Early Intervention with Parents of Children with Autism Spectrum Disorders: A Review of Programs



Abstract
:1. Introduction
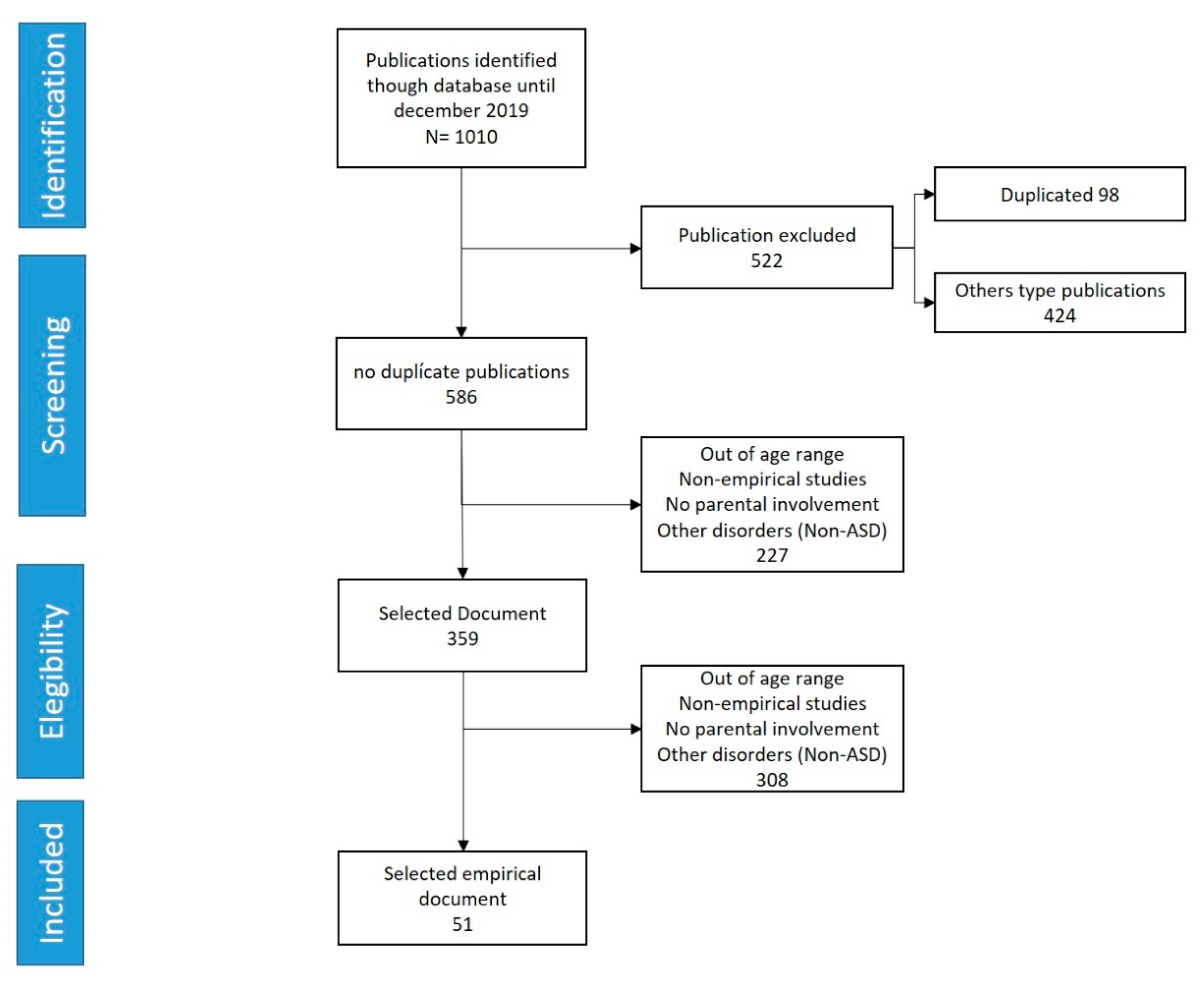
2. Method
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Quality Assessment
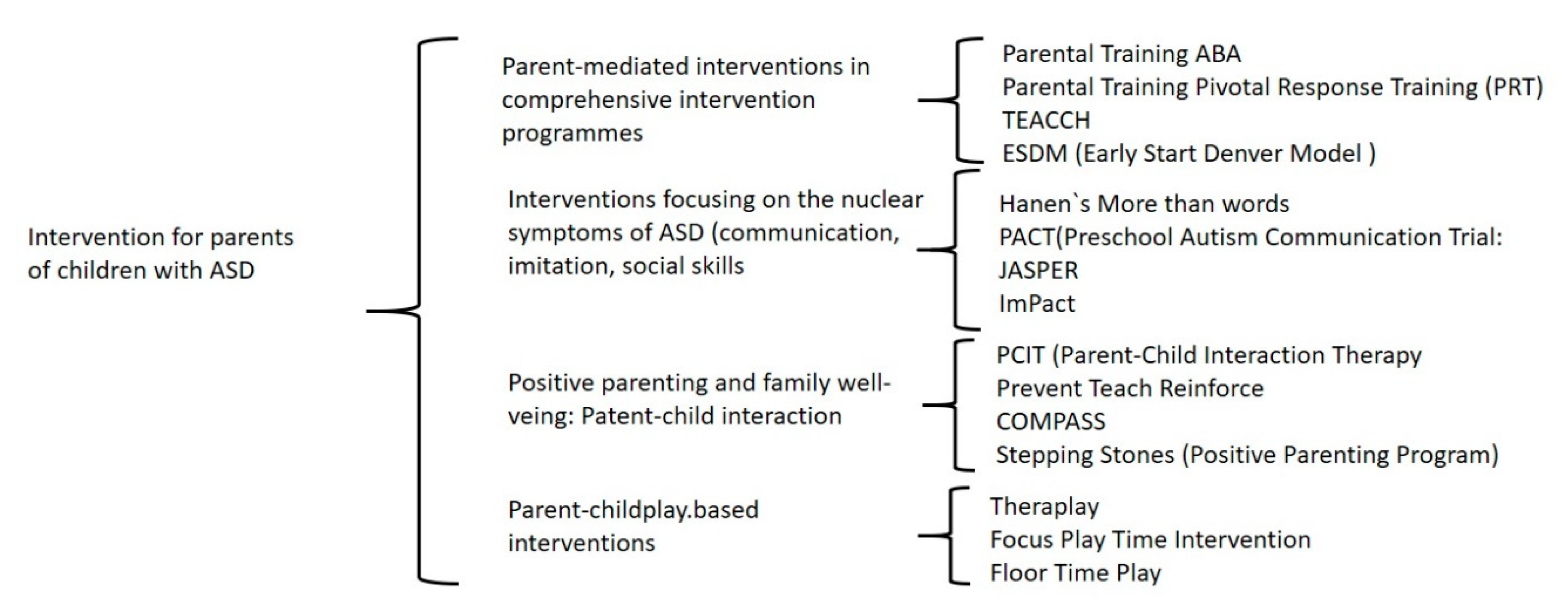
3. Results
3.1. Parent-Mediated Intervention in Comprehensive Intervention Programs
3.1.1. Parental Training (PT)
3.1.2. Pivotal Response Training (PRT)
3.1.3. Treatment and Education of Autistic and Related Communication-Handicapped Children (TEACCH)
3.1.4. Early Start Denver Model (ESDM)
3.2. Parent-Mediated Programs Focused on ASD Symptoms
3.2.1. Hanen More Than Words
3.2.2. Preschool Autism Communication Trial (PACT)
3.2.3. Joint Attention Symbolic Play, Engagement, and Regulation (JASPER)
3.2.4. Improving Parents as Communication Teachers (ImPact)
3.3. Programs for the Promotion of Positive Parenthood and Family Well-Being
3.3.1. Parent–Child Interaction Therapy (PCIT)
3.3.2. Prevent–Teach–Reinforce (PTR)
3.3.3. Collaborative Model for Promoting Competence and Success (COMPASS)
3.3.4. Stepping Stones Triple P (SSTP)
3.4. Play-Focused Intervention Programs
3.4.1. Theraplay
3.4.2. Floortime Play
3.4.3. Focus Playtime Intervention (FPI)
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Falk, N.H.; Norris, K.; Quinn, M.G. The Factors Predicting Stress, Anxiety and Depression in the Parents of Children with Autism. J. Autism Dev. Disord. 2014, 44, 3185–3203. [Google Scholar] [CrossRef] [Green Version]
- Firth, I.; Dryer, R. The predictors of distress in parents of children with autism spectrum disorder. J. Intellect. Dev. Disabil. 2013, 38, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Merkaj, V.; Kika, M.; Simaku, A. Symptoms of Stress, Depression and Anxiety between Parents of Autistic Children and Parents of Tipically Developing Children. Acad. J. Interdiscip. Stud. 2013, 2, 345–3352. [Google Scholar] [CrossRef]
- Almansour, M.A.; AlAteeq, M.A.; Alzahrani, M.K.; Algeffari, M.A.; Alhomaidan, H.T. Depression and anxiety among parents and caregivers of autistic spectral disorder children. Neuroscience 2013, 18, 58–63. [Google Scholar]
- Hayes, S.A.; Watson, S.L. The Impact of Parenting Stress: A Meta-analysis of Studies Comparing the Experience of Parenting Stress in Parents of Children with and Without Autism Spectrum Disorder. J. Autism Dev. Disord. 2013, 43, 629–642. [Google Scholar] [CrossRef] [PubMed]
- Federación Estatal de Asociaciones de Profesionales de Atención Temprana (GAT). Libro Blanco de Atención Temprana [Early Care White Paper]; Federación Estatal de Asociaciones de Profesionales de Atención Temprana Real Patronato sobre Discapacidad: Madrid, Spain, 2000. [Google Scholar]
- Giné, C.; Gràcia, M.; Vilaseca, R.; Balcells, A. Trabajar con las familias en atención temprana, [Working with families in early care]. Rev. Interuniv. Form.Profr. 2009, 23, 95–113. [Google Scholar]
- Giné, C.; Gràcia, M.; Vilaseca, R.; García-Díe, M.T. Repensar la atención temprana: Propuestas para un desarrollo futuro. Infanc. Aprendiz. 2006, 29, 297–313. [Google Scholar] [CrossRef]
- Hamilton, L.M. Facing Autism: Giving Parents Reasons for Hope and Guidance for Help; Random House Digital, Inc.: New York, NY, USA, 2009. [Google Scholar]
- Whitaker, P. Supporting Families of Preschool Children with Autism. Autism 2002, 6, 411–426. [Google Scholar] [CrossRef]
- Botana, I.; Peralbo, M. Familia, estrés y atención temprana. Family, stress and early care attention. Rev. Estud. Investig. Psicol. Educ. 2014, 1, 55. [Google Scholar] [CrossRef] [Green Version]
- Koizumi, H. The concept of ‘developing the brain’: A new natural science for learning and education. Brain Dev. 2004, 26, 434–441. [Google Scholar] [CrossRef]
- Perpiñán, S. Atención Temprana y Familia [Early Care and Family]; Narcea: Madrid, Spain, 2009. [Google Scholar]
- Pons-Salvador, G.; Cerezo, M.A.; Bernabé, G. Cambio y estabilidad en los factores que afectan negativamente a la parentalidad, [Change and stability in factors negatively affecting parenting]. Psicothema 2005, 17, 31–36. [Google Scholar]
- Osborne, L.A.; McHugh, L.; Saunders, J.; Reed, P. Parenting Stress Reduces the Effectiveness of Early Teaching Interventions for Autistic Spectrum Disorders. J. Autism Dev. Disord. 2008, 38, 1092–1103. [Google Scholar] [CrossRef] [PubMed]
- Palomo, R. Autismo: Teorías Explicativas Actuales [Autism: Current Explanatory Theories]; Alianza Editorial: Madrid, Spain, 2017. [Google Scholar]
- Rogers, S.J.; Pennington, B.F. A theoretical approach to the deficits in infantile autism. Dev. Psychopathol. 1991, 3, 137–162. [Google Scholar] [CrossRef]
- Thomas, M.S.; Annaz, D.; Ansari, D.; Scerif, G.; Jarrold, C.; Karmiloff-Smith, A.; Dimitriou, D. Using Developmental Trajectories to Understand Developmental Disorders. J. Speech Lang. Hear. Res. 2009, 52, 336–358. [Google Scholar] [CrossRef] [Green Version]
- Baker, J.K.; Messinger, D.S.; Lyons, K.K.; Grantz, C.J. A Pilot Study of Maternal Sensitivity in the Context of Emergent Autism. J. Autism Dev. Disord. 2010, 40, 988–999. [Google Scholar] [CrossRef] [Green Version]
- Osborne, L.A.; Reed, P. Stress and self-perceived parenting behaviors of parents of children with autistic spectrum conditions. Res. Autism Spectr. Disord. 2010, 4, 405–414. [Google Scholar] [CrossRef]
- Mundy, P.; Crowson, M. Joint Attention and Early Social Communication: Implications for Research on Intervention with Autism. J. Autism Dev. Disord. 1997, 27, 653–676. [Google Scholar] [CrossRef]
- Pierce, K.; Courchesne, E.; Bacon, E.C. To Screen or Not to Screen Universally for Autism is not the Question: Why the Task Force Got It Wrong. J. Pediatr. 2016, 176, 182–194. [Google Scholar] [CrossRef] [Green Version]
- Crowell, J.A.; Keluskar, J.; Gorecki, A. Parenting behavior and the development of children with autism spectrum disorder. Compr. Psychiatry 2019, 90, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Green, J.; Pickles, A.; Pasco, G.; Bedford, R.; Wan, M.W.; Elsabbagh, M.; Slonims, V.; Gliga, T.; Jones, E.J.H.; Cheung, C.; et al. Randomised trial of a parent-mediated intervention for infants at high risk for autism: Longitudinal outcomes to age 3 years. J. Child Psychol. Psychiatry 2017, 58, 1330–1340. [Google Scholar] [CrossRef]
