Integrated Strength and Fundamental Movement Skill Training in Children: A Pilot Study



Abstract
:1. Introduction
2. Materials and Methods
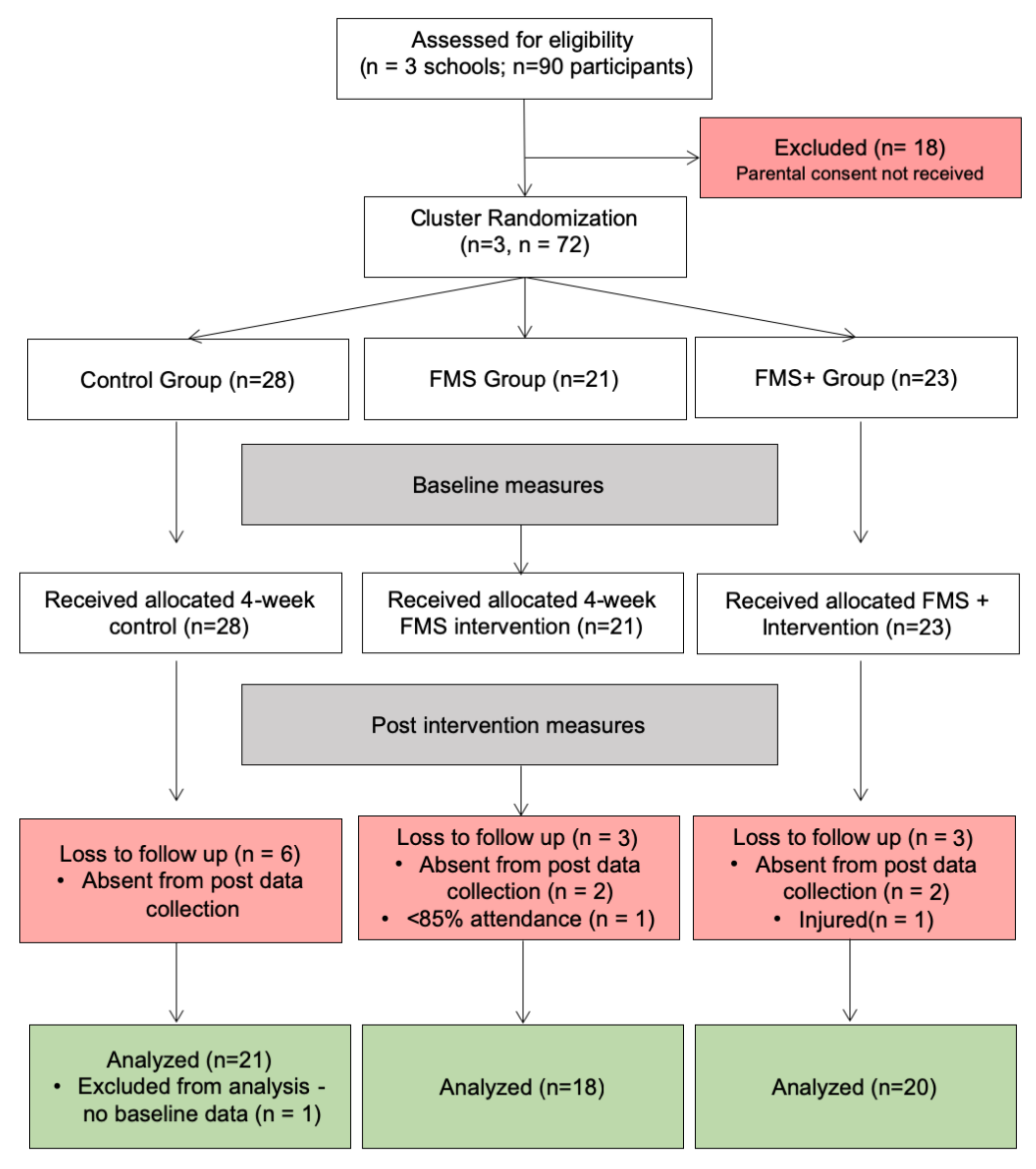
2.1. Participants
2.2. Procedures
2.3. Intervention
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018; pp. 1–104. [Google Scholar]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.-P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor Gorber, S.; Kho, M.E.; et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S197–S239. [Google Scholar] [CrossRef] [PubMed]
- Parfitt, G.; Eston, R. The relationship between children’s habitual activity level and psychological well-being. Acta Paediatr. 2005, 94, 1791–1797. [Google Scholar] [CrossRef] [PubMed]
- Twisk, J.; Kemper, H.C.; van Mechelen, W. Prediction of cardiovascular disease risk factors later in life by physical activity and physical fitness in youth: General comments and conclusions. Int. J. Sports Med. 2002, 23, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Robertson, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A developmental perspective on the role of motor skill competence in physical activity: An emergent relationship. Phys. Educ. Sport Pedagog. 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Department of Health and Social Care. UK Chief Medical Officers Physical Activity Guidelines; Department of Health and Social Care: London, UK, 2019; pp. 1–66. [Google Scholar]
- Sport England, Active Lives Children and Young People Survey Academic Year 2018/19; Sport England: London, UK, 2018; pp. 1–48.
- Farooq, M.A.; Parkinson, K.N.; Adamson, A.J.; Pearce, M.S.; Reilly, J.K.; Hughes, A.R.; Janssen, X.; Basterfield, L.; Reilly, J.J. Timing of the decline in physical activity in childhood and adolescence: Gateshead Millennium Cohort Study. Br. J. Sports Med. 2018, 52, 1002–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birch, S.; Cummings, L.; Oxford, S.W.; Duncan, M.J. Examining relative age effects in fundamental skill proficiency in British children aged 6–11 years. J. Strength. Cond. Res. 2016, 30, 2809–2815. [Google Scholar] [CrossRef] [PubMed]
