
Responses to Sensory Events in Daily Life in Children with Cerebral Palsy from a Parent Reported Perspective and in a Swedish Context

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
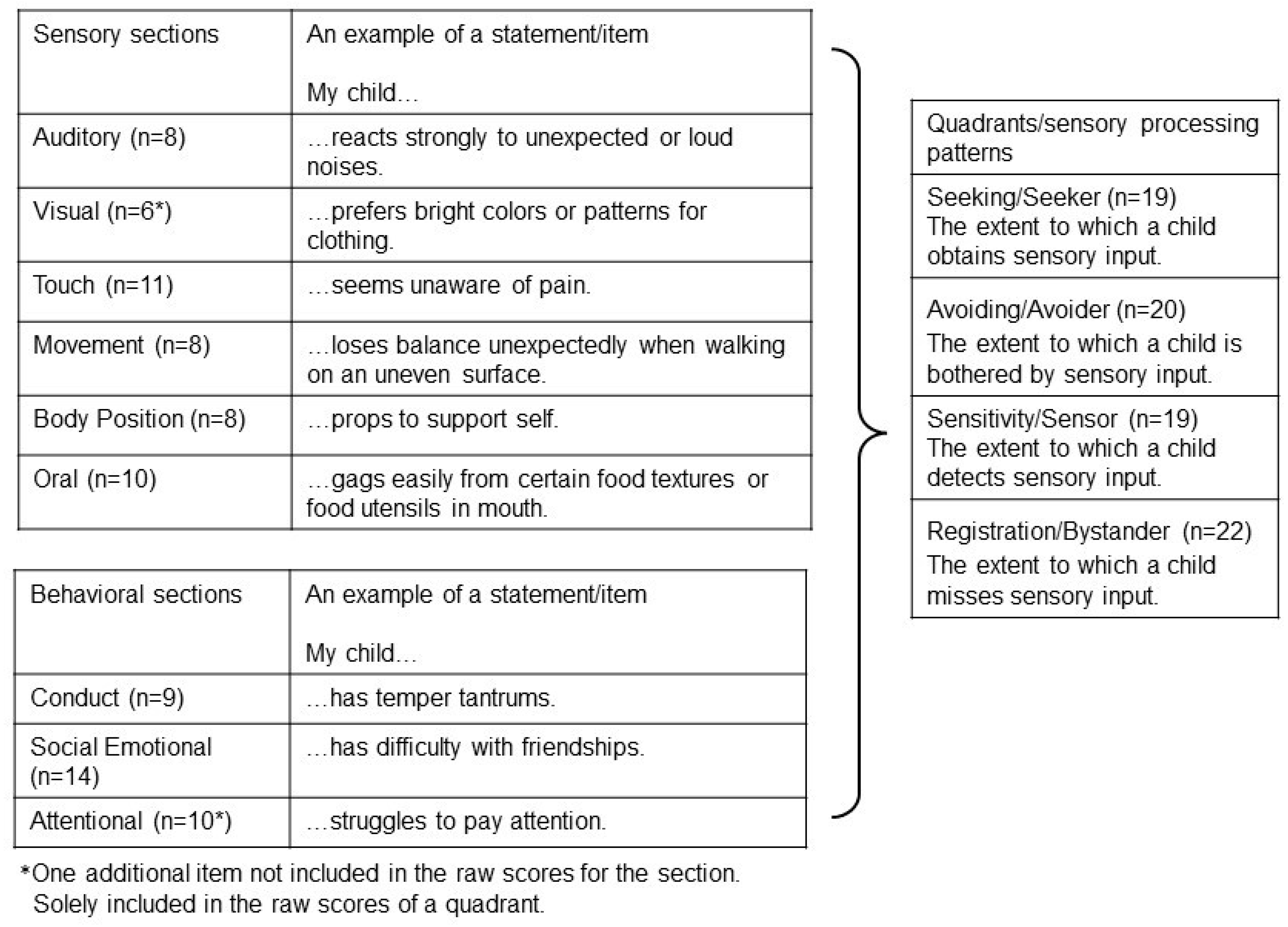
2.2. The Child Sensory Profile-2© (CSP-2©)
2.3. Questions Regarding Maintaining Body Posture and Sound Sensitivity
2.4. Procedures
2.5. Data and Statistical Analysis
3. Results
3.1. Participants
3.2. Child Sensory Profile-2©
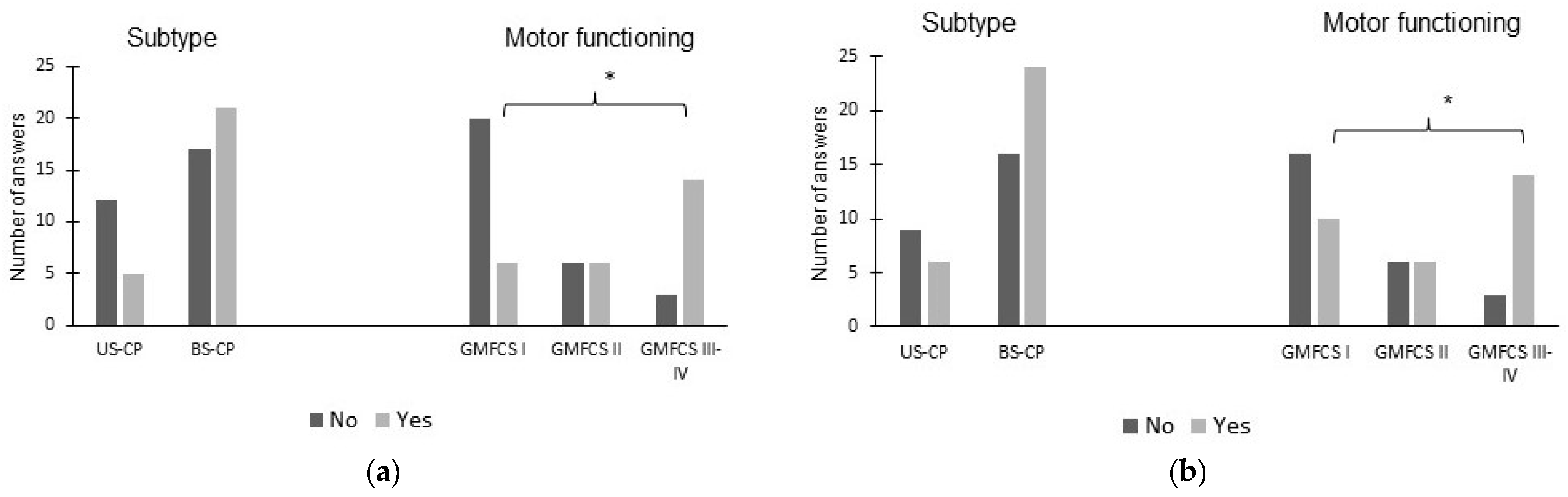
3.3. Maintaining Body Posture and Sound Sensitivity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADHD | Attention-Deficit/Hyperactivity Disorder |
| BS-CP | Bilateral Spastic Cerebral Palsy |
| CP | Cerebral Palsy |
| CSP-2 | Child Sensory Profile-2 |
| GMFCS | Gross Motor Function Classification System |
| US-CP | Unilateral Spastic Cerebral Palsy |
References
- Ayres, J. What is sensory integration? In Sensory Integration and the Child; Western Psychological Services: Los Angeles, CA, USA, 1979; pp. 3–11. [Google Scholar]
- Shumway-Cook, A.W.M. Development of postural control. In Motor Control: Translating Research into Clinical Practice, 5th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2016; pp. 183–205. [Google Scholar]
- Dunn, W.; Little, L.; Dean, E.; Robertson, S.; Evans, B. The State of the Science on Sensory Factors and Their Impact on Daily Life for Children: A Scoping Review. OTJR 2016, 36, 3S–26S. [Google Scholar] [CrossRef]
- WHO. International Classification of Functioning Disabilty and Health, Version for Children and Youth, ICF-CY; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Shumway-Cook, A.W.M. Motor Control: Issues and Theories. In Motor Control: Translating Research into Clinical Practice, 5th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2016; pp. 3–20. [Google Scholar]
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Damiano, D.; Dan, B.; Jacobsson, B. A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child Neurol. Suppl. 2007, 109, 8–14. [Google Scholar]
- Påhlman, M.; Gillberg, C.; Himmelmann, K. One-third of school-aged children with cerebral palsy have neuropsychiatric impairments in a population-based study. Acta Paediatr. 2019, 108, 2048–2055. [Google Scholar] [CrossRef] [PubMed]
- Påhlman, M.; Gillberg, C.; Wentz, E.; Himmelmann, K. Autism spectrum disorder and attention-deficit/hyperactivity disorder in children with cerebral palsy: Results from screening in a population-based group. Eur. Child Adolesc. Psychiatry 2020, 29, 1569–1579. [Google Scholar] [CrossRef] [PubMed]
