
Impaired Personality Functioning in Children and Adolescents Assessed with the LoPF-Q 6-18 PR in Parent-Report and Convergence with Maladaptive Personality Traits and Personality Structure in School and Clinic Samples
 , , and
, , and
Abstract
:1. Introduction
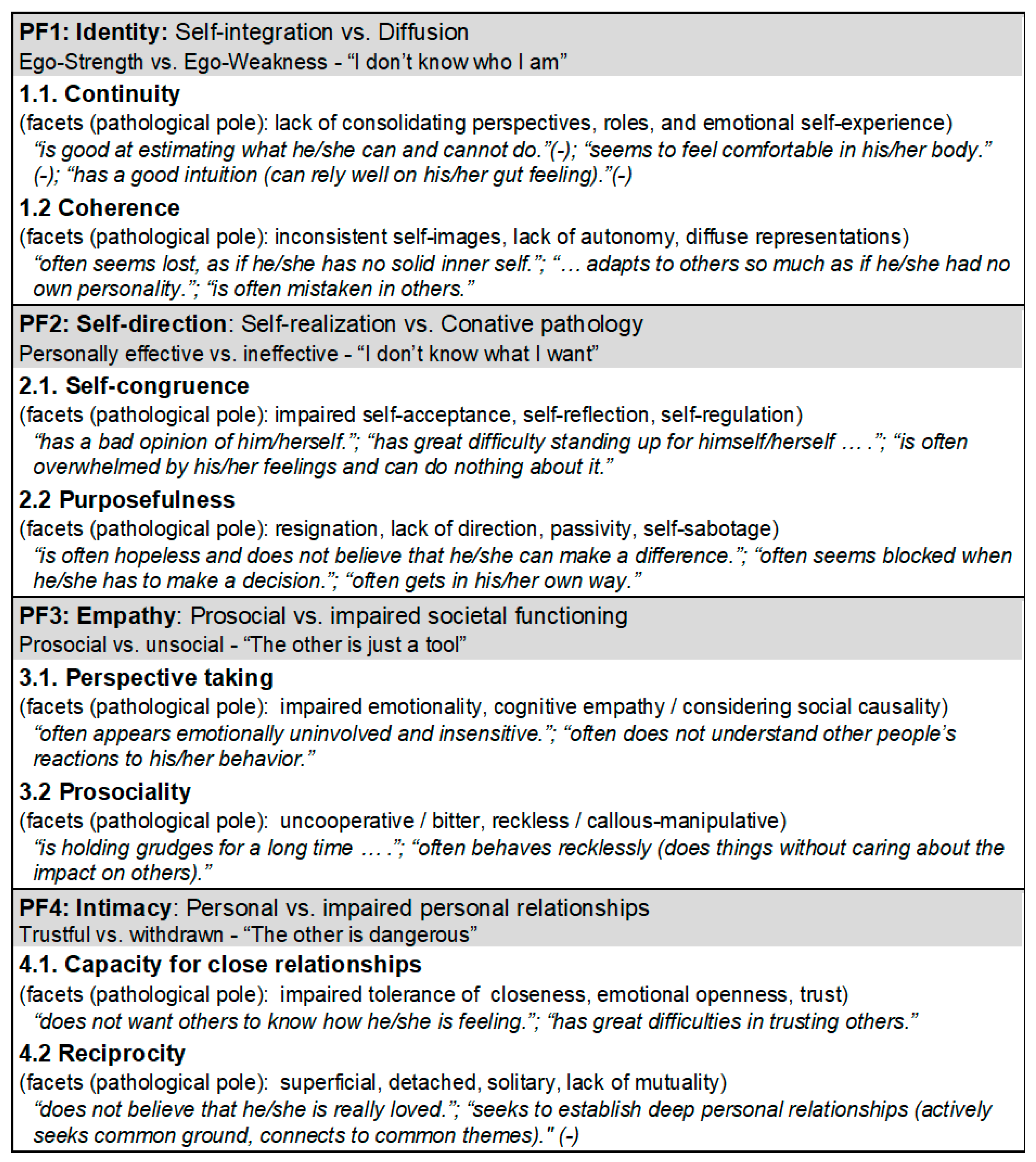
Development of the Age-Specific Assessment Tool LoPF-Q 6-18 PR
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.2.1. Adolescents
2.2.2. Parents
2.3. Data Analytic Plan
3. Results
3.1. Descriptive Analyses
3.2. Reliability and Correlational Informant Agreement between Parent-Report and Self-Report
3.3. Factorial Validity
3.4. Covariation with PD Pathology
3.5. Convergence with Broader Psychopathology, Maladaptive Traits, and Personality Structure
3.6. Short Version of the LoPF-Q 12-18
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. ICD-11 Clinical Descriptions and Diagnostic Guidelines for Mental and Behavioural Disorders; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Taskforce OPD-CA-2 (Ed.) OPD-KJ-2—Operationalisierte Psychodynamische Diagnostik im Kindes- und Jugendalter: Grundlagen und Manual. 3. Aufl. [OPD-CA-2—Operationalized Psychodynamic Diagnosis in Childhood and Adolescence: Theoretical Basis and User Manual, 3rd ed.; Hogrefe: Göttingen, Germany, 2020. [Google Scholar]
- Gozi, A. Highlights of ICD-11 Classification of Mental, Behavioral, and Neurodevelopmental Disorders. Indian J. Psychiatry 2019, 13, 11–17. [Google Scholar] [CrossRef]
- Schmeck, K.; Birkhölzer, M. The Classification of Personality Disorders in ICD-11. Z. Fur Kinder-Und Jugendpsychiatrie Und Psychother. 2020, 49, 480–485. [Google Scholar] [CrossRef]
- Solmi, M.; Radua, J.; Olivola, M.; Croce, E.; Soardo, L.; Salazar de Pablo, G.; Shin, J.I.; Kirkbride, J.B.; Jones, P.; Kim, J.H.; et al. Age at onset of mental disorders worldwide: Large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatry 2022, 27, 281–295. [Google Scholar] [CrossRef]
- Lahey, B.B.; Zald, D.H.; Hakes, J.K.; Krueger, R.F.; Rathouz, P.J. Patterns of heterotypic continuity associated with the cross-sectional correlational structure of prevalent mental disorders in adults. JAMA Psychiatry 2014, 71, 989–996. [Google Scholar] [CrossRef] [PubMed]
- d’Huart, D.; Steppan, M.; Seker, S.; Bürgin, D.; Boonmann, C.; Birkhölzer, M.; Jenkel, N.; Fegert, J.M.; Schmid, M.; Schmeck, K. Prevalence and 10-year stability of personality disorders from adolescence to young adulthood in a high-risk sample. Front. Psychiatry 2022, 13, 840678. [Google Scholar] [CrossRef] [PubMed]
- Sharp, C.; Ha, C.; Michonski, J.; Venta, A.; Carbone, C. Borderline Personality Disorder in Adolescents: Evidence in Support of the Childhood Interview for DSM-IV Borderline Personality Disorder in a Sample of Adolescent Inpatients. Compr. Psychiatry 2012, 53, 765–774. [Google Scholar] [CrossRef]
- Chanen, A.; Sharp, C.; Hoffman, P. Prevention and Early Intervention for Borderline Personality Disorder: A Novel Public Health Priority. World J. Psychiatry 2017, 16, 215–216. [Google Scholar] [CrossRef]