- Kim, S.H.; Bal, V.H.; Lord, C. Longitudinal follow-up of academic achievement in children with autism from age 2 to 18. J. Child Psychol. Psychiatry 2017, 59, 258–267. [Google Scholar] [CrossRef] [PubMed]
- McConachie, H.; Diggle, T. Parent implemented early intervention for young children with autism spectrum disorder: A systematic review. J. Eval. Clin. Pr. 2007, 13, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Oono, I.P.; Honey, E.J.; McConachie, H. Parent-mediated early intervention for young children with autism spectrum disorders (ASD). Cochrane Db. Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed]
- Bearss, K.; Burrell, T.L.; Stewart, L.M.; Scahill, L. Parent Training in Autism Spectrum Disorder: What’s in a Name? Clin. Child Fam. Psychol. Rev. 2015, 18, 170–182. [Google Scholar] [CrossRef] [PubMed]
- Siller, M.; Morgan, L. Handbook of Parent-Implemented Interventions for Very Young Children with Autism; Springer: Cham, Switzerland, 2018. [Google Scholar] [CrossRef]
- Diggle, T.T.J.; McConachie, H.H.R. Parent-mediated early intervention for young children with autism spectrum disorder. Cochrane Db. Syst. Rev 2002. [Google Scholar] [CrossRef]
- Diggle, T.T.J.; McConachie, H. Parent-mediated early intervention for young children with autism spectrum disorder. Cochrane Db. Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Torres, L.R.; Esteban, Y.A.; Alcantud-Marín, F. Revisión de evidencias de las técnicas de DIR/Floortime™ para la intervención en niños y niñas con Trastornos del Espectro del Autismo. Siglo Cero 2020, 51, 7–32. [Google Scholar] [CrossRef]
- Morgan, G.A.; Gliner, J.A.; Harmon, R.J. Quasi-Experimental Designs. J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 794–796. [Google Scholar] [CrossRef] [Green Version]
- Horner, R.H.; Carr, E.G.; Halle, J.W.; McGee, G.G.; Odom, S.L.; Wolery, M. The Use of Single-Subject Research to Identify Evidence-Based Practice in Special Education. Except. Child. 2005, 71, 165–179. [Google Scholar] [CrossRef]
- Oosterling, I.; Visser, J.; Swinkels, S.H.N.; Rommelse, N.N.J.; Donders, R.; Woudenberg, T.; Roos, S.; Van Der Gaag, R.J.; Buitelaar, J.K. Randomized Controlled Trial of the Focus Parent Training for Toddlers with Autism: 1-Year Outcome. J. Autism Dev. Disord. 2010, 40, 1447–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bearss, K.; Johnson, C.; Handen, B.; Smith, T.; Scahill, L. A Pilot Study of Parent Training in Young Children with Autism Spectrum Disorders and Disruptive Behavior. J. Autism Dev. Disord. 2012, 43, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Bagaiolo, L.F.; Mari, J.D.J.; Bordini, D.; Ribeiro, T.C.; Martone, M.C.C.; Caetano, S.C.; Brunoni, D.; Brentani, H.; Paula, C.S. Procedures and compliance of a video modeling applied behavior analysis intervention for Brazilian parents of children with autism spectrum disorders. Autism 2017, 21, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Wacker, D.; Lee, J.F.; Dalmau, Y.C.P.; Kopelman, T.G.; Lindgren, S.D.; Kuhle, J.; Pelzel, K.E.; Waldron, D.B. Conducting Functional Analyses of Problem Behavior Via Telehealth. J. Appl. Behav. Anal. 2013, 46, 31–46. [Google Scholar] [CrossRef] [Green Version]
- Blackman, A.L.; Jimenez-Gomez, C.; Shvarts, S. Comparison of the efficacy of online versus in-vivo behavior analytic training for parents of children with autism spectrum disorder. Behav. Anal. Res. Pr. 2020, 20, 13–23. [Google Scholar] [CrossRef]
- Iadarola, S.; Levato, L.; Harrison, B.; Smith, T.; Lecavalier, L.; Johnson, C.; Swiezy, N.; Bearss, K.; Scahill, L. Teaching Parents Behavioral Strategies for Autism Spectrum Disorder (ASD): Effects on Stress, Strain, and Competence. J. Autism Dev. Disord. 2018, 48, 1031–1040. [Google Scholar] [CrossRef]
- Minjarez, M.B.; Williams, S.E.; Mercier, E.; Hardan, A.Y. Pivotal Response Group Treatment Program for Parents of Children with Autism. J. Autism Dev. Disord. 2010, 41, 92–101. [Google Scholar] [CrossRef]
- Gengoux, G.W.; Berquist, K.L.; Salzman, E.; Schapp, S.; Phillips, J.M.; Frazier, T.W.; Minjarez, M.B.; Hardan, A.Y. Pivotal Response Treatment Parent Training for Autism: Findings from a 3-Month Follow-Up Evaluation. J. Autism Dev. Disord. 2015, 45, 2889–2898. [Google Scholar] [CrossRef]
- Hardan, A.Y.; Gengoux, G.W.; Berquist, K.L.; Libove, R.A.; Ardel, C.M.; Phillips, J.; Frazier, T.W.; Minjarez, M.B. A randomized controlled trial of Pivotal Response Treatment Group for parents of children with autism. J. Child Psychol. Psychiatry 2015, 56, 884–892. [Google Scholar] [CrossRef]
- Bradshaw, J.; Koegel, L.K.; Koegel, R.L. Improving Functional Language and Social Motivation with a Parent-Mediated Intervention for Toddlers with Autism Spectrum Disorder. J. Autism Dev. Disord. 2017, 47, 2443–2458. [Google Scholar] [CrossRef]
- D’Elia, L.; Valeri, G.; Sonnino, F.; Fontana, I.; Mammone, A.; Vicari, S. A Longitudinal Study of the Teacch Program in Different Settings: The Potential Benefits of Low Intensity Intervention in Preschool Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2014, 44, 615–626. [Google Scholar] [CrossRef] [PubMed]
- Howlin, P. Early Start Denver Model for Young Children with Autism: Promoting Language, Learning, and Engagement; Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Rogers, S.J.; Vismara, L.A.; Wagner, A.L.; McCormick, C.; Young, G.; Ozonoff, S. Autism Treatment in the First Year of Life: A Pilot Study of Infant Start, a Parent-Implemented Intervention for Symptomatic Infants. J. Autism Dev. Disord. 2014, 44, 2981–2995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vivanti, G.; Paynter, J.M.; Duncan, E.; Fothergill, H.; Dissanayake, C.; Rogers, S.J.; ASELCC Team. Effectiveness and Feasibility of the Early Start Denver Model Implemented in a Group-Based Community Childcare Setting. J. Autism Dev. Disord. 2014, 44, 3140–3153. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S.; Estes, A.; Vismara, L.; Munson, J.; Zierhut, C.; Greenson, J.; Dawson, G.; Rocha, M.; Sugar, C.; Senturk, D.; et al. Enhancing Low-Intensity Coaching in Parent Implemented Early Start Denver Model Intervention for Early Autism: A Randomized Comparison Treatment Trial. J. Autism Dev. Disord. 2019, 49, 632–646. [Google Scholar] [CrossRef]
