
Investigation of the Seasonal Variation in Fat Patterning of Ellisras Rural Children and Adolescents, in the Limpopo Province, South Africa
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Sampling Procedure
2.2. Data Collection
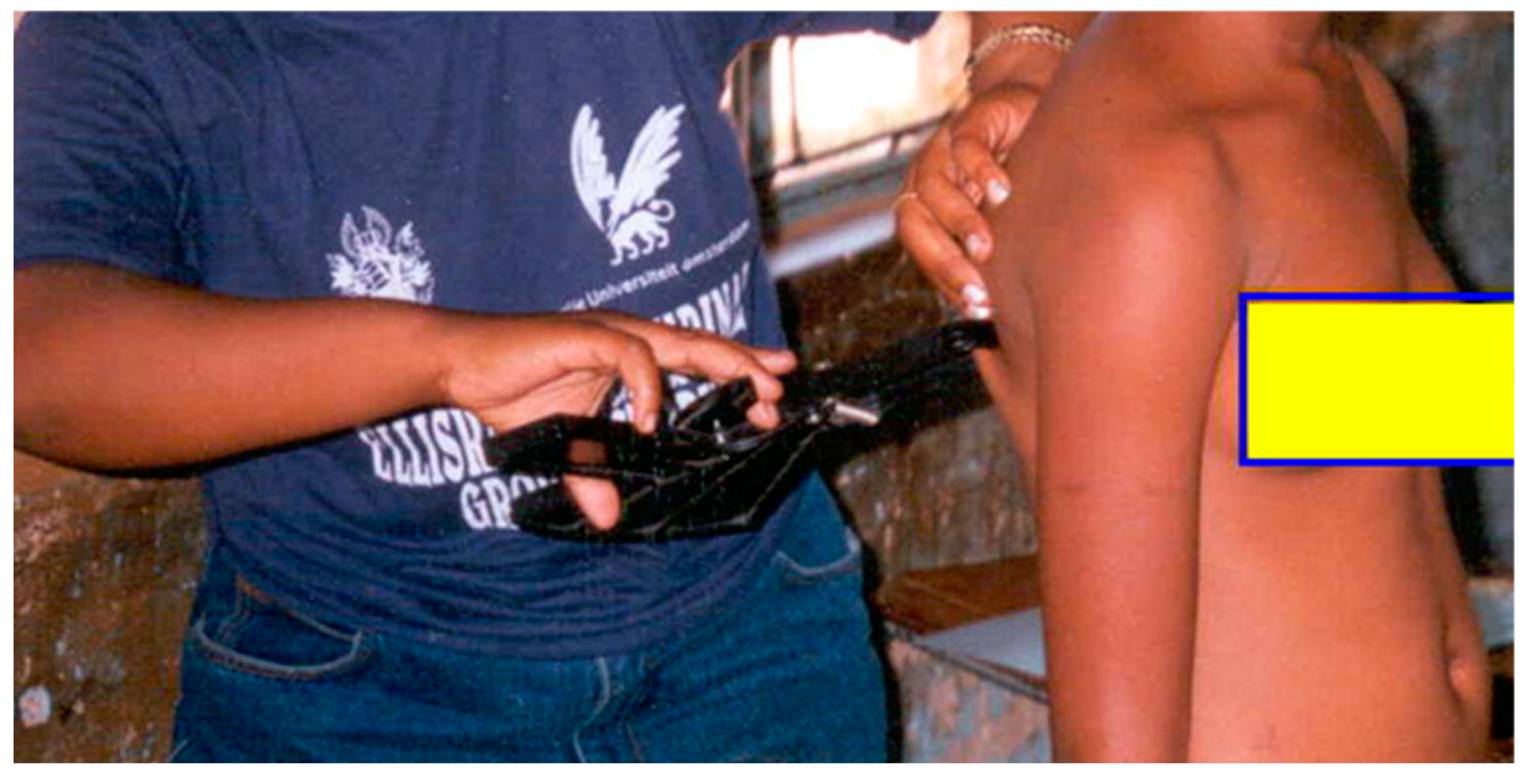
2.2.1. Anthropometry
Triceps
Biceps
Subscapular
Suprailiac
2.3. Data Analysis
2.4. Ethical Clearance
3. Results
3.1. Characteristics of the Population
3.2. The Prevalence of Obesity Based on ST, SST, and SSTB Ratio
3.3. The Correlation of ST, SST, and SSTB Ratio with Season
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gupta, N.; Goel, K.; Shah, P.; Misra, A. Childhood obesity in Developing Countries: Epidemiology, Determinants, and Prevention. Endocr. Rev. 2012, 33, 48–70. [Google Scholar] [CrossRef]
- Toriola, A.L.; Moselakgomo, V.K.; Shaw, B.S. Overweight, obesity and underweight in rural black South African children. S. Afr. J. Clin. Nutr. 2012, 25, 57–61. [Google Scholar] [CrossRef]
- Sedibe, M.H.; Pisa, P.T.; Feeley, A.B.; Pedro, T.M.; Kahn, K.; Norris, S.A. Dietary habits and eating practices and their association with overweight and obesity in rural and urban black South African adolescents. Nutrients 2018, 10, 145. [Google Scholar] [CrossRef]
- Onis, M.; Blossner, M.; Borghi, E. Global prevalence and trends of overweight and obesity among preschool children. Am. J. Clin. Nutr. 2010, 92, 1257–1264. [Google Scholar] [CrossRef]
- Lee, E.Y.; Yoon, K.H. Epidemic obesity in children and adolescents: Risk factors and prevention. Front. Med. 2018, 12, 658–666. [Google Scholar] [CrossRef]
- Li, P.; Yang, F.; Xiong, F.; Huo, T.; Tong, Y.; Yang, S.; Mao, M. Nutritional status and risk factors of overweight and obesity for children aged 9–15 years in Chengdu, Southwest China. Biomed. Cent. Public Health 2012, 12, 636. [Google Scholar] [CrossRef] [PubMed]
