

Alterations of Nutritional Status in Children and Adolescents with Acute Lymphoblastic Leukemia
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Podpeskar, A.; Crazzolara, R.; Kropshofer, G.; Obexer, P.; Rabensteiner, E.; Michel, M.; Salvador, C. Supportive methods for childhood acute lymphoblastic leukemia then and now: A compilation for clinical practice. Front. Pediatr. 2022, 10, 980234. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Cancer Facts & Figures 2022|American Cancer Society. 2022. Available online: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2022.html (accessed on 15 January 2024).
- Henry, M.; Sung, L. Supportive care in pediatric oncology: Oncologic emergencies and management of fever and neutropenia. Pediatr. Clin. N. Am. 2015, 62, 27–46. [Google Scholar] [CrossRef] [PubMed]
- Rogers, P.C.; Barr, R.D. The relevance of nutrition to pediatric oncology: A cancer control perspective. Pediatr. Blood Cancer 2020, 67 (Suppl. S3), e28213. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization—Regional Office for the Eastern Mediterranean. WHO EMRO|Double Burden of Nutrition|Nutrition Site. Available online: https://www.emro.who.int/nutrition/double-burden-of-nutrition/index.html (accessed on 15 January 2024).
- Pedretti, L.; Massa, S.; Leardini, D.; Muratore, E.; Rahman, S.; Pession, A.; Esposito, S.; Masetti, R. Role of Nutrition in Pediatric Patients with Cancer. Nutrients 2023, 15, 710. [Google Scholar] [CrossRef] [PubMed]
- Sonowal, R.; Gupta, V. Nutritional status in children with acute lymphoblastic leukemia, and its correlation with severe infection. Indian J. Cancer 2021, 58, 190–194. [Google Scholar] [PubMed]
- Brinksma, A.; Huizinga, G.; Sulkers, E.; Kamps, W.; Roodbol, P.; Tissing, W. Malnutrition in childhood cancer patients: A review on its prevalence and possible causes. Crit. Rev. Oncol. 2012, 83, 249–275. [Google Scholar] [CrossRef] [PubMed]
- Połubok, J.; Malczewska, A.; Rąpała, M.; Szymocha, J.; Kozicka, M.; Dubieńska, K.; Duczek, M.; Kazanowska, B.; Barg, E. Nutritional status at the moment of diagnosis in childhood cancer patients. Pediatr. Endocrinol. Diabetes Metab. 2017, 23, 77–82. [Google Scholar] [CrossRef]
- Iniesta, R.R.; Paciarotti, I.; Davidson, I.; McKenzie, J.M.; Brougham, M.F.; Wilson, D.C. Nutritional status of children and adolescents with cancer in Scotland: A prospective cohort study. Clin. Nutr. ESPEN 2019, 32, 96–106. [Google Scholar] [CrossRef]
- Gaynor, E.P.T.; Sullivan, P.B. Nutritional status and nutritional management in children with cancer. Arch. Dis. Child. 2015, 100, 1169–1172. [Google Scholar] [CrossRef]
- Paccagnella, A.; Morassutti, I.; Rosti, G. Nutritional intervention for improving treatment tolerance in cancer patients. Curr. Opin. Oncol. 2011, 23, 322–330. [Google Scholar] [CrossRef]
- World Health Organization. BMI-for-Age (5–19 Years). 2019. Available online: https://www.who.int/tools/growth-reference-data-for-5to19-years/indicators/bmi-for-age (accessed on 16 January 2024).