- Waddington, H.; Van Der Meer, L.; Sigafoos, J.; Whitehouse, A. Examining parent use of specific intervention techniques during a 12-week training program based on the Early Start Denver Model. Autism 2019, 24, 484–498. [Google Scholar] [CrossRef]
- Sameroff, A.J.; Emde, R.N. Relationship Disturbances in Early Childhood: A Developmental Approach; Basic Books: New York, NY, USA, 1989. [Google Scholar]
- Green, J.; Charman, T.; McConachie, H.; Aldred, C.; Slonims, V.; Howlin, P.; Le Couteur, A.; Leadbitter, K.; Hudry, K.; Byford, S.; et al. Parent-mediated communication-focused treatment in children with autism (PACT): A randomised controlled trial. Lancet 2010, 375, 2152–2160. [Google Scholar] [CrossRef] [Green Version]
- Pickles, A.; Harris, V.; Green, J.; Aldred, C.; McConachie, H.; Slonims, V.; Le Couteur, A.; Hudry, K.; Charman, T. Treatment mechanism in the MRC preschool autism communication trial: Implications for study design and parent-focussed therapy for children. J. Child Psychol. Psychiatry 2014, 56, 162–170. [Google Scholar] [CrossRef]
- Kasari, C.; Gulsrud, A.; Paparella, T.; Hellemann, G.; Berry, K. Randomized comparative efficacy study of parent-mediated interventions for toddlers with autism. J. Consult. Clin. Psychol. 2015, 83, 554–563. [Google Scholar] [CrossRef]
- Gulsrud, A.; Hellemann, G.; Shire, S.; Kasari, C. Isolating active ingredients in a parent-mediated social communication intervention for toddlers with autism spectrum disorder. J. Child Psychol. Psychiatry 2016, 57, 606–613. [Google Scholar] [CrossRef]
- Shire, S.Y.; Gulsrud, A.; Kasari, C. Increasing Responsive Parent–Child Interactions and Joint Engagement: Comparing the Influence of Parent-Mediated Intervention and Parent Psychoeducation. J. Autism Dev. Disord. 2016, 46, 1737–1747. [Google Scholar] [CrossRef] [Green Version]
- Ingersoll, B.; Dvortcsak, A. Teaching Social Communication to Children with Autism: A Practitioner’s Guide to Parent Training; The Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Ingersoll, B.; Wainer, A.L. Initial Efficacy of Project ImPACT: A Parent-Mediated Social Communication Intervention for Young Children with ASD. J. Autism Dev. Disord. 2013, 43, 2943–2952. [Google Scholar] [CrossRef] [PubMed]
- Stadnick, N.A.; Stahmer, A.; Brookman-Frazee, L. Preliminary Effectiveness of Project ImPACT: A Parent-Mediated Intervention for Children with Autism Spectrum Disorder Delivered in a Community Program. J. Autism Dev. Disord. 2015, 45, 2092–2104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ingersoll, B.; Wainer, A.L.; Berger, N.I.; Pickard, K.E.; Bonter, N. Comparison of a Self-Directed and Therapist-Assisted Telehealth Parent-Mediated Intervention for Children with ASD: A Pilot RCT. J. Autism Dev. Disord. 2016, 46, 2275–2284. [Google Scholar] [CrossRef] [PubMed]
- Ingersoll, B.; Wainer, A.L.; Berger, N.I.; Walton, K.M. Efficacy of low intensity, therapist-implemented Project ImPACT for increasing social communication skills in young children with ASD. Dev. Neurorehabilit. 2017, 20, 502–510. [Google Scholar] [CrossRef]
- Newacheck, P.W. Health Services Use and Health Care Expenditures for Children with Disabilities. Pediatrics 2004, 114, 79–85. [Google Scholar] [CrossRef] [Green Version]
- Hansen, B.; Shillingsburg, M.A. Using a Modified Parent-Child Interaction Therapy to Increase Vocalizations in Children with Autism. Child Fam. Behav. Ther. 2016, 38, 318–330. [Google Scholar] [CrossRef]
- Masse, J.J.; McNeil, C.B.; Wagner, S.; Quetsch, L.B. Examining the Efficacy of Parent–Child Interaction Therapy with Children on the Autism Spectrum. J. Child Fam. Stud. 2016, 25, 2508–2525. [Google Scholar] [CrossRef]
- Zlomke, K.R.; Jeter, K.; Murphy, J. Open-Trial Pilot of Parent-Child Interaction Therapy for Children with Autism Spectrum Disorder. Child Fam. Behav. Ther. 2017, 39, 1–18. [Google Scholar] [CrossRef]
- Parladé, M.V.; Weinstein, A.; Garcia, D.; Rowley, A.M.; Ginn, N.C.; Jent, J.F. Parent–Child Interaction Therapy for children with autism spectrum disorder and a matched case-control sample. Autism 2019, 24, 160–176. [Google Scholar] [CrossRef]
- Dunlap, G.; Iovannone, R.; Kincaid, D.; Wilson, K.; Christiansen, K.; Strain, P.S.; English, C.; Sugai, G. Prevent-Teach-Reinforce: The School-Based Model. of Individualized Positive Behavior Support; Paul H Brookes Publishing Co.: Baltimor, MA, USA, 2019. [Google Scholar]
- Bailey, K.M.; Blair, K.-S.C. Feasibility and potential efficacy of the family-centered Prevent-Teach-Reinforce model with families of children with developmental disorders. Res. Dev. Disabil. 2015, 47, 218–233. [Google Scholar] [CrossRef]
- Ruble, L.A.; Dalrymple, N.J.; McGrew, J.H. The Effects of Consultation on Individualized Education Program Outcomes for Young Children with Autism: The Collaborative Model for Promoting Competence and Success. J. Early Interv. 2010, 32, 286–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuravackel, G.M.; Ruble, L.A.; Reese, R.J.; Ables, A.P.; Rodgers, A.D.; Toland, M.D. COMPASS for Hope: Evaluating the Effectiveness of a Parent Training and Support Program for Children with ASD. J. Autism Dev. Disord. 2017, 48, 404–416. [Google Scholar] [CrossRef] [PubMed]
- Sanders, M.R.; Mazzucchelli, T.G.; Studman, L.J. Practitioner’s Manual for Standard Stepping Stones Triple P; Triple P International Pty Ltd.: Brisbane, Australia, 2003. [Google Scholar]
- Tellegen, C.L.; Sanders, M. A randomized controlled trial evaluating a brief parenting program with children with autism spectrum disorders. J. Consult. Clin. Psychol. 2014, 82, 1193–1200. [Google Scholar] [CrossRef] [PubMed]
