
Examining the Utility of the Early Childhood Development Index (ECDI) among Children in the Nigeria Context

 , , , ,
, , , ,
Abstract
:1. Introduction
Review of the Literature
- i.
- There is an underlying factorial structure of the ECDI items.
- ii.
- The ECDI demonstrates acceptable power in distinguishing between children whose development is on track and those who are not.
2. Materials and Methods
2.1. Study Design and Sample
2.2. Measures
2.3. Analytical Approach
3. Results
3.1. Demographic Statistics
3.2. Correlation
3.3. Internal Consistency
3.4. The Kuder–Richardson Coefficient of Reliability (KR-20)
3.5. Measure of Sampling Adequacy (MSA)
3.6. EFA Results
3.7. Uni-Dimensionality and CFA Results
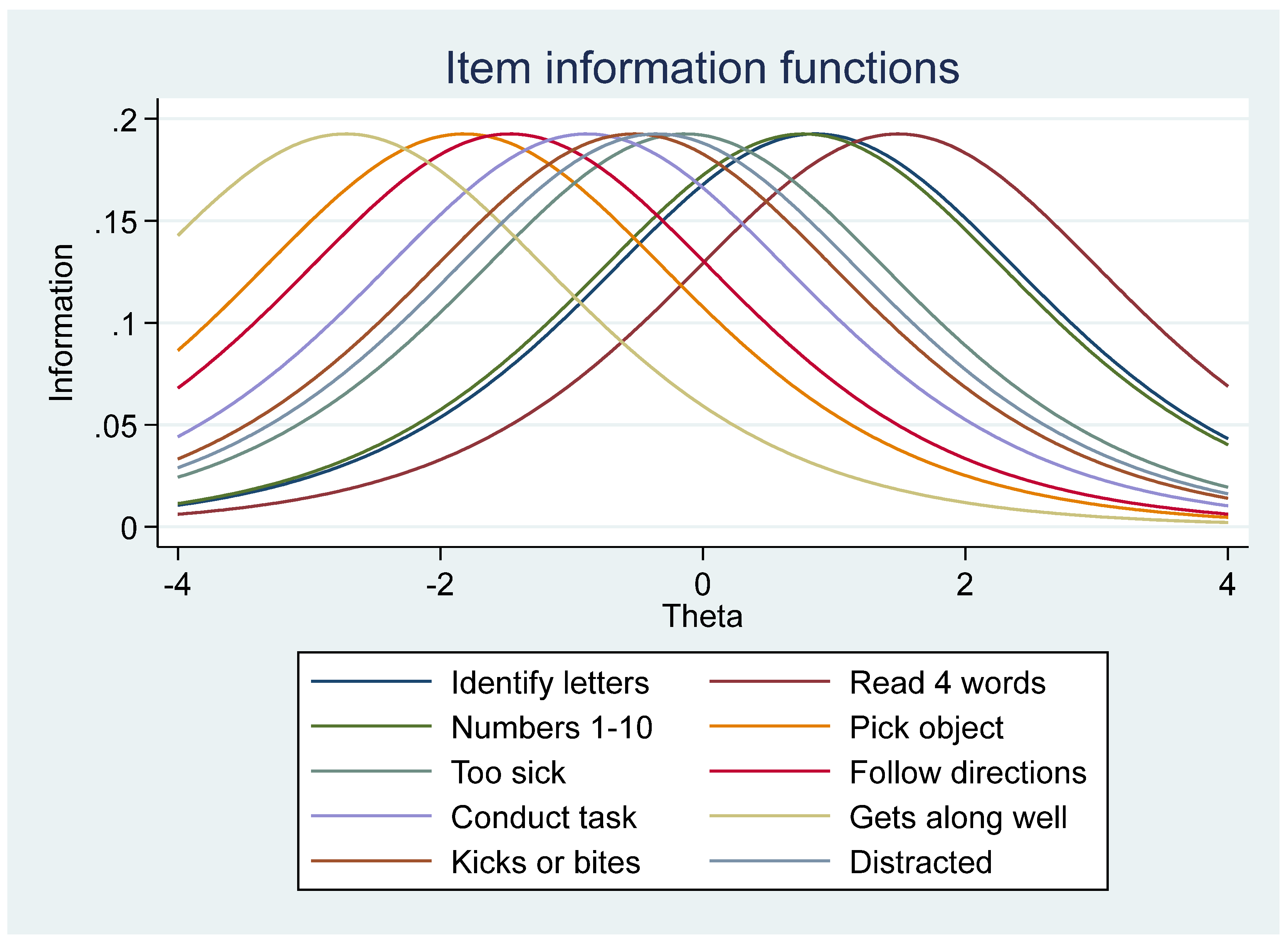
3.8. IRT Modeling
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Black, M.M.; Walker, S.P.; Fernald, L.C.H.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J.; et al. Early childhood development coming of age: Science through the life course. Lancet 2017, 389, 77–90. [Google Scholar] [CrossRef]
- Kang, Y.; Aguayo, V.M.; Campbell, R.K.; West, K.P. Association between stunting and early childhood development among children aged 36–59 months in South Asia. Matern. Child Nutr. 2018, 14, e12684. [Google Scholar] [CrossRef]
- Engle, P.L.; Black, M.M.; Behrman, J.R.; Cabral de Mello, M.; Gertler, P.J.; Kapiriri, L.; Martorell, R.; Young, M.E.; International Child Development Steering Group. Strategies to avoid the loss of developmental potential in more than 200 million children in the developing world. Lancet 2007, 369, 229–242. [Google Scholar] [CrossRef] [PubMed]