- Monyeki, K.D.; Kemper, H.C.G.; Makgae, P.J. Relationship between fat patterns, physical fitness and blood pressure of rural South African children: Ellisras Longitudinal Growth and Health Study. J. Hum. Hypertens. 2008, 22, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Silva, K.S.; Silva, R.C.; Duarte, M.F. Undernutrition and obesity associated with high blood. Paediatr. Cardiol. 2009, 30, 248–255. [Google Scholar] [CrossRef]
- Kemper, H.C.; Post, G.B.; Twisk, J.W.; Mechelen, V. Lifestyle and obesity in adolescence and young adulthood: Results from the Amsterdam Growth and Health Longitudinal Study (AGAHLS). Int. J. Obes. 1999, 23, S34–S40. [Google Scholar] [CrossRef]
- Mitchikpe CE, S.; Dossa RA, M.; Ategbo EA, D.; Raaij JM, A.; Kok, F.J. Seasonal variation in food pattern but not in energy and nutrient intakes of rural Beninese school-aged children. Public Health Nutr. 2008, 12, 414–422. [Google Scholar] [CrossRef]
- Zhu, Z.; Wu, C.; Lou, B.; Zang, J.; Wang, Z.; Guo, C.; Jia, X.; Wang, W.; Shen, X.; Lu, Y.; et al. The dietary intake and its features across four seasons in the Metropolis of China. J. Nutr. Sci. Vitaminol. 2019, 65, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Park, K.S.; Lee, M.G. Effects of summer school participation and psychosocial outcomes on changes in body composition and physical fitness during summer break. J. Exerc. Nutr. Biochem. 2015, 19, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Monyeki, K.D.; Siweya, H.J.; Kemper, H.C.G.; Ramoshaba, N.E. Health Status and Permanent Loss to Follow Up of Ellisras Longitudinal Study Subjects: Rural South African Context. In Nutrition in Health and Disease—Our Challenges Now and Forthcoming Time; IntechOpen: London, UK, 2019. [Google Scholar] [CrossRef]
- Weather to Visit. What’s the Weather Like in Lephalale (Limpopo) in May 2023? 2023. Available online: www.weather2visit.com (accessed on 12 June 2023).
