
Complementary Feeding Methods, Feeding Problems, Food Neophobia, and Picky Eating among Polish Children


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Rationale for the Selection of the Test Group
2.3. Exclusion and Inclusion Criteria
2.4. Research Tool
2.5. Statistical Analyses
3. Results
3.1. Characteristics of the Study Population
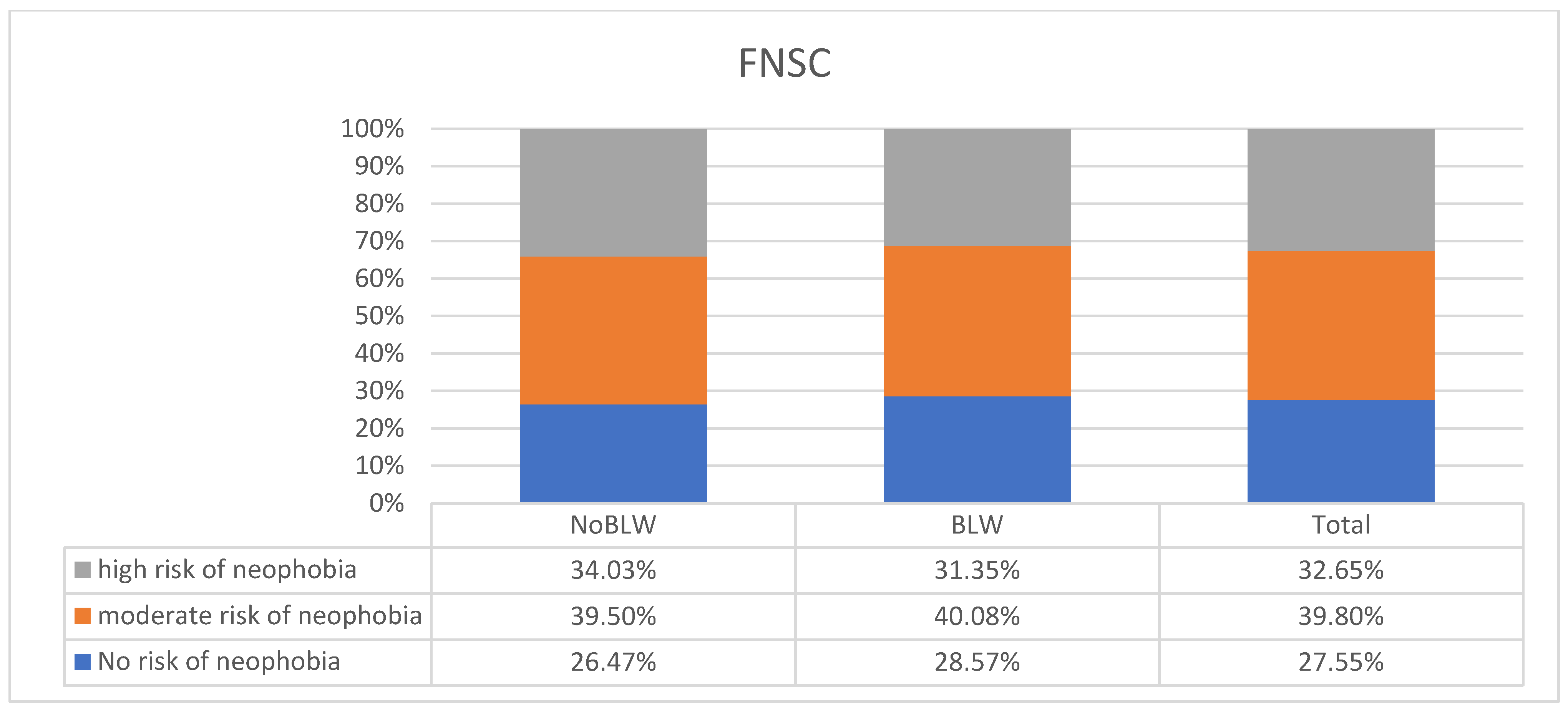
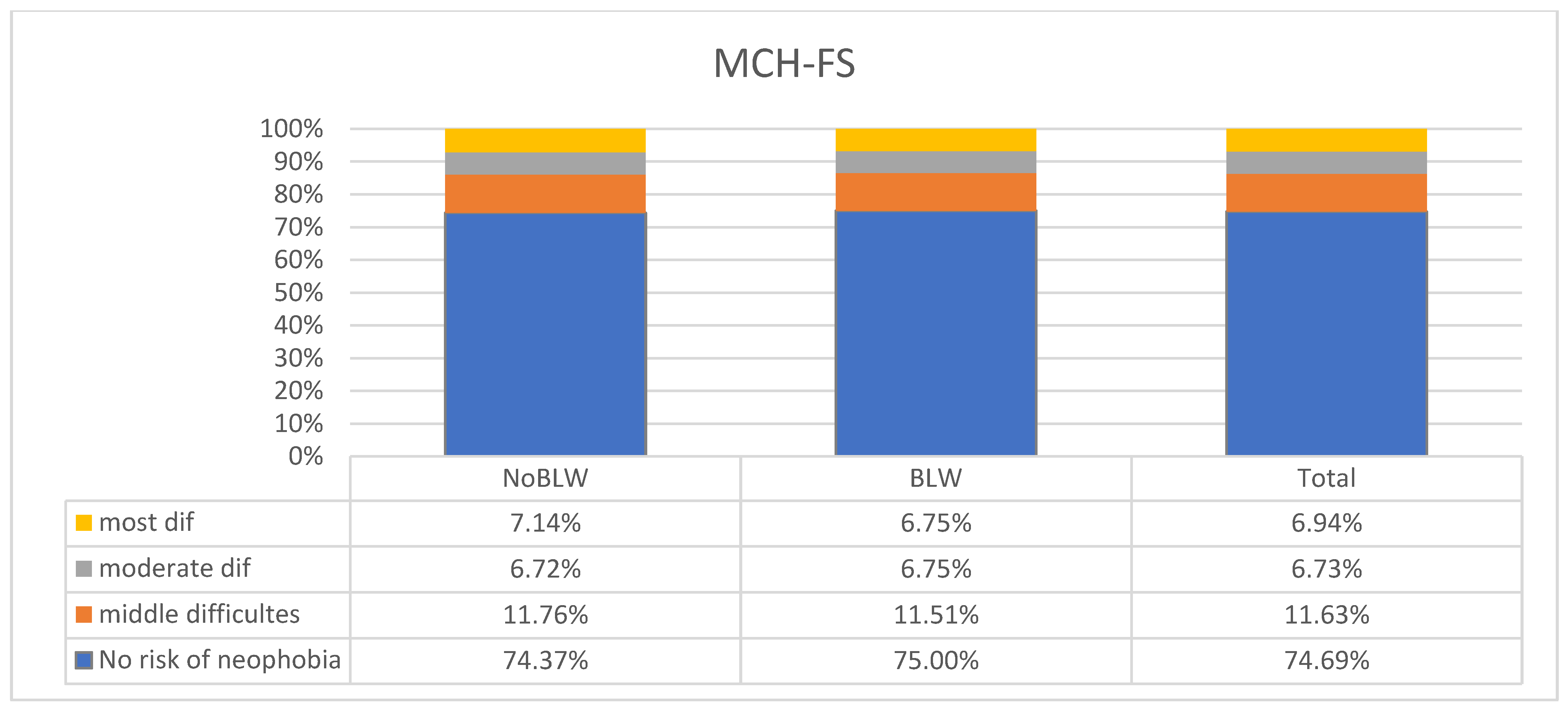
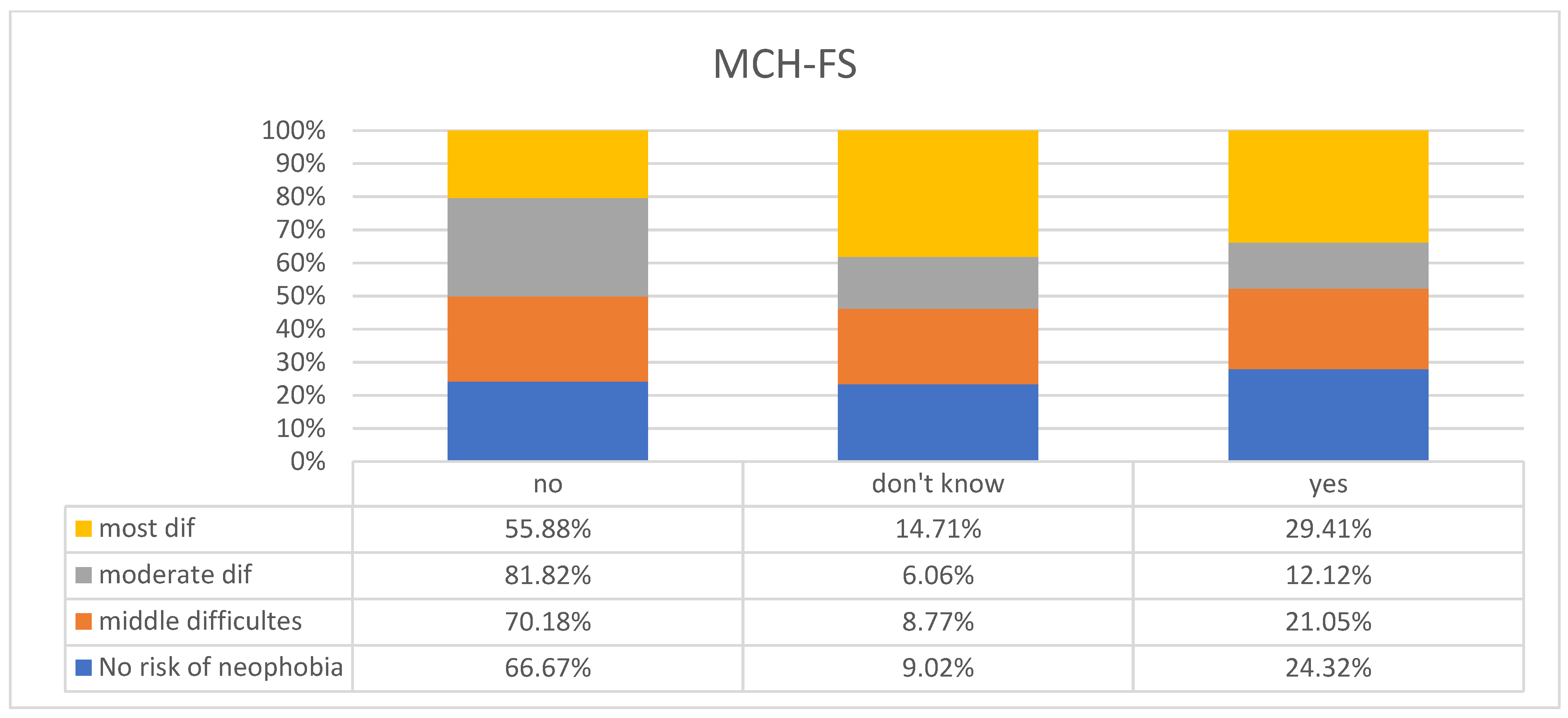
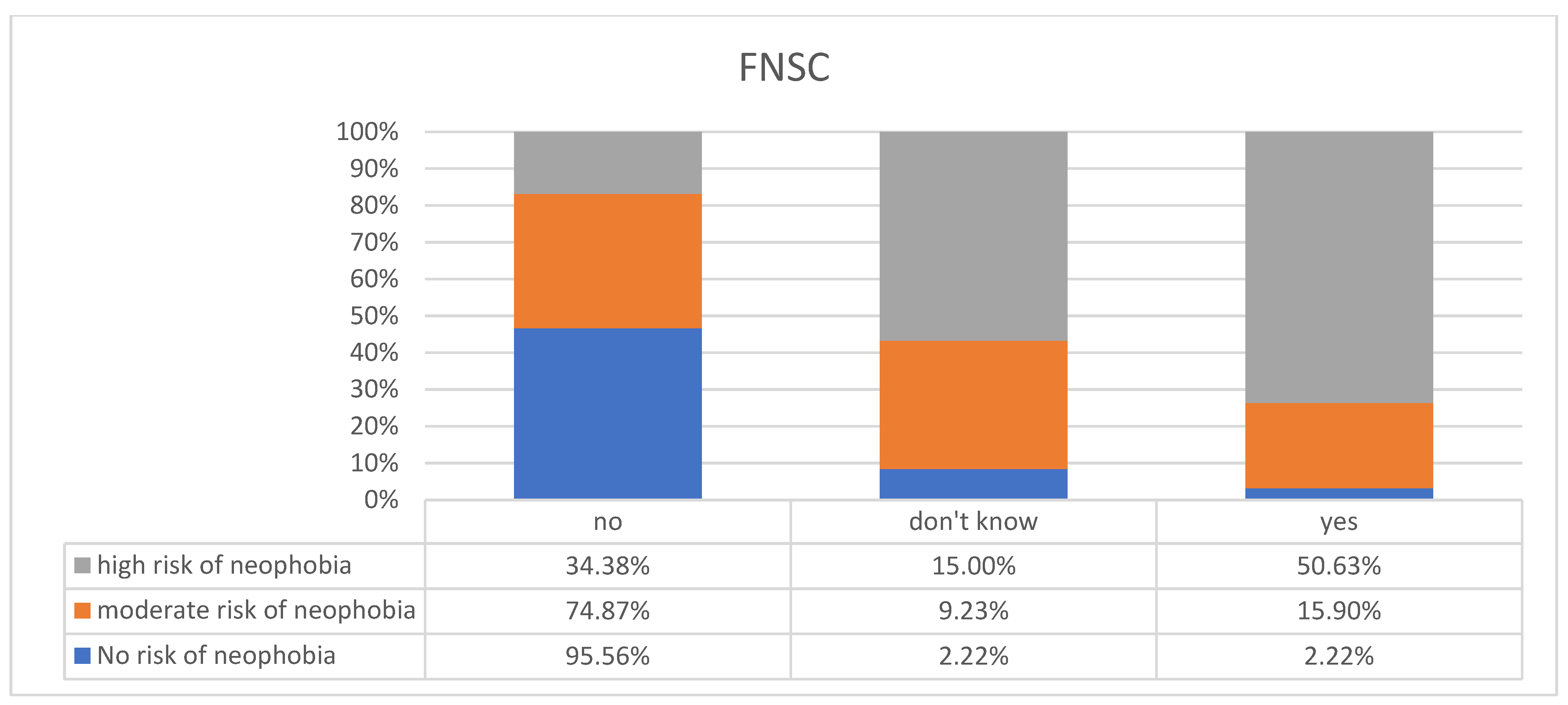
3.2. Interpretations of Food Neophobia Based on Standardized Questionnaires
4. Discussion
5. Strengths and Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Szajewska, H.; Socha, P.; Horvath, A. Zasady żywienia zdrowych niemowląt. Stanowisko Polskiego Towarzystwa Gastroenterologii, Hepatologii i Żywienia Dzieci. Stand. Med. 2021, 18, 805–822. [Google Scholar]