- Association, A.P. Diagnostic and statistical manual of mental disorders: DSM-5. In DSM 5, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013; pp. 50–59. [Google Scholar]
- Palisano, R.J.; Rosenbaum, P.; Bartlett, D.; Livingston, M.H. Content validity of the expanded and revised Gross Motor Function Classification System. Dev. Med. Child Neurol. 2008, 50, 744–750. [Google Scholar] [CrossRef] [PubMed]
- SCPE. Surveillance of cerebral palsy in Europe: A collaboration of cerebral palsy surveys and registers. Dev. Med. Child Neurol. 2000, 42, 816–824. [Google Scholar] [CrossRef] [PubMed]
- Carnahan, K.D.; Arner, M.; Hägglund, G. Association between gross motor function (GMFCS) and manual ability (MACS) in children with cerebral palsy. A population-based study of 359 children. BMC Musculoskelet. Disord. 2007, 8, 50. [Google Scholar] [CrossRef]
- Dobson, F.; Morris, M.E.; Baker, R.; Graham, H.K. Unilateral cerebral palsy: A population-based study of gait and motor function: Unilateral CP Cohort Study. Dev. Med. Child Neurol. 2011, 53, 429–435. [Google Scholar] [CrossRef]
- Himmelmann, K.; Beckung, E.; Hagberg, G.; Uvebrant, P. Gross and fine motor function and accompanying impairments in cerebral palsy. Dev. Med. Child Neurol. 2006, 48, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Himmelmann, K.; Horber, V.; Sellier, E.; De la Cruz, J.; Papavasiliou, A.; Kraegeloh-Mann, I. Neuroimaging Patterns and Function in Cerebral Palsy-Application of an MRI Classification. Front. Neurol. 2021, 11, 617740. [Google Scholar] [CrossRef]
- Wingert, J.R.; Burton, H.; Sinclair, R.J.; Brunstrom, J.E.; Damiano, D.L. Tactile sensory abilities in cerebral palsy: Deficits in roughness and object discrimination. Dev. Med. Child Neurol. 2008, 50, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Damiano, D.L.; Wingert, J.R.; Stanley, C.J.; Curatalo, L. Contribution of hip joint proprioception to static and dynamic balance in cerebral palsy: A case control study. J. Neuroeng. Rehabil. 2013, 10, 57. [Google Scholar] [CrossRef] [PubMed]
- Ego, A.; Lidzba, K.; Brovedani, P.; Belmonti, V.; Gonzalez-Monge, S.; Boudia, B.; Ritz, A.; Cans, C. Visual–perceptual impairment in children with cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2015, 57, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Fazzi, E.; Bova, S.M.; Uggetti, C.; Signorini, S.G.; Bianchi, P.E.; Maraucci, I.; Zoppello, M.; Lanzi, G. Visual–perceptual impairment in children with periventricular leukomalacia. Brain Dev. 2004, 26, 506–512. [Google Scholar] [CrossRef]