- Schrott, B.; Kasperzack, D.; Weber, L.; Becker, K.; Burghardt, R.; Kamp-Becker, I. Effectiveness of the Stepping Stones Triple P Group Parenting Program as an Additional Intervention in the Treatment of Autism Spectrum Disorders: Effects on Parenting Variables. J. Autism Dev. Disord. 2018, 49, 913–923. [Google Scholar] [CrossRef]
- Piaget, J. Play, Dreams and Imitation in Childhood; W. W. Norton & Co.: New York, NY, USA, 1952. [Google Scholar]
- Wieder, S.; Greenspan, S.I. Climbing the Symbolic Ladder in the DIR Model Through Floor Time/Interactive Play. Autism 2003, 7, 425–435. [Google Scholar] [CrossRef]
- Pajareya, K.; Nopmaneejumruslers, K. A pilot randomized controlled trial of DIR/Floortime™ parent training intervention for pre-school children with autistic spectrum disorders. Autism 2011, 15, 563–577. [Google Scholar] [CrossRef]
- Pajareya, K.; Nopmaneejumruslers, K. A One-Year Prospective Follow-Up Study of a DIR/Floortime™ Parent Training Intervention for Pre-School Children with Autistic Spectrum Disorders. J. Med. Assoc. Thai 2012, 1184–1193. [Google Scholar]
- Lal, R.; Chhabria, R. Early Intervention of Autism: A Case for Floor Time Approach. Recent Adv. Autism Spectr. Disord. Vol. I 2013. [Google Scholar] [CrossRef] [Green Version]
- Solomon, R.; Van Egeren, L.A.; Mahoney, G.; Huber, M.S.Q.; Zimmerman, P. PLAY Project Home Consultation Intervention Program for Young Children with Autism Spectrum Disorders. J. Dev. Behav. Pediatr. 2014, 35, 475–485. [Google Scholar] [CrossRef]
- Aali, S.; Yazdi, S.; Abdekhodaei, M.; Chamanabad, A.; Moharreri, F. Developing a mixed family-focused therapy based on intergrated human developmental model and comparing its effectiveness with Floortimme play-therapy on the developmental family function and the functional-emotional development of children with autism spectrum disorders. J. Fundam. Ment. Health 2015, 17, 87–97. [Google Scholar]
- Sealy, J.; Glovinsky, I.P. Strengthening the Reflective Functioning Capacities of Parents Who Have a Child With a Neurodevelopmental Disability Through a Brief, Relationship-Focused Intervention. Child Adolesc. Soc. Work. J. 2016, 37, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Aber, J.L.; Slade, A.; Berger, B.; Bresgi, I.; Kaplan, M. The Parent Development Interview; Barnard College Departament of Psychology: New York, NY, USA, 1985. [Google Scholar]
- Siller, M.; Swanson, M.; Gerber, A.; Hutman, T.; Sigman, M. A Parent-Mediated Intervention That Targets Responsive Parental Behaviors Increases Attachment Behaviors in Children with ASD: Results from a Randomized Clinical Trial. J. Autism Dev. Disord. 2014, 44, 1720–1732. [Google Scholar] [CrossRef] [PubMed]
- Provenzani, U.; Fusar-Poli, L.; Brondino, N.; Damiani, S.; Vercesi, M.; Meyer, N.; Rocchetti, M.; Politi, P. What are we targeting when we treat autism spectrum disorder? A systematic review of 406 clinical trials. Autism 2019, 24, 274–284. [Google Scholar] [CrossRef] [PubMed]
- Yoder, P.; Lieberman, R.G. Brief Report: Randomized test of the efficacy of picture exchange communication system on highly generalized picture exchanges in children with ASD. J. Autism Dev. Disord. 2010, 40, 629–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carr, J.E.; Severtson, J.M.; Lepper, T.L. Noncontingent reinforcement is an empirically supported treatment for problem behavior exhibited by individuals with developmental disabilities. Res. Dev. Disabil. 2009, 30, 44–57. [Google Scholar] [CrossRef] [PubMed]
- Matson, J.L.; LoVullo, S.V. A Review of Behavioral Treatments for Self-Injurious Behaviors of Persons with Autism Spectrum Disorders. Behav. Modif. 2008, 32, 61–76. [Google Scholar] [CrossRef] [PubMed]
- Chawner, L.R.; Blundell-Birtill, P.; Hetherington, M.M. Interventions for Increasing Acceptance of New Foods Among Children and Adults with Developmental Disorders: A Systematic Review. J. Autism Dev. Disord. 2019, 49, 3504–3525. [Google Scholar] [CrossRef] [Green Version]
- Patterson, G.R. Interventions for boys with conduct problems: Multiple settings, treatments, and criteria. J. Consult. Clin. Psychol. 1974, 42, 471–481. [Google Scholar] [CrossRef]
- McMahon, R.J.; Forehand, R.; Griest, D.L. Effects of knowledge of social learning principles on enhancing treatment outcome and generalization in a parent training program. J. Consult. Clin. Psychol. 1981, 49, 526–532. [Google Scholar] [CrossRef]
- Carr, E.G.; Durand, V.M. Reducing behavior problems through functional communication training. J. Appl. Behav. Anal. 1985, 18, 111–126. [Google Scholar] [CrossRef] [Green Version]
- Koegel, L.K.; Koegel, R.L.; Harrower, J.K.; Carter, C.M. Pivotal Response Intervention I: Overview of Approach. J. Assoc. Pers. Sev. Handicap. 1999, 24, 174–185. [Google Scholar] [CrossRef]
- Koegel, R.L.; Koegel, L.; Brookman, L. Empirically supported pivotal response intervention for children with autism. In Evidence-Based Psychotherapies for Children and Adolescents; Guilford Press: New York, NY, USA, 2003; pp. 341–357. [Google Scholar]
- Schopler, E.; Brehm, S.S.; Kinsbourne, M.; Reichler, R.J. Effect of Treatment Structure on Development in Autistic Children. Arch. Gen. Psychiatry 1971, 24, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Schopler, E.; Mesibov, G.B.; Hearsey, K. Structured Teaching in the TEACCH System. In Learning and Cognition in Autism; Plenum Press: New York, NY, USA, 1995; pp. 243–268. [Google Scholar]
- Schopler, E.; Reichler, R.J. Parents as cotherapists in the treatment of psychotic children. J. Autism Dev. Disord. 1971, 1, 87–102. [Google Scholar] [CrossRef] [PubMed]
- Schopler, E.; Mesibov, G.; Baker, A. Evaluation of Treatment for Autistic Children and Their Parents. J. Am. Acad. Child Psychiatry 1982, 21, 262–267. [Google Scholar] [CrossRef]
- Ozonoff, S.; Cathcart, K. Effectiveness of a home program intervention for young children with autism. J. Autism Dev. Disord. 1998, 28, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Panerai, S.; Ferrante, L.; Zingale, M. Benefits of the Treatment and Education of Autistic and Communication Handicapped Children (TEACCH) programme as compared with a non-specific approach. J. Intellect. Disabil. Res. 2002, 46, 318–327. [Google Scholar] [CrossRef] [Green Version]
