
The Diagnostic Process for Children with Autism Spectrum Disorder: A Preliminary Study of Jordanian Parents’ Perspectives

Abstract
:1. Introduction
1.1. Literature Review
1.2. The Current Status of Diagnosing ASD in Jordan
2. Materials and Methods
2.1. Research Design
2.2. Ethical Consideration
2.3. Participants
2.4. Data Collection
2.5. Data Analysis
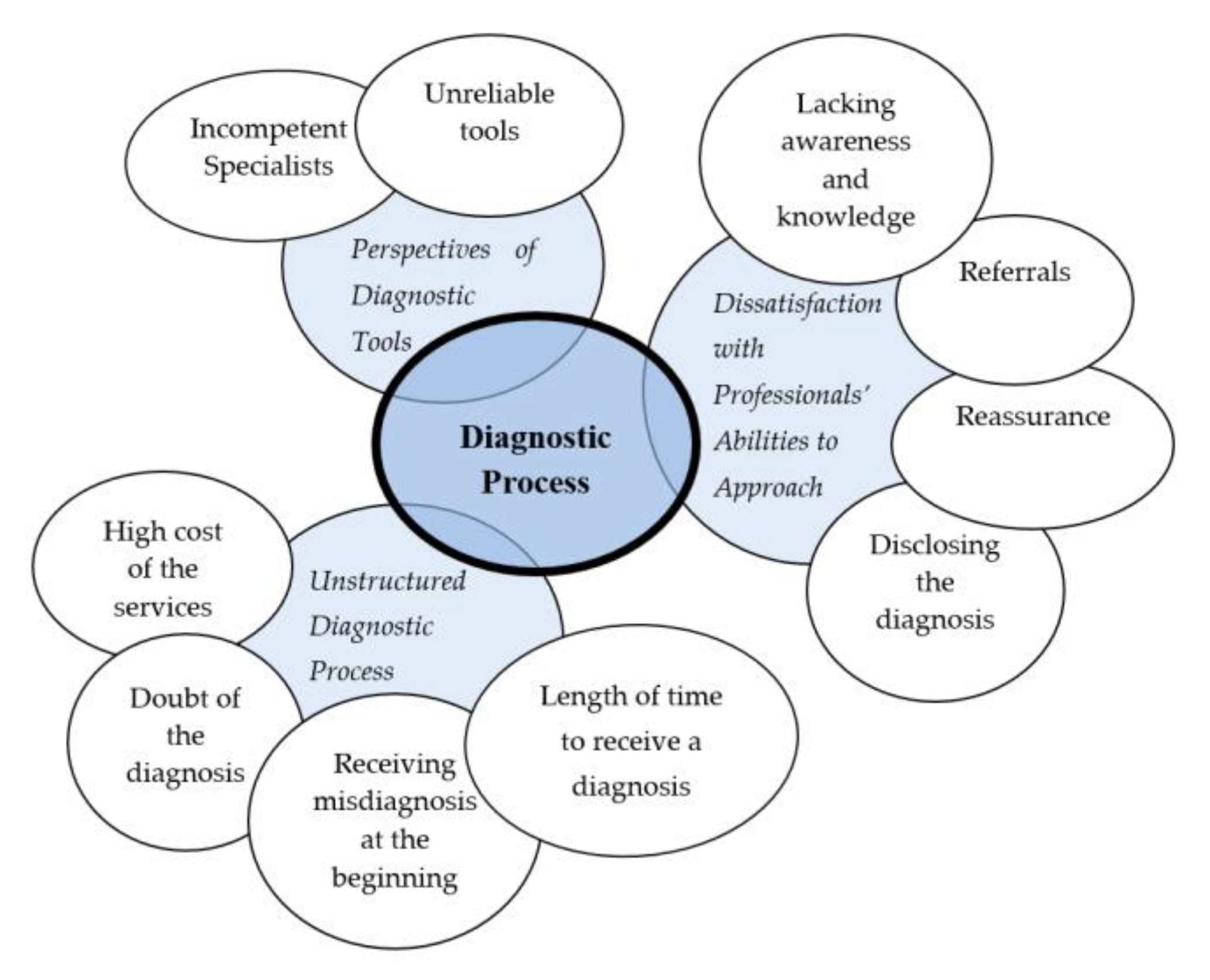
3. Results
3.1. Dissatisfaction with Professionals’ Abilities to Approach Parents
3.2. Unstructured Diagnostic Process
3.3. Perspectives on Diagnostic Tools
4. Discussion
4.1. Dissatisfaction with Professionals’ Abilities to Approach Parents
4.2. Unstructured Diagnostic Process
4.3. Perspectives on Diagnostic Tools
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berenguer, C.; Baixauli, I.; Gómez, S.; Andrés, M.D.E.P.; De Stasio, S. Exploring the impact of augmented reality in children and adolescents with autism spectrum disorder: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 6143. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, T.C.; Nassar, N.; Boulton, K.A.; Guastella, A.J.; Lain, S.J. Estimating the Prevalence of Autism Spectrum Disorder in New South Wales, Australia: A Data Linkage Study of Three Routinely Collected Datasets. J. Autism Dev. Disord. 2023, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bougeard, C.; Picarel-Blanchot, F.; Schmid, R.; Campbell, R.; Buitelaar, J. Prevalence of autism spectrum disorder and co-morbidities in children and adolescents: A systematic literature review. Front. Psychiatry 2021, 12, 744709. [Google Scholar] [CrossRef] [PubMed]
- Russell, G.; Norwich, B. Dilemmas, diagnosis and de-stigmatization: Parental perspectives on the diagnosis of autism spectrum disorders. Clin. Child Psychol. Psychiatry 2012, 17, 229–245. [Google Scholar] [CrossRef] [PubMed]
- Zablotsky, B.; Black, L.I.; Maenner, M.J.; Schieve, L.A.; Danielson, M.L.; Bitsko, R.H.; Boyle, C.A. Prevalence and trends of developmental disabilities among children in the United States: 2009–2017. Pediatrics 2019, 144, e20190811. [Google Scholar] [CrossRef] [PubMed]
- Crane, L.; Chester, J.W.; Goddard, L.; Henry, L.A.; Hill, E. Experiences of autism diagnosis: A survey of over 1000 parents in the United Kingdom. Autism 2016, 20, 153–162. [Google Scholar] [CrossRef]