- Barnett, L.M.; Stodden, D.; Cohen, K.E.; Smith, J.J.; Lubans, D.R.; Lenoir, M.; Iivonen, S.; Miller, A.D.; Laukkanen, A.; Dudley, D.; et al. Fundamental Movement Skills: An Important Focus. J. Teach. Phys. Educ. 2016, 35, 219–225. [Google Scholar] [CrossRef]
- Clark, J.E.; Metcalfe, J.S. The mountain of motor development: A metaphor. In Motor Development Research and Reviews; Clark, J.E., Humphrey, J., Eds.; Sports Performance and Science Reports: Reston, VA, USA, 2002; Volume 2, pp. 163–190. [Google Scholar]
- Gallahue, D.L.; Ozmun, J.C.; Goodway, J.D. Understanding Motor Development: Infants, Children, Adolescents, Adults; McGraw-Hill Education: New York, NY, USA, 2012. [Google Scholar]
- O’Brien, W.; Belton, S.; Issartel, J. Fundamental movement skill proficiency amongst adolescent youth. Phys. Educ. Sport Pedagog. 2016, 21, 557–571. [Google Scholar] [CrossRef]
- Institute of Medicine. Educating the Student Body: Taking Physical Activity and Physical Education to School; National Academies Press: Washington, DC, USA, 2017; pp. 1–503. [Google Scholar]
- UK Department for Education. National Curriculum—Physical Education Key Stages 1 to 2; UK Department for Education: London, UK, 2013; pp. 1–3. [Google Scholar]
- Rudd, J.R.; Crotti, M.; Fitton-Davies, K.; O’Callaghan, L.; Bardid, F.; Utesch, T.; Roberts, S.; Boddy, L.M.; Cronin, C.J.; Knowles, Z.; et al. Skill Acquisition Methods Fostering Physical Literacy in Early-Physical Education (SAMPLE-PE): Rationale and Study Protocol for a Cluster Randomized Controlled Trial in 5–6-Year-Old Children From Deprived Areas of North West England. Front. Psychol. 2020, 11, 1128. [Google Scholar] [CrossRef]
- Harris, J. The Case for Physical Education becoming a Core Subject in the National Curriculum. Available online: https://www.afpe.org.uk/physical-education/wp-content/uploads/PE-Core-Subject-Paper-20-3-18.pdf (accessed on 4 September 2020).