- Hutsebaut, J.; Willemsen, E.; Bachrach, N.; Van, R. Improving Access to and Effectiveness of Mental Health Care for Personality Disorders: The Guideline-Informed Treatment for Personality Disorders (GIT-PD) Initiative in the Netherlands. Borderline Personal. Disord. Emot. Dysregulation 2020, 7, 16. [Google Scholar] [CrossRef]
- Schmeck, K.; Weise, S.; Schlüter-Müller, S.; Birkhölzer, M.; Fürer, L.; Koenig, J.; Krause, M.; Lerch, S.; Schenk, N.; Valdes, N.; et al. Effectiveness of Adolescent Identity Treatment (AIT) versus DBT-a for the Treatment of Adolescent Borderline Personality Disorder. Personal. Disord. Theory Res. Treat. 2022, 14, 148–160. [Google Scholar] [CrossRef]
- Wertz, J.; Caspi, A.; Ambler, A.; Arseneault, L.; Belsky, D.W.; Danese, A.; Fisher, H.L.; Matthews, T.; Richmond-Rakerd, L.; Moffitt, T.E. Borderline Symptoms at Age 12 Signal Risk for Poor Outcomes during the Transition to Adulthood: Findings from a Genetically Sensitive Longitudinal Cohort Study. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 1165–1177. [Google Scholar] [CrossRef]
- Suzuki, T.; Samuel, D.B.; Pahlen, S.; Krueger, R.F. DSM-5 Alternative Personality Disorder Model Traits as Maladaptive Extreme Variants of the Five-Factor Model: An Item-Response Theory Analysis. J. Abnorm. Psychol. 2015, 124, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Krueger, R.F.; Derringer, J.; Markon, K.E.; Watson, D.; Skodol, A.E. Initial Construction of a Maladaptive Personality Trait Model and Inventory for DSM-5. Psychol. Med. 2012, 42, 1879–1890. [Google Scholar] [CrossRef] [PubMed]
- Bach, B.; Kerber, A.; Aluja, A.; Bastiaens, T.; Keeley, J.W.; Claes, L.; Fossati, A.; Gutierrez, F.; Oliveira, S.E.S.; Pires, R.; et al. International Assessment of DSM-5 and ICD-11 Personality Disorder Traits: Toward a Common Nosology in DSM-5.1. Psychopathology 2020, 53, 179–188. [Google Scholar] [CrossRef]
- Kerber, A.; Schaeuffele, C.; Krieger, T.; Urech, A.; Riper, H.; Berger, T.; Boettcher, J.; Knaevelsrud, C. Differential effects of psychological interventions in online and face-to-face settings on DSM-5 and ICD-11 maladaptive trait domains: An exploratory pilot study. Front. Psychiatry 2021, 12, 648367. [Google Scholar] [CrossRef] [PubMed]
- Oltmanns, J.R.; Widiger, T.A. The Five-Factor Personality Inventory for ICD-11: A Facet-Level Assessment of the ICD-11 Trait Model. Psychol. Assess. 2020, 32, 60–71. [Google Scholar] [CrossRef]
- Bach, B.; Sellbom, M.; Kongerslev, M.; Simonsen, E.; Krueger, R.F.; Mulder, R. Deriving ICD-11 Personality Disorder Domains from Dsm-5 Traits: Initial Attempt to Harmonize Two Diagnostic Systems. Acta Psychiatr. Scand. 2017, 136, 108–117. [Google Scholar] [CrossRef]
- Sellbom, M.; Solomon-Krakus, S.; Bach, B.; Bagby, R.M. Validation of Personality Inventory for DSM-5 (PID-5) Algorithms to Assess ICD-11 Personality Trait Domains in a Psychiatric Sample. Psychol. Assess. 2020, 32, 40–49. [Google Scholar] [CrossRef]
