Effect of Linear and Nonlinear Pedagogy Physical Education Interventions on Children’s Physical Activity: A Cluster Randomized Controlled Trial (SAMPLE-PE)

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
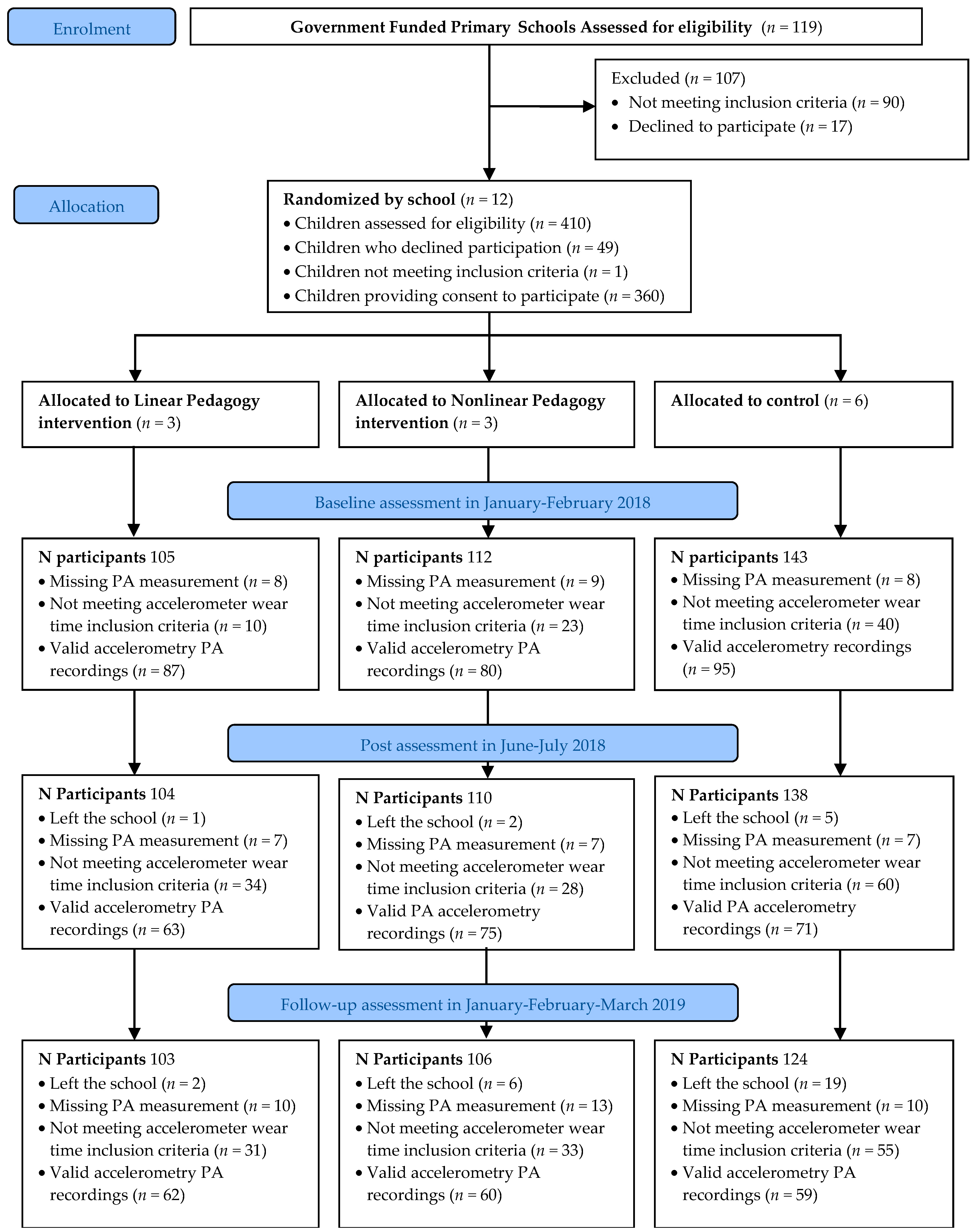
2.1. Study Design and Participants
2.2. Intervention
2.2.1. Intervention Deliverers Training
2.2.2. Interventions
2.2.3. Linear Pedagogy Intervention
2.2.4. Nonlinear Pedagogy Intervention
2.3. Outcomes
2.3.1. Demographics
2.3.2. Anthropometrics
2.3.3. Physical Activity
2.4. Intervention Fidelity
2.5. Randomization and Power
2.6. Data Analysis
3. Results
3.1. Baseline Characteristics
3.2. Fidelity Assessment
3.3. Intervention Effect on Physical Activity Outcomes
3.4. Effects of Covariates on Physical Activity Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marker:, A.M.; Steele, R.G.; Noser, A.E. Physical activity and health-related quality of life in children and adolescents: A systematic review and meta-analysis. Health Psychol. 2018, 37, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.; Richards, J.; Hillman, C.; Faulkner, G.; Beauchamp, M.; Nilsson, M.; Kelly, P.; Smith, J.; Raine, L.; Biddle, S. Physical activity for cognitive and mental health in youth: A systematic review of mechanisms. Pediatrics 2016, 138, e20161642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarp, J.; Brønd, J.C.; Andersen, L.B.; Møller, N.C.; Froberg, K.; Grøntved, A. Physical activity, Sedentary behavior, And long-term cardiovascular risk in young people: A review and discussion of methodology in prospective studies. J. Sport Health Sci. 2016, 5, 145–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whooten, R.; Kerem, L.; Stanley, T. Physical activity in adolescents and children and relationship to metabolic health. Curr. Opin. Endocrinol. Diabetes Obes. 2019, 26, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.E.; Hillman, C.H.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szabo-Reed, A.N. Physical activity, fitness, cognitive function, and academic achievement in children: A systematic review. Med. Sci. Sports Exerc. 2016, 48, 1197–1222. [Google Scholar] [CrossRef] [Green Version]
- Telama, R.; Yang, X.; Leskinen, E.; Kankaanpää, A.; Hirvensalo, M.; Tammelin, T.; Viikari, J.S.A.; Raitakari, O.T. Tracking of physical activity from early childhood through youth into adulthood. Med. Sci. Sports Exerc. 2014, 46, 955–962. [Google Scholar] [CrossRef]
- Griffiths, L.J.; Cortina-Borja, M.; Sera, F.; Pouliou, T.; Geraci, M.; Rich, C.; Cole, T.J.; Law, C.; Joshi, H.; Ness, A.R.; et al. How active are our children? Findings from the millennium cohort study. BMJ Open 2013, 3, e002893. [Google Scholar] [CrossRef] [Green Version]
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [Green Version]
- Manyanga, T.; Barnes, J.D.; Chaput, J.P.; Katzmarzyk, P.T.; Prista, A.; Tremblay, M.S. Prevalence and correlates of adherence to movement guidelines among urban and rural children in Mozambique: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2019, 16. [Google Scholar] [CrossRef]