- Quarmby, T.; Daly-Smith, A.; Kime, N. “You get some very archaic ideas of what teaching is … ”: Primary school teachers’ perceptions of the barriers to physically active lessons. Education 3-13 2018, 47, 308–321. [Google Scholar] [CrossRef]
- Morgan, P.J.; Young, M.D.; Barnes, A.T.; Eather, N.; Pollock, E.R.; LUBANS, D.R. Engaging Fathers to Increase Physical Activity in Girls: The “Dads And Daughters Exercising and Empowered” (DADEE) Randomized Controlled Trial. Ann. Behav. Med. 2018, 53, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Salmon, J.; Ball, K.; Hume, C.; Booth, M.; Crawford, D. Outcomes of a group-randomized trial to prevent excess weight gain, reduce screen behaviours and promote physical activity in 10-year-old children: Switch-Play. Int. J. Obes. 2008, 32, 601–612. [Google Scholar] [CrossRef] [Green Version]
- Barnes, A.T.; Plotnikoff, R.C.; Collins, C.E.; Morgan, P.J. Feasibility and Preliminary Efficacy of the MADE4Life Program: A Pilot Randomized Controlled Trial. J. Phys. Act. Health 2016, 12, 1378–1393. [Google Scholar] [CrossRef] [PubMed]
- Cohen, K.E.; Morgan, P.J.; Plotnikoff, R.C.; Callister, R.; Lubans, D.R. Physical activity and skills intervention: SCORES cluster randomized controlled trial. Med. Sci. Sport Exerc. 2015, 47, 765–774. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; McGrane, B.; Sanders, G.; Taylor, S.; Owen, M.; Curry, W. A non-equivalent group pilot trial of a school-based physical activity and fitness intervention for 10–11 year old english children: Born to move. BMC Public Health 2016, 16, 861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Telford, R.M.; Olive, L.S.; Cochrane, T.; Davey, R.; Telford, R.D. Outcomes of a four-year specialist-taught physical education program on physical activity: A cluster randomized controlled trial, the LOOK study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 64. [Google Scholar] [CrossRef] [Green Version]
- Adab, P.; Pallan, M.J.; Lancashire, E.R.; Hemming, K.; Frew, E.; Barrett, T.; Bhopal, R.; Cade, J.E.; Canaway, A.; Clarke, J.L.; et al. Effectiveness of a childhood obesity prevention programme delivered through schools, targeting 6 and 7 year olds: Cluster randomised controlled trial (WAVES study). Br. Med. J. 2018, 7, 360. [Google Scholar] [CrossRef] [Green Version]
- Weber, K.; Spörkel, O.; Mertens, M.; Freese, A.; Strassburger, K.; Kemper, B.; Bachmann, C.; Diehlmann, K.; Stemper, T.; Buyken, A.; et al. Positive Effects of Promoting Physical Activity and Balanced Diets in a Primary School Setting with a High Proportion of Migrant School Children. Exp. Clin. Endocrinol. Diabetes 2017, 125, 554–562. [Google Scholar] [CrossRef]
- Taylor, S.; Noonan, R.; Knowles, Z.; Owen, M.; McGrane, B.; Curry, W.; Fairclough, S. Evaluation of a Pilot School-Based Physical Activity Clustered Randomised Controlled Trial—Active Schools: Skelmersdale. Int. J. Environ. Res. Public Health 2018, 15, 1011. [Google Scholar] [CrossRef] [Green Version]
- Robinson, L.E.; Goodway, J.D. Instructional climates in preschool children who are at-risk. Part II: Perceived physical competence. Res. Q. Exerc. Sport 2009, 80, 533–542. [Google Scholar] [CrossRef]