- Greer, F.R.; Sicherer, S.H.; Burks, A.W.; Committee on Nutrition; Section on Allergy and Immunology. The Effects of Early Nutritional Interventions on the Development of Atopic Disease in Infants and Children: The Role of Maternal Dietary Restriction, Breastfeeding, Hydrolyzed Formulas, and Timing of Introduction of Allergenic Complementary Foods. Pediatrics 2019, 143, e20190281. [Google Scholar] [CrossRef] [PubMed]
- Lanigan, J.; Singhal, A. Early Nutrition and long-term health: A practical approach. Proc. Nutr. Soc. 2009, 68, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Bocquet, A.; Brancato, S.; Turck, D.; Chalumeau, M.; Darmaun, D.; De Luca, A.; Feillet, F.; Frelut, M.L.; Guimber, D.; Lapillonne, A.; et al. “Baby-led weaning”—Progress in infant feeding or risky trend? Arch. Pediatr. Organe Off. Soc. Fr. Pediatr. 2022, 29, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Castenmiller, J.; de Henauw, S.; Hirsch-Ernst, K.I.; Kearney, J.; Knutsen, H.K.; Maciuk, A.; Mangelsdort, I.; Mcardle, H.J.; Naska, A.; EFSA NDA Panel (EFSA Panel on Nutrition, Novel Foods and Food Allergens); et al. Scientific Opinion on the appropriate age range for introduction of complementary feeding into an infant’s diet. EFSA J. 2019, 17, 5780. [Google Scholar]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Mis, N.F.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef] [PubMed]
- WHO (Światowa Organizacja Zdrowia). Karmienie Uzupełniające. Sprawozdanie z Globalnych Konsultacji i Podsumowanie zasad Przewodnich. Genewa: WHO (Światowa Organizacja Zdrowia). 2002. Available online: http://www.who.int/nutrition/publications/Complementary_Feeding.pdf (accessed on 15 December 2023).