- Lidbeck, C.; Bartonek, A.; Yadav, P.; Tedroff, K.; Astrand, P.; Hellgren, K.; Gutierrez-Farewik, E.M. The role of visual stimuli on standing posture in children with bilateral cerebral palsy. BMC Neurol. 2016, 16, 151. [Google Scholar] [CrossRef]
- Lidbeck, C.; Tedroff, K.; Bartonek, Å. Muscle strength does not explain standing ability in children with bilateral spastic cerebral palsy: A cross sectional descriptive study. BMC Neurol. 2015, 15, 188. [Google Scholar] [CrossRef]
- Nashner, L.M.; Shumway-Cook, A.; Marin, O. Stance posture control in select groups of children with cerebral palsy: Deficits in sensory organization and muscular coordination. Exp. Brain Res. 1983, 49, 393–409. [Google Scholar] [CrossRef]
- Saavedra, S.; Woollacott, M.; van Donkelaar, P. Head stability during quiet sitting in children with cerebral palsy: Effect of vision and trunk support. Exp. Brain Res. 2009, 201, 13–23. [Google Scholar] [CrossRef]
- Lidbeck, C.M.; Gutierrez-Farewik, E.M.; Brostrom, E.; Bartonek, A. Postural orientation during standing in children with bilateral cerebral palsy. Pediatr. Phys. Ther. 2014, 26, 223–229. [Google Scholar] [CrossRef]
- Bartonek, A.; Lidbeck, C.; Hellgren, K.; Gutierrez-Farewik, E. Head and Trunk Movements During Turning Gait in Children with Cerebral Palsy. J. Mot. Behav. 2019, 51, 362–370. [Google Scholar] [CrossRef]
- Ferrari, A.; Sghedoni, A.; Alboresi, S.; Pedroni, E.; Lombardi, F. New definitions of 6 clinical signs of perceptual disorder in children with cerebral palsy: An observational study through reliability measures. Eur. J. Phys. Rehabil. Med. 2014, 50, 709–716. [Google Scholar]
- Ferrari, A.; Tersi, L.; Ferrari, A.; Sghedoni, A.; Chiari, L. Functional reaching discloses perceptive impairment in diplegic children with cerebral palsy. Gait Posture 2010, 32, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A. Perceptive Defects. In The Spastic Forms of Cerebral Palsy; Ferrari, A., Cioni, G., Eds.; Springer: Milan, Italy, 2010; pp. 73–98. [Google Scholar]
- Dan, B. Cerebral palsy is a sensorimotor disorder. Dev. Med. Child Neurol. 2020, 62, 768. [Google Scholar] [CrossRef] [PubMed]
- Pavão, S.L.; dos Santos, A.N.; Woollacott, M.H.; Rocha, N.A.C.F. Assessment of postural control in children with cerebral palsy: A review. Res. Dev. Disabil. 2013, 34, 1367–1375. [Google Scholar] [CrossRef]
- Holmström, L.; Lennartsson, F.; Eliasson, A.C.; Flodmark, O.; Clark, C.; Tedroff, K.; Forssberg, H.; Vollmer, B. Diffusion MRI in corticofugal fibers correlates with hand function in unilateral cerebral palsy. Neurology 2011, 77, 775–783. [Google Scholar] [CrossRef]