- Virues-Ortega, J.; Julio, F.M.; Pastor-Barriuso, R. The TEACCH program for children and adults with autism: A meta-analysis of intervention studies. Clin. Psychol. Rev. 2013, 33, 940–953. [Google Scholar] [CrossRef] [Green Version]
- Welterlin, A.; Turner-Brown, L.M.; Harris, S.; Mesibov, G.; Delmolino, L. The Home TEACCHing Program for Toddlers with Autism. J. Autism Dev. Disord. 2011, 42, 1827–1835. [Google Scholar] [CrossRef]
- Rogers, S.J.; Estes, A.; Lord, C.; Vismara, L.; Winter, J.; Fitzpatrick, A.; Guo, M.; Dawson, G. Effects of a Brief Early Start Denver Model (ESDM)–Based Parent Intervention on Toddlers at Risk for Autism Spectrum Disorders: A Randomized Controlled Trial. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 1052–1065. [Google Scholar] [CrossRef] [Green Version]
- De Mello, M.C. Responsive parenting: Interventions and outcomes. Bull. World Heal. Organ. 2006, 84, 991–998. [Google Scholar] [CrossRef]
- Mahoney, G.; Nam, S. The Parenting Model of Developmental Intervention. Int. Rev. Res. Dev. Disabil. 2011, 41, 73–125. [Google Scholar] [CrossRef]
- Manolson, A. It Takes Two to Talk: A Parent’s Guide to Helping Children Communicate, 2nd ed.; Hanen Center: Toronto, ON, Canada, 1992. [Google Scholar]
- Baxendale, J.; Hesketh, A. Comparison of the effectiveness of the Hanen Parent Programme and traditional clinic therapy. Int. J. Lang. Commun. Disord. 2003, 38, 397–415. [Google Scholar] [CrossRef] [PubMed]
- Fong, N.W.Y.; Ho, S.K.Y.; So, B.J.W.; Lian, W.B. Evaluation of the Hanen it Takes Two to Talk Intervention Programme. Proc. Singap. Heal. 2012, 21, 251–256. [Google Scholar] [CrossRef] [Green Version]
- Pennington, L.; Thomson, K. It Takes Two to Talk–The Hanen Program® and families of children with motor disorders: A UK perspective. Child Care Heal. Dev. 2007, 33, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.S.; Messinger, D.S.; Stone, W.L.; Celimli, S.; Nahmias, A.S.; Yoder, P. A randomized controlled trial of Hanen’s ‘More Than Words’ in toddlers with early autism symptoms. J. Child Psychol. Psychiatry 2011, 52, 741–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pickles, A.; Le Couteur, A.; Leadbitter, K.; Salomone, E.; Cole-Fletcher, R.; Tobin, H.; Gammer, I.; Lowry, J.; Vamvakas, G.; Byford, S.; et al. Parent-mediated social communication therapy for young children with autism (PACT): Long-term follow-up of a randomised controlled trial. Lancet 2016, 388, 2501–2509. [Google Scholar] [CrossRef] [Green Version]
- Kasari, C.; Freeman, S.; Paparella, T. Joint attention and symbolic play in young children with autism: A randomized controlled intervention study. J. Child Psychol. Psychiatry 2006, 47, 611–620. [Google Scholar] [CrossRef]
- Kasari, C.; Gulsrud, A.C.; Wong, C.; Kwon, S.; Locke, J. Randomized Controlled Caregiver Mediated Joint Engagement Intervention for Toddlers with Autism. J. Autism Dev. Disord. 2010, 40, 1045–1056. [Google Scholar] [CrossRef] [Green Version]
- Kasari, C.; Freeman, S.F.; Paparella, T. Early intervention in autism: Joint attention and symbolic play. Int. Rev. Res. Ment. Retard. 2000, 32, 207–237. [Google Scholar]
- Kasari, C.; Gulsrud, A.; Freeman, S.; Paparella, T.; Hellemann, G. Longitudinal Follow-Up of Children with Autism Receiving Targeted Interventions on Joint Attention and Play. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 487–495. [Google Scholar] [CrossRef] [Green Version]
- Goods, K.S.; Ishijima, E.; Chang, Y.-C.; Kasari, C. Preschool Based JASPER Intervention in Minimally Verbal Children with Autism: Pilot RCT. J. Autism Dev. Disord. 2013, 43, 1050–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ingersoll, B.; Dvortcsak, A. Including Parent Training in the Early Childhood Special Education Curriculum for Children with Autism Spectrum Disorders. J. Posit. Behav. Interv. 2006, 8, 79–87. [Google Scholar] [CrossRef]
- Ingersoll, B.; Dvortcsak, A.; Whalen, C.; Sikora, D. The Effects of a Developmental, Social—Pragmatic Language Intervention on Rate of Expressive Language Production in Young Children with Autistic Spectrum Disorders. Focus Autism Other Dev. Disabil. 2005, 20, 213–222. [Google Scholar] [CrossRef]
- Ingersoll, B. The effect of context on imitation skills in children with autism. Res. Autism Spectr. Disord. 2008, 2, 332–340. [Google Scholar] [CrossRef]
- Ingersoll, B. The Social Role of Imitation in Autism. Infants Young Child. 2008, 21, 107–119. [Google Scholar] [CrossRef] [Green Version]
- Ingersoll, B. Brief Report: Pilot Randomized Controlled Trial of Reciprocal Imitation Training for Teaching Elicited and Spontaneous Imitation to Children with Autism. J. Autism Dev. Disord. 2010, 40, 1154–1160. [Google Scholar] [CrossRef] [Green Version]
- Ingersoll, B. Brief report: Effect of a focused imitation intervention on social functioning in children with autism. J. Autism Dev. Disord. 2012, 42, 1768–1773. [Google Scholar] [CrossRef] [Green Version]
- Ingersoll, B.; Gergans, S. The effect of a parent-implemented imitation intervention on spontaneous imitation skills in young children with autism. Res. Dev. Disabil. 2007, 28, 163–175. [Google Scholar] [CrossRef]
- Ingersoll, B.R. Teaching Social Communication. J. Posit. Behav. Interv. 2010, 12, 33–43. [Google Scholar] [CrossRef]
- Ingersoll, B.R.; Wainer, A.L. Pilot study of a school-based parent training program for preschoolers with ASD. Autism 2011, 17, 434–448. [Google Scholar] [CrossRef]
- Sen, E.; Yurtsever, S. Difficulties Experienced by Families with Disabled Children. Pediatr. Nurs. 2007, 12, 238–252. [Google Scholar] [CrossRef] [PubMed]
- Eyberg, S. Parent-Child Interaction Therapy: Integration of Traditional and Behavior Concerns. Child Fam. Behav. Ther. 1988, 10, 33–46. [Google Scholar] [CrossRef]
- McElreath, L.H.; Eisenstadt, T.H. Child directed interaction: Family play therapy for developmentally delayed preschoolers. In Family Play Therapy; Aronson: West New York, NJ, USA, 1994; pp. 271–292. [Google Scholar]
