Implementation of a Competency-Based, Interdisciplinary Pediatric Palliative Care Curriculum Using Content and Format Preferred by Pediatric Residents

Abstract
:1. Introduction
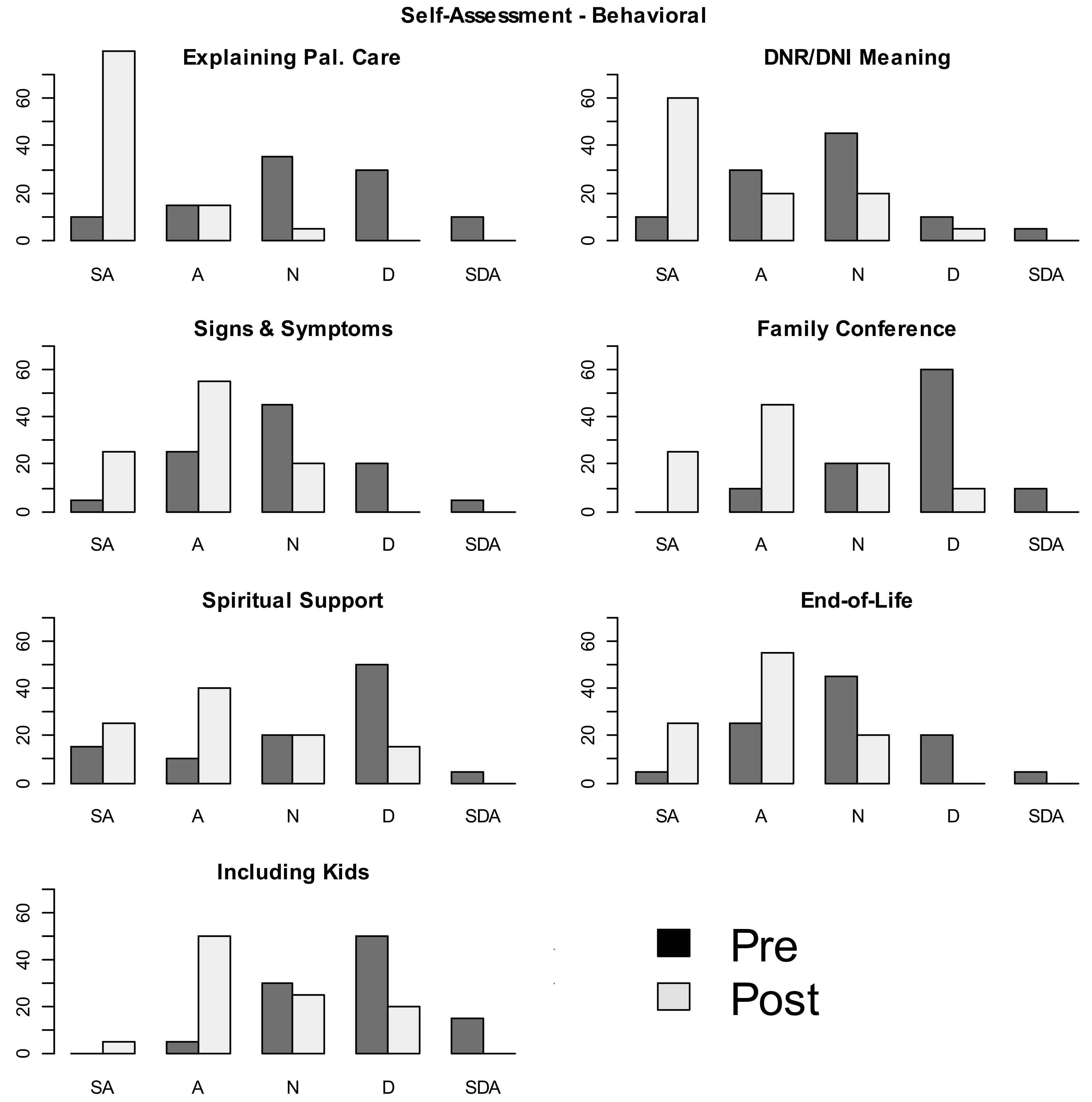
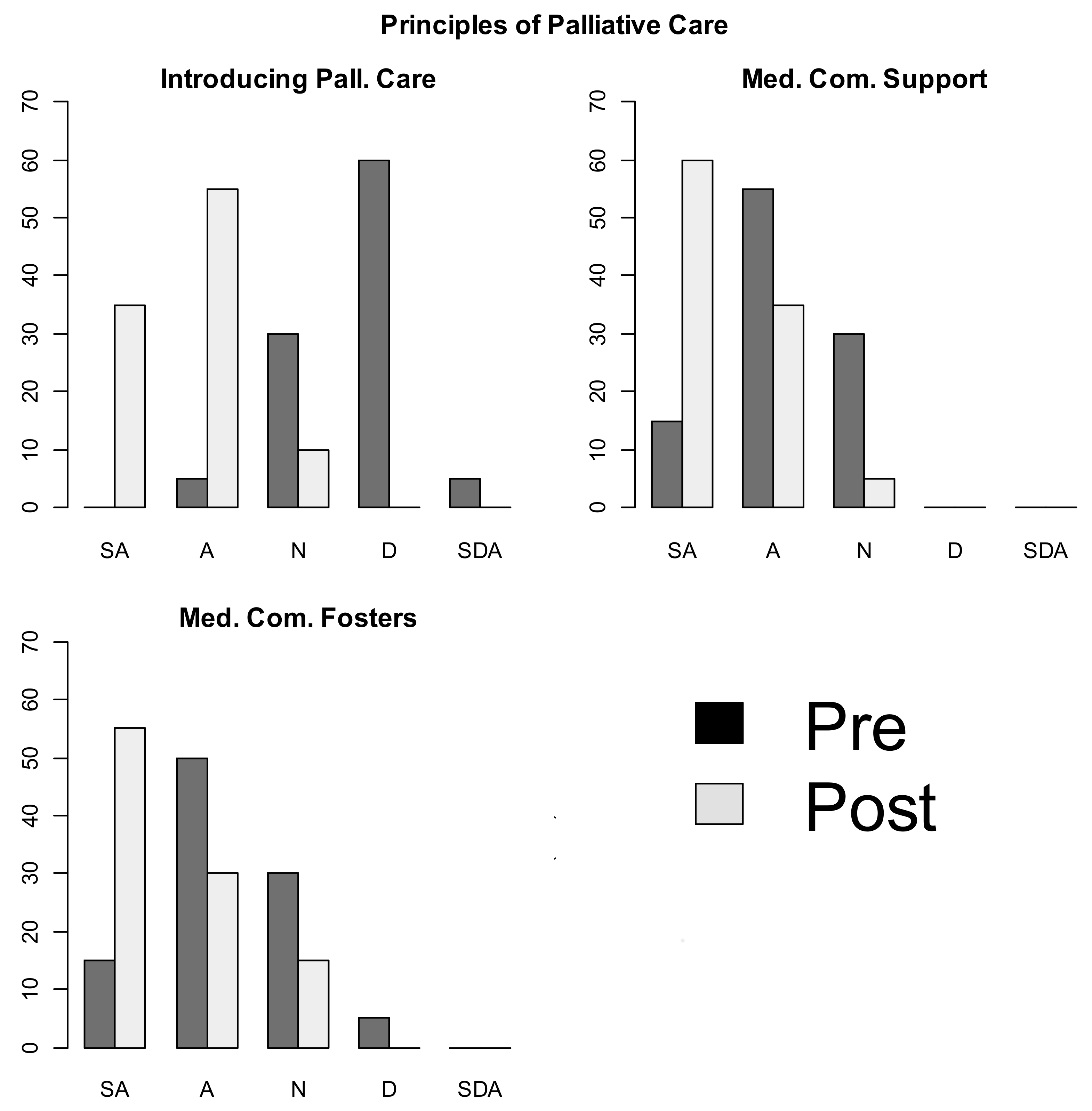
- Self-efficacy: the pediatric resident feels confident introducing principles of primary palliative care.
- Behavioral capability: the pediatric resident believes he/she can obtain the knowledge and skill to integrative palliative care principles as part of his/her training.
- Intentions (proximal goals): the pediatric resident intends to incorporate palliative care principles into patient care.
- Situation (perceived environment): the pediatric resident perceives opportunities for integrating palliative care into patient care.
- Social support: the training setting encourages the pediatric resident to consider palliative care principles in patient care and fosters a learner applying palliative care principles during residency years.
- Outcome expectations: the pediatric resident believes exposure to palliative care principles improves patient care (professional development) and enhances sense of resiliency (personal wellness).
- Expectancies: the learning community places value on the potential outcome of palliative care principles for patient care.
2. Materials and Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A. Pediatric Pal Care Power Hour Learning Series Content
- Delivering hard news with children and families (discussing pediatric prognosis).
- Discussing and documenting goals of care to include child’s code status.
- Integrative therapies and staff self-care/resilience (mindfulness, guided imagery, massage therapy, tai chi, reflexology, Healing Touch and Reiki principles); co-taught with integrative therapists.
- Pediatric complex pain control with pharmaceutical focus (adjuvant therapies for pain, opiate selection and rotation); co-taught with acute pain service and anesthesiology team.