- Kuczmarski, R.R.J.; Ogden, C.L.C.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC Growth Charts for the United States: Methods and Development. Vital Health Stat. 2002, 246, 1–190. [Google Scholar]
- Murphy, A.J.; White, M.; Elliott, S.A.; Lockwood, L.; Hallahan, A.; Davies, P.S. Body composition of children with cancer during treatment and in survivorship. Am. J. Clin. Nutr. 2015, 102, 891–896. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, N.; Lu, X.; Cai, R.; Liu, M.; Liu, K. Nutritional Screening and Assessment, and Quality of Life in Children with Cancer: A Cross-Sectional Study in Mainland China. J. Pediatr. Nurs. 2021, 57, 99–105. [Google Scholar] [CrossRef] [PubMed]
- van der Haak, N.; Edwards, S.; Perem, M.; Landorf, E.; Osborn, M. Nutritional Status at Diagnosis, During, and After Treatment in Adolescents and Young Adults with Cancer. J. Adolesc. Young Adult Oncol. 2021, 10, 668–674. [Google Scholar] [CrossRef]
- Tripodi, S.I.; Bergami, E.; Panigari, A.; Caissutti, V.; Brovia, C.; De Cicco, M.; Cereda, E.; Caccialanza, R.; Zecca, M. The role of nutrition in children with cancer. Tumori J. 2023, 109, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Tah, P.C.; Shanita, S.N.; Poh, B.K. Nutritional status among pediatric cancer patients: A comparison between hematological malignancies and solid tumors. J. Spéc. Pediatr. Nurs. 2012, 17, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Lemos, P.d.S.M.; de Oliveira, F.L.C.; Caran, E.M.M. Nutritional status of children and adolescents at diagnosis of hematological and solid malignancies. Rev. Bras. Hematol. Hemoter. 2014, 36, 420–423. [Google Scholar] [CrossRef]
- Li, Y.; Lu, Z.; Ma, A.; Yao, W.; Dong, R.; Li, K.; Wu, M.; Dong, K.; Qian, T. Nutritional status associated with clinical outcomes in children with solid tumors: A retrospective cohort study from China. Cancer Med. 2024, 13, e6798. [Google Scholar] [CrossRef]
- Ermamilia, A.; Aulia, B.; Mulatsih, S. A cross-sectional study of nutritional status and dietary intake of paediatric oncology patients in Indonesia: Comparison between cancer aetiologies. Nutr. Health 2023, 2601060231166163. [Google Scholar] [CrossRef]
- Antillon, F.; Rossi, E.; Molina, A.L.; Sala, A.; Pencharz, P.; Valsecchi, M.G.; Barr, R. Nutritional status of children during treatment for acute lymphoblastic leukemia in Guatemala. Pediatr. Blood Cancer 2013, 60, 911–915. [Google Scholar] [CrossRef]
- Hafiz, M.G.; Mannan, M.A. Nutritional status at initial presentation in childhood acute lymphoblastic leukemia and its effect on induction of remission. Mymensingh Med. J. 2008, 17, S46–S51. [Google Scholar] [PubMed]