- Białek-Dratwa, A.; Szczepańska, E.; Trzop, P.; Grot, M.; Grajek, M.; Kowalski, O. Practical Implementation of the BLW Method during the Expansion of the Infant Diet-A Study among Polish Children. Front. Nutr. 2022, 24, 890843. [Google Scholar] [CrossRef] [PubMed]
- Cameron, S.L.; Taylor, R.W.; Heath, A.-L.M. Development and pilot testing of baby-led introduction to SolidS—A version of baby-led weaning modified to address concerns about iron deficiency, growth faltering and choking. BMC Pediatr. 2015, 15, 99. [Google Scholar] [CrossRef]
- Knaapila, A.; Silventoinen, K.; Broms, U.; Rose, R.J.; Perola, M.; Kaprio, J.; Tuorila, H.M. Food neophobia in young adults. Genetic architecture and relation to personality, pleasantness and use frequency of foods, and body mass index—A twin study. Behav. Genet. 2011, 41, 512–521. [Google Scholar] [CrossRef]
- Szakály, Z.; Kovács, B.; Soós, M.; Kiss, M.; Balsa-Budai, N. Adaptation and Validation of the Food Neophobia Scale: The Case of Hungary. Foods 2021, 10, 1766. [Google Scholar] [CrossRef]
- Karaağaç, Y.; Bellikci-Koyu, E. A narrative review on food neophobia throughout the lifespan: Relationships with dietary behaviours and interventions to reduce it. Br. J. Nutr. 2022, 130, 793–826. [Google Scholar] [CrossRef] [PubMed]
- Capiola, A.; Raudenbush, B. The effects of food neophobia and food neophilia on diet and metabolic processing. Food Nutr. Sci. 2012, 3, 1397–1403. [Google Scholar] [CrossRef]
- Galloway, A.T.; Lee, Y.; Birch, L.L. Predictors and consequences of Food neophobia and pickiness in young girls. J. Am. Diet. Assoc. 2003, 103, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Kaar, J.L.; Shapiro, A.L.B.; Fell, D.M.; Johnson, S.L. Parental feeding practices, food neophobia, and child food preferences: What combination of factors results in children eating a variety of foods? Food Qual. Prefer. 2016, 50, 57–64. [Google Scholar] [CrossRef]
- Alley, T.R.; Potter, K.A. Food Neophobia and Sensation Seeking. In Handbook of Behavior, Food and Nutrition; Preedy, V., Watson, R., Martin, C., Eds.; Springer: New York, NY, USA, 2011; pp. 707–724. [Google Scholar]
- Cooke, L.; Wardle, J.; Gibson, E.J. Relationship between parental report of food neophobia and everyday food consumption in 2–6-year-old children. Appetite 2003, 41, 205–206. [Google Scholar] [CrossRef] [PubMed]
- Dovey, T.M.; Staples, P.A.; Gibson, E.L.; Halford, J.C. Food neophobia and ‘picky/fussy’ eating in children: A review. Appetite 2008, 50, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L. Development of food preferences. Annu. Rev. Nutr. 1999, 19, 41–62. [Google Scholar] [CrossRef]
- Perry, R.A.; Mallan, K.M.; Koo, J.; Mauch, C.E.; Daniels, L.A.; Magarey, A.M. Food neophobia and its association with diet quality and weight in children aged 24 months: A cross sectional study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 13. [Google Scholar] [CrossRef]
- Białek-Dratwa, A.; Szczepańska, E.; Szymańska, D.; Grajek, M.; Krupa-Kotara, K.; Kowalski, O. Neophobia—A Natural Developmental Stage or Feeding Difficulties for Children? Nutrients 2022, 14, 1521. [Google Scholar] [CrossRef]
- Kutbi, H.A.; Alhatmi, A.A.; Alsulami, M.H.; Alghamdi, S.S.; Albagar, S.M.; Mumena, W.A.; Mosli, R.H. Food neophobia and pickiness among children and associations with socioenvironmental and cognitive factors. Appetite 2019, 142, 104373. [Google Scholar] [CrossRef]
- Pickard, A.; Thibaut, J.P.; Philippe, K.; Lafraire, J. Poor conceptual knowledge in the food domain and food rejection dispositions in 3- to 7-year-old children. J. Exp. Child. Psychol. 2023, 226, 105546. [Google Scholar] [CrossRef]
- DeJesus, J.M.; Gerdin, E.; Sullivan, K.R.; Kinzler, K.D. Children judge others based on their food choices. J. Exp. Child. Psychol. 2019, 179, 143–161. [Google Scholar] [CrossRef]
- Foinant, D.; Lafraire, J.; Thibaut, J.P. Strength or Nausea? Children’s Reasoning About the Health Consequences of Food Consumption. Front. Psychol. 2021, 12, 651889. [Google Scholar] [CrossRef]
- Obwieszczenie Marszałka Sejmu Rzeczypospolitej Polskiej z Dnia 18 Czerwca 2020 r. w Sprawie Ogłoszenia Jednolitego Tekstu Ustawy—Kodeks Pracy Warszawa, Dnia 30 Lipca 2020 r. Poz. 1320. Available online: https://www.pip.gov.pl/pl/f/v/224803/D2020000132001.pdf (accessed on 15 December 2023).
- Ustawa z Dnia 26 Czerwca 1974 r.—Kodeks Pracy (Dz. U. z 2022 r. poz. 1510, z Późn. Zm.) Wraz z Aktualizacjami. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20220001510 (accessed on 15 December 2023).
- Rozporządzenie Ministra Rodziny, Pracy i Polityki Społecznej z Dnia 8 Grudnia 2015 r. w Sprawie Wniosków Dotyczących Uprawnień Pracowników Związanych z Rodzicielstwem Oraz Dokumentów Dołączanych do Takich Wniosków (Dz. U. z 2015 r. poz. 2243) Wraz z Aktualizacjami. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20150002243 (accessed on 15 December 2023).
- Ustawa z Dnia 25 Czerwca 1999 r. o Świadczeniach Pieniężnych z Ubezpieczenia Społecznego w Razie Choroby i Macierzyństwa (Dz. U. z 2022 r. poz. 1732) Wraz z Aktualizacjami. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=wdu19990600636 (accessed on 15 December 2023).
- Zakład Ubezpieczeń Społecznych. Ojcowie na Zasiłku Macierzyńskim. 23.06.2021 r. Available online: https://www.zus.pl/o-zus/aktualnosci/-/publisher/aktualnosc/0/ojcowie-na-zasilku-macierzynskim/4070408 (accessed on 15 December 2023).
- Kulaga, Z.; Litwin, M.; Tkaczyk, M.; Różdżyńska, A.; Barwicka, K.; Grajda, A.; Świąder, A.; Gurzkowska, B.; Napieralska, E.; Pan, H. Wzrost, masa ciała i BMI w zależności od wieku polskich dzieci i młodzieży w wieku szkolnym w odniesieniu do międzynarodowych i lokalnych punktów odniesienia dotyczących wzrostu. BMC Public Health 2010, 10, 109. [Google Scholar] [CrossRef]
- WHO. WHO Multicentre Growth Reference Study WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Rozporządzenie Ministra Zdrowia z Dnia 6 Kwietnia 2020 r. w Sprawie Rodzajów, Zakresu i Wzorów Dokumentacji Medycznej Oraz Sposobu Jej Przetwarzania. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20200000666 (accessed on 15 December 2023).