- McCoy, D.C.; Peet, E.D.; Ezzati, M.; Danaei, G.; Black, M.M.; Sudfeld, C.R.; Fawzi, W.; Fink, G. Early childhood developmental status in low- and middle-income countries: National, regional, and global prevalence estimates using predictive modeling. PLoS Med. 2016, 13, e1002034. [Google Scholar] [CrossRef] [PubMed]
- McCoy, D.C.; Peet, E.D.; Ezzati, M.; Danaei, G.; Black, M.M.; Sudfeld, C.R.; Fawzi, W.; Fink, G. Correction: Early childhood developmental status in low- and middle-income countries: National, regional, and global prevalence estimates using predictive modeling. PLoS Med. 2017, 14, e1002233. [Google Scholar] [CrossRef]
- National Population Commission [Nigeria]. Nigeria Demographic and Health Survey 2018; ICF: Abuja, Nigeria; Rockville, MD, USA, 2019.
- Betancourt, T.S. Using mixed methods to plan and evaluate mental health programs for war-affected children in sub-Saharan Africa. In The Culture of Mental Illness and Psychiatric Practice in Africa; Akyeampong, E., Hill, A.G., Kleinman, A., Eds.; Indiana University Press: Bloomington, IN, USA, 2015; pp. 311–332. [Google Scholar]
- American Academy of Pediatrics. Supplemental appendix S12: Mental health screening and assessment tools for primary care. Pediatrics 2010, 125, S173–S192. [Google Scholar] [CrossRef]
- Ringwalt, S. Developmental Screening, and Assessment Instruments with an Emphasis on Social and Emotional Development for Young Children from Ages Birth through Five. National Early Childhood Technical Assistance Center. 2008. Available online: http://eric.ed.gov/?id=ED505971 (accessed on 10 January 2024).
- Loizillon, A.N.; Petrowski, P.; Britto, P.; Cappa, C. Development of the Early Childhood Development Index in MICS Surveys. MICS Methodological Papers, No. 6., Data and Analytics Section, Division of Data, Research and Policy. New York. 2017. Available online: Mics.unicef.org (accessed on 3 December 2018).