- Kumar, R.; Marwaha, R.K.; Bhalla, A.K.; Gulati, M. Protein energey malnutrition and skeletal muscle wasting in childhood acute lymphoblastic lukemia. Indian Pediatr. 2000, 37, 720–726. [Google Scholar]
- Dushnicky, M.J.; Nazarali, S.; Mir, A.; Portwine, C.; Samaan, M.C. Is There a Causal Relationship between Childhood Obesity and Acute Lymphoblastic Leukemia? A Review. Cancers 2020, 12, 3082. [Google Scholar] [CrossRef] [PubMed]
- Brinksma, A.; Roodbol, P.F.; Sulkers, E.; Kamps, W.A.; de Bont, E.S.; Boot, A.M.; Burgerhof, J.G.; Tamminga, R.Y.; Tissing, W.J. Changes in nutritional status in childhood cancer patients: A prospective cohort study. Clin. Nutr. 2015, 34, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Kellerman, I.; Blaauw, R.; Schoeman, J.; Kruger, M. Changes in anthropometrical status and body composition in children with cancer during initial chemotherapy. Pediatr. Hematol. Oncol. 2023, 40, 659–672. [Google Scholar] [CrossRef]
- Zhang, F.F.; Kelly, M.J.; Saltzman, E.; Must, A.; Roberts, S.B.; Parsons, S.K. Obesity in pediatric all survivors: A meta-analysis. Pediatrics 2014, 133, e704–e715. [Google Scholar] [CrossRef]
- Browne, E.K.; Inaba, H. Obesity and height in children and adolescents with acute lymphoblastic leukemia and its future management. Oncotarget 2019, 10, 1233–1234. [Google Scholar] [CrossRef]
- Jansen, H.; Postma, A.; Stolk, R.P.; Kamps, W.A. Acute lymphoblastic leukemia and obesity: Increased energy intake or decreased physical activity? Support. Care Cancer 2009, 17, 103–106. [Google Scholar] [CrossRef]
- Reilly, J.J.; Brougham, M.; Montgomery, C.; Richardson, F.; Kelly, A.; Gibson, B.E.S. Effect of glucocorticoid therapy on energy intake in children treated for acute lymphoblastic leukemia. J. Clin. Endocrinol. Metab. 2001, 86, 3742–3745. [Google Scholar] [CrossRef]
- Vilela, M.I.O.P.; Viana, M.B. Longitudinal growth and risk factors for growth deficiency in children treated for acute lymphoblastic leukemia. Pediatr. Blood Cancer 2006, 48, 86–92. [Google Scholar] [CrossRef]
- Browne, E.K.; Zhou, Y.; Chemaitilly, W.; Panetta, J.C.; Ness, K.K.; Kaste, S.C.; Cheng, C.; Relling, M.V.; Pui, C.; Inaba, H. Changes in body mass index, height, and weight in children during and after therapy for acute lymphoblastic leukemia. Cancer 2018, 124, 4248–4259. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Almaguer, D.; Ruiz-Argüelles, G.J.; Ponce-de-León, S. Nutritional status and socio-economic conditions as prognostic fac-tors in the outcome of therapy in childhood acute lymphoblastic leukemia. Int. J. Cancer Suppl. 1998, 11, 52–55. [Google Scholar] [CrossRef]