- Malina, R.M. Motor Development during Infancy and Early Childhood: Overview and Suggested Directions for Research. Int. J. Sport Health Sci. 2004, 2, 50–66. [Google Scholar] [CrossRef] [Green Version]
- Tietjens, M.; Barnett, L.M.; Dreiskämper, D.; Holfelder, B.; Utesch, T.O.; Lander, N.; Hinkley, T.; Schott, N. Conceptualising and testing the relationship between actual and perceived motor performance: A cross-cultural comparison in children from Australia and Germany. J. Sports Sci. 2020, 38, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Britton, Ú.; Belton, S.; Issartel, J. Small fish, big pond: The role of health-related fitness and perceived athletic competence in mediating the physical activity-motor competence relationship during the transition from primary to secondary school. J. Sports Sci. 2019, 37, 2538–2548. [Google Scholar] [CrossRef] [PubMed]
- Faigenbaum, A.D.; Kraemer, W.J.; Blimkie, C.J.R.; Jeffreys, I.; Micheli, L.J.; Nitka, M.; Rowland, T.W. Youth Resistance Training: Updated Position Statement Paper From the National Strength and Conditioning Association. J. Strength Cond. Res. 2009, 23, S60–S79. [Google Scholar] [CrossRef]
- Carroll, T.J.; Selvanayagam, V.S.; Riek, S.; Semmler, J.G. Neural adaptations to strength training: Moving beyond transcranial magnetic stimulation and reflex studies. Acta Physiol. 2011, 202, 119–140. [Google Scholar] [CrossRef]
- Sale, D.G. Neural adaptation to resistance training. Med. Sci. Sports Exerc. 1988, 20, S135–S145. [Google Scholar] [CrossRef]
- Bosch, F. Strength Training and Coordination; Frans Bosch & 2010 Publishers: Rotterdam, The Netherlands, 2015. [Google Scholar]
- Peitz, M.; Behringer, M.; Granacher, U. A systematic review on the effects of resistance and plyometric training on physical fitness in youth- What do comparative studies tell us? PLoS ONE 2018, 13, e0205525. [Google Scholar]
- Faude, O.; Rössler, R.; Petushek, E.J.; Roth, R.; Zahner, L.; Donath, L. Neuromuscular Adaptations to Multimodal Injury Prevention Programs in Youth Sports: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Front. Physiol. 2017, 8, 791. [Google Scholar] [CrossRef] [Green Version]
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Lloyd, R.S.; Oliver, J.L.; Faigenbaum, A.D.; Howard, R.; De Ste Croix, M.B.A.; Williams, C.A.; Best, T.M.; Alvar, B.A.; Micheli, L.J.; Thomas, D.P.; et al. Long-Term Athletic Development- Part 1: A Pathway for All Youth. J. Strength Cond. Res. 2015, 29, 1439–1450. [Google Scholar] [CrossRef]
- Kennedy, S.G.; Smith, J.J.; Morgan, P.J.; Peralta, L.R.; Hilland, T.A.; Eather, N.; Lonsdale, C.; Okely, A.D.; Plotnikoff, R.C.; Salmon, J.; et al. Implementing Resistance Training in Secondary Schools: An Exploration of Teachers’ Perceptions. Med. Sci. Sport Exerc. 2018, 50, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Engel, F.A.; Wagner, M.O.; Schelhorn, F.; Deubert, F.; Leutzsch, S.; Stolz, A.; Sperlich, B. Classroom-Based Micro-Sessions of Functional High-Intensity Circuit Training Enhances Functional Strength but Not Cardiorespiratory Fitness in School Children—A Feasibility Study. Front. Public Health 2019, 7, 70–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, F.B.; Silventoinen, K.; Tynelius, P.; Rasmussen, F. Muscular strength in male adolescents and premature death: Cohort study of one million participants. Br. Med. J. 2012, 345, e7279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, H.; Booth, J.N.; Duncan, A.; Fawkner, S.; Niven, A. The Effect of Resistance Training Interventions on “The Self” in Youth: A Systematic Review and Meta-analysis. Sports Med. Open 2019, 5, 29. [Google Scholar] [CrossRef] [Green Version]