- Staudt, M.; Grodd, W.; Gerloff, C.; Erb, M.; Stitz, J.; KrÄGeloh-Mann, I. Two types of ipsilateral reorganization in congenital hemiparesis: A TMS and fMRI study. Brain 2002, 125, 2222–2237. [Google Scholar] [CrossRef]
- Van de Winckel, A.; Verheyden, G.; Wenderoth, N.; Peeters, R.; Sunaert, S.; Van Hecke, W.; De Cock, P.; Desloovere, K.; Eyssen, M.; Feys, H. Does somatosensory discrimination activate different brain areas in children with unilateral cerebral palsy compared to typically developing children? An fMRI study. Res. Dev. Disabil. 2013, 34, 1710–1720. [Google Scholar] [CrossRef]
- Jovellar-Isiegas, P.; Resa Collados, I.; Jaén-Carrillo, D.; Roche-Seruendo, L.E.; Cuesta García, C. Sensory Processing, Functional Performance and Quality of Life in Unilateral Cerebral Palsy Children: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 7116. [Google Scholar] [CrossRef]
- Pavao, S.L.; Lima, C.R.G.; Rocha, N. Association between sensory processing and activity performance in children with cerebral palsy levels I-II on the gross motor function classification system. Braz. J. Phys. Ther. 2021, 25, 194–202. [Google Scholar] [CrossRef]
- Pavão, S.L.; Rocha, N. Sensory processing disorders in children with cerebral palsy. Infant Behav. Dev. 2017, 46, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Dunn, W. The Sensory Profile: Examiner’s Manual; Psycological Corporation: San Antonia, TX, USA, 1999. [Google Scholar]
- Dunn, W. Sensory Profile 2, User’s Manual; Psychological Corporation: San Antonia, TX, USA, 2014. [Google Scholar]
- Bäcklund, L.; Olsson, A.-K. Sensory Profile 2, Manual—Supplement, Svensk Verison; Pearson: Bromma, Sweden, 2016. [Google Scholar]
- Licciardi, L.; Brown, T. An overview & critical review of the Sensory Profile—Second edition. Scand. J. Occup. Ther. 2021, 1–13. [Google Scholar] [CrossRef]
- Tomchek, S.D.; Dunn, W. Sensory processing in children with and without autism: A comparative study using the short sensory profile. Am. J. Occup. Ther. 2007, 61, 190–200. [Google Scholar] [CrossRef]
- Hinkle, D.E.; Wiersma, W.; Jurs, S.G. Rule of thumb for interpreting the size of a correlation coefficient matrix showing correlation coefficients appropriate scales of measurements for varaiable x and variable y. In Applied Statistics for Behavioural Science, 5th ed.; Houghton Mifflin: Boston, MA, USA, 2003; pp. 95–120. [Google Scholar]