- Joffe, L.; Dwyer, S.; Bender, J.L.G.; Frazier, A.L.; Ladas, E.J. Nutritional status and clinical outcomes in pediatric patients with solid tumors: A systematic review of the literature. Semin. Oncol. 2019, 46, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Karalexi, M.A.; Markozannes, G.; Tagkas, C.F.; Katsimpris, A.; Tseretopoulou, X.; Tsilidis, K.K.; Spector, L.G.; Schüz, J.; Siahanidou, T.; Petridou, E.T.; et al. Nutritional Status at Diagnosis as Predictor of Survival from Childhood Cancer: A Review of the Literature. Diagnostics 2022, 12, 2357. [Google Scholar] [CrossRef] [PubMed]
- Iniesta, R.R.; Paciarotti, I.; Brougham, M.F.; McKenzie, J.M.; Wilson, D.C. Effects of pediatric cancer and its treatment on nutritional status: A systematic review. Nutr. Rev. 2015, 73, 276–295. [Google Scholar] [CrossRef] [PubMed]
- Lobato-Mendizábal, E.; López-Martínez, B.; Ruiz-Argüelles, G.J. A critical review of the prognostic value of the nutritional status at diagnosis in the outcome of therapy of children with acute lymphoblastic leukemia. Rev. Investig. Clin. 2003, 55, 31–35. [Google Scholar]
- Lin, J.L.; Liu, K.K.; Chu, J.H.; Huang, L.L.; Xie, Z.W.; Yang, L.H.; Tu, S.J.; Wang, N.L. Relationship between Nutritional Status and Nosocomial Infection in Children with Acute Lymphoblastic Leukemia. Zhongguo Shi Yan Xue Ye Xue Za Zhi 2020, 28, 767–774. [Google Scholar]
- Viani, K.; Trehan, A.; Manzoli, B.; Schoeman, J. Assessment of nutritional status in children with cancer: A narrative review. Pediatr. Blood Cancer 2020, 67 (Suppl. S3), e28211. [Google Scholar] [CrossRef]
- Butte, N.E.; Garza, C.; de Onis, M. Evaluation of the feasibility of international growth standards for school-aged children and adolescents. Food Nutr. Bull. 2006, 27, S169–S174. [Google Scholar] [CrossRef]
- Ladas, E.J.; Arora, B.; Howard, S.C.; Rogers, P.C.; Mosby, T.T.; Barr, R.D. A Framework for Adapted Nutritional Therapy for Children with Cancer in Low- and Middle-Income Countries: A Report from the SIOP PODC Nutrition Working Group. Pediatr. Blood Cancer 2016, 63, 1339–1348. [Google Scholar] [CrossRef]
- Brennan, B.M. Sensitive measures of the nutritional status of children with cancer in hospital and in the field. Int. J. Cancer Suppl. 1998, 11, 10–13. [Google Scholar] [CrossRef]
- Lifson, L.F.; Hadley, G.P.; Wiles, N.L.; Pillay, K. Nutritional status of children with Wilms’ tumour on admission to a South African hospital and its influence on outcome. Pediatr. Blood Cancer 2017, 64, e26382. [Google Scholar] [CrossRef] [PubMed]
- Barr, R.; Collins, L.; Nayiager, T.; Doring, N.; Kennedy, C.; Halton, J.; Walker, S.; Sala, A.; Webber, C. Nutritional status at diagnosis in children with cancer. 2. An assessment by arm anthropometry. J. Pediatr. Hematol. Oncol. 2011, 33, e101–e104. [Google Scholar] [CrossRef]