- Roman-Viñas, B.; Chaput, J.P.; Katzmarzyk, P.T.; Fogelholm, M.; Lambert, E.V.; Maher, C.; Maia, J.; Olds, T.; Onywera, V.; Sarmiento, O.L.; et al. Proportion of children meeting recommendations for 24-hour movement guidelines and associations with adiposity in a 12-country study. Int. J. Behav. Nutr. Phys. Act. 2016, 13. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, C.; Tremblay, M.S.; Okuda, M.; Inoue, S.; Tanaka, S. Proportion of Japanese primary school children meeting recommendations for 24-h movement guidelines and associations with weight status. In Obesity Research and Clinical Practice; Elsevier Ltd.: Amsterdam, The Netherlands, 2020; Volume 14, pp. 234–240. [Google Scholar]
- Love, R.; Adams, J.; Atkin, A.; Van Sluijs, E. Socioeconomic and ethnic differences in children’s vigorous intensity physical activity: A cross-sectional analysis of the UK Millennium Cohort Study. BMJ Open 2019, 9, e027627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, D.; Ramirez Varela, A.; Bauman, A.E.; Ekelund, U.; Lee, I.M.; Heath, G.; Katzmarzyk, P.T.; Reis, R.; Pratt, M. Towards better evidence-informed global action: Lessons learnt from the Lancet series and recent developments in physical activity and public health. Br. J. Sports Med. 2020, 54, 462–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.; Gu, X. Toward Active Living: Comprehensive School Physical Activity Program Research and Implications. Quest 2018, 70, 191–212. [Google Scholar] [CrossRef]
- Hills, A.P.; Dengel, D.R.; Lubans, D.R. Supporting Public Health Priorities: Recommendations for Physical Education and Physical Activity Promotion in Schools. Prog. Cardiovasc. Dis. 2015, 57, 368–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grao-Cruces, A.; Velásquez-Romero, M.J.; Rodriguez-Rodríguez, F. Levels of physical activity during school hours in children and adolescents: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 4773. [Google Scholar] [CrossRef] [PubMed]
- Yli-Piipari, S.; Kulmala, J.S.; Jaakkola, T.; Hakonen, H.; Fish, J.C.; Tammelin, T. Objectively measured school day physical activity among elementary students in the United States and Finland. J. Phys. Act. Health 2016, 13, 440–446. [Google Scholar] [CrossRef] [Green Version]
- Hollis, J.L.; Williams, A.J.; Sutherland, R.; Campbell, E.; Nathan, N.; Wolfenden, L.; Morgan, P.J.; Lubans, D.R.; Wiggers, J. A systematic review and meta-analysis of moderate-to-vigorous physical activity levels in elementary school physical education lessons. Prev. Med. 2016, 86, 34–54. [Google Scholar] [CrossRef]
- UNESCO. Quality Physical Education (QPE): Guidelines for Policy Makers; United Nations Educational, Scientific and Cultural Organization: Paris, France, 2015; Available online: https://en.unesco.org/inclusivepolicylab/sites/default/files/learning/document/2017/1/231101E.pdf (accessed on 23 September 2020).