- Cappa, C.; Petrowski, N.; De Castro, E.F.; Geisen, E.; LeBaron, P.; Allen-Leigh, B.; Place, J.M.; Scanlon, P.J. Identifying and minimizing errors in the measurement of early childhood development: Lessons learned from the cognitive testing of the ECDI2030. Int. J. Environ. Res. Public Health 2021, 18, 12181. [Google Scholar] [CrossRef]
- Fernald, L.C.H.; Kariger, P.; Engle, P.; Raikes, A. Examining early child development in low-income countries. In A Toolkit for the Assessment of Children in the First Five Years of Life; World Bank: Washington, DC, USA, 2009. [Google Scholar]
- Braveman, P.; Barclay, C. Health disparities beginning in childhood: A life-course perspective. Pediatrics 2009, 124 (Suppl. S3), S163–S175. [Google Scholar] [CrossRef]
- Monk, C.; Georgieff, M.K.; Osterholm, E.A. Maternal prenatal distress, and poor nutrition–mutually influencing risk factors affecting infant neurocognitive development. J. Child Psychol. Psychiatry 2012, 54, 115–130. [Google Scholar] [CrossRef] [PubMed]
- Halle, T.G.; Darling-Churchill, K.E. Review of measures of social and emotional development. J. Appl. Dev. Psychol. 2016, 45, 8–18. [Google Scholar] [CrossRef]
- Ertem, I.O. Developmental Difficulties in Early Childhood: Prevention, Early Identification, Assessment and Intervention in Low- and Middle-Income Countries: A Review; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Fernald, L.C.H.; Pitchik, H.O. The necessity of using direct measures of child development. Lancet Glob. Health 2019, 7, e1300–e1301. [Google Scholar] [CrossRef]
- Uchitel, J.; Alden, E.; Bhutta, Z.A.; Goldhagen, J.; Narayan, A.P.; Raman, S.; Spencer, N.; Wertlieb, D.; Wettach, J.; Woolfenden, S.; et al. The rights of children for optimal development and nurturing care. Pediatrics 2019, 144, e20190487. [Google Scholar] [CrossRef]
- Britto, P.R.; Ulkuer, N. Child development in developing countries: Child rights and policy implications. Child Dev. 2012, 83, 92–103. [Google Scholar] [CrossRef]
- Boggs, D.; Milner, K.M.; Chandna, J.; Black, M.; Cavallera, V.; Dua, T.; Fink, G.; Kc, A.; Grantham-McGregor, S.; Hamadani, J.; et al. Rating early child development outcome measurement tools for routine health programme use. Arch. Dis. Child. 2019, 104, S22–S33. [Google Scholar] [CrossRef]
- UNICEF. Early Childhood. ECD Monitoring. 2013. Available online: https://www.unicef.org/earlychildhood/index_69846.html (accessed on 15 June 2020).
- National Bureau of Statistics (NBS); United Nations Children’s Fund (UNICEF). 2017 Multiple Indicator Cluster Survey 2016–17: Survey Findings Report; NBS: Abuja, Nigeria, 2017. [Google Scholar]
- UNICEF. UNICEF Annual Report 2017 Nigeria. Abuja. 2017. Available online: https://www.unicef.org/about/annualreport/files/Nigeria_2017_COAR.pdf (accessed on 16 May 2019).
- Babatunde, A.O. Oil exploitation, local economy, and conflict in the oil-bearing areas of Nigeria’s Niger Delta. In Society of Petroleum Engineers Nigeria Annual International Conference and Exhibition 2011; NBS: Abuja, Nigeria, 2011. [Google Scholar]
- Gebremichael, M.; Kifle, A.A.; Kidane, A.; Wendyam, H.; Fitiwi, M.; Shariff, Z.S. Nigeria conflict insight. In Institute Peace and Security Studies; Addis Ababa University: Addis Ababa, Ethiopia, 2018. [Google Scholar]
- Howell, E.; Waidmann, T.; Holla, N.; Birdsall, N.; Jiang, K. The Impact of Civil Conflict on Child Malnutrition and Mortality, Nigeria, 2002–2013. 2018. Report No.: 494. Available online: www.cgdev.org (accessed on 14 December 2023).
- Kah, H.K. “Boko Haram Is Losing, But So Is Food Production”: Conflict and Food Insecurity in Nigeria and Cameroon. Afr. Dev. 2017, XLII, 177–196. Available online: https://about.jstor.org/terms (accessed on 18 October 2018).