- Pedro, J.; Martucci, R.; Monteiro, G.; Saraiva, D. Mid-upper arm circumference in hospitalized pediatric patients with cancer: Is there an association with malnutrition? Nutr. Clin. Pract. 2023, 38, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Yaprak, D.S.; Yalçın, B.; Pınar, A.A.; Büyükpamukçu, M. Assessment of nutritional status in children with cancer: Significance of arm anthropometry and serum visceral proteins. Pediatr. Blood Cancer 2021, 68, e28752. [Google Scholar] [CrossRef] [PubMed]
- Collins, L.; Beaumont, L.; Cranston, A.; Savoie, S.; Nayiager, T.; Barr, R. Anthropometry in Long-Term Survivors of Acute Lymphoblastic Leukemia in Childhood and Adolescence. J. Adolesc. Young Adult Oncol. 2017, 6, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Henry, L.; Aldiss, S.; Gibson, F.; Pugh, G.; Stevens, M.; Children, Teenagers and Young Adults (CTYA) Workstream of the NIHR Cancer and Nutrition Collaboration. Nutritional assessment and dietetic resource for children and young people with cancer in the United Kingdom. Pediatr. Blood Cancer 2022, 69, e29743. [Google Scholar] [CrossRef] [PubMed]
- Barr, R.D. Nutritional status in children with cancer: Before, during and after therapy. Indian J. Cancer 2015, 52, 173–175. [Google Scholar] [CrossRef]
- Priyanka, S.; Sandeep, J.; Gauri, K.; Gayatri, V. Dual-Energy X-Ray Absorptiometry and Anthropometry for Assessment of Nutritional Status at Diagnosis in Children with Cancer: A Single-Center Experience from India. South Asian J. Cancer 2022, 11, 164–171. [Google Scholar] [CrossRef]
- Collins, L.; Nayiager, T.; Doring, N.; Kennedy, C.; Webber, C.; Halton, J.; Walker, S.; Sala, A.; Barr, R.D. Nutritional status at diagnosis in children with cancer I. An assessment by dietary recall--compared with body mass index and body composition measured by dual energy X-ray absorptiometry. J. Pediatr. Hematol. Oncol. 2010, 32, e299–e303. [Google Scholar] [CrossRef]
- Marra, M.; Sammarco, R.; De Lorenzo, A.; Iellamo, F.; Siervo, M.; Pietrobelli, A.; Donini, L.M.; Santarpia, L.; Cataldi, M.; Pasanisi, F.; et al. Assessment of Body Composition in Health and Disease Using Bioelectrical Impedance Analysis (BIA) and Dual Energy X-Ray Absorptiometry (DXA): A Critical Overview. Contrast Media Mol. Imaging 2019, 2019, 3548284. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.; Lis, C.G. Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature. Nutr. J. 2010, 9, 69. [Google Scholar] [CrossRef] [PubMed]
- Sala, A.; Rossi, E.; Antillon, F.; Molina, A.L.; de Maselli, T.; Bonilla, M.; Hernandez, A.; Ortiz, R.; Pacheco, C.; Nieves, R.; et al. Nutritional status at diagnosis is related to clinical outcomes in children and adolescents with cancer: A perspective from Central America. Eur. J. Cancer 2012, 48, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Garófolo, A.; Lemos, P.S.M. Is serum albumin associated with prognostic in pediatric cancer patients? Hos. Pal. Med. Int. J. 2020, 4, 51–56. [Google Scholar] [CrossRef]