- Crane, L.; Batty, R.; Adeyinka, H.; Goddard, L.; Henry, L.A.; Hill, E.L. Autism diagnosis in the United Kingdom: Perspectives of autistic adults, parents and professionals. J. Autism Dev. Disord. 2018, 48, 3761–3772. [Google Scholar] [CrossRef] [Green Version]
- MacKenzie, K.T.; Mazefsky, C.A.; Eack, S.M. Obtaining a First Diagnosis of Autism Spectrum Disorder: Descriptions of the Diagnostic Process and Correlates of Parent Satisfaction from a National Sample. J. Autism Dev. Disord. 2022, 1–14. [Google Scholar] [CrossRef]
- McMorris, C.A.; Cox, E.; Hudson, M.; Liu, X.; Bebko, J.M. The diagnostic process of children with autism spectrum disorder: Implications for early identification and intervention. J. Dev. Disabil. 2013, 19, 42. [Google Scholar]
- Shimomura, H.; Hasunuma, H.; Tokunaga, S.; Taniguchi, Y.; Taniguchi, N.; Fujino, T.; Takeshima, Y. Early Developmental Signs in Children with Autism Spectrum Disorder: Results from the Japan Environment and Children’s Study. Children 2022, 9, 90. [Google Scholar] [CrossRef]
- Bejarano-Martín, Á.; Canal-Bedia, R.; Magán-Maganto, M.; Fernández-Álvarez, C.; Cilleros-Martín, M.V.; Sánchez-Gómez, M.C.; Posada de la Paz, M. Early detection, diagnosis and intervention services for young children with autism spectrum disorder in the European Union (ASDEU): Family and professional perspectives. J. Autism Dev. Disord. 2020, 50, 3380–3394. [Google Scholar] [CrossRef]
- Rivard, M.; Morin, D.; Coulombe, P.; Morin, M.; Mello, C. The diagnostic period for Autism: Risk and protective factors for Family Quality of Life in Early Childhood. J. Autism Dev. Disord. 2022, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Huerta, M.; Lord, C. Diagnostic evaluation of autism spectrum disorders. Pediatr. Clin. 2012, 59, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Chamak, B.; Bonniau, B.; Oudaya, L.; Ehrenberg, A. The autism diagnostic experiences of French parents. Autism 2011, 15, 83–97. [Google Scholar] [CrossRef]
- Eggleston, M.J.; Thabrew, H.; Frampton, C.M.; Eggleston, K.H.; Hennig, S.C. Obtaining an autism spectrum disorder diagnosis and supports: New Zealand parents’ experiences. Res. Autism Spectr. Disord. 2019, 62, 18–25. [Google Scholar] [CrossRef]
- Holliday, E.L.; Stanley, H.C.; Fodstad, J.C.; Minshawi, N.F. Stress and Satisfaction in the Diagnostic Process. In Handbook of Assessment and Diagnosis of Autism Spectrum Disorder; Johnny, L., Ed.; Autism and Child Psychopathology Series; Springer: Cham, Switzerland, 2016; pp. 137–155. [Google Scholar] [CrossRef]