- Kerber, A.; Schultze, M.; Müller, S.; Rühling, R.M.; Wright, A.G.C.; Spitzer, C.; Krueger, R.F.; Knaevelsrud, C.; Zimmermann, J. Development of a Short and ICD-11 Compatible Measure for DSM-5 Maladaptive Personality Traits Using Ant Colony Optimization Algorithms. Assessment 2022, 29, 467–487. [Google Scholar] [CrossRef]
- Goth, K.; Birkhoelzer, M.; Kerber, A.; Krueger, R.F.; Bach, B.; Zimmermann, J. The Personality Inventory for DSM-5 Brief Form + ICD-11—Modified—Adolescent Version (PID5BF+ M A). 2023. Available online: https://academic-tests.com (accessed on 7 July 2023).
- Goth, K.; Birkhoelzer, M.; Kerber, A.; Krueger, R.F.; Bach, B.; Zimmermann, J. The Personality Inventory for DSM-5 Brief Form + ICD-11—Modified—Children and Adolescents—Informant Report Form (PID5BF+ M CA IRF). 2023. Available online: https://academic-tests.com (accessed on 7 July 2023).
- Gluschkoff, K.; Jokela, M.; Rosenström, T. General Psychopathology Factor and Borderline Personality Disorder: Evidence for Substantial Overlap from Two Nationally Representative Surveys of U. S. Adults. Personal. Disord. Theory Res. Treat. 2021, 12, 86–92. [Google Scholar] [CrossRef]
- Sharp, C.; Wall, K. DSM-5 Level of Personality Functioning: Refocusing Personality Disorder on What It Means to Be Human. Annu. Rev. Clin. Psychol. 2021, 17, 313–337. [Google Scholar] [CrossRef]
- Zimmermann, J.; Kerber, A.; Rek, K.; Hopwood, C.J.; Krueger, R.F. A Brief but Comprehensive Review of Research on the Alternative DSM-5 Model for Personality Disorders. Curr. Psychiatry Rep. 2019, 21, 92. [Google Scholar] [CrossRef] [PubMed]
- Kotov, R.; Krueger, R.F.; Watson, D.; Achenbach, T.M.; Althoff, R.R.; Bagby, R.M.; Brown, T.A.; Carpenter, W.T.; Caspi, A.; Clark, L.A.; et al. The Hierarchical Taxonomy of Psychopathology (HiTOP): A Dimensional Alternative to Traditional Nosologies. J. Abnorm. Psychol. 2017, 126, 454–477. [Google Scholar] [CrossRef]
- De Los Reyes, A.; Augenstein, T.M.; Wang, M.; Thomas, S.A.; Drabick, D.A.; Burgers, D.E.; Rabinowitz, J. The validity of the multi-informant approach to assessing child and adolescent mental health. Psychol. Bull. 2015, 141, 858. [Google Scholar] [CrossRef] [PubMed]
- Achenbach, T.M. Manual for the Child Behavior Checklist/4-18 and 1991 Profile; University of Vermont, Department of Psychiatry: Burlington, VT, USA, 1991. [Google Scholar]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, C.R.; Kamphaus, R.W. BASC-3—Behavior Assessment System for Children, 3rd ed.; NCS Pearson, Inc.: Bloomington, MN, USA, 2015. [Google Scholar]
- Rothbart, M.K.; Ahadi, S.A.; Hershey, K.L.; Fisher, P. Investigations of Temperament at Three to Seven Years: The Children’s Behavior Questionnaire. Child Dev. 2001, 72, 1394–1408. [Google Scholar] [CrossRef]
- Halverson, C.F.; Havill, V.L.; Deal, J.; Baker, S.R.; Victor, J.B.; Pavlopoulos, V.; Besevegis, E.; Wen, L. Personality Structure as Derived from Parental Ratings of Free Descriptions of Children: The Inventory of Child Individual Differences. J. Pers. 2003, 71, 995–1026. [Google Scholar] [CrossRef]
- Vervoort, L.; Vandeweghe, L.; Vandewalle, J.; Van Durme, K.; Vandevivere, E.; Wante, L.; McIntosh, K.; Verbeken, S.; Moens, E.; Goossens, L.; et al. Measuring Punishment and Reward Sensitivity in Children and Adolescents with a Parent-Report Version of the Bis/Bas-Scales. Personal. Individ. Differ. 2015, 87, 272–277. [Google Scholar] [CrossRef]