- Bottcher, L.; Flachs, E.M.; Uldall, P. Attentional and executive impairments in children with spastic cerebral palsy. Dev. Med. Child Neurol. 2010, 52, e42–e47. [Google Scholar] [CrossRef]
- Lidbeck, C.; Bartonek, A. Motor function at increasing postural demands in children with bilateral cerebral palsy. Eur. J. Phys. Rehabil. Med. 2021, 57, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Shumway-Cook, A.W.M. Physiological basis of motor learning and recovery of function. In Motor Control: Translating Research into Clinical Practice, 5th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2016; pp. 80–105. [Google Scholar]
- Steele, K.M.; Damiano, D.L.; Eek, M.N.; Unger, M.; Delp, S.L. Characteristics associated with improved knee extension after strength training for individuals with cerebral palsy and crouch gait. J. Pediatr. Rehabil. Med. 2012, 5, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Eek, M.N.; Beckung, E. Walking ability is related to muscle strength in children with cerebral palsy. Gait Posture 2008, 28, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A. From movement to action: A new framework for cerebral palsy. Eur. J. Phys. Rehabil. Med. 2019, 55, 852–861. [Google Scholar] [CrossRef] [PubMed]
- Alboresi, S.; Sghedoni, A.; Borelli, G.; Costi, S.; Beccani, L.; Neviani, R.; Ferrari, A. Are perceptual disorder signs in diplegic cerebral palsied children stable over time? A retrospective cohort analysis. Minerva Pediatr. 2020, 72, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Østensjø, S.; Brogren Carlberg, E.; Vøllestad, N.K. Everyday functioning in young children with cerebral palsy: Functional skills, caregiver assistance, and modifications of the environment. Dev. Med. Child Neurol. 2003, 45, 603–612. [Google Scholar] [CrossRef]
- Lauruschkus, K.; Nordmark, E.; Hallström, I. Parents’ experiences of participation in physical activities for children with cerebral palsy—Protecting and pushing towards independence. Disabil. Rehabil. 2017, 39, 771–778. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| CSP-2 (n = 55) | Question (a) (n = 55) | Question (b) (n = 55) | |
|---|---|---|---|
| US-CP/BS-CP (n) | 18/37 | 17/38 | 15/40 |
| GMFCS levels (n) | |||
| I | 28 | 26 | 26 |
| II | 12 | 12 | 12 |
| III | 13 | 14 | 14 |
| IV | 2 | 3 | 3 |
| Age, median [min, max] years for: | |||
| Spastic CP | 12.3 [6.3, 18.0] | 12.7 [6.3, 18.0] | 12.4 [6.3, 18.0] |
| US-CP | 9.7 [6.3, 17.7] | 9.6 [6.3, 17.7] | 9.6 [6.3, 17.7] |
| BS-CP | 14.0 [6.4, 18.0] | 14.2 [6.4, 18.0] | 13.9 [6.4, 18.0] |
| GMFCS levels: | |||