- Faigenbaum, A.D.; MacDonald, J.P. Dynapenia: It’s not just for grown-ups anymore. Acta Paediatr. 2017, 106, 696–697. [Google Scholar] [CrossRef]
- Faigenbaum, A.D.; Myer, G.D. Exercise Deficit Disorder in Youth: Play Now or Pay Later. Curr. Sports Med. Rep. 2012, 11, 196–200. [Google Scholar] [CrossRef]
- Collins, H.; Booth, J.N.; Duncan, A.; Fawkner, S. The effect of resistance training interventions on fundamental movement skills in youth: A meta-analysis. Sports Med. Open 2019, 5, 17. [Google Scholar] [CrossRef]
- Van Sluijs, E.M.F.; Kriemler, S. Reflections on physical activity intervention research in young people—dos, don’ts, and critical thoughts. Int. J. Behav. Nutr. Phys. Act 2016, 13, 25. [Google Scholar] [CrossRef] [Green Version]
- Tomkinson, G.R.; Carver, K.D.; Atkinson, F.; Danielle, N.D.; Lewis, L.K.; Fitzgerald, J.S.; Lang, J.J.; Ortega, F.B. European normative values for physical fitness in children and adolescents aged 9–17 years: Results from 2 779 165 Eurofit performances representing 30 countries. Br. Med. J. 2018, 52, 1445–1456. [Google Scholar] [CrossRef] [Green Version]
- McWhannell, N.; Foweather, L.; Graves, L.; Henaghan, J.; Ridgers, N.; Stratton, G. From Surveillance to Intervention: Overview and Baseline Findings for the Active City of Liverpool Active Schools and SportsLinx (A-CLASS) Project. Int. J. Environ. Res. Public Health 2018, 15, 582. [Google Scholar] [CrossRef] [Green Version]
- Logan, S.W.; Ross, S.M.; Chee, K.; Stodden, D.F.; Robinson, L.E. Fundamental motor skills: A systematic review of terminology. J. Sports Sci. 2017, 36, 781–796. [Google Scholar] [CrossRef] [PubMed]
- Tyler, R.; Foweather, L.; Mackintosh, K.A.; Stratton, G. A Dynamic Assessment of Children’s Physical Competence. Med. Sci. Sports Exerc. 2018, 50, 2474–2487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longmuir, P.E.; Boyer, C.; Lloyd, M.; Borghese, M.M.; Knight, E.; Saunders, T.J.; Boiarskaia, E.; Zhu, W.; Tremblay, M.S. Canadian Agility and Movement Skill Assessment (CAMSA): Validity, objectivity, and reliability evidence for children 8–12 years of age. J. Sport Health Sci. 2017, 6, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Morley, D.; Till, K.; Ogilvie, P.; Turner, G. Influences of gender and socioeconomic status on the motor proficiency of children in the UK. Hum. Mov. Sci. 2015, 44, 150–156. [Google Scholar] [CrossRef]
- Duncan, M.J.; Eyre, E.L.J.; Oxford, S.W. The Effects of 10-week Integrated Neuromuscular Training on Fundamental Movement Skills and Physical Self-efficacy in 6–7-Year-Old Children. J. Strength Cond. Res. 2018, 32, 3348–3356. [Google Scholar] [CrossRef] [PubMed]
- Faigenbaum, A.D.; Farrell, A.; Fabiano, M.; Radler, T.; Naclerio, F.; Ratamess, N.A.; Kang, J.; Myer, G.D. Effects of Integrative Neuromuscular Training on Fitness Performance in Children. Pediatric Exerc. Sci. 2011, 23, 573–584. [Google Scholar] [CrossRef] [Green Version]