- Tompsett, C.; Sanders, R.; Taylor, C.; Cobley, S. Pedagogical Approaches to and Effects of Fundamental Movement Skill Interventions on Health Outcomes: A Systematic Review. Sport. Med. 2017, 47, 1795–1819. [Google Scholar] [CrossRef]
- Errisuriz, V.L.; Golaszewski, N.M.; Born, K.; Bartholomew, J.B. Systematic Review of Physical Education-Based Physical Activity Interventions Among Elementary School Children. J. Prim. Prev. 2018, 39, 303–327. [Google Scholar] [CrossRef]
- Sacchetti, R.; Ceciliani, A.; Garulli, A.; Dallolio, L.; Beltrami, P.; Leoni, E. Effects of a 2-Year School-Based Intervention of Enhanced Physical Education in the Primary School. J. Sch. Health 2013, 83, 639–646. [Google Scholar] [CrossRef]
- Manios, Y.; Kafatos, A.; Mamalakis, G. The effects of a health education intervention initiated at first grade over a 3 year period: Physical activity and fitness indices. Health Educ. Res. 1998, 13, 593–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatzisarantis, N.L.D.; Hagger, M.S. Effects of an intervention based on self-determination theory on self-reported leisure-time physical activity participation. Psychol. Health 2009, 24, 29–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Invernizzi, P.; Crotti, M.; Bosio, A.; Cavaggioni, L.; Alberti, G.; Scurati, R. Multi-Teaching Styles Approach and Active Reflection: Effectiveness in Improving Fitness Level, Motor Competence, Enjoyment, Amount of Physical Activity, and Effects on the Perception of Physical Education Lessons in Primary School Children. Sustainability 2019, 11, 405. [Google Scholar] [CrossRef] [Green Version]
- Verstraete, S.J.M.; Cardon, G.M.; De Clercq, D.L.R.; De Bourdeaudhuij, I.M.M. A comprehensive physical activity promotion programme at elementary school: The effects on physical activity, physical fitness and psychosocial correlates of physical activity. Public Health Nutr. 2007, 10, 477–484. [Google Scholar] [CrossRef]
- Caballero, B.; Clay, T.; Davis, S.M.; Ethelbah, B.; Rock, B.H.; Lohman, T.; Norman, J.; Story, M.; Stone, E.J.; Stephenson, L.; et al. Pathways: A school-based, randomized controlled trial for the prevention of obesity in American Indian schoolchildren. Am. J. Clin. Nutr. 2003, 78, 1030–1038. [Google Scholar] [CrossRef] [Green Version]
- Sallis, J.F.; McKenzie, T.L.; Alcaraz, J.E.; Kolody, B.; Faucette, N.; Hovell, M.F. The effects of a 2-year physical education program (SPARK) on physical activity and fitness in elementary school students. Am. J. Public Health 1997, 87, 1328–1334. [Google Scholar] [CrossRef] [Green Version]
- Telford, R.M.; Olive, L.S.; Cochrane, T.; Davey, R.; Telford, R.D. Outcomes of a four-year specialist-taught physical education program on physical activity: A cluster randomized controlled trial, the LOOK study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 64. [Google Scholar] [CrossRef] [Green Version]
- Donnelly, J.E.; Jacobsen, D.J.; Whatley, J.E.; Hill, J.O.; Swift, L.L.; Cherrington, A.; Polk, B.; Tran, Z.V.; Reed, G. Nutrition and physical activity program to attenuate obesity and promote physical and metabolic fitness in elementary school children. Obes. Res. 1996, 4, 229–243. [Google Scholar] [CrossRef]
- Kokkonen, J.; Yli-Piipari, S.; Kokkonen, M.; Quay, J. Effectiveness of a creative physical education intervention on elementary school students’ leisure-time physical activity motivation and overall physical activity in Finland. Eur. Phys. Educ. Rev. 2019, 25, 796–815. [Google Scholar] [CrossRef] [Green Version]
- Warren, W.H. The dynamics of perception and action. Psychol. Rev. 2006, 113, 358–389. [Google Scholar] [CrossRef] [Green Version]
- SHAPE America The Essential Components of Physical Education. Available online: www.shapeamerica.org (accessed on 17 November 2020).
- Physical Education Programmes of Study: Key Stages 1 and 2 National Curriculum in England, 2013. UK Government. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/239040/PRIMARY_national_curriculum_-_Physical_education.pdf (accessed on 17 November 2020).
- Australian Curriculum Assessment and Reporting Authority Health and Physical Education|The Australian Curriculum. Available online: https://www.australiancurriculum.edu.au/f-10-curriculum/health-and-physical-education/ (accessed on 17 November 2020).
- Utesch, T.; Bardid, F. Motor competence. In Dictionary of Sport Psychology: Sport, Exercise, and Performing Arts, 1st ed.; Dieter, H., Robert, S., Bernd, S., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; p. 186. [Google Scholar]
- Lima, R.A.; Pfeiffer, K.; Larsen, L.R.; Bugge, A.; Moller, N.C.; Anderson, L.B.; Stodden, D.F. Physical activity and motor competence present a positive reciprocal longitudinal relationship across childhood and early adolescence. J. Phys. Act. Health 2017, 14, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Davis, R.E.; Fu, Y.C. Early motor skill competence as a mediator of child and adult physical activity. Prev. Med. Reports 2015, 2, 833–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Utesch, T.; Dreiskämper, D.; Naul, R.; Geukes, K. Understanding physical (in-) activity, overweight, and obesity in childhood: Effects of congruence between physical self-concept and motor competence. Sci. Rep. 2018, 8, 5908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stodden, D.F.; Langendorfer, S.J.; Goodway, J.D.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A developmental perspective on the role of motor skill competence in physical activity: An emergent relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Robinson, L.E.; Stodden, D.F.; Barnett, L.M.; Lopes, V.P.; Logan, S.W.; Rodrigues, L.P.; D’Hondt, E. Motor Competence and its Effect on Positive Developmental Trajectories of Health. Sport. Med. 2015, 45, 1273–1284. [Google Scholar] [CrossRef]