- National Bureau of Statistics (NBS); United Nations Children’s Fund (UNICEF). Multiple Indicator Cluster Survey 2021, Statistical Snapshot Report; NBS: Abuja, Nigeria, 2022. [Google Scholar]
- Goldstein, J.M.; Simpson, J.C. Validity: Definitions and applications to psychiatric research. In Textbook in Psychiatric Epidemiology, 2nd ed.; Tsuang, M.T., Tohen, M., Eds.; Wiley-Liss: New York, NY, USA, 2002; pp. 149–163. [Google Scholar]
- Willse, J.T. Classical test theory. In Encyclopedia of Research Design; Salkind, N.J., Ed.; SAGE Publications Inc.: Thousand Oaks, CA, USA, 2010; pp. 150–153. [Google Scholar]
- Willoughby, M.T.; Wirth, R.; Blair, C.B. Contributions of modern measurement theory to measuring executive function in early childhood: An empirical demonstration. J. Exp. Child Psychol. 2011, 108, 414–435. [Google Scholar] [CrossRef] [PubMed]
- DeVellis, R.F. Classical test theory. Med. Care. 2006, 44, S50–S59. [Google Scholar] [CrossRef] [PubMed]
- Baker, F.B. The Basics of Item Response Theory; U.S. Department of Education: Washington, DC, USA, 2001.
- Steinberg, L.; Thissen, D. Item response theory. In The Oxford Handbook of Research Strategies for Clinical Psychology; Comer, J.S., Kendall, P.C., Eds.; Oxford University Press: Oxford, UK, 2013; pp. 150–171. [Google Scholar]
- Yang, H.; Chen, F.; Liu, X.; Xin, T. An item response theory analysis of DSM-5 heroin use disorder in a clinical sample of Chinese adolescents. Front. Psychol. 2019, 10, 2209. [Google Scholar] [CrossRef] [PubMed]
- Forrest, C.B.; Bevans, K.B.; Filus, A.; Devine, J.; Becker, B.D.; Carle, A.C.; E Teneralli, R.; Moon, J.; Ravens-Sieberer, U. Assessing children’s eudaimonic well-being: The PROMIS pediatric meaning and purpose item banks. J. Pediatr. Psychol. 2019, 44, 1074–1082. [Google Scholar] [CrossRef] [PubMed]
- Stone, M.D.; Matheson, B.E.; Leventhal, A.M.; Boutelle, K.N. Development and validation of a short form children’s power of food scale. Appetite 2020, 147, 104549. [Google Scholar] [CrossRef] [PubMed]
- Şahin, A.; Anıl, D. The effects of test length and sample size on item parameters in item response theory. Educ. Sci. Theory Pract. 2017, 17, 321–335. [Google Scholar]
- Schreiber, J.B.; Nora, A.; Stage, F.K.; Barlow, E.A.; King, J. Reporting structural equation modeling and confirmatory factor analysis: A review. J. Educ. Res. 2006, 99, 323–338. [Google Scholar] [CrossRef]
- Michalopoulos, L.M.; Meinhart, M.; Barton, S.M.; Kuhn, J.; Mukasa, M.N.; Namuwonge, F.; Feiring, C.; Ssewamala, F.M. Adaptation and validation of the shame questionnaire among Ugandan youth living with HIV. Child Indic. Res. 2019, 12, 1023–1042. [Google Scholar] [CrossRef] [PubMed]
- Padilla, M.A.; Divers, J. A comparison of composite reliability estimators: Coefficient omega confidence intervals in the current literature. Educ. Psychol. Meas. 2016, 76, 436–453. [Google Scholar] [CrossRef]
- Villodas, M.L.; Nebbitt, V.E.; Lombe, M.; Yu, M.; Foell, A.; McCoy, H.; Enelamah, N.V. Assessing the modified neighborhood cohesion instrument among African American adolescents living in public housing: An exploratory and confirmatory factor analysis. J. Soc. Soc. Work. Res. 2023, 14, 291–312. [Google Scholar] [CrossRef]
- Enelamah, N.V.; Lombe, M.; Betancourt, T.S.; Williams, D.R.; Shen, C. Variations in risk, resilience, and protective factors for cognitive and socioemotional development among 3- to 4-year-old children in Nigeria: A multilevel modeling. Early Child. Res. Q. 2023, 64, 162–173. [Google Scholar] [CrossRef]
- Linacre, J.M. Rasch Estimation: Iteration and Convergence. Rasch Measurement Transactions. 1987, Volume 1, pp. 7–8. Available online: https://www.rasch.org/rmt/rmt11b.htm (accessed on 21 June 2020).