- Pliner, P.; Hobden, K.L. Development of a scale to measure the trait of food neophobia in humans. Appetite 1992, 19, 105–120. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, M.; Martel, C.; Porporino, M.; Zygmuntowicz, C. The Montreal Children’s Hospital Feeding Scale: A brief bilingual screening tool for identifying feeding problems. Paediatr. Child. Health 2011, 16, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Bąbik, K.; Dziechciarz, P.; Horvath, A.; Ostaszewski, P. The Polish version of the Montreal Children’s Hospital Feeding Scale (MCH-FS): Translation, cross-cultural adaptation, and validation. J. Paediatr. 2019, 94, 299–305. [Google Scholar] [CrossRef]
- Białek-Dratwa, A.; Kowalski, O. Prevalence of Feeding Problems in Children and Associated Factors—A Cross-Sectional Study among Polish Children Aged 2–7 Years. Nutrients 2023, 15, 3185. [Google Scholar] [CrossRef] [PubMed]
- Białek-Dratwa, A.; Kowalski, O. Infant Complementary Feeding Methods and Subsequent Occurrence of Food Neophobia—A Cross-Sectional Study of Polish Children Aged 2–7 Years. Nutrients 2023, 15, 4590. [Google Scholar] [CrossRef]
- Verbeke, W. Consumer acceptance of functional foods: Socio-demographic, cognitive and attitudinal determinants. Food Qual. Prefer. 2005, 16, 45–57. [Google Scholar] [CrossRef]
- Brown, A. No difference in self-reported frequency of choking between infants introduced to solid foods using a baby-led weaning or traditional spoon-feeding approach. J. Hum. Nutr. Diet. 2018, 31, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Dogan, E.; Yilmaz, G.; Caylan, N.; Turgut, M.; Gokcay, G.; Oguz, M.M. Baby-led complementary feeding: Randomized controlled study. Pediatr. Int. Off. J. Jpn. Pediatr. Soc. 2018, 60, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- D’auria, E.; Pediatrics, O.B.O.T.I.S.O.; Bergamini, M.; Staiano, A.; Banderali, G.; Pendezza, E.; Penagini, F.; Zuccotti, G.V.; Peroni, D.G. Baby-led weaning: What a systematic review of the literature adds on. Ital. J. Pediatr. 2018, 44, 49. [Google Scholar] [CrossRef] [PubMed]
- Białek-Dratwa, A.; Kowalski, O.; Szczepańska, E. Traditional complementary feeding or BLW (Baby Led Weaning) method?—A cross-sectional study of Polish infants during complementary feeding. Front. Pediatr. 2022, 10, 992244. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.; Lee, M. A descriptive study investigating the use and nature of baby-led weaning in a UK sample of mothers. Matern. Child. Nutr. 2011, 7, 34–47. [Google Scholar] [CrossRef]
- Białek-Dratwa, A.; Soczewka, M.; Grajek, M.; Szczepańska, E.; Kowalski, O. Use of the Baby-Led Weaning (BLW) Method in Complementary Feeding of the Infant-A Cross-Sectional Study of Mothers Using and Not Using the BLW Method. Nutrients 2022, 14, 2372. [Google Scholar] [CrossRef]
- Pearce, J.; Langley-Evans, S.C. Comparison of food and nutrient intake in infants aged 6-12 months, following baby-led or traditional weaning: A cross-sectional study. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2022, 35, 310–324. [Google Scholar] [CrossRef] [PubMed]
- Rowan, H.; Lee, M.; Brown, A. Estimated energy and nutrient intake for infants following baby-led and traditional weaning approaches. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2022, 35, 325–336. [Google Scholar] [CrossRef]
- Fu, X.; Conlon, C.A.; Haszard, J.J.; Beck, K.L.; von Hurst, P.R.; Taylor, R.W.; Heath, A.M. Food fussiness and early feeding characteristics of infants following Baby-Led Weaning and traditional spoon-feeding in New Zealand: An internet survey. Appetite 2018, 130, 110–116. [Google Scholar] [CrossRef]
- Martí-Solsona, E.; González-Chordá, V.M.; Andreu-Pejo, L.; Cervera-Gasch, Á.; Valero-Chillerón, M.J.; Mena-Tudela, D. Parents’ Perception of the Complementary Baby-Led Weaning Feeding Method: A Validation Study. Nurs. Rep. 2020, 10, 115–123. [Google Scholar] [CrossRef]
- Moore, A.P.; Milligan, P.; Goff, L.M. An online survey of knowledge of the weaning guidelines, advice from health visitors and other factors that influence weaning timing in UK mothers. Matern. Child. Nutr. 2014, 10, 410–421. [Google Scholar] [CrossRef]
- Rowan, H.; Harris, C. Baby-led weaning and the family diet. A Pilot Study. Appetite 2012, 58, 1046–1049. [Google Scholar] [CrossRef] [PubMed]
- Cameron, S.L.; Heath, A.L.; Taylor, R.W. Healthcare professionals’ and mothers’ knowledge of, attitudes to and experiences with, baby-led weaning: A content analysis study. BMJ Open 2012, 2, e001542. [Google Scholar] [CrossRef] [PubMed]