- Hulteen, R.M.; Morgan, P.J.; Barnett, L.M.; Stodden, D.F.; Lubans, D.R. Development of Foundational Movement Skills: A Conceptual Model for Physical Activity Across the Lifespan. Sport. Med. 2018, 48, 1533–1540. [Google Scholar] [CrossRef]
- Engel, A.C.; Broderick, C.R.; van Doorn, N.; Hardy, L.L.; Parmenter, B.J. Exploring the Relationship Between Fundamental Motor Skill Interventions and Physical Activity Levels in Children: A Systematic Review and Meta-analysis. Sport. Med. 2018, 48, 1845–1857. [Google Scholar] [CrossRef]
- Rudd, J.R.; Pesce, C.; Strafford, B.W.; Davids, K. Physical Literacy—A Journey of Individual Enrichment: An Ecological Dynamics Rationale for Enhancing Performance and Physical Activity in All. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.A. A schema theory of discrete motor skill learning. Psychol. Rev. 1975, 82, 225–260. [Google Scholar] [CrossRef]
- Fitts, P.; Posner, M. Human Performance; Brooks/Cole: Belmont, CA, USA, 1967. [Google Scholar]
- Beilock, S.L.; Carr, T.H.; MacMahon, C.; Starkes, J.L. When paying attention becomes counterproductive: Impact of divided versus skill-focused attention on novice and experienced performance of sensorimotor skills. J. Exp. Psychol. Appl. 2002, 8, 6–16. [Google Scholar] [CrossRef]
- Kirk, D. Physical Education Futures; Taylor & Francis Group: London, UK, 2009; ISBN 0203874625. [Google Scholar]
- Metzler, M. Instructional Models in Physical Education; Routledge: New York, NY, USA, 2017. [Google Scholar]
- Magill, R.A. Motor learning is meaningful for physical educators. Quest 1990, 42, 126–133. [Google Scholar] [CrossRef]
- Peers, C.; Issartel, J.; Behan, S.; O’Connor, N.; Belton, S. Movement competence: Association with physical self-efficacy and physical activity. Hum. Mov. Sci. 2020, 70, 102582. [Google Scholar] [CrossRef] [PubMed]
- Susan, H. A model of mastery motivation in children: Individual differences and developmental change. In The Minnesota Symposium on Child Psychology; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1981; Volume 14, pp. 215–223. [Google Scholar]
- Chow, J.Y.; Atencio, M. Complex and nonlinear pedagogy and the implications for physical education. Sport. Educ. Soc. 2014, 19, 1034–1054. [Google Scholar] [CrossRef]
- Rudd, J.R.; Crotti, M.; Fitton-Davies, K.; O’Callaghan, L.; Bardid, F.; Utesch, T.; Roberts, S.; Boddy, L.M.; Cronin, C.J.; Knowles, Z.; et al. Skill Acquisition Methods Fostering Physical Literacy in Early-Physical Education (SAMPLE-PE): Rationale and Study Protocol for a Cluster Randomized Controlled Trial in 5–6-Year-Old Children from Deprived Areas of North West England. Front. Psychol. 2020, 11, 1228. [Google Scholar] [CrossRef]
- Moy, B.; Renshaw, I.; Davids, K. The impact of nonlinear pedagogy on physical education teacher education students’ intrinsic motivation. Phys. Educ. Sport Pedagog. 2016, 21, 517–538. [Google Scholar] [CrossRef]
- Lee, M.C.Y.; Chow, J.Y.; Button, C.; Tan, C.W.K. Nonlinear Pedagogy and its role in encouraging twenty-first century competencies through physical education: A Singapore experience. Asia Pacific J. Educ. 2017, 37, 483–499. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, 869. [Google Scholar] [CrossRef] [Green Version]
- Morgan, P.J.; Hansen, V. Classroom teachers’ perceptions of the impact of barriers to teaching physical education on the quality of physical education programs. Res. Q. Exerc. Sport 2008, 79, 506–516. [Google Scholar] [CrossRef]
- Griggs, G. Spending the Primary Physical Education and Sport Premium: A West Midlands case study. Educ. 3-13 2016, 44, 547–555. [Google Scholar] [CrossRef]
- Logan, S.W.; Robinson, L.E.; Wilson, A.E.; Lucas, W.A. Getting the fundamentals of movement: A meta-analysis of the effectiveness of motor skill interventions in children. Child. Care. Health Dev. 2012, 38, 305–315. [Google Scholar] [CrossRef]
- Foweather, L.; Rudd, J.R. Fundamental Movement Skills Interventions. In The Routledge Handbook of Youth Physical Activity; Brusseau, T.A., Faiclough, S.J., Lubans, D.R., Eds.; Routledge: New York, NY, USA, 2020; pp. 715–737. [Google Scholar]
- Adams, D.L. Develop Better Motor Skill Progressions with Gentile’s Taxonomy of Tasks. J. Phys. Educ. Recreat. Danc. 1999, 70, 35–38. [Google Scholar] [CrossRef]
- Guadagnoll, M.A.; Lee, T.D. Challenge Point: A Framework for Conceptualizing the Effects of Various Practice Conditions in Motor Learning. J. Mot. Behav. 2004, 36, 212–224. [Google Scholar] [CrossRef] [PubMed]
- STEP Academy Trust Physical Education Policy, 2015. Physical Education Policy–STEP Academy Trust. Available online: https://www.stepacademytrust.org/wp-content/uploads/2015/11/STEP-Physical-Education-Policy.pdf (accessed on 5 October 2020).
- English Indices of Deprivation; Ministry of Housing, Communities & Local Government: London, UK, 2018.