- Kralik, R. The influence of family and school in shaping the values of children and young people in the theory of free time and pedagogy. J. Educ. Cult. Soc. 2023, 14, 249–268. [Google Scholar] [CrossRef]
- Minarovičová, K. Social work with families of children placed in institutional care (Short Communication). Acta Missiologica 2021, 15, 179–183. [Google Scholar]
- Bornstein, M.H.; Britto, P.R.; Nonoyama-Tarumi, Y.; Ota, Y.; Petrovic, O.; Putnick, D.L. Child development in developing countries: Introduction and methods. Child Dev. 2012, 83, 16–31. [Google Scholar] [CrossRef]
- UNICEF. A New Tool to Measure SDG Indicator 4.2.1; UNICEF: New York, NY, USA, 2022. [Google Scholar]
- Van Ommeren, M. Validity issues in transcultural epidemiology. Br. J. Psychiatry 2003, 182, 376–378. [Google Scholar] [CrossRef] [PubMed]
- Emerson, E.; Savage, A.; Llewellyn, G. Significant cognitive delay among 3- to 4-year-old children in low- and middle-income countries: Prevalence estimates and potential impact of preventative interventions. Leuk. Res. 2018, 47, 1465–1474. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| 10-Item ECDI | |
|---|---|
| Literacy–numeracy | EC8. Can (name) identify or name at least ten letters of the alphabet? |
| EC9. Can (name) read at least four simple, popular words? | |
| EC10. Does (name) know the name and recognize the symbol of all numbers from 1 to 10 most of the time? | |
| Physical | EC11. Can (name) pick up a small object with two fingers, like a stick or a rock, from the ground? |
| EC12. Is (name) sometimes too sick to play? | |
| Approaches to learning | EC13. Does (name) follow the simple directions on how to do something correctly? |
| EC14. When given something to do, is (name) able to do it independently? | |
| Socioemotional | EC15. Does (name) get along well with other children? |
| EC16. Does (name) kick, bite, or hit other children or adults? | |
| EC17. Does (name) get distracted easily? | |
| Characteristic | n (%) |
|---|---|
| Child’s Age | |
| 3 years | 5643 (51) |
| 4 years | 5430 (49) |
| Child’s Gender | |
| Male | 5632 (51) |
| Female | 5441 (49) |
| Household Dwelling | |
| Rural | 8140 (74) |
| Urban | 2933 (26) |
| Mother’s Age | |
| 15–19 years | 156 (2) |
| 20–29 years | 4016 (39) |
| 30–39 years | 4425 (44) |
| 40–49 years | 1556 (15) |
| Mother’s Educational Level | |
| None | 3141 (28) |
| Primary/Non-formal | 4123 (37) |
| Secondary/Higher | 3808 (34) |
| ECDI Items | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Literacy–numeracy | 1 | Identify letters | 1 | |||||||||
| 2 | Read four words | 0.62 | 1 | |||||||||
| 3 | Numbers 1 to 10 | 0.76 | 0.60 | 1 | ||||||||
| Physical | 4 | Pick object | 0.20 | 0.18 | 0.21 | 1 | ||||||