- Sofronoff, K.; Farbotko, M. The effectiveness of parent management training to increase self-efficacy in parents of children with Asperger syndrome. Autism 2002, 6, 271–286. [Google Scholar] [CrossRef] [PubMed]
- Sofronoff, K.; Leslie, A.; Brown, W. Parent Management Training and Asperger Syndrome. Autism 2004, 8, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Lesack, R.; Bearss, K.; Celano, M.; Sharp, W.G. Parent–Child Interaction Therapy and autism spectrum disorder: Adaptations with a child with severe developmental delays. Clin. Pr. Pediatr. Psychol. 2014, 2, 68–82. [Google Scholar] [CrossRef]
- Dunlap, G.; Iovannone, R.; Wilson, K.J.; Kincaid, D.K.; Strain, P. Prevent-Teach-Reinforce: A Standardized Model of School-Based Behavioral Intervention. J. Posit. Behav. Interv. 2010, 12, 9–22. [Google Scholar] [CrossRef]
- Iovannone, R.; Greenbaum, P.E.; Wang, W.; Kincaid, D.; Dunlap, G.; Strain, P. Randomized Controlled Trial of the Prevent—Teach—Reinforce (PTR) Tertiary Intervention for Students with Problem Behaviors. J. Emot. Behav. Disord. 2009, 17, 213–225. [Google Scholar] [CrossRef] [Green Version]
- Sears, K.M.; Blair, K.-S.C.; Iovannone, R.; Crosland, K. Using the Prevent-Teach-Reinforce Model with Families of Young Children with ASD. J. Autism Dev. Disord. 2012, 43, 1005–1016. [Google Scholar] [CrossRef]
- Ruble, L.; Dalrymple, N.; McGrew, J. The Collaborative Model for Promoting Competence and Success for Students with ASD; Springer: New York, NY, USA, 2012. [Google Scholar]
- Ruble, L.A.; McGrew, J.H.; Toland, M.D.; Dalrymple, N.J.; Jung, L.A. A randomized controlled trial of COMPASS web-based and face-to-face teacher coaching in autism. J. Consult. Clin. Psychol. 2013, 81, 566–572. [Google Scholar] [CrossRef] [Green Version]
- Ruble, L.A.; Birdwhistell, J.; Toland, M.D.; McGrew, J.H. Analysis of Parent, Teacher, and Consultant Speech Exchanges and Educational Outcomes of Students with Autism During COMPASS Consultation. J. Educ. Psychol. Consult. 2011, 21, 259–283. [Google Scholar] [CrossRef] [Green Version]
- Sanders, M.R. Triple P-Positive Parenting Program: Towards an Empirically Validated Multilevel Parenting and Family Support Strategy for the Prevention of Behavior and Emotional Problems in Children. Clin. Child Fam. Psychol. Rev. 1999, 2, 71–90. [Google Scholar] [CrossRef] [PubMed]
- Sanders, M.R.; Markie-Dadds, C.; Turner, K.M.T. Practitioner’s Manual for Standard Triple P; Families International Publishing Pty Ltd.: Brisbane, Australia, 2001. [Google Scholar]
- Roux, G.; Sofronoff, K.; Sanders, M. A Randomized Controlled Trial of Group Stepping Stones Triple P: A Mixed-Disability Trial. Fam. Process. 2013, 52, 411–424. [Google Scholar] [CrossRef] [PubMed]
- Ginott, H.G. The theory and practice of “therapeutic intervention” in child treatment. J. Consult. Psychol. 1959, 23, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Ginott, H.G. A rationale for selecting toys in play therapy. J. Consult. Psychol. 1960, 24, 243–246. [Google Scholar] [CrossRef]
- Mastrangelo, S. Play and the child with autism spectrum disorder: From possibilities to practice. Int. J. Play. Ther. 2009, 18, 13–30. [Google Scholar] [CrossRef]
- Leblanc, M.; Ritchie, M. A meta-analysis of play therapy outcomes. Couns. Psychol. Q. 2010, 14, 149–163. [Google Scholar] [CrossRef]
- Bratton, S.C.; Ray, D.; Rhine, T.; Jones, L. The Efficacy of Play Therapy with Children: A Meta-Analytic Review of Treatment Outcomes. Prof. Psychol. Res. Pr. 2005, 36, 376–390. [Google Scholar] [CrossRef]
- Hillman, H. Child-centered play therapy as an intervention for children with autism: A literature review. Int. J. Play. Ther. 2018, 27, 198–204. [Google Scholar] [CrossRef]
- Prizant, B.M.; Wetherby, A.M. Understanding the Continuum of Discrete-Trial Traditional Behavioral to Social-Pragmatic Developmental Approaches in Communication Enhancement for Young Children with Autism/PDD. Semin. Speech Lang. 1998, 19, 329–353. [Google Scholar] [CrossRef]
- Booth, P.B.; Jernberg, A.M. Theraplay: Helping Parents and Children Build Better Relationships Through Attachment-Based Play; Wiley: New York, NY, USA, 2010. [Google Scholar]
- Simeone-Russell, R. A practical approach to implementing theraplay for children with autism spectrum disorder. Int. J. Play. Ther. 2011, 20, 224–235. [Google Scholar] [CrossRef] [Green Version]
- Howard, A.H.; Lindaman, S.; Copeland, R.; Cross, D.R. Theraplay impact on parents and children with autism spectrum disorder: Improvements in affect, joint attention, and social cooperation. Int. J. Play. Ther. 2018, 27, 56–68. [Google Scholar] [CrossRef]
- Greenspan, S.L.; Wieder, S. An integrated developmental approach to interventions for interventions for young children with severe difficulties in relating and communicating. In Assessing and Treating Infants and Young Children with Severe Difficulties in Relating and Communicating; Zero to Three: Washington, DC, USA, 1997; pp. 5–18. [Google Scholar]
- Greenspan, S.L.; Wieder, S. Engaging Autism: Using the Floortime Approach to Help Children Relate, Communicate, and Think; SaCapo Press: Cambirdge, MA, USA, 2006. [Google Scholar]
- Dionne, M.; Martini, R. Floor time play with a child with autism: A single-subject study. Can. J. Occup. Ther. 2011, 78, 196–203. [Google Scholar] [CrossRef]
- Siller, M.; Sigman, M. The Behaviors of Parents of Children with Autism Predict the Subsequent Development of Their Children’s Communication. J. Autism Dev. Disord. 2002, 32, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Siller, M.; Sigman, M. Modeling longitudinal change in the language abilities of children with autism: Parent behaviors and child characteristics as predictors of change. Dev. Psychol. 2008, 44, 1691–1704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siller, M.; Hutman, T.; Sigman, M. A Parent-Mediated Intervention to Increase Responsive Parental Behaviors and Child Communication in Children with ASD: A Randomized Clinical Trial. J. Autism Dev. Disord. 2013, 43, 540–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, T.; Iadarola, S. Evidence Base Update for Autism Spectrum Disorder. J. Clin. Child Adolesc. Psychol. 2015, 44, 897–922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, R.; Hancock, T.B.; Singh, N.N. Overview of Early Intensive Behavioral Intervention for Children with Autism. In Evidence-Based Practices in Behavioral Health; Springer International Publishing: Basel, Switzerland, 2016; pp. 1–14. [Google Scholar]