- Dettwyler, K.A. Anthropometric standardization reference manual, abridged edition. Edited by Timothy G. Lohman, Alex F. Roche, and Reynaldo Martoll. Champaign, Illinois: Human Kinetic Books. 1991. 90 pp. $16.00 (paper). Am. J. Phys. Anthropol. 1993, 92, 239–241. [Google Scholar] [CrossRef]
- Hinckson, E.A.; Curtis, A. Measuring physical activity in children and youth living with intellectual disabilities: A systematic review. Res. Dev. Disabil. 2013, 34, 72–86. [Google Scholar] [CrossRef] [PubMed]
- Van Kann, D.H.H.; Kremers, S.P.J.; de Vries, N.K.; de Vries, S.I.; Jansen, M.W.J. The effect of a school-centered multicomponent intervention on daily physical activity and sedentary behavior in primary school children: The Active Living study. Prev. Med. 2016, 89, 64–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strutz, E.; Browning, R.; Smith, S.; Lohse, B.; Cunningham-Sabo, L. Accelerometry-derived physical activity correlations between parents and their fourth-grade child are specific to time of day and activity level. J. Phys. Act. Health 2018, 15, 440–447. [Google Scholar] [CrossRef] [Green Version]
- Van Hees, V.T. Raw Accelerometer Data Analysis [R Package GGIR Version 2.1-0], 2020. CRAN. Available online: https://cran.r-project.org/web/packages/GGIR/GGIR.pdf (accessed on 16 November 2020).
- Montoye, A.H.K.; Moore, R.W.; Bowles, H.R.; Korycinski, R.; Pfeiffer, K.A. Reporting accelerometer methods in physical activity intervention studies: A systematic review and recommendations for authors. Br. J. Sports Med. 2018, 52, 1507–1516. [Google Scholar] [CrossRef]
- Met Office Hadley Centre HadUKP Data Download. Available online: https://www.metoffice.gov.uk/hadobs/hadukp/data/download.html (accessed on 27 November 2020).
- Timeanddate.com. Available online: https://www.timeanddate.com/ (accessed on 27 November 2020).
- Fairclough, S.J.; Rowlands, A.V.; Taylor, S.; Boddy, L.M. Cut-point-free accelerometer metrics to assess children’s physical activity: An example using the school day. Scand. J. Med. Sci. Sports 2020, 30, 117–125. [Google Scholar] [CrossRef]
- Rowlands, A.V.; Dawkins, N.P.; Maylor, B.; Edwardson, C.L.; Fairclough, S.J.; Davies, M.J.; Harrington, D.M.; Khunti, K.; Yates, T. Enhancing the value of accelerometer-assessed physical activity: Meaningful visual comparisons of data-driven translational accelerometer metrics. Sport. Med. Open 2019, 5. [Google Scholar] [CrossRef] [Green Version]
- Crotti, M.; Foweather, L.; Rudd, J.R.; Hurter, L.; Schwarz, S.; Boddy, L.M. Development of raw acceleration cut-points for wrist and hip accelerometers to assess sedentary behaviour and physical activity in 5–7-year-old children. J. Sports Sci. 2020, 38, 1036–1045. [Google Scholar] [CrossRef]
- Fairclough, S.J.; Taylor, S.; Rowlands, A.V.; Boddy, L.M.; Noonan, R.J. Average acceleration and intensity gradient of primary school children and associations with indicators of health and well-being. J. Sports Sci. 2019, 37, 2159–2167. [Google Scholar] [CrossRef] [PubMed]
- Active Lives Children and Young People Survey, 2019. Active Lives Children Survey Academic Year 2018-19. Available online: https://sportengland-production-files.s3.eu-west-2.amazonaws.com/s3fs-public/active-lives-children-survey-academic-year-18-19.pdf (accessed on 16 November 2020).
- Childhood Obesity: A Plan for Action—GOV.UK. Available online: https://www.gov.uk/government/publications/childhood-obesity-a-plan-for-action/childhood-obesity-a-plan-for-action (accessed on 16 November 2020).
- Cooper, A.R.; Goodman, A.; Page, A.S.; Sherar, L.B.; Esliger, D.W.; van Sluijs, E.M.F.; Andersen, L.B.; Anderssen, S.; Cardon, G.; Davey, R.; et al. Objectively measured physical activity and sedentary time in youth: The International children’s accelerometry database (ICAD). Int. J. Behav. Nutr. Phys. Act. 2015, 12, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, W.H.; Fredriksen, P.M. Objectively assessed moderate-to-vigorous physical activity levels among primary school children in Norway: The Health Oriented Pedagogical Project (HOPP). Scand. J. Public Health 2018, 46, 38–47. [Google Scholar] [CrossRef] [PubMed]