- OECD. Survival and mortality for leukaemia in children. In Health at a Glance 2017: OECD Indicators; OECD Publishing: Paris, France, 2017. [Google Scholar]
- Wang, K.-W.; Ladhani, S.; Empringham, B.; Portwine, C.; Fleming, A.; Banfield, L.; Balakumaran, J.; Sarpong, L.; Sims, E.D.; Popa, A.N.; et al. Bariatric interventions in obesity treatment and prevention in pediatric acute lymphoblastic leukemia: A systematic review and meta-analysis. Cancer Metastasis Rev. 2020, 39, 79–90. [Google Scholar] [CrossRef]
- Walters, M.; Mowbray, C.; Jubelirer, T.; Jacobs, S.; Kelly, K.M.; Smith, K.; Yao, Y.; Jin, Z.; Ladas, E.J. A bilingual dietary intervention early in treatment is feasible and prevents weight gain in childhood acute lymphoblastic leukemia. Pediatr. Blood Cancer 2021, 68, e28910. [Google Scholar] [CrossRef]
- Orgel, E.; Sposto, R.; Malvar, J.; Seibel, N.L.; Ladas, E.; Gaynon, P.S.; Freyer, D.R. Impact on survival and toxicity by duration of weight extremes during treatment for pediatric acute lymphoblastic leukemia: A report from the children’s oncology group. J. Clin. Oncol. 2014, 32, 1331–1337. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| TP1 (n = 26) | TP2 (n = 25) | TP3 (n = 24) | TP4 (n = 17) | p-Value | |
|---|---|---|---|---|---|
| BW for age z-score (SD), median (min–max) | 0.58 (−1.41–1.52) | 0.79 (−2.22–2.66) | 0.83 (−1.43–2.51) | 0.37 (−0.61–1.44) | 0.027 |
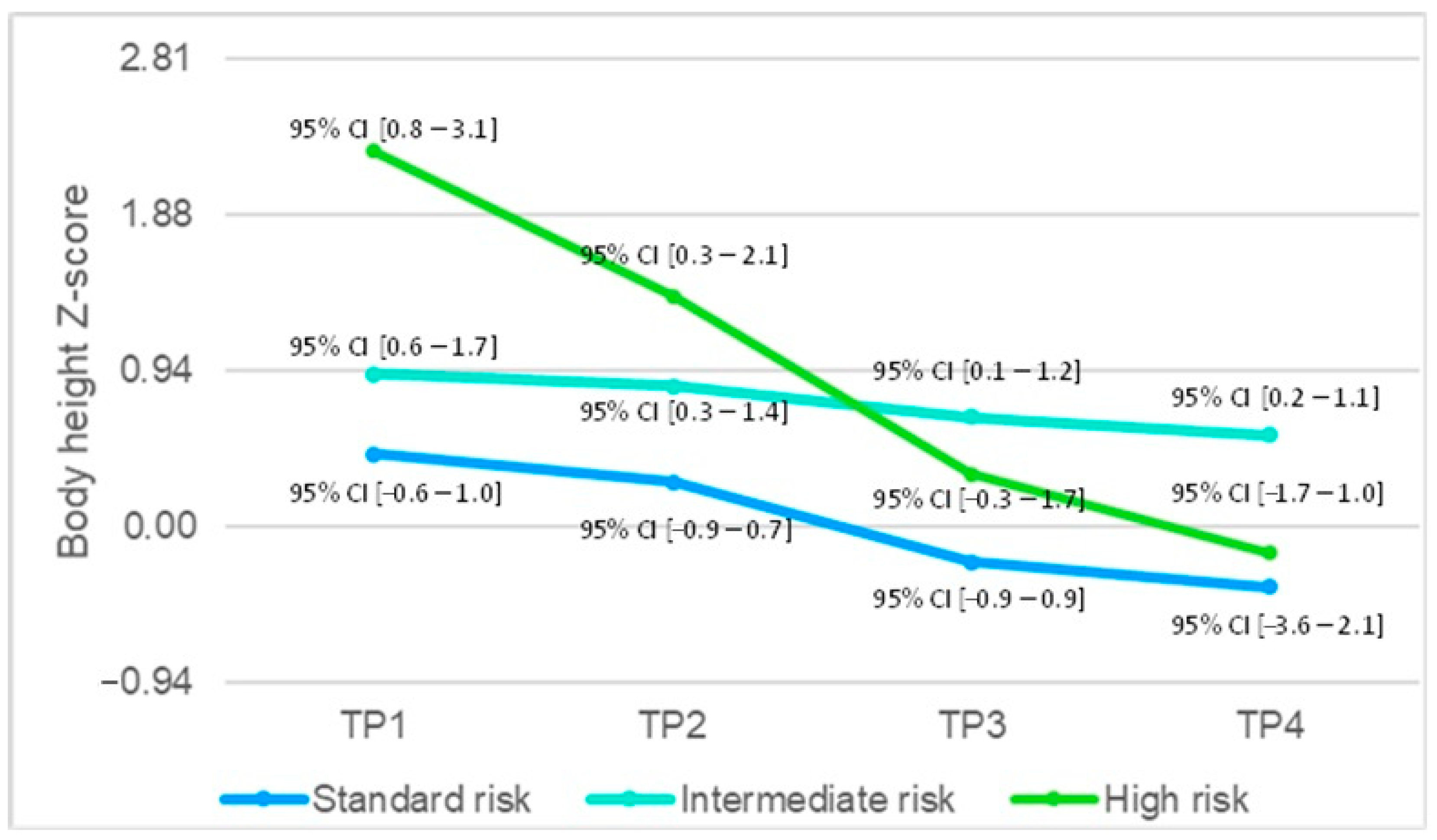
| BH/BL for age z-score (SD), median (min–max) | 0.94 (−1.13–3.21) | 0.59 (−1.69–2.62) | 0.42 (−2.18–2.11) | 0.19 (−2.03–1.85) | <0.001 |
| BMI for age z-score (SD), median (min–max) | 0.05 (−2.75–1.32) | 0.49 (−3.82–2.92) | 0.76 (−1.64–2.68) | 0.55 (−1.23–2.05) | 0.001 |
| Albumin (g/L), median (min–max) | 37 (29–46) | 36 (23–43) | 36 (22–41) | N/A | 0.695 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kranjčec, I.; Pranjić, I.; Roganović, J.; Pavlović, M.; Rajačić, N.; Sila, S. Alterations of Nutritional Status in Children and Adolescents with Acute Lymphoblastic Leukemia. Children 2024, 11, 334. https://doi.org/10.3390/children11030334
Kranjčec I, Pranjić I, Roganović J, Pavlović M, Rajačić N, Sila S. Alterations of Nutritional Status in Children and Adolescents with Acute Lymphoblastic Leukemia. Children. 2024; 11(3):334. https://doi.org/10.3390/children11030334
Chicago/Turabian StyleKranjčec, Izabela, Ines Pranjić, Jelena Roganović, Maja Pavlović, Nada Rajačić, and Sara Sila. 2024. "Alterations of Nutritional Status in Children and Adolescents with Acute Lymphoblastic Leukemia" Children 11, no. 3: 334. https://doi.org/10.3390/children11030334