- Treatment of respiratory symptoms at a child’s end of life (secretions, dyspnea); co-taught with pediatric respiratory therapy team.
- Treatment of pediatric gastrointestinal symptoms at end of life (constipation, malignant bowel obstruction, anorexia, cachexia); co-taught with gastrointestinal nurse practitioner.
- Treatment of pediatric neurologic symptoms at end of life (agitation, delirium, anxiety); co-taught with pediatric psychiatry team.
- Treatment of pediatric dermatologic symptoms at end of life (intractable pruritis, wound care, skin breakdown); co-taught with wound care team.
- Recognizing and preparing for a child’s imminent death (anticipatory guidance on physical changes).
- Existential and spiritual distress in children and families with a focus on cultural respect; co-taught with spiritual ministry team.
- Pediatric home hospice care; co-taught with community hospice representatives.
- Bereavement care for siblings, grandparents, and child’s peers; co-taught with bereaved parent panel and with grief counselors.
References
- Denney-Koelsch, E.M.; Horowitz, R.; Quill, T.; Baldwin, C.D. An Integrated, Developmental Four-Year Medical School Curriculum in Palliative Care: A Longitudinal Content Evaluation Based on National Competency Standards. J. Palliat. Med. 2018, 21, 1221–1233. [Google Scholar] [CrossRef] [PubMed]
- Morrison, L.J.; Thompson, B.M.; Gill, A.C. A required third-year medical student palliative care curriculum impacts knowledge and attitudes. J. Palliat. Med. 2012, 15, 784–789. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.L.; Friederici, J.; Goff, S.L. The impact of a palliative care team on residents' experiences and comfort levels with pediatric palliative care. J. Palliat. Med. 2014, 17, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, J.D.; Chamberlain, L.J.; Palmer, L.; Contro, N.; Sourkes, B.; Sectish, T.C. Introduction of a pediatric palliative care curriculum for pediatric residents. J. Palliat. Med. 2008, 11, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, K.G.; Chittenden, E.H.; Sullivan, A.M.; Periyakoil, V.S.; Morrison, L.J.; Carey, E.C.; Sanchez-Reilly, S.; Block, S.D. Raising the bar for the care of seriously ill patients: Results of a national survey to define essential palliative care competencies for medical students and residents. Acad. Med. 2014, 89, 1024–1031. [Google Scholar] [CrossRef] [PubMed]
- Oya, H.; Matoba, M.; Murakami, S.; Ohshiro, T.; Kishino, T.; Satoh, Y.; Tsukahara, T.; Hori, S.; Maeda, M.; Makino, T.; et al. Mandatory palliative care education for surgical residents: Initial focus on teaching pain management. Jpn. Clin. Oncol. 2013, 43, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Schunk, D.H.; Pajares, F. The development of academic self-efficacy. In Development of achievement motivation; Wigfield, A., Eccles, J., Eds.; Academic Press: San Diego, CA, USA, 2002; pp. 16–31. [Google Scholar]
- Bandura, A. Social cognitive theory: An agentive perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Klick, J.C.; Friebert, S.; Hutton, N.; Osenga, K.; Pituch, K.J.; Vesel, T.; Weidner, N.; Block, S.D.; Morrison, L.J.; American Board of Hospice and Palliative Medicine Competencies Work Group. Developing competencies for pediatric hospice and palliative medicine. Pediatrics 2014, 134, e167–e1677. [Google Scholar] [CrossRef] [PubMed]
- Dillman, D.; Smyth, J.; Christian, L. Internet, Mail, and Mixed-Mode Surveys: The Tailored Design Method, 3rd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2009. [Google Scholar]
- Hall, E.; Chai, W.; Koszewski, W.; Albrecht, J. Development and validation of a social cognitive theory-based survey for elementary nutrition education program. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 47. [Google Scholar] [CrossRef] [PubMed]
- Peng, N.H.; Lee, C.H.; Lee, M.C.; Huang, L.C.; Chang, Y.C.; DeSwarte-Wallace, J. Effectiveness of Pediatric Palliative Care Education on Pediatric Clinicians. West. J. Nurs. Res. 2017, 39, 1624–1638. [Google Scholar] [CrossRef] [PubMed]