- Höfer, J.; Hoffmann, F.; Kamp-Becker, I.; Poustka, L.; Roessner, V.; Stroth, S.; Bachmann, C.J. Pathways to a diagnosis of autism spectrum disorder in Germany: A survey of parents. Child Adolesc. Psychiatry Ment. Health 2019, 13, 16. [Google Scholar] [CrossRef] [PubMed]
- Goin-Kochel, R.P.; Mackintosh, V.H.; Myers, B.J. How many doctors does it take to make an autism spectrum diagnosis? Autism 2006, 10, 439–451. [Google Scholar] [CrossRef] [PubMed]
- McCrimmon, A.W.; Gray, S.M. A systematic review of factors relating to parental satisfaction with the diagnostic process for autism spectrum disorder. Rev. J. Autism Dev. Disord. 2021, 8, 334–349. [Google Scholar] [CrossRef]
- Moh, T.A.; Magiati, I. Factors associated with parental stress and satisfaction during the process of diagnosis of children with autism spectrum disorders. Res. Autism Spectr. Disord. 2012, 6, 293–303. [Google Scholar] [CrossRef]
- Siklos, S.; Kerns, K.A. Assessing the diagnostic experiences of a small sample of parents of children with autism spectrum disorders. Res. Dev. Disabil. 2007, 28, 9–22. [Google Scholar] [CrossRef]
- Dababnah, S.; Bulson, K. “On the sidelines”: Access to autism-related services in the West Bank. J. Autism Dev. Disord. 2015, 45, 4124–4134. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo, N.J.; McIntyre, L.L.; McWhirter, E.H. Sociodemographic differences in parental satisfaction with an autism spectrum disorder diagnosis. J. Intellect. Dev. Disabil. 2015, 40, 147–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutton, A.M.; Caron, S.L. Experiences of families with children with autism in rural New England. Focus Autism Other Dev. Disabl. 2005, 20, 180–189. [Google Scholar] [CrossRef]
- Sansosti, F.J.; Lavik, K.B.; Sansosti, J.M. Family experiences through the autism diagnostic process. Focus Autism Other Dev. Disabl. 2012, 27, 81–92. [Google Scholar] [CrossRef]
- Makino, A.; Hartman, L.; King, G. Parent Experiences of Autism Spectrum Disorder Diagnosis: A Scoping Review. Rev. J. Autism Dev. Disord. 2021, 8, 267–284. [Google Scholar] [CrossRef]
- Small, R.; Belluigi, D.Z. Parents’ Reported Satisfaction of Their Children’s Assessment and Diagnoses of ASD: A Cross-Country Systematic Literature Review. Rev. J. Autism Dev. Disord. 2023, 1–13. [Google Scholar] [CrossRef]
- Calzada, L.; Pistrang, N.; Mandy, W. High-functioning autism and Asperger’s disorder: Utility and meaning for families. J. Autism Dev. Disord. 2012, 42, 230–243. [Google Scholar] [CrossRef]