- McLellan, G.; Arthur, R.; Donnelly, S.; Buchan, D.S. Segmented sedentary time and physical activity patterns throughout the week from wrist-worn ActiGraph GT3X+ accelerometers among children 7–12 years old. J. Sport Health Sci. 2020, 9, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Owen, C.G.; Nightingale, C.M.; Rudnicka, A.R.; Sattar, N.; Cook, D.G.; Ekelund, U.; Whincup, P.H. Physical activity, obesity and cardiometabolic risk factors in 9- to 10-year-old UK children of white European, South Asian and black African-Caribbean origin: The Child Heart and health Study in England (CHASE). Diabetologia 2010, 53, 1620–1630. [Google Scholar] [CrossRef] [Green Version]
- Ridgers, N.D.; Stratton, G.; Fairclough, S.J. Assessing physical activity during recess using accelerometry. Prev. Med. 2005, 41, 102–107. [Google Scholar] [CrossRef]
- Herrmann, S.D.; Barreira, T.V.; Kang, M.; Ainsworth, B.E. Impact of accelerometer wear time on physical activity data: A NHANES semisimulation data approach. Br. J. Sports Med. 2014, 48, 278–282. [Google Scholar] [CrossRef]
- Harrison, F.; Goodman, A.; van Sluijs, E.M.F.; Andersen, L.B.; Cardon, G.; Davey, R.; Janz, K.F.; Kriemler, S.; Molloy, L.; Page, A.S.; et al. Weather and children’s physical activity; How and why do relationships vary between countries? Int. J. Behav. Nutr. Phys. Act. 2017, 14, 74. [Google Scholar] [CrossRef] [Green Version]
- Goodman, A.; Paskins, J.; MacKett, R. Day length and weather effects on children’s physical activity and participation in play, sports, and active travel. J. Phys. Act. Health 2012, 9, 1105–1116. [Google Scholar] [CrossRef] [Green Version]
- Thabane, L.; Mbuagbaw, L.; Zhang, S.; Samaan, Z.; Marcucci, M.; Ye, C.; Thabane, M.; Giangregorio, L.; Dennis, B.; Kosa, D.; et al. A tutorial on sensitivity analyses in clinical trials: The what, why, when and how. BMC Med. Res. Methodol. 2013, 13, 92. [Google Scholar] [CrossRef] [Green Version]
- Jakobsen, J.C.; Gluud, C.; Wetterslev, J.; Winkel, P. When and how should multiple imputation be used for handling missing data in randomised clinical trials—A practical guide with flowcharts. BMC Med. Res. Methodol. 2017, 17, 162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Package ‘mice’. Available online: https://cran.r-project.org/web/packages/mice/mice.pdf (accessed on 16 November 2020).
- Van Buuren, S. Flexible Imputation of Missing Data, 2nd ed.; Chapman and Hall/CRC: Boca Raton, FL, USA, 2018. [Google Scholar]
- Rubin, D. Multiple Imputation for Nonresponse in Surveys; John Wiley & Sons: Hoboken, NJ, USA, 2004. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistic Notes: Regression towards the mean. BMJ 1994, 308, 1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grund, S.; Lüdtke, O.; Robitzsch, A. Multiple Imputation of Missing Data for Multilevel Models. Organ. Res. Methods 2018, 21, 111–149. [Google Scholar] [CrossRef]
- Warren, J.M.; Ekelund, U.; Besson, H.; Mezzani, A.; Geladas, N.; Vanhees, L. Experts Panel Assessment of physical activity—A review of methodologies with reference to epidemiological research: A report of the exercise physiology section of the European Association of Cardiovascular Prevention and Rehabilitation. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 127–139. [Google Scholar] [CrossRef]
- Lahti, A.; Rosengren, B.E.; Nilsson, J.Å.; Karlsson, C.; Karlsson, M.K. Long-term effects of daily physical education throughout compulsory school on duration of physical activity in young adulthood: An 11-year prospective controlled study. BMJ Open Sport Exerc. Med. 2018, 4, e000360. [Google Scholar] [CrossRef]
- Beets, M.W.; Okely, A.; Weaver, R.G.; Webster, C.; Lubans, D.; Brusseau, T.; Carson, R.; Cliff, D.P. The theory of expanded, extended, and enhanced opportunities for youth physical activity promotion. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Brown, H.E.; Atkin, A.J.; Panter, J.; Wong, G.; Chinapaw, M.J.M.; van Sluijs, E.M.F. Family-based interventions to increase physical activity in children: A systematic review, meta-analysis and realist synthesis. Obes. Rev. 2016, 17, 345–360. [Google Scholar] [CrossRef] [Green Version]
- Noonan, R.J.; Boddy, L.M.; Knowles, Z.R.; Fairclough, S.J. Cross-sectional associations between high-deprivation home and neighbourhood environments, and health-related variables among Liverpool children. BMJ Open 2016, 6, e008693. [Google Scholar] [CrossRef] [Green Version]