| 5 | Too sick c | 0.03 | 0.02 | 0.06 | −0.11 | 1 | ||||||
| Cognitive–approaches | 6 | Follow direction | 0.21 | 0.18 | 0.21 | 0.31 | −0.07 | 1 | ||||
| 7 | Conducts a task | 0.18 | 0.16 | 0.19 | 0.25 | −0.04 | 0.56 | 1 | ||||
| Socioemotional | 8 | Gets along well | 0.14 | 0.12 | 0.15 | 0.32 | −0.12 | 0.34 | 0.27 | 1 | ||
| 9 | Kicks/bites c | 0.00 | 0.01 | 0.00 | −0.09 | 0.19 | −0.07 | −0.01 | −0.10 | 1 | ||
| 10 | Distracted c | 0.02 | 0.01 | 0.01 | −0.02 | 0.20 | −0.04 | 0.01 | −0.11 | 0.25 | 1 |
| ECDI Items | Mean (SD) | KMO | SMC | COM | Overall Alpha α | Age 3 α | Age 4 α | Urban α | Rural α | Yes Edu α | No Edu α | Igbo α | Lang Yoruba α | Hausa α |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Can identify letters | 0.34 (0.47) | 0.70 | 0.64 | 0.72 | 0.58 | 0.56 | 0.58 | 0.55 | 0.59 | 0.50 | 0.58 | 0.58 | 0.57 | 0.61 |
| Read four words | 0.24 (0.43) | 0.84 | 0.45 | 0.51 | 0.60 | 0.59 | 0.60 | 0.59 | 0.61 | 0.55 | 0.59 | 0.61 | 0.61 | 0.63 |
| Numbers 1 to 10 | 0.36 (0.48) | 0.70 | 0.63 | 0.71 | 0.58 | 0.57 | 0.58 | 0.54 | 0.59 | 0.50 | 0.58 | 0.59 | 0.56 | 0.62 |
| Pick small object | 0.80 (0.40) | 0.83 | 0.16 | 0.23 | 0.66 | 0.64 | 0.66 | 0.66 | 0.65 | 0.61 | 0.59 | 0.65 | 0.65 | 0.64 |
| Too sick (re-coded) | 0.47 (0.50) | 0.66 | 0.09 | 0.17 | 0.69 | 0.67 | 0.70 | 0.68 | 0.68 | 0.63 | 0.62 | 0.69 | 0.68 | 0.67 |
| Follows directions | 0.75 (0.43) | 0.68 | 0.38 | 0.50 | 0.65 | 0.63 | 0.66 | 0.65 | 0.64 | 0.60 | 0.58 | 0.65 | 0.65 | 0.63 |
| Conducts a task | 0.66 (0.47) | 0.67 | 0.34 | 0.44 | 0.66 | 0.63 | 0.67 | 0.65 | 0.65 | 0.60 | 0.59 | 0.66 | 0.64 | 0.64 |
| Gets along well | 0.89 (0.31) | 0.79 | 0.17 | 0.25 | 0.66 | 0.64 | 0.67 | 0.67 | 0.66 | 0.62 | 0.59 | 0.67 | 0.67 | 0.65 |
| Kicks (re-coded) | 0.60 (0.49) | 0.63 | 0.10 | 0.19 | 0.69 | 0.67 | 0.69 | 0.68 | 0.66 | 0.62 | 0.62 | 0.69 | 0.68 | 0.67 |
| Distracted (re-coded) | 0.56 (0.50) | 0.58 | 0.10 | 0.20 | 0.69 | 0.67 | 0.69 | 0.67 | 0.68 | 0.61 | 0.62 | 0.70 | 0.66 | 0.66 |
| Overall | 4.6 (0.40) | 0.72 | 0.67 | 0.66 | 0.68 | 0.67 | 0.67 | 0.62 | 0.62 | 0.68 | 0.67 | 0.67 |
| ECDI Domains | ECDI Items | KMO | SMC | COM | Principal Axis Factors (paf) | |||
|---|---|---|---|---|---|---|---|---|
| Factor | Factor 1 | Factor 2 | Factor 3 | Factor 4 | ||||
| Literacy–Numeracy | Can identify letters | 0.70 | 0.64 | 0.72 | 0.85 | |||
| Read four words | 0.84 | 0.45 | 0.51 | 0.71 | ||||
| Numbers 1 to 10 | 0.70 | 0.63 | 0.71 | 0.84 | ||||
| Physical | Pick small object | 0.83 | 0.16 | 0.23 | 0.44 | |||
| Too sick c | 0.66 | 0.09 | 0.17 | 0.34 | ||||
| Cognitive–Learning | Follows directions | 0.68 | 0.38 | 0.50 | 0.64 | |||
| Conduct a task | 0.67 | 0.34 | 0.44 | 0.69 | ||||