- Evans, K.; van der Meer, L.; Eggleston, M.J.; Taylor, L.J.; Thabrew, H.; Waddington, H.; Whitehouse, A.J. A survey of autistic adults from New Zealand on the autism diagnostic process during adolescence and adulthood. J. Autism Dev. Disord. 2022, 52, 771–781. [Google Scholar] [CrossRef]
- Jones, L.; Goddard, L.; Hill, E.L.; Henry, L.A.; Crane, L. Experiences of Receiving a Diagnosis of Autism Spectrum Disorder: A Survey of Adults in the United Kingdom. J. Autism Dev. Disord. 2014, 44, 3033–3044. [Google Scholar] [CrossRef]
- Braiden, H.; Bothwell, J.; Duffy, J. Parents’ Experience of the Diagnostic Process for Autistic Spectrum Disorders. Child Care Pract. 2010, 16, 377–389. [Google Scholar] [CrossRef]
- Wong, V.; Yu, Y.; Keyes, M.L.; McGrew, J.H. Pre-diagnostic and diagnostic stages of autism spectrum disorder: A parent perspective. Child Care Pract. 2017, 23, 195–217. [Google Scholar] [CrossRef] [Green Version]
- Kanfiszer, L.; Davies, F.; Collins, S. ‘I was just so different’: The experiences of women diagnosed with an autism spectrum disorder in adulthood in relation to gender and social relationships. Autism 2017, 21, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Alallawi, B.; Hastings, R.P.; Gray, G. A systematic scoping review of social, educational, and psychological research on individuals with autism spectrum disorder and their family members in Arab countries and cultures. Rev. J. Autism Dev. Disord. 2020, 7, 364–382. [Google Scholar] [CrossRef] [Green Version]
- Abualhoul, M.; Amayreh, A. Individuals with Autism Spectrum Disorders In Jordan An Overview Of the Literature NBlogs of Civil Servants of the Republic of Tatarstan in Social. Resmilitaris 2022, 12, 47–54. [Google Scholar]
- al-Zyoud, N.; Hyassat, M. Mental Health of Jordanian Parents of Children with Autism Spectrum Disorder during COVID-19: A qualitative study. Int. J. Spec. Educ. 2023, 38, 34–42. [Google Scholar] [CrossRef]
- Dardas, L.A. Stress, coping strategies, and quality of life among Jordanian parents of children with Autistic Disorder. Autism 2014, 4, 2. [Google Scholar] [CrossRef] [Green Version]
- Thompson, S. The Current Situation of Persons with Disabilities in Jordan. Institute of Development Studies. Available online: https://assets.publishing.service.gov.uk/media/5bb22804ed915d258ed26e2c/Persons_with_disabilities_in_Jordan.pdf (accessed on 1 April 2023).