- Howlin, P.; Charman, T.; Ghaziuddin, M. Autism Spectrum Disorders: Interventions and Outcome. In The SAGE Handbook of Developmental Disorders; SAGE Publications: London, UK, 2012; pp. 307–328. [Google Scholar] [CrossRef]
- Bradshaw, J.L.; Steiner, A.M.; Gengoux, G.; Koegel, L.K. Feasibility and Effectiveness of Very Early Intervention for Infants At-Risk for Autism Spectrum Disorder: A Systematic Review. J. Autism Dev. Disord. 2015, 45, 778–794. [Google Scholar] [CrossRef]
- Harris, S.L.; Handleman, J.S. Age and IQ at Intake as Predictors of Placement for Young Children with Autism: A Four- to Six-Year Follow-Up. J. Autism Dev. Disord. 2000, 30, 137–142. [Google Scholar] [CrossRef]
- Smith, T.; Klorman, R.; Mruzek, D.W. Predicting Outcome of Community-Based Early Intensive Behavioral Intervention for Children with Autism. J. Abnorm. Child Psychol. 2015, 43, 1271–1282. [Google Scholar] [CrossRef]
- Howard, J.S.; Stanislaw, H.; Green, G.; Sparkman, C.R.; Cohen, H.G. Comparison of behavior analytic and eclectic early interventions for young children with autism after three years. Res. Dev. Disabil. 2014, 35, 3326–3344. [Google Scholar] [CrossRef] [Green Version]
- Klintwall, L.; Eldevik, S.; Eikeseth, S. Narrowing the gap: Effects of intervention on developmental trajectories in autism. Autism 2015, 19, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Virues-Ortega, J. Applied behavior analytic intervention for autism in early childhood: Meta-analysis, meta-regression and dose–response meta-analysis of multiple outcomes. Clin. Psychol. Rev. 2010, 30, 387–399. [Google Scholar] [CrossRef] [PubMed]
- Strauss, K.; Mancini, F.; Fava, L. Parent inclusion in early intensive behavior interventions for young children with ASD: A synthesis of meta-analyses from 2009 to 2011. Res. Dev. Disabil. 2013, 34, 2967–2985. [Google Scholar] [CrossRef] [PubMed]
- Farmer, J.; Reupert, A.E. Understanding Autism and understanding my child with Autism: An evaluation of a group parent education program in rural Australia. Aust. J. Rural. Heal. 2013, 21, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.E.; Greenberg, J.S.; Mailick, M.R. The Family Context of Autism Spectrum Disorders. Child Adolesc. Psychiatr. Clin. North Am. 2014, 23, 143–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonge, B.; Brereton, A.; Kiomall, M.; MacKinnon, A.; King, N.; Rinehart, N. Effects on Parental Mental Health of an Education and Skills Training Program for Parents of Young Children with Autism: A Randomized Controlled Trial. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Drahota, A.; Aarons, G.A.; Stahmer, A.C.; Leonard, K.L.; Solomon, D.; Hepel, J.T.; Hiatt, J.R.; Wazer, D.E.; DiPetrillo, T.A. Developing the Autism Model of Implementation for Autism spectrum disorder community providers: Study protocol. Implement. Sci. 2012, 7, 72–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreibman, L.; Dawson, G.; Stahmer, A.C.; Landa, R.J.; Rogers, S.J.; McGee, G.G.; Kasari, C.; Ingersoll, B.; Kaiser, A.P.; Bruinsma, Y.; et al. Naturalistic Developmental Behavioral Interventions: Empirically Validated Treatments for Autism Spectrum Disorder. J. Autism Dev. Disord. 2015, 45, 2411–2428. [Google Scholar] [CrossRef] [Green Version]
- Wood, J.J.; McLeod, B.D.; Klebanoff, S.; Brookman-Frazee, L. Toward the Implementation of Evidence-Based Interventions for Youth with Autism Spectrum Disorders in Schools and Community Agencies. Behav. Ther. 2015, 46, 83–95. [Google Scholar] [CrossRef]
- Chiri, G.; Warfield, M.E. Unmet Need and Problems Accessing Core Health Care Services for Children with Autism Spectrum Disorder. Matern. Child Heal. J. 2011, 16, 1081–1091. [Google Scholar] [CrossRef]
- Dingfelder, H.E.; Mandell, D.S. Bridging the Research-to-Practice Gap in Autism Intervention: An Application of Diffusion of Innovation Theory. J. Autism Dev. Disord. 2011, 41, 597–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phaneuf, L.; McIntyre, L.L. The Application of a Three-Tier Model of Intervention to Parent Training. J. Posit. Behav. Interv. 2011, 13, 198–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, S.; Weiss, J.A. Examining the relationship between social support and stress for parents of individuals with autism. Res. Autism Spectr. Disord. 2020, 74, 101557. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| LEVEL 1 |
|
| Individual data analysis; homogeneous studies; different analysis techniques; meta-regression; meta-analysis; quality of studies |
|
| Evaluation of statistical power; multilevel; quality of the studies | |
| LEVEL 2 |
|
| Evaluation of statistical power; matching controls in time; quality of the studies |
|
| Individual data analysis; homogeneous studies; different analysis techniques; quality of the studies | |
| LEVEL 3 |
|
| Quality of the studies |
| |||
| |||
| LEVEL 4 |
|
|
| Study Quality Criteria | Evaluation | |
|---|---|---|
| 1 | Design and assignment of participants to groups: the study includes two group designs with random assignment of participants to the control and treatment groups. The randomization procedure should be specified. |
|
| 2 | Independent variable is well defined: it is properly defined, and manuals or treatment scripts are used. |
|
| 3 | Well-clarified reference population: the study is conducted on a well-defined population, and addresses a specific problem for which the inclusion criteria have been clearly defined. |
|
| 4 | Outcome evaluation: evaluation is done using reliable standardized tests designed to measure the specific problems targeted by the intervention. |