- Buss, A.H.; Plomin, R. EAS Temperament Survey for Children. Temperament: Early Developing Personality Traits; Erlbaum: Hillsdale, NJ, USA, 1984. [Google Scholar]
- Mervielde, I.; De Fruyt, F. Construction of the Hierarchical Personality Inventory for Children (HiPIC). In Personality Psychology in Europe, Proceedings of the Eight European Conference on Personality Psychology (Ghent, Belgium, 8–12 July 1996); Mervielde, I., Deary, I., De Fruyt, F., Ostendorf, F.O., Eds.; Tilburg University Press: Tilburg, The Netherlands, 1999; pp. 107–127. [Google Scholar]
- Constantino, J.N.; Cloninger, C.R.; Clarke, A.R.; Hashemi, B.; Przybeck, T. Application of the Seven-Factor Model of Personality to Early Childhood. Psychiatry Res. 2002, 109, 229–243. [Google Scholar] [CrossRef]
- Goth, K.; Schmeck, K. Das Junior Temperament und Charakter Inventar“. Eine Inventarfamilie zur Erfassung der Persönlichkeit vom Kindergarten bis zum Jugendalter nach Cloningers Biopsychosozialem Persönlichkeitsmodell; Hofgrefe: Göttingen, Germany, 2009. [Google Scholar]
- Cloninger, C.R.; Przybeck, T.R.; Svrakic, D.M.; Wetzel, R.D. The Temperament and Character Inventory (TCI): A Guide to Its Development and Use; Washington University Center for Psychobiology of Personality: St. Louis, MO, USA, 1994. [Google Scholar]
- Goth, K.; Schmeck, K. AIDA (Assessment of Identity Development in Adolescence) German Version: A Self-Report Questionnaire for Measuring Identity Development in Adolescence—Short Manual; Academic-Tests: Offenbach, Germany, 2018; Available online: https://academic-tests.com (accessed on 7 July 2023). (In German)
- Goth, K.; Birkhölzer, M.; Schmeck, K. LoPF-Q 12-18 (Levels of Personality Functioning Questionnaire) German Version: A Self-Report Questionnaire for Measuring Personality Functioning in Adolescence—Short Manual; Academic-Tests: Offenbach, Germany, 2018; Available online: https://academic-tests.com (accessed on 7 July 2023). (In German)
- Goth, K.; Schrobildgen, C.; Schmeck, K. OPD-CA2-SQ (Operationalised Psychodynamic Diagnosis in Children and Adolescents—Structure Questionnaire) German Version: A Self-Report Questionnaire for Measuring Personality Structure in Adolescence—Short Manual; Academic-Tests: Offenbach, Germany, 2018; Available online: https://academic-tests.com (accessed on 7 July 2023). (In German)
- Sarrar, L.; Goth, K. Defense Mechanisms Reloaded in the Light of Impaired Personality Functioning: An Attempt of Clarification and Simplification Resulting in the DSQ-22-A for Adolescents. Front. Psychiatry 2022, 13, 866837. [Google Scholar] [CrossRef]
- Sharp, C.; Vanwoerden, S.; Odom, A.; Foelsch, P. Culture-Adapted Version English USA of the Self-Report Questionnaire AIDA (Assessment of Identity Development in Adolescence; Authors Goth & Schmeck)—Short Manual; Academic-Tests: Offenbach, Germany, 2018; Available online: https://academic-tests.com (accessed on 7 July 2023).