- Huberty, J.; Dinkel, D.; Coleman, J.; Beighle, A.; Apenteng, B. The role of schools in children’s physical activity participation: Staff perceptions. Health Educ. Res. 2012, 27, 986–995. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Wen, L.M.; Rissel, C. Associations of parental influences with physical activity and screen time among young children: A systematic review. J. Obes. 2015, 2015. [Google Scholar] [CrossRef] [Green Version]
- Clennin, M.N.; Lian, M.; Colabianchi, N.; Kaczynski, A.; Dowda, M.; Pate, R.R. Associations among Neighborhood Socioeconomic Deprivation, Physical Activity Facilities, and Physical Activity in Youth during the Transition from Childhood to Adolescence. Int. J. Environ. Res. Public Health 2019, 16, 3703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooke, H.L.; Corder, K.; Atkin, A.J.; van Sluijs, E.M.F. A Systematic Literature Review with Meta-Analyses of Within- and Between-Day Differences in Objectively Measured Physical Activity in School-Aged Children. Sport. Med. 2014, 44, 1427–1438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castelli, D.M.; Centeio, E.E.; Beighle, A.E.; Carson, R.L.; Nicksic, H.M. Physical literacy and Comprehensive School Physical Activity Programs. Prev. Med. 2014, 66, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Daly-Smith, A.; Quarmby, T.; Archbold, V.S.J.; Corrigan, N.; Wilson, D.; Resaland, G.K.; Bartholomew, J.B.; Singh, A.; Tjomsland, H.E.; Sherar, L.B.; et al. Using a multi-stakeholder experience-based design process to co-develop the Creating Active Schools Framework. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandelanotte, C.; Short, C.E.; Plotnikoff, R.C.; Rebar, A.; Alley, S.; Schoeppe, S.; Canoy, D.F.; Hooker, C.; Power, D.; Oldmeadow, C.; et al. Are web-based personallytailored physical activity videos more effective than personally tailored text-based interventions? Results from the three-arm randomised controlled TaylorActive trial. Br. J. Sports Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Riiser, K.; Richardsen, K.R.; Haugen, A.L.H.; Lund, S.; Løndal, K. Active play in ASP-a matched-pair cluster-randomized trial investigating the effectiveness of an intervention in after-school programs for supporting children’s physical activity. BMC Public Health 2020, 20. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Linear Pedagogy (n = 105) | Nonlinear Pedagogy (n = 112) | Control (n = 143) | ||||
|---|---|---|---|---|---|---|
| Baseline Characteristic | Mean (SD) or % | Missing Data | Mean (SD) or % | Missing Data | Mean (SD) or % | Missing Data |
| Decimal Age (years) | 6.0 (0.3) | 5 | 5.9 (0.3) | 1 | 5.9 (0.3) | 2 |
| Females | 53% | 0 | 52% | 0 | 58% | 0 |
| White British | 68% | 8 | 52% | 9 | 50% | 5 |
| SEN | 8% | 1 | 15% | 1 | 12% | 0 |
| Living within the 30% most deprived areas (IMD) | 96% | 4 | 77% | 1 | 89% | 3 |
| IOTF SDS BMI | 0.4 (1.3) | 9 | 0.5 (1.1) | 8 | 0.3 (1.1) | 27 |
| Thinness grade 3 | 1% | 0% | 1% | |||
| Thinness grade 2 | 2% | 1% | 0% | |||
| Thinness grade 1 | 6% | 4% | 6% | |||
| Healthy weight | 61% | 67% | 67% | |||
| Overweight | 21% | 72% | 22% | |||
| Obese | 8% | 9% | 4% | |||
| Meeting PA guidelines | ||||||
| Whole week | 68% | 18 | 64% | 32 | 62% | 48 |
| Weekdays | 70% | 18 | 71% | 32 | 72% | 48 |
| Weekend | 53% | 18 | 48% | 32 | 53% | 48 |
| Category | Global | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Category Mean (SD) | Global Mean (SD) | ||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 1 | 2 | |
| Nonlinear | 5.00 (0.00) | 5.00 (0.00) | 4.90 (0.28) | 3.95 (0.78) | 4.05 (0.77) | 4.73 (0.41) | 4.58 (0.43) | 5.00 (0.00) | 5.00 (0.00) |
| Linear | 1.40 (0.64) | 1.48 (0.85) | 1.20 (0.41) | 1.77 (0.94) | 1.20 (0.41) | 1.63 (0.88) | 1.63 (0.75) | 10.40 (0.74) | 1.33 (0.82) |
| Control | 2.10 (0.83) | 2.15 (1.04) | 2.19 (0.88) | 1.44 (0.97) | 2.33 (0.87) | 2.21 (0.75) | 2.50 (0.54) | 2.00 (1.08) | 1.92 (1.11) |
| MVPA | Mean ENMO | M60 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Predictors | β | SE | p | β | SE | p | β | SE | p |
| WHOLE WEEK PA | |||||||||
| Intention to treat analysis | |||||||||
| Group [NLP] * Time [T1] | −2.62 | 3.17 | 0.414 | −1.881 | 2.652 | 0.483 | −1.805 | 10.466 | 0.864 |
| Group [NLP] * Time [T2] | 1.566 | 3.75 | 0.680 | 0.402 | 2.448 | 0.870 | 3.156 | 11.981 | 0.794 |
| Group [LP] * Time [T1] | −0.637 | 4.04 | 0.876 | −0.936 | 2.85 | 0.743 | −0.071 | 14.383 | 0.996 |