| Socioemotional | Gets along well | 0.79 | 0.17 | 0.25 | 0.41 | |||
| Kicks or bites c | 0.63 | 0.10 | 0.19 | 0.44 | ||||
| Distracted c | 0.58 | 0.10 | 0.20 | 0.45 | ||||
| Overall | 0.72 | |||||||
| Factor Loadings | One-Factor ECDI Model | Four-Factor ECDI Model | |||
|---|---|---|---|---|---|
| (Observed -> Latent Construct) Measurement Model | Unstandardized Coefficients (SE) | Standardized Coefficients (SE) | Unstandardized Coefficients (SE) | Standardized Coefficients (SE) | |
| Literacy– Numeracy | Can identify letters | 1 *** | 0.87 (0.01) *** | 1 *** | 0.88(0.01) *** |
| Read four words | 0.69 (0.02) *** | 0.68 (0.01) *** | 0.69 (0.02) *** | 0.68 (0.01) *** | |
| Numbers 1 to 10 | 1.0 (0.02) *** | 0.87 (0.01) *** | 1.0 (0.02) *** | 0.88 (0.01) *** | |
| Physical | Pick small object | 0.26 (0.02) *** | 0.27 (0.020) *** | 1 *** | 0.67 (0.06) *** |
| Too sick (not) | 0.04 (0.02) | 0.03 (0.02) | −0.34 (0.05) *** | −0.18 (0.02) *** | |
| Cognitive– Approach | Follows directions | 0.29 (0.02) *** | 0.30 (0.02) *** | 1 *** | 0.84 (0.02) *** |
| Conducts a task | 0.27 (0.02) *** | 0.26 (0.02) *** | 0.85 (0.04) *** | 0.64 (0.06) *** | |
| Socioemotional | Gets along well | 0.13 (0.01) *** | 0.18 (0.02) *** | 1 *** | 0.63 (0.03) *** |
| Kicks or bites (not) | −0.02 (0.02) | −0.02 (0.02) | −0.54 (0.07) *** | −0.21 (0.02) *** | |
| Distracted (not) | 0.00 (0.02) | 0.00 (0.02) | −0.41 (0.06) *** | −0.16 (0.02) *** | |
| Measurement Error Variances | |||||
| Can identify letters | 0.05 (0.00) | 0.25 (0.01) | 0.05 (0.00) | 0.23 (0.01) | |
| Read four words | 0.10 (0.00) | 0.54 (0.01) | 0.10 (0.00) | 0.54 (0.01) | |
| Numbers 1 to 10 | 0.06 (0.00) | 0.25 (0.01) | 0.06 (0.00) | 0.25 (0.01) | |
| Pick small object | 0.15 (0.00) | 0.93 (0.01) | 0.09 (0.01) | 0.55 (0.07) | |
| Too sick (not) | 0.25 (0.01) | 1.0 (0.00) | 0.24 (0.01) | 0.97 (0.01) | |
| Follows directions | 0.17 (0.00) | 0.91 (0.01) | 0.06 (0.00) | 0.30 (0.03) | |
| Conducts a task | 0.21 (0.00) | 0.93 (0.01) | 0.13 (0.00) | 0.59 (0.02) | |
| Gets along well | 0.09 (0.00) | 0.97 (0.01) | 0.06 (0.00) | 0.60 (0.04) | |
| Kicks or bites (not) | 0.24 (0.01) | 1.0 (0.00) | 0.23 (0.01) | 0.96 (0.01) | |
| Distracted (not) | 0.25 (0.01) | 1.0 (0.00) | 0.24 (0.01) | 0.98 (0.01) | |
| R-Squared (Overall parameter fit) | |||||
| Can identify letters | 0.76 | 0.77 | |||
| Read four words | 0.46 | 0.68 | |||
| Numbers 1 to 10 | 0.75 | 0.75 | |||
| Pick small object | 0.07 | 0.44 | |||
| Too sick (not) | 0.00 | 0.03 | |||
| Follows directions | 0.08 | 0.70 | |||
| Conducts a task | 0.06 | 0.41 | |||
| Gets along well | 0.03 | 0.40 | |||
| Kicks or bites (not) | 0.00 | 0.04 | |||