- Monyeki, K.D.; Cameron, N.; Getz, B. Growth and nutritional status of rural South African children 3–10 years old: The Ellisras growth study. Am. J. Hum. Biol. 2000, 12, 42–49. [Google Scholar] [CrossRef]
- Monyeki, K.D.; Kemper, H.C.G.; Makgae, P.J. The association of fat patterning with blood pressure in rural South African children: The Ellisras Longitudinal Growth and Health Study. Int. J. Epidemiol. 2006, 35, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Norton, K.; Olds, T. Anthropometrica; University of New South Wales Press: Sydney, Australia, 1996; pp. 120–267. [Google Scholar]
- Dietz, W.H. Critical periods in childhood for the development of obesity. Am. J. Clin. Nutr. 1994, 59, 955–959. [Google Scholar] [CrossRef]
- Pinyerd, B.; Zipf, W.B. Puberty—Timing is everything! J. Pediatr. Nurs. 2005, 20, 75–82. [Google Scholar] [CrossRef]
- Loomba-Albrecht, L.A.; Styne, D.M. Effect of puberty on body composition. Curr. Opin. Endocrinol. Diabetes Obes. 2009, 16, 10–15. [Google Scholar] [CrossRef]
- Thakur, R.; Gautam, R.K. Pre- and post-pubertal growth difference among boys and girls of 5–18 years of age: A cross-sectional study among central Indian Population. Hum. Biol. Rev. 2017, 6, 164–187. [Google Scholar]
- Leal, D.B.; de Assis, M.A.A.; González-Chica, D.A.; da Costa, F.F.; de Andrade, D.F.; Lobo, A.S. Changes in total and central adiposity and body fat distribution among 7–10-year-old schoolchildren in Brazil. Public Health Nutr. 2015, 18, 2105–2114. [Google Scholar] [CrossRef]
- Stacey, N.; van Walbeek, C.; Maboshe, M. Energy drink consumption and marketing in South Africa. Prev. Med. 2017, 105, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Sardinha, L.B.; Going, S.B.; Teixeira, P.J.; Lohman, T.G. Receiver operating characteristic analysis of body mass index, triceps skinfold thickness, and arm girth for obesity screening in children and adolescents. Am. J. Clin. Nutr. 1999, 70, 1090–1095. [Google Scholar] [CrossRef]
- Ulijaszek, S.J.; Kerr, D.A. Anthropometric measurement error and the assessment of nutritional status. Br. J. Nutr. 1999, 82, 165–177. [Google Scholar] [CrossRef]
- Kuhle, S.; Ashley-Martin, J.; Maguire, B.; Hamilton, D.C. Percentile curves for skinfold thickness for Canadian children and youth. Peer J. 2016, 4, e2247. [Google Scholar] [CrossRef]
- Monyeki, K.D.; Kemper, H.C.; Makgae, P.J. Development and tracking of central patterns of subcutaneous fat of rural South African youth: Ellisras longitudinal study. Biomed. Cent. Pediatr. 2009, 9, 74. [Google Scholar] [CrossRef]
- Kanikowska, D.; Sato, M.; Witowski, J. Contribution of daily and seasonal biorhythms to obesity in humans. Int. J. Biometeorol. 2015, 59, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Von Hippel, P.; Benson, R. Obesity and the natural environment across US counties. Am. J. Public Health 2014, 104, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar] [CrossRef]
- Silva, H.P.; Veiga, G.V.; Kac, G.; Pereira, R.A. Anthropometric measurements of adolescents from two Amazonian ecosystems: Variations according to seasonality. J. Biosoc. Sci. 2010, 42, 145–160. [Google Scholar] [CrossRef]
- Kumar, S.; Mahabalaraju, D.K.; Anuroopa, M.S. Prevalence of Obesity and Its Influencing Factor among Affluent School Children of Davangere City. Indian J. Community Med. 2007, 32, 15–17. [Google Scholar] [CrossRef]
- Lafta, R.K.; Kadhim, M.J. Childhood obesity in Iraq: Prevalence and possible risk factors. Ann. Saudi Med. 2005, 25, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Perichart-Perera, O.; Balas-Nakash, M.; Schiffman-Selechnik, E.; Barbato-Dosal, A.; Vadillo-Ortega, F. Obesity increases metabolic syndrome risk factors in school-aged children from an urban school in Mexico City. J. Am. Diet. Assoc. 2007, 107, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Skinner, A.C.; Ravanbakht, S.N.; Skelton, J.A.; Perrin, E.M.; Armstrong, S.C. Prevalence of obesity and severe obesity in US children, 1999–2016. Pediatrics 2018, 141, e20173459. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.J.J.A.; Sark, I.N.; Sallis, J.F. Tracking of health-related fitness components in young ages 9 to 12 years. Med. Sci. Sports Exerc. 1998, 30, 910–916. [Google Scholar]
- Nickolas, S. What Do Correlation Coefficients Positive, Negative, and Zero Mean? Available online: https://www.investopedia.com/ask/answers/032515/what-does-it-mean-if-correlation-coefficient-positive-negative-or-zero.asp (accessed on 25 October 2022).