- Faigenbaum, A.D.; Westcott, W.L.; Micheli, L.J.; Outerbridge, A.R.; Long, C.J.; LaRosa-Loud, R.; Zaichkowsky, L.D. The Effects of Strength Training and Detraining on Children. J. Strength Cond. Res. 1996, 10, 109–114. [Google Scholar] [CrossRef]
- Wright, M.F.; Laas, M.-M. Strength Training and Metabolic Conditioning for Female Youth and Adolescent Soccer Players. Strength Cond. J. 2016, 38, 96–104. [Google Scholar] [CrossRef] [Green Version]
- Stearns, J.A.; Wohlers, B.; McHugh, T.-L.F.; Kuzik, N.; Spence, J.C. Reliability and Validity of the PLAYfun Tool with Children and Youth in Northern Canada. Meas. Phys. Educ. Exerc. Sci. 2019, 23, 47–57. [Google Scholar] [CrossRef]
- Lander, N.; Morgan, P.J.; Salmon, J.; Logan, S.W.; Barnett, L.M. The reliability and validity of an authentic motor skill assessment tool for early adolescent girls in an Australian school setting. J. Sci. Med. Sport 2017, 20, 590–594. [Google Scholar] [CrossRef] [Green Version]
- Haugen, T.; Buchheit, M. Sprint Running Performance Monitoring: Methodological and Practical Considerations. Sports Med. 2016, 46, 641–656. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Artero, E.G.; Ruiz, J.R.; Vicente-Rodriguez, G.; Bergman, P.; Hagströmer, M.; Ottevaere, C.; Nagy, E.; Konsta, O.; Rey-López, J.P.; et al. Reliability of health-related physical fitness tests in European adolescents. The HELENA Study. Int. J. Obes. 2008, 32, S49–S57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nevill, A.M.; Williams, A.M.; Boreham, C.; Wallace, E.S.; Davison, G.W.; Abt, G.; Lane, A.M.; Winter, E.M. Can we trust “Magnitude-based inference?”. J. Sports Sci. 2018, 36, 2769–2770. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G. Measures of Reliability in Sports Medicine and Science. Sports Med. 2012, 30, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Canadian Assessment of Physical Literacy. Manual for Test Administration, 2nd ed.; Canadian Assessment of Physical Literacy: Ottawa, ON, Canada, 2017; pp. 1–101. [Google Scholar]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Cook, J.A.; Julious, S.A.; Sones, W.; Hampson, L.V.; Hewitt, C.; Berlin, J.A.; Ashby, D.; Emsley, R.; Fergusson, D.A.; Walters, S.J.; et al. DELTA2 guidance on choosing the target difference and undertaking and reporting the sample size calculation for a randomised controlled trial. Trials 2018, 363, k3750. [Google Scholar]
- Pek, J.; Flora, D.B. Reporting effect sizes in original psychological research: A discussion and tutorial. Psychol. Methods 2018, 23, 208–225. [Google Scholar] [CrossRef]
- Blume, J.D.; D’Agostino McGowan, L.; Dupont, W.D.; Greevy, R.A. Second-generation p-values: Improved rigor, reproducibility, & transparency in statistical analyses. PLoS ONE 2018, 13, e0188299. [Google Scholar]
- Lakens, D.; Scheel, A.M.; Isager, P.M. Equivalence Testing for Psychological Research: A Tutorial. Adv. Methods Pract. Psychol. Sci. 2018, 1, 259–269. [Google Scholar] [CrossRef] [Green Version]
- Flanagan, S.P.; Laubach, L.L.; De Marco, G.M., Jr.; Alvarze, C.; Borchers, S.; Dressman, E.; Gorka, C.; Lauer, M.; McKelvy, A.; Metzler, M.; et al. Effects of Two Different Strength Training Modes on Motor Performance in Children. Res. Q. Exerc. Sport 2002, 73, 340–344. [Google Scholar] [CrossRef]