|
| 5 | Adequacy of the statistical analysis: appropriate analysis methods are used, and the sample size is sufficient to detect the studied effects. |
|
| Subjects | Level of Evidence | Quality of the Study | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Country ** | Sample | Age | 1 | 2 | 3 | 4 | 5 | ||
| Parent-Mediated Intervention in Comprehensive Intervention Programs | |||||||||
| Search Results for “Parent Training” | |||||||||
| Bearss et al. (2015) [28] | US | 180 | 36 to 84 | 2.1 | 2 | 3 | 3 | 2 | 3 |
| Oosterling et al. (2010) [36] | NL | 67 | 12 to 42 | 2.1 | 3 | 2 | 3 | 3 | 3 |
| Bearss et al. (2013) [37] | US | 16 | 36 to 72 | 3.2 | 0 | 3 | 3 | 3 | 2 |
| Bagaiolo et al. (2017) [38] | BR | 67 | 48 | 2.1 | 2 | 1 | 2 | 1 | 2 |
| Wacker et al. (2013) [39] | US | 17 | 24 to 84 | 4.2 | 0 | 2 | 3 | 3 | 2 |
| Blackman et al. (2020) [40] | US | 80 | 36 to 60 | 2.1 | 2 | 3 | 3 | 2 | 3 |
| Iadarola et al. (2018) [41] | US | 108 | 36 to 84 | 2.1 | 3 | 3 | 3 | 3 | 3 |
| Search Results for “Pivotal Response Training” | |||||||||
| Minjarez et al. (2011) [42] | US | 28 | 24 to 84 | 2.1 | 1 | 2 | 3 | 2 | 2 |
| Gengoux et al. (2015) [43] | US | 23 | 24 to 72 | 2.1 | 2 | 2 | 2 | 2 | 3 |
| Hardan et al. (2015) [44] | US | 53 | 24 to72 | 2.1 | 2 | 2 | 3 | 2 | 3 |
| Bradshaw et al. (2017) [45] | US | 3 | 15 to 21 | 3.3 | 0 | 3 | 2 | 2 | 2 |
| Search Results Classified as TEACCH * | |||||||||
| Welterlin et al. (2012) [46] | US | 20 | 24 to 36 | 2.1 | 3 | 2 | 2 | 2 | 3 |
| D’Elia et al. (2014) [47] | IT | 30 | 24 to 72 | 2.1 | 2 | 2 | 3 | 2 | 3 |
| Search Results Classified as ESDM * Methodology | |||||||||
| Rogers et al. (2012) [48] | US | 98 | 12 to 24 | 2.1 | 2 | 3 | 2 | 3 | 3 |
| Rogers et al. (2014) [49] | US | 7 | 7 to 15 | 2.1 | 2 | 3 | 3 | 3 | 3 |
| Vivanti et al. (2014) [50] | AU | 7 | 24 to 72 | 2.1 | 2 | 2 | 3 | 3 | 3 |
| Rogers et al. (2018) [51] | US | 45 | 12 to 30 | 2.1 | 3 | 2 | 3 | 3 | 3 |
| Waddington et al. (2019) [52] | NZ | 5 | 23 to 59 | 3.2 | 0 | 2 | 2 | 3 | 2 |
| Parent-Mediated Programs Focused on ASD Symptoms | |||||||||
| Search results classified as Hanen program | |||||||||
| Carter et al. (2011) [53] | US | 62 | 20 | 2.1 | 2 | 2 | 2 | 3 | 2 |
| Search Results Classified as the “PACT” Method | |||||||||
| Green et al. (2010) [54] | UK | 152 | 24 to 48 | 2.1 | 3 | 3 | 3 | 3 | 3 |
| Search Results for the JASPER * Model | |||||||||
| Goods et al. (2013) [55] | US | 15 | 36 to 60 | 2.1 | 3 | 3 | 3 | 3 | 3 |
| Kasari et al. (2015) [56] | US | 86 | 22 to 36 | 2.1 | 3 | 3 | 3 | 2 | 3 |
| Gulsrud et al. (2016) [57] | US | 86 | 36 | 2.1 | 2 | 3 | 3 | 3 | 3 |
| Shiere et al. (2016) [58] | US | 85 | 36 | 2.1 | 2 | 3 | 3 | 3 | 3 |
| Search Results for the ImPact * Model | |||||||||
| Ingersoll and Wainer (2013) [59] | US | 27 | 36 | 2.1 | 2 | 3 | 2 | 2 | 3 |
| Ingersoll and Wainer (2013) [60] | US | 8 | 36 to 72 | 3.3 | 0 | 0 | 2 | 2 | 3 |
| Stadnick et al. (2015) [61] | US | 16 | 47 | 2.1 | 2 | 3 | 3 | 3 | 3 |
| Ingersoll et al. (2016) [62] | US | 28 | 19 to 73 | 2.1 | 2 | 3 | 3 | 3 | 3 |
| Ingersoll et al. (2017) [63] | US | 9 | 32 to 65 | 2.2 | 0 | 3 | 3 | 3 | 3 |
| Programs for the Promotion of Positive Parenthood and Family well-being | |||||||||
| Search results for the PCIT * model | |||||||||
| Lesack et al. (2014) [64] | US | 1 | 60 | 3.3 | 0 | 2 | 2 | 2 | 2 |
| Hansen and Shillingsburg (2016) [65] | US | 2 | 45 and 32 | 3.3 | 0 | 2 | 3 | 2 | 2 |
| Masse et al. (2016) [66] | US | 3 | 24 to 84 | 3.3 | 0 | 2 | 3 | 3 | 3 |
| Zlomke et al. (2017) [67] | US | 17 | 24 to 96 | 3.3 | 0 | 3 | 3 | 2 | 2 |
| Parladé et al. (2020) [68] | US | 36 | 36 to 84 | 2.1 | 3 | 3 | 3 | 3 | 3 |
| Search Results for the PRT-F * Model | |||||||||
| Sears et al. (2013) [69] | US | 2 | 36 to 60 | 3.3 | 0 | 1 | 2 | 3 | 3 |
| Bailey et al. (2015) [70] | US | 3 | 60 to 84 | 3.3 | 0 | 2 | 3 | 2 | 3 |
| Search Results for the COMPASS * Method | |||||||||
| Ruble et al. (2011) [71] | US | 35 | 72 | 3.1 | 1 | 3 | 3 | 3 | 2 |
| Kuravackel et al. (2018) [72] | US | 33 | 96 | 2.1 | 2 | 3 | 3 | 3 | 3 |
| Search Results for the SSTP * Method | |||||||||
| Roux et al. (2013) [73] | AU | 52 | 24 to 108 | 2.1 | 3 | 3 | 2 | 3 | 3 |
| Tellegen et al. (2014) [74] | AU | 64 | 24 to 108 | 2.1 | 2 | 3 | 2 | 3 | 3 |
| Schortt et al. (2018) [75] | DE | 24 | 36 to 144 | 3.1 | 0 | 2 | 3 | 2 | 3 |
| Play-Focused Intervention Programs | |||||||||
| Search Results for the Theraplay Method | |||||||||
| Howard et al. (2018) [76] | US | 8 | 36 to 108 | 3.3 | 0 | 2 | 2 | 2 | 2 |
| Search Results for the Floor Time Play Method | |||||||||
| Dionne et al. (2011) [77] | CA | 1 | 42 | 3.3 | 0 | 1 | 0 | 1 | 0 |
| Pajareya and Nopmaneejumruslers (2011) [78] Pajareya and Nopmaneejumruslers (2012) [79] | TH | 32 | 24 to 72 | 2.1 | 3 | 2 | 2 | 2 | 2 |
| Lil and Chhanbria (2013) [80] | TW | 11 | 42 to 69 | 3.1 | 0 | 3 | 2 | 2 | 3 |
| Solomon et al. (2014) [81] | US | 128 | 32 to 72 | 2.1 | 3 | 2 | 2 | 2 | 3 |
| Aali et al. (2015) [82] | IR | 12 | 36 to 96 | 3.1 | 0 | 0 | 0 | 1 | 1 |
| Sealy and Glovinsky (2016) [83] | US | 40 | 24 to 72 | 2.1 | 3 | 2 | 3 | 2 | 3 |
| Search Results for the FPI * | |||||||||
| Siller et al. (2013) [84] Siller et al. (2014) [85] | US | 70 | 36 to 72 | 2.1 | 3 | 2 | 3 | 3 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojas-Torres, L.P.; Alonso-Esteban, Y.; Alcantud-Marín, F. Early Intervention with Parents of Children with Autism Spectrum Disorders: A Review of Programs. Children 2020, 7, 294. https://doi.org/10.3390/children7120294
Rojas-Torres LP, Alonso-Esteban Y, Alcantud-Marín F. Early Intervention with Parents of Children with Autism Spectrum Disorders: A Review of Programs. Children. 2020; 7(12):294. https://doi.org/10.3390/children7120294
Chicago/Turabian StyleRojas-Torres, Liliana Paulina, Yurena Alonso-Esteban, and Francisco Alcantud-Marín. 2020. "Early Intervention with Parents of Children with Autism Spectrum Disorders: A Review of Programs" Children 7, no. 12: 294. https://doi.org/10.3390/children7120294