- Morison, B.J.; Taylor, R.W.; Haszard, J.J.; Schramm, C.J.; Erickson, L.W.; Fangupo, L.J. How different are baby-led weaning and conventional complementary feeding? A cross-sectional study of infants aged 6-8 months. BMJ Open 2016, 6, e010665. [Google Scholar] [CrossRef] [PubMed]
- D’andrea, E.; Jenkins, K.; Mathews, M.; Roebothan, B. Baby-led weaning: A preliminary investigation. Can. J. Diet. Pr. Res. 2016, 77, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Fangupo, L.J.; Heath, A.-L.M.; Williams, S.M.; Williams, L.W.E.; Morison, B.J.; Fleming, E.A.; Taylor, B.J.; Wheeler, B.J.; Taylor, R.W. A Baby-led approach to eating solids and risk of choking. Pediatrics 2016, 138, e20160772. [Google Scholar] [CrossRef] [PubMed]
- Özyüksel, G.; Soyer, T.; Üzümcügil, F.; Yalçın, Ş.; Ekinci, S.; Karnak, İ.; Çiftçi, A.Ö.; Tanyel, F.C. Foreign Body Aspiration in Infants: Role of Self-Feeding. Pediatr. Allergy Immunol. Pulmonol. 2019, 32, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Cameron, S.L.; Taylor, R.W.; Heath, A.L. Parent-led or baby-led? Associations between complementary feeding practices and health-related behaviours in a survey of New Zealand families. BMJ Open 2013, 3, e003946. [Google Scholar] [CrossRef] [PubMed]
- Quintiliano-Scarpelli, D.; Lehmann, N.; Castillo, B.; Blanco, E. Infant Feeding and Information Sources in Chilean Families Who Reported Baby-Led Weaning as a Complementary Feeding Method. Nutrients 2021, 13, 2707. [Google Scholar] [CrossRef]
- Cole, N.C.; An, R.; Lee, S.Y.; Donovan, S.M. Correlates of picky eating and food neophobia in young children: A systematic review and meta-analysis. Nutr. Rev. 2017, 75, 516–532. [Google Scholar] [CrossRef]
- Cardona Cano, S.; Hoek, H.W.; van Hoeken, D.; de Barse, L.M.; Jaddoe, V.W.; Verhulst, F.C.; Tiemeier, H. Behavioral outcomes of picky eating in childhood: A prospective study in the general population. J. Child Psychol. Psychiatry Allied Discip. 2016, 57, 1239–1246. [Google Scholar] [CrossRef] [PubMed]
- Dubois, L.; Farmer, A.; Girard, M.; Peterson, K.; Tatone-Tokuda, F. Problem eating behaviors related to social factors and body weight in preschool children: A longitudinal study. Int. J. Behav. Nutr. Phys. Act. 2007, 4, 9. [Google Scholar] [CrossRef] [PubMed]
- Zucker, N.; Copeland, W.; Franz, L.; Carpenter, K.; Keeling, L.; Angold, A.; Egger, H. Psychological and Psychosocial Impairment in Preschoolers with Selective Eating. Pediatrics 2015, 136, e582–e590. [Google Scholar] [CrossRef] [PubMed]
- Machado, B.C.; Dias, P.; Lima, V.S.; Campos, J.; Gonçalves, S. Prevalence and correlates of picky eating in preschool-aged children: A population-based study. Eat. Behav. 2016, 22, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Fildes, A.; van Jaarsveld, C.H.; Cooke, L.; Wardle, J.; Llewellyn, C.H. Common genetic architecture underlying young children’s food fussiness and liking for vegetables and fruit. Am. J. Clin. Nutr. 2016, 103, 1099–1104. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.; Lee, M.D. Early influences on child satiety-responsiveness: The role of weaning style. Pediatr. Obes. 2015, 10, 57–66. [Google Scholar] [CrossRef]
- Taylor, R.W.; Williams, S.M.; Fangupo, L.J.; Wheeler, B.J.; Taylor, B.J.; Daniels, L.; Fleming, E.A.; McArthur, J.; Morison, B.; Erickson, L.W.; et al. Effect of a Baby-Led Approach to Complementary Feeding on Infant Growth and Overweight: A Randomized Clinical Trial. JAMA Pediatr. 2017, 171, 838–846. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.B.; Gao, Z.B.; Li, Y.X.; Zhang, X.Y.; Zou, L.Q. The food neophobia scale (FNS): Exploration and confirmation of factor structure in a healthy Chinese sample. Food Qual. Prefer. 2020, 79, 103791. [Google Scholar] [CrossRef]
- Kozioł-Kozakowska, A.; Piórecka, B.; Schlegel-Zawadzka, M. Prevalence of food neophobia in pre-school children from southern Poland and its association with eating habits, dietary intake and anthropometric parameters: A cross-sectional study. Public Health Nutr. 2018, 21, 1106–1114. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Average | Standard Deviation | Min–Max | ||
|---|---|---|---|---|
| Characteristics of the group of mothers surveyed | age (years) | 33.36 | ±4.93 | 20–60 |
| Characteristics of the study group of children | gestational age and child birth (gestational week) | 39.00 | ±1.99 | 29–42 |
| length of breast-milk-only feeding (in months) | 3.86 | ±0.8 | 0–6 | |
| length of breast milk feeding (in months) | 10.9 | ±5.89 | 0–33 | |
| current age (years) | 4.18 | ±1.6 | 2–7 | |
| current weight (kg) | 17.73 | ±5.21 | 9–48 | |
| current body height (cm) | 107.19 | ±13.43 | 80–150 | |
| current BMI (kg/m2) | 15.20 | ±1.79 | 10–24.4 |