- Kassin, M.; Hackradt, J. Culture-Adapted Version Spanish Mexico of the Self-Report Questionnaire LoPF-Q 12-18 (Levels of Personality Functioning Questionnaire; Authors Goth & Schmeck)—Short Manual; Academic-Tests: Offenbach, Germany, 2019; Available online: https://academic-tests.com (accessed on 7 July 2023). (In Spanish)
- Cosgun, S.; Cakiroglu, S. Culture-Adapted Version Turkish of the Self-Report Questionnaire LoPF-Q 12-18 (Levels of Personality Functioning Questionnaire; Authors Goth & Schmeck)—Short Manual; Academic-Tests: Offenbach, Germany, 2020; Available online: https://academic-tests.com (accessed on 7 July 2023). (In Turkish)
- Cosgun, S.; Goth, K.; Cakiroglu, S. Levels of Personality Functioning Questionnaire (LoPF-Q) 12-18 Turkish Version: Reliability, Validity, Factor Structure and Relationship with Comorbid Psychopathology in a Turkish Adolescent Sample. J. Psychopathol. Behav. Assess. 2021, 43, 620–631. [Google Scholar] [CrossRef]
- International Test Commission. International Guidelines for Test Use. Int. J. Test. 2001, 1, 93–114. [CrossRef]
- Goth, K.; Birkhölzer, M.; Schmeck, K. Assessment of Personality Functioning in Adolescents with the LoPF-Q 12-18 Self-Report Questionnaire. J. Personal. Assess. 2018, 100, 680–690. [Google Scholar] [CrossRef]
- Zimmermann, R.; Steppan, M.; Zimmermann, J.; Oeltjen, L.; Birkhölzer, M.; Schmeck, K.; Goth, K. A DSM-5 AMPD and ICD-11 Compatible Measure for an Early Identification of Personality Disorders in Adolescence-LoPF-Q 12-18 Latent Structure and Short Form. PLoS ONE 2022, 17, 0269327. [Google Scholar] [CrossRef]
- Birkhölzer, M.; Schmeck, K.; Goth, K. LoPF-Q 6-18 PR (Levels of Personality Functioning Questionnaire, Parent Report) German Version: A Parent-Report Questionnaire for Measuring Impairments in Personality Functioning (IPF) in Children and Adolescents Aged 6–18 Years—Short Manual; Academic-Tests: Offenbach, Germany, 2023; Available online: https://academic-tests.com (accessed on 7 July 2023). (In German)
- Sheehan, D.V.; Sheehan, K.H.; Shytle, R.D.; Janavs, J.; Bannon, Y.; Rogers, J.E.; Milo, K.M.; Stock, S.L.; Wilkinson, B. Reliability and Validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). J. Clin. Psychiatry 2010, 71, 313–326. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th ed.; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD- 10. J. Clin. Psychiatry 1998, 59 (Suppl. 20), 22–33. [Google Scholar] [PubMed]
- Fydrich, T.; Renneberg, B.; Schmitz, B.; Wittchen, H.U. Strukturiertes Klinisches Interview for DSM-IV, Achse II (Persönlichkeitsstörungen)-SKID-II; Hogrefe: Göttingen, Germany, 1997. [Google Scholar]
- Smith, T.L.; Klein, M.H.; Benjamin, L.S. Validation of the Wisconsin Personality Disorders Inventory-IV with the SCID-II. J. Personal. Disord. 2003, 17, 173–187. [Google Scholar] [CrossRef]
- Jucksch, V.; Salbach-Andrae, H.; Lehmkuhl, U. Persönlichkeitsentwicklung Im Kindes- Und Jugendalter. Der Nervenarzt 2009, 80, 1322–1326. [Google Scholar] [CrossRef]
- Kaess, M.; von Ceumern-Lindenstjerna, I.-A.; Parzer, P.; Chanen, A.; Mundt, C.; Resch, F.; Brunner, R. Axis I and II Comorbidity and Psychosocial Functioning in Female Adolescents with Borderline Personality Disorder. Psychopathology 2013, 46, 55–62. [Google Scholar] [CrossRef]