- Alkinj, I.; Pereira, A.; Santos, P. Educators’ Attitudes towards the Inclusion of Students with Autism Spectrum Disorder (ASD) in Jordanian Public Schools. Rev. Bras. Educ. Espec. 2022, 28, e0157. [Google Scholar] [CrossRef]
- Shattnawi, K.; BaniSaeed, M.; Al-Natour, A.; Al-Hammouri, M.; Al-Azzam, M.; Joseph, R.A. Parenting a child with autism spectrum disorder: Perspective of Jordanian mothers. J. Transcult. Nurs. 2021, 32, 474–483. [Google Scholar] [CrossRef]
- Alqhazo, M.T.; Hatamleh, L.S.; Bashtawi, M. Phonological and lexical abilities of Jordanian children with autism. Appl. Neuropsychol. Child. 2018, 9, 116–124. [Google Scholar] [CrossRef]
- Bryman, A. Social Research Methods, 4th ed.; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Creswell, J.W.; Creswell, J.D. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 5th ed.; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Leavy, P. Research Design: Quantitative, Qualitative, Mixed Methods, Arts-Based, and Community-Based Participatory Research Approaches; Guilford Publications: New York, NY, USA, 2022. [Google Scholar]
- Lune, H.; Berg, B.L. Qualitative Research Methods for the Social Sciences, 9th ed.; Pearson: Boston, MA, USA, 2017. [Google Scholar]
- Dawson, C. Practical Research Methods: A User-Friendly Guide to Mastering Research Techniques and Projects, 3rd ed.; How To Books Ltd.: Oxford, UK, 2007. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, C.; Joffe, H. Intercoder Reliability in Qualitative Research: Debates and Practical Guidelines. Int. J. Qual. Methods 2020, 19, 1609406919899220. [Google Scholar] [CrossRef]
- Reed, P.; Osborne, L.A. Diagnostic practice and its impacts on parental health and child behaviour problems in autism spectrum disorders. Arch. Dis. Child. 2012, 97, 927–931. [Google Scholar] [CrossRef]
- Koegel, L.K.; Koegel, R.L.; Ashbaugh, K.; Bradshaw, J. The importance of early identification and intervention for children with or at risk for autism spectrum disorders. Int. J. Speech Lang. Pathol. 2014, 16, 50–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, S.; Salisbury, H. ‘You know what boys are like’: Pre-diagnosis experiences of parents of children with autism spectrum conditions. Br. J. Gen. Pract. 2012, 62, e378–e383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamak, B.; Bonniau, B. Changes in the diagnosis of autism: How parents and professionals act and react in France. Cult. Med. Psychiatry 2013, 37, 405–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yi, H.; Siu, Q.; Ngan, O.; Chan, D. Parents’ experiences of screening, diagnosis, and intervention for children with autism spectrum disorder. Am. J. Orthopsychiatry 2020, 90, 297–311. [Google Scholar] [CrossRef] [PubMed]
- Fallowfield, L.; Jenkins, V. Communicating sad, bad, and difficult news in medicine. Lancet 2004, 363, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Graungaard, A.H.; Skov, L. Why do we need a diagnosis? A qualitative study of parents’ experiences, coping and needs, when the newborn child is severely disabled. Child Care Health Dev. 2007, 33, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Chiu, Y.N.; Chou, M.C.; Lee, J.C.; Wong, C.C.; Chou, W.J.; Wu, Y.Y.; Gau, S.S.F. Determinants of maternal satisfaction with diagnosis disclosure of autism. J. Formos. Med. Assoc. 2014, 113, 540–548. [Google Scholar] [CrossRef] [Green Version]
- Penner, M.; King, G.A.; Hartman, L.; Anagnostou, E.; Shouldice, M.; Hepburn, C.M. Community general pediatricians’ perspectives on providing autism diagnoses in Ontario, Canada: A qualitative study. J. Dev. Behav. Pediatr. 2017, 38, 593. [Google Scholar] [CrossRef]