| I | 10.1 [6.3, 18.0] | 10.2 [6.3, 18.0] | 10.2 [6.3, 18.0] |
| II | 12.1 [6.4, 17.8] | 12.1 [6.4, 17.8] | 11.0 [6.4, 17.8] |
| III–IV | 15.6 [9.6, 17.7] | 15.0 [9.6, 17.7] | 15.0 [9.6, 17.7] |
| CSP-2© | Norm Group Mean (SD) | CP n = 55 Mean (SD) | z-Value | p-Value | US-CP n = 18 Mean (SD) | z-Value | p-Value | BS-CP n = 37 Mean (SD) | z-Value | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|
| Quadrants/sensory processing patterns: | ||||||||||
| Seeking | 22.4 (16.7) | 29.0 (15.1) | 2.9 | 0.003 * | 34.4 (13.1) | 3.1 | 0.002 * | 26.4 (15.5) | 1.5 | 0.144 |
| Avoiding | 26.3 (17.7) | 42.9 (18.0) | 7.0 | <0.001 * | 42.7 (17.7) | 3.9 | <0.001 * | 43.0 (18.3) | 5.7 | <0.001 * |
| Sensitivity | 21.6 (15.0) | 32.3 (13.8) | 5.3 | <0.001 * | 34.8 (10.5) | 3.7 | <0.001 * | 31.1 (15.1) | 3.9 | <0.001 * |
| Registration | 22.4 (17.3) | 46.3 (16.3) | 10.2 | <0.001 * | 47.0 (14.6) | 6.0 | <0.001 * | 46.0 (17.2) | 8.3 | <0.001 * |
| Sensory sections: | ||||||||||
| Auditory | 14.3 (7.5) | 18.8 (8.8) | 4.4 | <0.001 * | 20.5 (8.4) | 3.5 | <0.001 * | 17.9 (9.0) | 2.9 | 0.003 * |
| Visual | 9.2 (5.2) | 11.5 (6.0) | 3.3 | <0.001 * | 12.7 (4.2) | 2.9 | 0.004 * | 10.9 (6.6) | 1.9 | 0.052 |
| Touch | 10.8 (8.7) | 14.3 (8.2) | 3.0 | 0.003 * | 16.6 (6.9) | 2.8 | 0.005 * | 13.2 (8.6) | 1.7 | 0.091 |
| Movement | 7.9 (6.8) | 13.1 (6.4) | 5.7 | <0.001 * | 14.9 (6.4) | 4.4 | <0.001 * | 12.2 (6.3) | 3.9 | <0.001 * |
| Body position | 6.5 (6.6) | 18.4 (7.6) | 13.4 | <0.001 * | 16.9 (6.0) | 6.7 | <0.001 * | 19.1 (8.3) | 11.6 | <0.001 * |
| Oral | 9.8 (9.3) | 14.1 (9.2) | 3.4 | <0.001 * | 15.1 (7.0) | 2.4 | 0.016 * | 13.7 (10.1) | 2.5 | 0.012 * |
| Behavioural sections: | ||||||||||
| Conduct | 10.9 (8.4) | 15.2 (5.9) | 3.8 | <0.001 * | 16.2 (5.0) | 2.7 | 0.008 * | 14.8 (6.3) | 2.8 | 0.005 * |
| Social emotional | 16.9 (13.9) | 31.7 (13.0) | 7.9 | <0.001 * | 30.0 (13.0) | 4.0 | <0.001 * | 32.6 (13.1) | 6.9 | <0.001 * |
| Attentional | 10.9 (8.9) | 19.5 (9.8) | 7.2 | <0.001 * | 22.0 (8.8) | 5.3 | <0.001 * | 18.2 (10.1) | 5.0 | <0.001 * |
| Child Sensory Profile-2© | CP n = 55 | US-CP n = 18 | BS-CP n = 37 | Differences between US-CP/BS-CP | GMFCS I n = 28 | GMFCS II n = 12 | GMFCS III–IV n = 15 | Differences between GMFCS |
|---|---|---|---|---|---|---|---|---|
| Quadrants: | n (%) Score >2 SD | n (%) Score >2 SD | n (%) Score >2 SD | p-Value | n (%) Score >2 SD | n (%) Score >2 SD | n (%) Score >2 SD | p-Value |
| Seeking | 1 (2) | 1 (6) | 0 (0) | 0.148 | 1 (4) | 0 (0) | 0 (0) | 0.612 |
| Avoiding | 8 (15) | 4 (22) | 4 (11) | 0.260 | 4 (14) | 1 (8) | 3 (20) | 0.693 |