- Hutsebaut, J.; Kamphuis, J.H.; Feenstra, D.J.; Weekers, L.C.; De Saeger, H. Assessing DSM-5-Oriented Level of Personality Functioning: Development and Psychometric Evaluation of the Semi-Structured Interview for Personality Functioning DSM-5 (STiP-5.1). Personal. Disord. Theory Res. Treat 2017, 8, 94–101. [Google Scholar] [CrossRef]
- Weekers, L.C.; Verhoeff, S.C.E.; Kamphuis, J.H.; Hutsebaut, J. Assessing Criterion a in Adolescents Using the Semistructured Interview for Personality Functioning DSM-5. Personal. Disord. Theory Res. Treat. 2020, 12, 312. [Google Scholar] [CrossRef]
- Zettl, M.; Taubner, S.; Hutsebaut, J.; Volkert, J. Psychometric evaluation of the German version of the semi-structured interview for personality functioning DSM-5 (STiP-5.1). Psychother. Psychosom. Med. Psychol. 2019, 69, 499–504. [Google Scholar] [PubMed]
- Birkhölzer, M.; Schlüter-Müller, S.; Goth, K. OPD-CA2-SQ PR (Operationalised Psychodynamic Diagnosis in Children and Adolescents—Structure Questionnaire, Parent Report) German Version: A Parent-Report Questionnaire for Measuring Impairments in Personality Structure in Children and Adolescents Aged 6–18 Years—Short Manual; Academic-Tests: Offenbach, Germany, 2023; Available online: https://academic-tests.com (accessed on 7 July 2023). (In German)
- Döpfner, M.; Melchers, P.; Fegert, J.; Lehmkuhl, G.; Lehmkuhl, U.; Schmeck, K.; Steinhausen, H.C.; Poustka, F. Deutschsprachige Konsensus-Versionen der Child Behavior Checklist (CBCL 4-18), der Teacher Report Form (TRF) und der Youth Self Report Form (YSR). Kindh. Und Entwickl. 1994, 3, 54–59. [Google Scholar]
- Rosseel, Y. Lavaan An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar]
- McDonald, R.P. Test Theory: A Unified Treatment; Erlbaum Associates: Mahwah, NJ, USA, 1999. [Google Scholar]
- Jorgensen, T.D.; Pornprasertmanit, S.; Schoemann, A.M.; Rosseel, Y. semTools: Useful Tools for Structural Equation Modeling, R Package Version 0.5-6; 2022. Available online: https://CRAN.R-project.org/package=semTools (accessed on 7 July 2023).
- Zinbarg, R.E.; Revelle, W.; Yovel, I.; Li, W. Cronbach’s α, Revelle’s β, and Mcdonald’s ωH: Their relations with each other and two alternative conceptualizations of reliability. Psychometrika 2005, 70, 123–133. [Google Scholar] [CrossRef]
- Rodriguez, A.; Reise, S.P.; Haviland, M.G. “Applying bifactor statistical indices in the evaluation of psychological measures”: Correction. J. Personal. Assess. 2016, 98, 444. [Google Scholar] [CrossRef]
- Carlson, E.N.; Vazire, S.; Oltmanns, T.F. Self-other knowledge asymmetries in personality pathology. J. Personal. 2013, 81, 155–170. [Google Scholar] [CrossRef]
- Liang, X.; Yang, Y. An evaluation of WLSMV and Bayesian methods for confirmatory factor analysis with categorical indicators. Int. J. Quant. Res. Educ. 2014, 2, 17–38. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford: New York, NY, USA, 2015. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Erlbaum: Mahwah, NJ, USA, 1988. [Google Scholar]
- Sharp, C.; McLaren, V.; Musetti, A.; Vanwoerden, S.; Hernandez Ortiz, J.; Schmeck, K.; Birkhoelzer, M.; Goth, K. The Assessment of Identity Development in Adolescence (AIDA) Questionnaire: First Psychometric Evaluation in Two North American Samples of Young People. J. Personal. Assess. 2022, 105, 451–462. [Google Scholar] [CrossRef]