- Dardas, L.A.; Simmons, L.A. The stigma of mental illness in Arab families: A concept analysis. J. Psychiatr. Ment. Health Nurs. 2015, 22, 668–679. [Google Scholar] [CrossRef]
- Hyassat, M. Jordanian Parents of Young Children with Disabilities Perspectives on Care, Coping and Service Provision, 1st ed.; Scholars’ Press: Saarbrücken, Germany, 2013. [Google Scholar]
- Jacobs, D.; Steyaert, J.; Dierickx, K.; Hens, K. Implications of an autism spectrum disorder diagnosis: An interview study of how physicians experience the diagnosis in a young child. J. Clin. Med. 2018, 7, 348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oswald, D.P.; Haworth, S.M.; Mackenzie, B.K.; Willis, J.H. Parental report of the diagnostic process and outcome: ASD compared with other developmental disabilities. Focus Autism Other Dev. Disabl. 2017, 32, 152–160. [Google Scholar] [CrossRef]
- Huang, Y.; Arnold, S.R.C.; Foley, K.R.; Trollor, J.N. Diagnosis of autism in adulthood: A scoping review. Autism 2020, 24, 1311–1327. [Google Scholar] [CrossRef]
- Fusar-Poli, L.; Brondino, N.; Politi, P.; Aguglia, E. Missed diagnoses and misdiagnoses of adults with autism spectrum disorder. Eur. Arch. Psychiatry Clin. Neurosci. 2022, 272, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Farrugia, D. Exploring stigma: Medical knowledge and the stigmatisation of parents of children diagnosed with autism spectrum disorder. Sociol. Health Illn. 2009, 31, 1011–1027. [Google Scholar] [CrossRef]
- Leslie, D.L.; Martin, A. Health care expenditures associated with autism spectrum disorders. Arch. Pediatr. Adolesc. Med. 2007, 161, 350–355. [Google Scholar] [CrossRef] [Green Version]
- Zuckerman, K.E.; Lindly, O.J.; Reyes, N.M.; Chavez, A.E.; Macias, K.; Smith, K.N.; Reynolds, A. Disparities in diagnosis and treatment of autism in Latino and non-Latino white families. Pediatrics 2017, 139, e20163010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timimi, S.; Milton, D.; Bovell, V.; Kapp, S.; Russell, G. Deconstructing diagnosis: Four commentaries on a diagnostic tool to assess individuals for autism spectrum disorders. Autonomy 2019, 1, AR26. [Google Scholar]
- Mayes, S.D.; Calhoun, S.L.; Murray, M.J.; Morrow, J.D.; Yurich, K.K.; Mahr, F.; Petersen, C. Comparison of scores on the Checklist for Autism Spectrum Disorder, Childhood Autism Rating Scale, and Gilliam Asperger’s Disorder Scale for children with low functioning autism, high functioning autism, Asperger’s disorder, ADHD, and typical development. J. Autism Dev. Disord. 2009, 39, 1682–1693. [Google Scholar] [CrossRef]
- Hanratty, J.; Livingstone, N.; Robalino, S.; Terwee, C.B.; Glod, M.; Oono, I.P.; McConachie, H. Systematic review of the measurement properties of tools used to measure behaviour problems in young children with autism. PLoS ONE 2015, 10, e0144649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, C.L.; Goddard, L.; Hill, E.L.; Henry, L.A.; Crane, L. Experiences of diagnosing autism spectrum disorder: A survey of professionals in the United Kingdom. Autism 2016, 20, 820–831. [Google Scholar] [CrossRef] [PubMed]
- Choi, S. Rethinking the Validity of Autism Assessment. Ph.D. Thesis, University of California, Santa Barbara, CA, USA, June 2022. [Google Scholar]
- Higher Council for the Rights of Persons with Disabilities. Executive Summary of the Second Annual Report on the Status and Rights of Persons with Disabilities in the Hashemite Kingdom of Jordan. Available online: http://www.hcd.gov.jo/sites/default/files/Exectuve%20Summary%202.pdf (accessed on 4 April 2023).