| Not Using BLW (NoBLW) (n = 238) | Use of BLW (n = 252) | Total (n = 490) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Place of residence: | p = 0.02175 | ||||||
| City ≥ 100,000 inhabitants | 74 | 31.09 | 107 | 42.46 | 181 | 36.94 | |
| City of 50–100,000 inhabitants | 56 | 23.53 | 63 | 25.00 | 119 | 24.29 | |
| City of 10–50,000 inhabitants | 39 | 16.39 | 33 | 13.10 | 72 | 14.69 | |
| City ≤ 10,000 inhabitants | 18 | 7.56 | 8 | 3.17 | 26 | 5.31 | |
| village | 51 | 21.43 | 41 | 16.27 | 92 | 18.78 | |
| Mother’s education: | p = 0.00410 | ||||||
| Higher | 159 | 66.81 | 199 | 78.97 | 358 | 73.06 | |
| Medium | 60 | 25.21 | 50 | 19.84 | 110 | 22.45 | |
| Professional | 9 | 3.78 | 1 | 0.40 | 10 | 2.04 | |
| Basic | 10 | 4.20 | 2 | 0.79 | 12 | 2.45 | |
| Gender of the child: | p = 0.42328 | ||||||
| Boy | 121 | 50.84 | 119 | 47.22 | 240 | 48.98 | |
| Girl | 117 | 49.16 | 133 | 52.78 | 250 | 51.02 | |
| Current age of the child [in years]: | p = 0.00068 | ||||||
| 2 | 35 | 14.71 | 63 | 25.00 | 98 | 20.00 | |
| 3 | 56 | 23.53 | 50 | 19.84 | 106 | 21.63 | |
| 4 | 33 | 13.87 | 51 | 20.24 | 84 | 17.14 | |
| 5 | 33 | 13.87 | 39 | 15.48 | 72 | 14.69 | |
| 6 | 48 | 20.17 | 24 | 9.52 | 72 | 14.69 | |
| 7 | 33 | 13.87 | 24 | 9.92 | 58 | 11.84 | |
| Child’s current weight [BMI percentile]: | p = 0.47349 | ||||||
| Underweight | 52 | 21.85 | 64 | 25.40 | 116 | 23.67 | |
| Normal weight | 171 | 71.85 | 168 | 66.67 | 339 | 69.18 | |
| Overweight | 12 | 5.04 | 13 | 5.16 | 25 | 5.10 | |
| Obesity | 3 | 1.26 | 7 | 2.78 | 10 | 2.04 | |
| Not Using BLW (NoBLW) (n = 238) | Use of BLW (n = 252) | Total (n = 490) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Method of delivery: | p = 0.00108 | ||||||
| Naturally | 121 | 50.84 | 145 | 57.54 | 266 | 54.29 | |
| Unplanned cesarean section | 49 | 20.59 | 69 | 27.38 | 118 | 24.08 | |
| Planned cesarean section | 68 | 28.57 | 38 | 15.08 | 106 | 21.63 | |
| For how long the baby was fed ONLY breast milk | p < 0.001 | ||||||
| Not fed with breast milk | 20 | 8.40 | 18 | 7.14 | 38 | 7.76 | |
| Less than 1 month | 71 | 29.83 | 41 | 16.27 | 112 | 22.86 | |
| Up to 2 months | 15 | 6.30 | 10 | 3.97 | 25 | 5.1 | |
| Up to 3 months | 10 | 4.20 | 10 | 3.97 | 20 | 4.08 | |
| Up to 4 months | 18 | 7.56 | 9 | 3.57 | 27 | 5.51 | |
| Up to 5 months | 20 | 8.40 | 21 | 8.33 | 41 | 8.37 | |
| Up to 6 months | 71 | 29.83 | 140 | 55.56 | 211 | 43.06 | |
| I do not remember | 13 | 5.46 | 3 | 1.19 | 16 | 3.72 | |
| Breast milk feeding time: | p = 0.00002 | ||||||
| Not fed with breast milk | 10 | 4.2 | 8 | 3.17 | 18 | 3.67 | |
| Less than 1 month | 42 | 17.65 | 20 | 7.94 | 62 | 12.65 | |
| 1–2 months | 27 | 11.34 | 22 | 8.73 | 49 | 10.00 | |
| 3–4 months | 22 | 9.24 | 20 | 7.94 | 42 | 8.57 | |
| 5–6 months | 22 | 9.24 | 8 | 3.17 | 30 | 6.12 | |
| 6–12 months | 45 | 18.91 | 39 | 15.48 | 84 | 17.14 | |
| 13–24 months | 42 | 17.65 | 74 | 29.37 | 116 | 23.67 | |
| Over 24 months | 20 | 8.4 | 48 | 19.05 | 68 | 13.88 | |
| I continue to feed | 6 | 2.52 | 12 | 4.76 | 18 | 3.67 | |
| I do not remember | 2 | 0.84 | 1 | 0.40 | 3 | 0.61 | |
| Timing of the CF: | p < 0.001 | ||||||
| Before 4 months of age | 15 | 6.30 | 0 | 0 | 15 | 3.06 | |
| Between 4–6 months of age | 141 | 59.24 | 83 | 32.94 | 224 | 45.71 | |
| After the baby is 6 months old | 78 | 32.77 | 168 | 66.67 | 246 | 50.20 | |
| I do not remember | 4 | 1.68 | 1 | 0.40 | 5 | 1.02 | |
| Introducing puree * during a child’s complementary feeding: | p < 0.001 | ||||||
| Yes | 229 | 96.22 | 188 | 74.60 | 417 | 85.10 | |
| Not | 5 | 2.10 | 62 | 24.60 | 67 | 13.67 | |
| I do not remember | 4 | 1.68 | 2 | 0.79 | 6 | 1.22 | |
| Introduction of puree with lumps ** during child’s complementary feeding | p = 0.00261 | ||||||
| Yes | 156 | 65.55 | 189 | 75.00 | 345 | 70.41 | |
| Not | 62 | 26.05 | 58 | 23.02 | 120 | 24.49 | |
| I do not remember | 20 | 8.4 | 5 | 1.98 | 25 | 5.10 | |
| The group of food products with which CF was started | p = 0.11954 | ||||||
| Green vegetables | 43 | 18.07 | 54 | 21.43 | 97 | 19.80 | |
| Potatoes | 25 | 10.50 | 22 | 8.73 | 47 | 9.59 | |
| Other vegetables | 114 | 47.90 | 138 | 54.76 | 252 | 51.43 | |
| Domestic fruit (apple, pear, plum) | 34 | 14.29 | 15 | 5.95 | 49 | 10.00 | |
| Citrus fruits | 0 | 0.00 | 2 | 0.79 | 2 | 0.41 | |
| Berries | 1 | 0.42 | 2 | 0.79 | 3 | 0.61 | |
| White meat | 1 | 0.42 | 1 | 0.40 | 2 | 0.41 | |
| Eggs | 2 | 0.84 | 0 | 0.00 | 2 | 0.41 | |
| Gluten-free products | 11 | 4.62 | 7 | 2.78 | 18 | 3.67 | |
| Cereal products containing gluten | 6 | 2.52 | 3 | 1.19 | 9 | 1.84 | |
| All at once | 0 | 0.00 | 7 | 2.78 | 7 | 1.43 | |
| I did not pay attention to it | 1 | 0.42 | 1 | 0.40 | 2 | 0.41 | |