- Newell, K.M. What are Fundamental Motor Skills and what is Fundamental about Them? J. Mot. Learn Dev. 2020, 8, 280–314. [Google Scholar] [CrossRef]
- Arabatzi, F.; Kellis, E. Olympic Weightlifting Training Causes Different Knee Muscle–Coactivation Adaptations Compared with Traditional Weight Training. J. Strength Cond. Res. 2012, 26, 2192–2201. [Google Scholar] [CrossRef] [PubMed]
- MacNamara, Á.; Collins, D.; Giblin, S. Just let them play? Deliberate preparation as the most appropriate foundation for lifelong physical activity. Front. Psychol. 2015, 6, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Wright, M.D.; Portas, M.D.; Evans, V.J.; Weston, M. The Effectiveness of 4 Weeks of Fundamental Movement Training on Functional Movement Screen and Physiological Performance in Physically Active Children. J. Strength Cond. Res. 2015, 29, 254–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curlik, D.M., 2nd; Shors, T.J. Training your brain: Do mental and physical (MAP) training enhance cognition through the process of neurogenesis in the hippocampus? Neuropharmacology 2013, 64, 506–514. [Google Scholar] [CrossRef]
- Duncan, M.; Cunningham, A.; Eyre, E. A combined movement and story-telling intervention enhances motor competence and language ability in pre-schoolers to a greater extent than movement or story-telling alone. Eur. Phys. Educ. Rev. 2017, 25, 221–235. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | CON (n = 21; 48% F) | FMS (n = 18; 50% F) | FMS+ (n = 20; 60% F) |
|---|---|---|---|
| Stature (cm) | 140.8 ± 7.3 | 147.6 ± 7.0 | 147.9 ± 5.8 |
| Mass (kg) | 37.2 ± 7.8 | 44.7 ± 10.9 | 38.9 ± 6.7 |
| Age (years) | 10.4 ± 0.3 | 11.3 ± 0.3 | 11.2 ± 0.2 |
| Warm-Up (10 Min) | Activity 2 (10 Min) | Activity 3 (10 Min) | Activity 4 (15 Min) | Activity 5 (15 Min) | |
|---|---|---|---|---|---|
| Week 1 | Inchworm (2 × 15 s) Froggies (2 × 15 s) Bear Crawl (2 × 15 s) | Spots: Locomotor patterns (jump, hop, skip) on a whistle return to “the spot” and balance | Skipping with ropes Over—Under hurdle Ball roll and sprint | Throwing + catch to a wall. Progression—Distance from wall or one-hand catch | Football dribble (gates) |
| Week 2 | Crab walk (2 × 30 s) Spiderman (2 × 30 s) Flamingo(×30 EL) | Balance stuck in the mud (single leg stand—Freed by high 5) | Skipping with ropes Over—Under hurdle Ball roll and sprint | Throw “over the river” to a partner. Progress under to over arm throw. Two to one-hand catch | Dribble around cones and shoot for goal |
| Week 3 | Bunny hops (2 × 15 s) Inchworm (2 × 15 s) Bear Crawl (3 × 30 s) | Balance stuck in the mud (single leg stand—Freed by high 5) | Ladder steps Side-ways over—Under Ball roll and sprint | As above with different size balls | Passing a football in groups of 4 Dribble around cones and pass back |
| Week 4 | Froggies (2 × 15 s) Spiderman (2 × 15 s) Bear Crawl (3 × 30 s) | Bean bag throw and catch (standing on one leg) | Ladder steps Side-ways over—Under Ball roll and sprint | Throwing + catch to a wall. Hoop throws Progression—As above | Passing a football in groups of 4 (introduce defender) Dribble around cones and shoot for goal on command |