{kind=link}
| Parent | Child with ASD | |||||||
|---|---|---|---|---|---|---|---|---|
| No. | Age | Education | Monthly Income JOD | Urban/Rural | Pseudonym | Age | Gender | Functional Level |
| 1 | 45 | Bachelor | 600 | Urban | Sameer | 7 | Boy | High |
| 2 | 40 | Bachelor | 650 | Urban | Rami | 8 | Girl | High |
| 3 | 39 | Bachelor | Not given | Urban | Faris | 8 | Boy | High |
| 4 | 37 | Diploma | 600 | Urban | Laith | 7 | Boy | High |
| 5 | 45 | Bachelor | 1100 | Urban | Oon | 10 | Boy | Middle |
| 6 | 42 | High School | 500 | Urban | Farah | 6 | Girl | High |
| 7 | 47 | Diploma | 450 | Urban | Naser | 10 | Boy | High |
| 8 | 42 | Ph.D. | 1600 | Urban | Nashmi | 7 | Boy | Middle |
| 9 | 30 | Bachelor | 800 | Urban | Nedal | 6 | Boy | Middle |
| 10 | 45 | Bachelor | 600 | Rural | Odai | 7 | Boy | Middle |
| 11 | 31 | Bachelor | 400 | Urban | Saad | 6 | Boy | Low |
| 12 | 45 | Diploma | 650 | Urban | Bader | 9 | Boy | High |
| 13 | 44 | High school | 700 | Urban | Majd | 11 | Boy | High |
| 14 | 44 | High school | Not given | Rural | Leen | 9 | Girl | High |
| 15 | 38 | Bachelor | 600 | Urban | Reem | 7 | Girl | High |
| 16 | 37 | Masters | 1300 | Urban | Baram | 6 | Boy | Low |
| 17 | 30 | Bachelor | 1000 | Urban | Jad | 5 | Boy | High |
| 18 | 44 | Masters | 1500 | Urban | Zaid | 11 | Boy | Middle |
|
| Child’s Pseudonym | Age at First Parental Concerns | First Symptoms | First Professional Contact | Time Delay between the First Concerns and the Diagnosis | Who Confirmed the Final Diagnosis |
|---|---|---|---|---|---|
| 1. Sameer | 30 months | Language delay | Pediatrician | 30 months | Psychologist |
| 2. Rami | 36 months | Avoiding eye contact | Pediatrician | 24 months | Psychologist |
| 3. Faris | Did not recall | Not responding to his name | Pediatrician | - | Special education teacher |
| 4. Laith | 36 months | Stereotyped behaviors | GP | 20 months | Special education teacher |
| 5. Oon | Did not recall | Language delay | Pediatrician | - | Special education teacher |
| 6. Farah | 24 months | Stereotyped behaviors | Pediatrician | 36 months | Psychologist |
| 7. Naser | 40 months | Language delay | GP | 48 months | Special education teacher |
| 8. Nashmi | 30 months | Avoiding eye contact | Pediatrician | 12 months | Special education teacher |
| 9. Nedal | 34 months | Hyperactivity | Pediatrician | 24 months | Special education teacher |
| 10. Odai | 24 months | Language delay | Pediatrician | 30 months | Psychologist |
| 11. Saad | 26 months | Not responding to his name | Pediatrician | 18 months | Psychologist |
| 12. Bader | 38 months | Stereotyped behaviors | Pediatrician | 34 months | Special education teacher |
| 13. Majd | Did not recall | Not responding to his name | Pediatrician | - | Psychologist |
| 14. Leen | Did not recall | Language delay | Pediatrician | - | Psychologist |
| 15. Reem | 36 | Avoiding eye contact | Pediatrician | 20 months | Special education teacher |
| 16. Baram | 32 months | Language delay | GP | 24 months | Psychologist |
| 17. Jad | 36 months | Language delay | Pediatrician | 20 months | Psychologist |
| 18. Zaid | 36 months | Language delay | Pediatrician | 14 months | Psychologist |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hyassat, M.; Al-Makahleh, A.; Rahahleh, Z.; Al-Zyoud, N. The Diagnostic Process for Children with Autism Spectrum Disorder: A Preliminary Study of Jordanian Parents’ Perspectives. Children 2023, 10, 1394. https://doi.org/10.3390/children10081394
Hyassat M, Al-Makahleh A, Rahahleh Z, Al-Zyoud N. The Diagnostic Process for Children with Autism Spectrum Disorder: A Preliminary Study of Jordanian Parents’ Perspectives. Children. 2023; 10(8):1394. https://doi.org/10.3390/children10081394
Chicago/Turabian StyleHyassat, Mizyed, Ahmad Al-Makahleh, Zahraa Rahahleh, and Nawaf Al-Zyoud. 2023. "The Diagnostic Process for Children with Autism Spectrum Disorder: A Preliminary Study of Jordanian Parents’ Perspectives" Children 10, no. 8: 1394. https://doi.org/10.3390/children10081394