| Distracted (not) | 0.00 | 0.02 | |||
| Overall | 0.88 | 0.99 | |||
| Fit Statistics | |||||
| Chi-squared (df) | 1600.28 (34) *** | 503.25 (29) *** | |||
| RMSEA | 0.10 | 0.067 | |||
| CFI | 0.82 | 0.94 | |||
| TLI | 0.76 | 0.91 | |||
| SRMR | 0.10 | 0.05 | |||
| CD | 0.88 | 0.99 | |||
| AIC | 37,669.56 | 36,582.54 | |||
| BIC | 37,863.18 | 36,806.23 | |||
| 1PL IRT Model Estimates | ||||
|---|---|---|---|---|
| Items | Item Definition | Yes (%) | Mean (SD) (Listwise) | Difficulty (SE) |
| 1PL overall item discrimination 0.99 (0.05) *** | ||||
| Can identify letters | Can (name) identify or name at least ten letters of the alphabet? | 34 | 0.36 (0.48) | 0.69 (0.11) *** |
| Read four words | Can (name) read at least four simple, popular words? | 24 | 0.27 (0.45) | 1.18 (0.12) *** |
| Numbers 1 to 10 | Does (name) know the name and recognize the symbol of all numbers from 1 to 10 most of the time? | 37 | 0.39 (0.49) | 0.54 (0.11) *** |
| Pick small object | Can (name) pick up a small object with two fingers, like a stick or a rock, from the ground? | 80 | 0.81 (0.40) | −1.71 (0.14) *** |
| Too sick | Is (name) sometimes too sick to play? (Re-coded) | 47 | 0.51 (50) | −0.04 (0.10) *** |
| Follows directions c | Does (name) follow the simple directions on how to do something correctly? | 75 | 0.75 (0.43) | −1.34 (0.13) *** |
| Conducts a task | When given something to do, is (name) able to do it independently? | 67 | 0.65 (0.48) | −0.75 (0.11) *** |
| Gets along well | Does (name) get along well with other children? | 89 | 0.89 (0.30) | −2.54 (0.19) *** |
| Kicks or bites c | Does (name) kick, bite, or hit other children or adults? (Re-coded) | 60 | 0.43 (0.50) | 0.37 (0.10) *** |
| Distracted c | Does (name) get distracted easily? (Re-coded) | 57 | 0.45 (0.50) | 0.24 (0.10) *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Enelamah, N.V.; Rao, S.; Lombe, M.; Yu, M.; Newransky, C.; Villodas, M.L.; Foell, A.; Nebbitt, V. Examining the Utility of the Early Childhood Development Index (ECDI) among Children in the Nigeria Context. Children 2024, 11, 361. https://doi.org/10.3390/children11030361
Enelamah NV, Rao S, Lombe M, Yu M, Newransky C, Villodas ML, Foell A, Nebbitt V. Examining the Utility of the Early Childhood Development Index (ECDI) among Children in the Nigeria Context. Children. 2024; 11(3):361. https://doi.org/10.3390/children11030361
Chicago/Turabian StyleEnelamah, Ngozi V., Smitha Rao, Margaret Lombe, Mansoo Yu, Chrisann Newransky, Melissa L. Villodas, Andrew Foell, and Von Nebbitt. 2024. "Examining the Utility of the Early Childhood Development Index (ECDI) among Children in the Nigeria Context" Children 11, no. 3: 361. https://doi.org/10.3390/children11030361