| Warm-Up (10 Min) | Activity 2 (10 Min) | Activity 3 (10 Min) | Activity 4 (15 Min) | Activity 5 (15 Min) | |
|---|---|---|---|---|---|
| Week 1 | Inchworm (2 × 15 s) Froggies (2 × 15 s) Bear Crawl (2 × 15 s) | Jumping and landing games (resistance band) | Skipping with ropes Over—Under hurdle Ball roll and sprint | Body weight squat 4 × 10 Squat ball throws with jump | Lung walks with leg drive 4 × 10 Football dribble (gates) |
| Week 2 | Crab walk (2 × 30 s) Spiderman (2 × 30 s) Flamingo (×30 EL) | Jumping and landing games (resistance band) | Skipping with ropes Over—Under hurdle Ball roll and sprint | Body weight squat 4 × 10 Squat ball throws with jump (beanbag to self) | Hip raises on beaches 2 × 10 each leg Dribble around cones and shoot for goal |
| Week 3 | Bunny hops (2 × 15 s) Inchworm (2 × 15 s) Bear Crawl (3 × 30 s) | Hopping into hoops Low hurdle jumps Stuck in the Mud | Ladder steps Side-ways over—Under Ball roll and sprint | Squat (1 kg med ball) 4 × 10 Squat ball throws with jump (1 kg) | Press ups 4 × 10 Dribble around cones and pass back |
| Week 4 | Froggies (2 × 15 s) Spiderman (2 × 15 s) Bear Crawl (3 × 30 s) | Hopping into hoops Low hurdle jumps Stuck in the Mud | Ladder steps Side-ways over—Under Ball roll and sprint | Squat (2 kg med ball) 4 × 10 Squat ball throws with jump (1 kg) | Lung walks with leg drive 4 × 10 Dribble around cones and shoot for goal on command |
| Outcome Measure | Control | FMS | FMS+ | |
|---|---|---|---|---|
| CAMSA (AU) | Baseline | 18.1 ± 4.2 | 14.7 ± 2.7 | 19.2 ± 4.3 |
| Post | 18.0 ± 3.5 | 20.6 ± 2.5 | 22.2 ± 3.5 | |
| CMJ (cm) | Baseline | 18.9 ± 5.8 | 17.1 ± 4.6 | 22.3 ± 4.7 |
| Post | 15.6 ± 4.5 | 15.9 ± 3.6 | 22.4 ± 4.8 | |
| 40 m Time (s) | Baseline | 6.3 ± 1.0 | 6.3 ± 0.5 | 6.0 ± 0.6 |
| Post | 6.3 ± 0.8 | 6.6 ± 0.7 | 5.9 ± 0.7 | |
| Grip L (kg) | Baseline | 13.0 ± 3.1 | 16.4 ± 3.2 | 14.9 ± 4.2 |
| Post | 13.7 ± 2.8 | 15.8 ± 3.1 | 15.2 ± 4.7 | |
| Grip R (kg) | Baseline | 13.0 ± 3.1 | 16.4 ± 3.4 | 16.1 ± 4.3 |
| Post | 13.7 ± 2.8 | 16.7 ± 3.0 | 16.4 ± 4.9 |
| Change in the Mean (95% CI) | Typical Error (95% CI) | ICC3,1 (95% CI) | |
|---|---|---|---|
| CAMSA (AU) | 0.0 (−1.3, 1.3) | 2.0 (1.6, 2.9) | 0.73 (0.44, 0.88) |
| CMJ (%) | −16 (−22, −10) | 12 (9.4, 18) | 0.88 (0.74, 0.95) |
| 40 m Run (%) | 0.1 (−3.2, 3.5) | 5.5 (4.2, 7.9) | 0.86 (0.69, 0.94) |
| Grip Left (%) | 6.1 (1.1, 11) | 8.0 (6.1, 12) | 0.91 (0.79, 0.96) |
| Grip Right (%) | 2.1 (−2.2, 6.5) | 7.1] (5.4, 10) | 0.90 (0.76, 0.96) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grainger, F.; Innerd, A.; Graham, M.; Wright, M. Integrated Strength and Fundamental Movement Skill Training in Children: A Pilot Study. Children 2020, 7, 161. https://doi.org/10.3390/children7100161
Grainger F, Innerd A, Graham M, Wright M. Integrated Strength and Fundamental Movement Skill Training in Children: A Pilot Study. Children. 2020; 7(10):161. https://doi.org/10.3390/children7100161
Chicago/Turabian StyleGrainger, Fay, Alison Innerd, Michael Graham, and Matthew Wright. 2020. "Integrated Strength and Fundamental Movement Skill Training in Children: A Pilot Study" Children 7, no. 10: 161. https://doi.org/10.3390/children7100161