| Sensitivity | 5 (9) | 1 (6) | 4 (11) | 0.525 | 2 (7) | 1 (8) | 2 (13) | 0.793 |
| Registration | 14 (26) | 4 (22) | 10 (27) | 0.701 | 5 (18) | 3 (25) | 6 (40) | 0.283 |
| Sensory sections: | ||||||||
| Auditory | 7 (13) | 4 (22) | 3 (8) | 0.141 | 5 (18) | 2 (17) | 0 (0) | 0.221 |
| Visual | 3 (6) | 0 (0) | 3 (8) | 0.214 | 1 (4) | 0 (0) | 2 (13) | 0.260 |
| Touch | 3 (6) | 2 (11) | 1 (3) | 0.198 | 2 (7) | 0 (0) | 1 (7) | 0.641 |
| Movement | 5 (9) | 3 (17) | 2 (5) | 0.173 | 2 (7) | 1 (8) | 2 (13) | 0.793 |
| Body position | 22 (40) | 4 (22) | 18 (49) | 0.061 | 8 (29) | 5 (42) | 9 (60) | 0.133 |
| Oral | 5 (9) | 1 (6) | 4 (11) | 0.525 | 2 (7) | 1 (8) | 2 (13) | 0.793 |
| Behavioural sections: | ||||||||
| Conduct | 0 (0) | 0 (0) | 0 (0) | ns | 0 (0) | 0 (0) | 0 (0) | ns |
| Social emotional | 10 (18) | 4 (22) | 6 (16) | 0.588 | 5 (18) | 1 (8) | 4 (27) | 0.470 |
| Attentional | 8 (15) | 3 (17) | 5 (14) | 0.756 | 4 (14) | 3 (25) | 1 (7) | 0.405 |
| Children with a score > 2 SD in one or more sections and/or quadrants | 30 (55) | 7 (39) | 23 (62) | 0.104 | 13 (46) | 6 (50) | 11 (73) | 0.225 |
| Correlation Coefficient (rs) | p-Value | |
|---|---|---|
| Child Sensory Profile-2© | Age | |
| Quadrants: | ||
| Seeking | −0.305 * | 0.024 * |
| Avoiding | -0.006 | 0.968 |
| Sensitivity | -0.109 | 0.429 |
| Registration | 0.041 | 0.765 |
| Sensory sections: | ||
| Auditory | −0.306 * | 0.023 * |
| Visual | −0.014 | 0.918 |
| Touch | −0.079 | 0.569 |
| Movement | −0.133 | 0.333 |
| Body Position | 0.076 | 0.579 |
| Oral | −0.235 | 0.085 |
| Behavioural sections: | ||
| Conduct | −0.223 | 0.101 |
| Social Emotional | 0.106 | 0.442 |
| Attentional | −0.077 | 0.577 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ericson, A.; Bartonek, Å.; Tedroff, K.; Lidbeck, C. Responses to Sensory Events in Daily Life in Children with Cerebral Palsy from a Parent Reported Perspective and in a Swedish Context. Children 2023, 10, 1139. https://doi.org/10.3390/children10071139
Ericson A, Bartonek Å, Tedroff K, Lidbeck C. Responses to Sensory Events in Daily Life in Children with Cerebral Palsy from a Parent Reported Perspective and in a Swedish Context. Children. 2023; 10(7):1139. https://doi.org/10.3390/children10071139
Chicago/Turabian StyleEricson, Annika, Åsa Bartonek, Kristina Tedroff, and Cecilia Lidbeck. 2023. "Responses to Sensory Events in Daily Life in Children with Cerebral Palsy from a Parent Reported Perspective and in a Swedish Context" Children 10, no. 7: 1139. https://doi.org/10.3390/children10071139