| Fed/supplemented by spoon during complementary feeding: | p < 0.001 | ||||||
| The child ate completely or mostly independently | 4 | 1.68 | 68 | 26.98 | 72 | 14.69 | |
| Baby fully or mostly spoon-fed by an adult | 109 | 45.80 | 19 | 7.54 | 128 | 26.12 | |
| Baby half fed by an adult with a spoon, half eating independently | 125 | 52.52 | 165 | 65.48 | 290 | 59.18 | |
| When expanding the diet, did you allow your child to decide for himself/herself what to eat? | p < 0.001 | ||||||
| Yes | 80 | 33.61 | 183 | 72.62 | 263 | 53.67 | |
| Sometimes | 101 | 42.44 | 59 | 23.41 | 160 | 32.65 | |
| Not | 57 | 23.95 | 10 | 3.97 | 67 | 13.67 | |
| When expanding the diet, did you let your child decide how much to eat? | p = 0.00008 | ||||||
| Yes | 192 | 80.67 | 236 | 93.65 | 428 | 87.35 | |
| Sometimes | 32 | 13.45 | 12 | 4.76 | 44 | 8.98 | |
| Not | 14 | 5.88 | 4 | 1.59 | 18 | 3.67 | |
| Occurrence of difficulties in introducing new foods to the child during complementary feeding: | p = 0.85869 | ||||||
| There was no | 164 | 68.91 | 177 | 70.24 | 341 | 69.59 | |
| Yes there were | 57 | 23.95 | 61 | 24.21 | 118 | 24.08 | |
| I do not remember | 16 | 6.72 | 14 | 5.56 | 30 | 6.12 | |
| Problems during Complementary Feeding | Not Using BLW (NoBLW) (n = 238) | Use of BLW (n = 252) | Total (n = 490) | p-Value | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Vomiting reflex | 64 | 26.89 | 77 | 30.56 | 141 | 28.77 | p = 0.37047 |
| Spitting food out of mouth | 143 | 60.08 | 173 | 68.65 | 316 | 64.49 | p = 0.04764 |
| Gagging | 56 | 23.53 | 103 | 40.87 | 159 | 32.45 | p = 0.00004 |
| Choking | 13 | 5.46 | 21 | 8.33 | 34 | 6.97 | p = 0.21129 |
| Choked and needed medical attention | 0 | 0 | 1 | 0.40 | 1 | 0.20 | p = 0.33064 |
| Not Using BLW (NoBLW) (n = 238) | Use of BLW (n = 252) | Summary (n = 490) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Using a spoon | 232 | 97.48 | 251 | 99.60 | 483 | 98.57 | p = 0.04766 |
| Using a fork | 231 | 97.06 | 250 | 99.21 | 481 | 98.16 | p = 0.07682 |
| Using a fork and knife at the same time | 106 | 44.54 | 113 | 44.84 | 219 | 44.69 | p = 0.94616 |
| Average age of entry into service: | |||||||
| By teaspoon (in months) | 17.8 | 15.0 | 16.4 | p = 0.00001 | |||
| Fork (in months) | 20.9 | 17.3 | 19.1 | p < 0.001 | |||
| With a fork and knife at the same time (in years) | 3.8 | 3.4 | 3.6 | p = 0.00275 | |||
| Not Using BLW (NoBLW) (n = 238) | Use of BLW (n = 252) | Total (n = 490) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Parent’s perception of food: | p = 0.16666 | ||||||
| The child often does not want to eat and I have to encourage/force him to do so | 73 | 30.67 | 44 | 17.46 | 117 | 23.88 | |
| The child has an appetite and eats almost everything he is given | 129 | 54.20 | 133 | 52.78 | 262 | 53.47 | |
| The child does not want to eat, but I do not force him to | 25 | 10.50 | 68 | 26.98 | 93 | 18.98 | |
| I did not pay attention to it | 11 | 4.62 | 7 | 2.78 | 18 | 3.67 | |
| Do you think your child is an picky eater? | p = 0.04766 | ||||||
| Not | 152 | 63.87 | 178 | 70.63 | 330 | 67.35 | |
| I do not know | 24 | 10.08 | 21 | 8.33 | 45 | 9.18 | |
| Yes | 62 | 26.05 | 53 | 21.03 | 115 | 23.47 | |
| Does your child only eat dishes with a certain consistency (e.g., mush, lumps, small pieces)? | p = 0.07682 | ||||||
| No, can and does eat meals with different consistencies | 222 | 93.28 | 244 | 96.83 | 466 | 95.1 | |
| I do not know/difficult to say | 4 | 1.68 | 2 | 2.38 | 6 | 1.22 | |
| Yes | 12 | 5.04 | 6 | 0.79 | 18 | 3.67 | |
| Does the child only eat dishes with a specific taste (e.g., only sweet, only salty)? | p = 0.94616 | ||||||
| Yes, he only consumes products with the flavor of his choice. | 16 | 6.72 | 10 | 3.97 | 26 | 5.31 | |
| I do not know/difficult to say | 12 | 5.04 | 13 | 5.16 | 25 | 5.10 | |
| No, it consumes products from different taste groups. | 210 | 88.24 | 229 | 90.87 | 439 | 89.59 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Białek-Dratwa, A.; Kowalski, O. Complementary Feeding Methods, Feeding Problems, Food Neophobia, and Picky Eating among Polish Children. Children 2024, 11, 45. https://doi.org/10.3390/children11010045
Białek-Dratwa A, Kowalski O. Complementary Feeding Methods, Feeding Problems, Food Neophobia, and Picky Eating among Polish Children. Children. 2024; 11(1):45. https://doi.org/10.3390/children11010045
Chicago/Turabian StyleBiałek-Dratwa, Agnieszka, and Oskar Kowalski. 2024. "Complementary Feeding Methods, Feeding Problems, Food Neophobia, and Picky Eating among Polish Children" Children 11, no. 1: 45. https://doi.org/10.3390/children11010045