | CS | n = 8 DEFO = 8 | 5.5 | Spastic diplegia (I–III) | STV: walking speed MT: 10-MWT | Pre/During/ Post-intervention (Immediate effects and 6 w/later) | 30 ses (8 h) 1 ses/day, 5 day/week 6 weeks | Five subjects showed significant changes in walking time and four in walking time variation, between pre-intervention and during intervention in both cases. However, changes were not uniform |
| Flanagan et al. 2009 [31] C,4 | QED | n = 5 TTG = 5 | 7–13 | Spastic diplegia (I) | STV: walking speed, cadence, step length, stride length MT: 3D-MAS | Pre/Post-intervention (I. effects with/without suit, 2 and 4 months/later without suit) | 84 ses, 1 ses/day, 5 days/week, 12 weeks | There were no significant pre/post-intervention changes in spatio-temporal gait parameters |
| Jung et al. 2021 [57] | Skublewska-Paszkowska et al. 2018 [58] | Degelaen et al. 2016 [33] | Kim et al. 2016 [59] | Lee 2016 [60] | Chang et al. 2015 [61] | Abd El-Kafy 2014 [62] | Ko et al. 2014 [63] | Christy et al. 2012 [35] | Bailes et al. 2010 [34] | Matthews et al. 2009 [32] | Flanagan et al. 2009 [31] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study quality | 7 | 6 | 6 | 8 | 5 | 7 | 7 | 7 | 9 | 7 | 6 | 6 |
| External validity (study bias) | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 1 |
| Internal validity (study bias) | 7 | 2 | 4 | 9 | 2 | 9 | 9 | 3 | 4 | 5 | 2 | 2 |
| Statistical power | 5 | 1 | 1 | 5 | 1 | 5 | 5 | 1 | 5 | 1 | 5 | 3 |
| Total score | 19 | 9 | 11 | 23 | 8 | 21 | 22 | 11 | 19 | 13 | 14 | 12 |
| Percentage (%) | 59 | 28 | 34 | 71 | 25 | 65 | 68 | 34 | 59 | 40 | 43 | 37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belizón-Bravo, N.; Romero-Galisteo, R.P.; Cano-Bravo, F.; Gonzalez-Medina, G.; Pinero-Pinto, E.; Luque-Moreno, C. Effects of Dynamic Suit Orthoses on the Spatio-Temporal Gait Parameters in Children with Cerebral Palsy: A Systematic Review. Children 2021, 8, 1016. https://doi.org/10.3390/children8111016
Belizón-Bravo N, Romero-Galisteo RP, Cano-Bravo F, Gonzalez-Medina G, Pinero-Pinto E, Luque-Moreno C. Effects of Dynamic Suit Orthoses on the Spatio-Temporal Gait Parameters in Children with Cerebral Palsy: A Systematic Review. Children. 2021; 8(11):1016. https://doi.org/10.3390/children8111016
Chicago/Turabian StyleBelizón-Bravo, Natalia, Rita Pilar Romero-Galisteo, Fatima Cano-Bravo, Gloria Gonzalez-Medina, Elena Pinero-Pinto, and Carlos Luque-Moreno. 2021. "Effects of Dynamic Suit Orthoses on the Spatio-Temporal Gait Parameters in Children with Cerebral Palsy: A Systematic Review" Children 8, no. 11: 1016. https://doi.org/10.3390/children8111016