| Group [LP] * Time [T2] | −2.073 | 3.33 | 0.538 | −2.204 | 2.539 | 0.390 | −1.692 | 11.085 | 0.879 |
| Complete case analysis | |||||||||
| Group [NLP] * Time [T1] | −2.02 | 3.71 | 0.587 | −0.32 | 2.90 | 0.913 | 0.28 | 14.03 | 0.984 |
| Group [NLP] * Time [T2] | 5.73 | 4.35 | 0.188 | 4.52 | 3.40 | 0.183 | 3.12 | 16.44 | 0.849 |
| Group [LP] * Time [T1] | −1.63 | 4.94 | 0.742 | −1.65 | 3.86 | 0.668 | −6.98 | 18.67 | 0.708 |
| Group [LP] * Time [T2] | −1.22 | 4.04 | 0.762 | −0.80 | 3.16 | 0.799 | −10.63 | 15.28 | 0.487 |
| WEEKEND PA | |||||||||
| Intention to treat analysis | |||||||||
| Group [NLP] * Time [T1] | −2.50 | 4.68 | 0.595 | −0.75 | 4.26 | 0.861 | 7.55 | 14.69 | 0.608 |
| Group [NLP] * Time [T2] | 1.67 | 5.39 | 0.758 | 2.74 | 4.16 | 0.515 | 7.61 | 14.86 | 0.610 |
| Group [LP] * Time [T1] | 0.64 | 4.88 | 0.897 | −0.81 | 4.02 | 0.841 | 4.76 | 18.96 | 0.803 |
| Group [LP] * Time [T2] | −3.91 | 4.87 | 0.426 | −1.74 | 4.18 | 0.680 | −13.69 | 14.70 | 0.355 |
| Complete case analysis | |||||||||
| Group [NLP] * Time [T1] | −1.18 | 5.86 | 0.841 | 1.97 | 4.44 | 0.656 | 19.29 | 23.17 | 0.405 |
| Group [NLP] * Time [T2] | 9.41 | 6.57 | 0.152 | 8.71 | 4.97 | 0.080 | 33.42 | 25.96 | 0.198 |
| Group [LP] * Time [T1] | 0.88 | 7.40 | 0.905 | −0.28 | 5.60 | 0.959 | 12.70 | 29.26 | 0.664 |
| Group [LP] * Time [T2] | −0.88 | 5.87 | 0.881 | −0.91 | 4.44 | 0.838 | −2.41 | 23.19 | 0.917 |
| MVPA | Mean ENMO | M30 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Predictors | β | SE | p | β | SE | p | β | SE | p |
| IN SCHOOL WEEKDAY PA | |||||||||
| Intention to treat analysis | |||||||||
| Group [NLP] * Time [T1] | −1.56 | 1.55 | 0.318 | −3.29 | 3.57 | 0.358 | −14.936 | 13.151 | 0.257 |
| Group [NLP] * Time [T2] | 2.23 | 1.57 | 0.162 | 1.45 | 5.19 | 0.783 | −3.185 | 15.374 | 0.837 |
| Group [LP] * Time [T1] | 0.81 | 2.27 | 0.724 | 0.71 | 5.02 | 0.887 | −5.437 | 18.36 | 0.768 |
| Group [LP] * Time [T2] | 0.39 | 1.48 | 0.792 | 2.62 | 3.72 | 0.482 | 2.341 | 14.128 | 0.869 |
| Complete case analysis | |||||||||
| Group [NLP] * Time [T1] | 0.16 | 1.78 | 0.930 | −0.86 | 4.61 | 0.852 | −14.68 | 20.57 | 0.475 |
| Group [NLP] * Time [T2] | 5.18 | 2.11 | 0.014 | 7.42 | 5.46 | 0.174 | −25.53 | 24.34 | 0.294 |
| Group [LP] * Time [T1] | 1.98 | 2.56 | 0.439 | 1.33 | 6.64 | 0.841 | −4.73 | 29.59 | 0.873 |
| Group [LP] * Time [T2] | 2.34 | 2.01 | 0.244 | 5.08 | 5.20 | 0.329 | −6.74 | 23.19 | 0.771 |
| OUTSIDE SCHOOL WEEKDAY PA | |||||||||
| Intention to treat analysis | |||||||||
| Group [NLP] * Time [T1] | −2.09 | 2.11 | 0.326 | −1.58 | 3.20 | 0.623 | 3.24 | 13.46 | 0.811 |
| Group [NLP] * Time [T2] | −0.28 | 2.27 | 0.902 | 0.49 | 3.83 | 0.899 | 10.71 | 13.04 | 0.413 |
| Group [LP] * Time [T1] | −4.17 | 2.69 | 0.126 | −5.84 | 4.78 | 0.228 | −15.90 | 16.16 | 0.327 |
| Group [LP] * Time [T2] | −3.89 | 2.19 | 0.079 | −4.30 | 3.73 | 0.253 | 0.11 | 12.67 | 0.993 |
| Complete case analysis | |||||||||
| Group [NLP] * Time [T1] | −2.61 | 2.64 | 0.323 | −3.37 | 4.19 | 0.421 | −4.48 | 17.59 | 0.799 |
| Group [NLP] * Time [T2] | 0.61 | 3.07 | 0.844 | 0.52 | 4.87 | 0.916 | 6.64 | 20.43 | 0.745 |
| Group [LP] * Time [T1] | −7.74 | 3.71 | 0.037 | −12.24 | 5.89 | 0.038 | −48.03 | 24.70 | 0.052 |
| Group [LP] * Time [T2] | −4.41 | 2.94 | 0.134 | −7.44 | 4.66 | 0.111 | −23.25 | 19.58 | 0.235 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crotti, M.; Rudd, J.R.; Roberts, S.; Boddy, L.M.; Fitton Davies, K.; O’Callaghan, L.; Utesch, T.; Foweather, L. Effect of Linear and Nonlinear Pedagogy Physical Education Interventions on Children’s Physical Activity: A Cluster Randomized Controlled Trial (SAMPLE-PE). Children 2021, 8, 49. https://doi.org/10.3390/children8010049
Crotti M, Rudd JR, Roberts S, Boddy LM, Fitton Davies K, O’Callaghan L, Utesch T, Foweather L. Effect of Linear and Nonlinear Pedagogy Physical Education Interventions on Children’s Physical Activity: A Cluster Randomized Controlled Trial (SAMPLE-PE). Children. 2021; 8(1):49. https://doi.org/10.3390/children8010049
Chicago/Turabian StyleCrotti, Matteo, James R. Rudd, Simon Roberts, Lynne M. Boddy, Katie Fitton Davies, Laura O’Callaghan, Till Utesch, and Lawrence Foweather. 2021. "Effect of Linear and Nonlinear Pedagogy Physical Education Interventions on Children’s Physical Activity: A Cluster Randomized Controlled Trial (SAMPLE-PE)" Children 8, no. 1: 49. https://doi.org/10.3390/children8010049