- Dixius, A.; Goth, K.; Möhler, E. Pilotevaluation eines neuen Programms zur Förderung von Emotionsregulation und Stressresilienz bei Kindern. START-Kids: Stress-Arousal-Regulation-Treatment for Kids. Prax. Kinderpsychol. Kinderpsychiatr. 2021, 70, 679–698. [Google Scholar]
- Herpertz, S.C.; Bertsch, K. Opportunities and Challenges of New Classification Systems for Personality Disorders: Commentary on “Clinical Utility of the AMPD: A 10th Year Anniversary Review”. Personal. Disord. Theory Res. Treat. 2022, 13, 380–382. [Google Scholar] [CrossRef]
- Chang, B.; Sharp, C.; Ha, C. The criterion validity of the Borderline Personality Features Scale for Children in an adolescent inpatient setting. J. Personal. Disord. 2011, 25, 492–503. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| School Sample | Patient Sample | Full Sample | |
|---|---|---|---|
| N | 343 | 256 | 599 |
| Gender in % m/f | 47.1/52.9 | 47.8/52.2 | 47.4/52.6 |
| Age | 6–21 (M 11.1, SD 3.6) | 6–26 (M 13.8, SD 3.0) | 6–26 (M 12.3, SD 3.6) |
| 6–11 | 62% (N = 213) | 22% (N = 57) | 45% (N = 270) |
| 12–18+ | 38% (N = 130) | 78% (N = 199) | 55% (N = 329) |
| Diagnoses/Status | CBCL T-scores > 70 Internalizing: 5.3% Externalizing: 3.0% Total: 3.0% | Diagnose groups N = 38 PD N = 70 Comorbid N = 88 Internalizing N = 38 Externalizing N = 22 Other diagnose N = 218 No PD | PD types N = 18 Antisocial N = 8 Borderline N = 3 Narcissistic N = 2 Anxious-avoidant N = 1 Histrionic N = 1 Paranoid N = 1 Schizoid N = 4 Other/not otherwise specified |
| Rated by | Parents (100%) | Parents (79%) Nurse (18%) | Parents (92%) Nurse (8%) |
| Gender in % m/f | 21.3/78.7 | 27.6/72.4 | 23.6/76.4 |
| Age | 25-68 (M 45.3, SD 6.0) | 24-73 (M 44.9, SD 9.1) | 24-73 (M 45.1, SD 7.3) |
| Scale | No Items | r-it Range | Reliability α | Reliability ωh | Correlation with Self-Report LoPF-Q 12-18 | ||||
|---|---|---|---|---|---|---|---|---|---|
| Total | ID | SD | EMP | INT | |||||
| LoPF-Q 6-18 PR: IPF total score | 36 | 0.49–0.77 | 0.96 | 0.99 | 0.47 | 0.45 | 0.42 | 0.40 | 0.45 |
| IPF1 Identity | 9 | 0.46–0.73 | 0.87 | 0.96 | 0.44 | 0.43 | 0.41 | 0.37 | 0.40 |
| 1.1 Continuity | 4 | 0.40–0.56 | 0.68 | 0.74 | 0.41 | 0.38 | 0.38 | 0.35 | 0.36 |
| 1.2 Coherence | 5 | 0.55–0.70 | 0.84 | 0.88 | 0.40 | 0.39 | 0.36 | 0.34 | 0.36 |
| IPF2 Self-direction | 9 | 0.55–0.76 | 0.90 | 0.94 | 0.50 | 0.47 | 0.47 | 0.37 | 0.47 |
| 2.1 Self-Congruence | 4 | 0.47–0.74 | 0.81 | 0.91 | 0.53 | 0.51 | 0.50 | 0.35 | 0.52 |
| 2.2 Purposefulness | 5 | 0.59–0.70 | 0.84 | 0.84 | 0.42 | 0.39 | 0.39 | 0.35 | 0.38 |
| IPF3 Empathy | 9 | 0.54–0.77 | 0.90 | 0.88 | 0.31 | 0.27 | 0.25 | 0.36 | 0.25 |
| 3.1 Perspective taking | 4 | 0.56–0.74 | 0.84 | 0.87 | 0.32 | 0.29 | 0.26 | 0.34 | 0.28 |
| 3.2 Prosociality | 5 | 0.51–0.68 | 0.80 | 0.84 | 0.27 | 0.24 | 0.21 | 0.36 | 0.19 |
| IPF4 Intimacy | 9 | 0.49–0.76 | 0.88 | 0.90 | 0.46 | 0.44 | 0.40 | 0.34 | 0.50 |
| 4.1 Close relationships | 4 | 0.55–0.70 | 0.82 | 0.84 | 0.41 | 0.40 | 0.36 | 0.29 | 0.44 |
| 4.2 Reciprocity | 5 | 0.44–0.64 | 0.77 | 0.83 | 0.45 | 0.42 | 0.39 | 0.35 | 0.49 |
| Sample | Clinical Validity | |||||
|---|---|---|---|---|---|---|
| School N = 131 | PD Patients N = 38 Age 12–18 | p | d | |||
| M | SD | M | SD | |||
| LoPF-Q 6-18 PR: IPF total score | 23.8 | 14.7 | 70.3 | 21.5 | <0.001 | 2.8 |
| IPF1 Identity | 4.2 | 3.1 | 16.2 | 6.0 | <0.001 | 3.1 |