- Kato, Y.; Akiyama, M.; Itoh, F.; Ida, H. A study investigating the need and impact of pediatric palliative care education on undergraduate medical students in Japan. J. Palliat. Med. 2011, 14, 560–562. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.; Gibbins, J.; Paes, P.; Adams, A.; Chandratilake, M.; Gishen, F.; Lodge, P.; Wee, B.; Barclay, S. Palliative care education for medical students: Differences in course evolution, organisation, evaluation and funding: A survey of all UK medical schools. Palliat. Med. 2017, 31, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, D.; Heah, R.; Patten, S.; Ward, H. Palliative Care in Undergraduate Medical Education-How Far Have We Come? Am. J. Hosp. Palliat. Care 2017, 34, 762–773. [Google Scholar] [CrossRef] [PubMed]
- Moody, K.; McHugh, M.; Baker, R.; Cohen, H.; Pinto, P.; Deutsch, S.; Santizo, R.O.; Schechter, M.; Fausto, J.; Joo, P. Providing Pediatric Palliative Care Education Using Problem-Based Learning. J. Palliat. Med. 2018, 21, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Michelson, K.N.; Ryan, A.D.; Jovanovic, B.; Frader, J. Pediatric residents' and fellows' perspectives on palliative care education. J. Palliat. Med. 2009, 12, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Kolarik, R.C.; Walker, G.; Arnold, R.M. Pediatric resident education in palliative care: A needs assessment. Pediatrics 2006, 117, 1949–1954. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Domain | Principles of Palliative Care | Timing | Count (%) | ||||
|---|---|---|---|---|---|---|---|
| SA | A | N | DA | SDA | |||
| Attitude | I feel confident introducing principles of palliative care | Pre | 0 (0) | 1 (5) | 6 (30) | 12 (60) | 1 (5) |
| Post | 7 (35) | 11 (55) | 2 (10) | 0 (0) | 0 (0) | ||
| Attitude | I believe I can obtain the knowledge and skills to integrate palliative care principles | Pre | 4 (20) | 12 (60) | 3 (15) | 1 (5) | 0 (0) |
| Post | 8 (40) | 10 (50) | 2 (10) | 0 (0) | 0 (0) | ||
| Attitude | In the next 3 months, I intend to incorporate palliative care principles in my care for patients and families | Pre | 4 (20) | 13 (65) | 3 (15) | 0 (0) | 0 (0) |
| Post | 9 (45) | 9 (45) | 2 (10) | 0 (0) | 0 (0) | ||
| Attitude | I believe exposure to palliative care principles improves my care of patients and families (professional development) | Pre | 14 (70) | 4 (20) | 2 (10) | 0 (0) | 0 (0) |
| Post | 15 (75) | 4 (20) | 1 (5) | 0 (0) | 0 (0) | ||
| Attitude | I believe exposure to palliative care principles enhances my own sense of resiliency (personal wellness) | Pre | 10 (50) | 9 (45) | 1 (5) | 0 (0) | 0 (0) |
| Post | 16 (80) | 4 (20) | 0 (0) | 0 (0) | 0 (0) | ||
| Attitude | I place value on the potential outcome of palliative care principles for patient care | Pre | 9 (45) | 10 (50) | 1 (5) | 0 (0) | 0 (0) |
| Post | 15 (75) | 5 (25) | 0 (0) | 0 (0) | 0 (0) | ||
| Environment | The medical community supports me in my learning about palliative care | Pre | 3 (15) | 11 (55) | 6 (30) | 0 (0) | 0 (0) |
| Post | 12 (60) | 7 (35) | 1 (5) | 0 (0) | 0 (0) | ||
| Environment | The medical community fosters my applying palliative care principles | Pre | 3 (15) | 10 (50) | 6 (30) | 1 (5) | 0 (0) |
| Post | 11 (55) | 6 (30) | 3 (15) | 0 (0) | 0 (0) | ||
| Environment | I perceive opportunities for integrating palliative care for children and families | Pre | 5 (25) | 12 (60) | 2 (10) | 1 (5) | 0 (0) |
| Post | 11 (55) | 8 (40) | 0 (0) | 1 (5) | 0 (0) | ||
| Environment | This hospital encourages me to consider palliative care principles in my care of patients and families | Pre | 3 (15) | 9 (45) | 8 (40) | 0 (0) | 0 (0) |
| Post | 10 (50) | 8 (40) | 2 (10) | 0 (0) | 0 (0) | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weaver, M.S.; Wichman, C. Implementation of a Competency-Based, Interdisciplinary Pediatric Palliative Care Curriculum Using Content and Format Preferred by Pediatric Residents. Children 2018, 5, 156. https://doi.org/10.3390/children5120156
Weaver MS, Wichman C. Implementation of a Competency-Based, Interdisciplinary Pediatric Palliative Care Curriculum Using Content and Format Preferred by Pediatric Residents. Children. 2018; 5(12):156. https://doi.org/10.3390/children5120156
Chicago/Turabian StyleWeaver, Meaghann S., and Christopher Wichman. 2018. "Implementation of a Competency-Based, Interdisciplinary Pediatric Palliative Care Curriculum Using Content and Format Preferred by Pediatric Residents" Children 5, no. 12: 156. https://doi.org/10.3390/children5120156