| IPF2 Self-direction | 7.0 | 5.2 | 19.2 | 7.3 | <0.001 | 2.1 |
| IPF3 Empathy | 5.9 | 4.7 | 16.9 | 7.5 | <0.001 | 2.0 |
| IPF4 Intimacy | 6.7 | 4.9 | 18.0 | 6.4 | <0.001 | 2.1 |
| Sample | Clinical Validity | |||||
|---|---|---|---|---|---|---|
| School N = 213 | Patients N = 57 Age 6–11 | p | d | |||
| M | SD | M | SD | |||
| LoPF-Q 6-18 PR: IPF total score | 25.5 | 17.2 | 68.4 | 26.0 | <0.001 | 2.2 |
| IPF1 Identity | 4.3 | 3.8 | 13.8 | 7.2 | <0.001 | 2.0 |
| IPF2 Self-direction | 8.6 | 6.2 | 20.3 | 7.6 | <0.001 | 1.8 |
| IPF3 Empathy | 7.0 | 5.2 | 18.8 | 8.1 | <0.001 | 2.0 |
| IPF4 Intimacy | 5.6 | 4.9 | 15.5 | 6.6 | <0.001 | 1.9 |
| Scale | LoPF-Q 6-18 PR | ||||
|---|---|---|---|---|---|
| IPF Total Score | IPF1 Identity | IPF2 Self-direction | IPF3 Empathy | IPF4 Intimacy | |
| STiP-5.1 | |||||
| Total score | 0.34 * | 0.32 * | 0.44 *** | 0.09 | 0.26 |
| Identity | 0.47 *** | 0.43 ** | 0.50 *** | 0.24 | 0.41 |
| Self-direction | 0.22 | 0.27 * | 0.35 ** | −0.02 | 0.14 |
| Empathy | 0.02 | 0.04 | 0.09 | −0.05 | 0.00 |
| Intimacy | 0.30 * | 0.23 | 0.41 ** | 0.12 | 0.24 |
| OPD-CA2-SQ PR | |||||
| Total score | 0.96 *** | 0.88 *** | 0.90 *** | 0.87 *** | 0.84 *** |
| IPS2 Identity | 0.94 *** | 0.86 *** | 0.94 *** | 0.80 *** | 0.82 *** |
| IPS1 Control | 0.83 *** | 0.79 *** | 0.75 *** | 0.84 *** | 0.66 *** |
| IPS3 Interpersonality | 0.90 *** | 0.81 *** | 0.82 *** | 0.81 *** | 0.85 *** |
| IPS4 Attachment | 0.86 *** | 0.80 *** | 0.78 *** | 0.76 *** | 0.78 *** |
| PID5BF+ M CA IRF | |||||
| Negative Affectivity | 0.62 *** | 0.56 *** | 0.66 *** | 0.54 *** | 0.50 *** |
| Detachment | 0.78 *** | 0.70 *** | 0.71 *** | 0.64 *** | 0.81 *** |
| Antagonism | 0.65 *** | 0.64 *** | 0.50 *** | 0.74 *** | 0.50 *** |
| Disinhibition | 0.66 *** | 0.62 *** | 0.64 *** | 0.69 *** | 0.47 *** |
| Anankastia | 0.25 *** | 0.23 *** | 0.20 *** | 0.19 *** | 0.28 *** |
| Psychoticism | 0.69 *** | 0.66 *** | 0.60 *** | 0.67 *** | 0.58 *** |
| CBCL 4-18 | |||||
| Total score | 0.78 *** | 0.72 *** | 0.72 *** | 0.73 *** | 0.60 *** |
| Internalizing | 0.70 *** | 0.62 *** | 0.65 *** | 0.55 *** | 0.66 *** |
| Externalizing | 0.68 *** | 0.63 *** | 0.58 *** | 0.74 *** | 0.44 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazreku, G.; Birkhölzer, M.; Cosgun, S.; Kerber, A.; Schmeck, K.; Goth, K. Impaired Personality Functioning in Children and Adolescents Assessed with the LoPF-Q 6-18 PR in Parent-Report and Convergence with Maladaptive Personality Traits and Personality Structure in School and Clinic Samples. Children 2023, 10, 1186. https://doi.org/10.3390/children10071186
Mazreku G, Birkhölzer M, Cosgun S, Kerber A, Schmeck K, Goth K. Impaired Personality Functioning in Children and Adolescents Assessed with the LoPF-Q 6-18 PR in Parent-Report and Convergence with Maladaptive Personality Traits and Personality Structure in School and Clinic Samples. Children. 2023; 10(7):1186. https://doi.org/10.3390/children10071186
Chicago/Turabian StyleMazreku, Gresa, Marc Birkhölzer, Sefa Cosgun, André Kerber, Klaus Schmeck, and Kirstin Goth. 2023. "Impaired Personality Functioning in Children and Adolescents Assessed with the LoPF-Q 6-18 PR in Parent-Report and Convergence with Maladaptive Personality Traits and Personality Structure in School and Clinic Samples" Children 10, no. 7: 1186. https://doi.org/10.3390/children10071186