- Kobayashi, M.; Kobayashi, M. The relationship between obesity and seasonal variation in body weight among elementary school children in Tokyo. Econ. Hum. Biol. 2006, 4, 253–261. [Google Scholar] [CrossRef]
- Yoshimura, E.; Tajiri, E.; Hatamoto, Y.; Tanaka, S. Changes in season affect body weight, physical activity, food intake, and sleep in female college students: A preliminary study. Int. J. Environ. Res. Public Health 2020, 17, 8713. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N | Boys Autumn 2000 | N | Boys Spring 2000 | N | Girls Autumn 2000 | N | Girls Spring 2000 |
|---|---|---|---|---|---|---|---|---|
| Median (25:75 IQR) | ||||||||
| Biceps | ||||||||
| 5–10 years | 413 | 4.0 ** (3.0:4.0) | 335 | 4.0 ** (3.5:4.5) | 378 | 5.5 * (4.5:6.5) | 301 | 6.0 (4.5:7.0) |
| 11–15 years | 593 | 3.5 ** (3.0:4.0) | 601 | 4.0 ** (3.5:4.5) | 540 | 6.0 ** (5.0:7.0) | 575 | 6.75 ** (5.5:8.0) |
| Subscapular | ||||||||
| 5–10 years | 413 | 5.0 (5.0:6.0) | 335 | 5.0 (5.0:6.0) | 378 | 6.0 ** (5.0:7.0) | 301 | 6.5 ** (6.0:7.5) |
| 11–15 years | 593 | 5.5 (5.0:6.25) | 599 | 6.0 (5.0:6.5) | 540 | 7.0 ** (6.0:8.0) | 575 | 8.0 ** (6.75:9.0) |
| Triceps | ||||||||
| 5–10 years | 413 | 6.5 (5.5:7.5) | 335 | 6.5 (6.0:7.5) | 378 | 7.88 (6.5:9.0) | 301 | 8.0 (6.5:9.0) |
| 11–15 years | 593 | 6.75 ** (6.0:8.0) | 599 | 7.0 ** (6.0:8.0) | 540 | 9.0 * (7.5:11) | 575 | 9.75 * (8.0:11.5) |
| Suprailiac | ||||||||
| 5–10 years | 413 | 4.0 (3.0:4.0) | 335 | 4.0 (3.5:4.5) | 378 | 5.0 (4.0:6.0) | 301 | 5.0 (4.0:6.0) |
| 11–15 years | 593 | 4.0 ** (3.5:5.0) | 599 | 4.25 ** (4.0:5.0) | 540 | 6.0 ** (5.0:8.0) | 575 | 6.75 ** (5.5:8.0) |
| Variables | N | Boys Autumn 2000 | N | Boys Spring 2000 | N | Girls Autumn 2000 | N | Girls Spring 2000 |
|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | |||||
| Abdominal obesity by ST ratio | ||||||||
| 5–10 years | 413 | 33 (8) | 335 | 24 (7) | 378 | 17 (5) * | 301 | 20 (7) * |
| 11–15 years | 593 | 63 (11) ** | 599 | 45 (8) ** | 540 | 16 (3) ** | 575 | 41 (7) ** |
| Abdominal obesity by SST ratio | ||||||||
| 5–10 years | 413 | 22 (5) | 335 | 22 (7) | 378 | 19 (5) | 301 | 16 (5) |
| 11–15 years | 593 | 25 (4) ** | 599 | 43 (7) ** | 540 | 26 (5) | 575 | 33 (6) |
| Obesity by SSTB ratio | ||||||||
| 5–10 years | 413 | 23 (6) | 335 | 19 (6) | 378 | 13 (3) ** | 130 | 20 (7) ** |
| 11–15 years | 593 | 29 (5) | 599 | 33 (6) | 540 | 30 (6) | 575 | 26 (5) |
| Autumn | Spring | |||||
| Unadjusted | ||||||
| Beta | p Value | 95% CI | Beta | p Value | 95% CI | |
| Abdominal obesity based on ST ratio | −2.633 | <0.001 ** | −2.822:−2.449 | −2.559 | <0.001 ** | −2.738:−2.382 |
| Abdominal obesity based on the SST ratio | −2.991 | <0.001 ** | −3.233:−2.803 | −2.700 | <0.001 ** | −2.893:−2.518 |
| Abdominal obesity based on the SSTB ratio | −2.958 | <0.00 ** | −3.191:−2.756 | −2.860 | <0.001 ** | −3.087:−2.672 |
| Adjusted for age and gender | ||||||
| Abdominal obesity based on ST ratio | −1.084 | 0.054 | −2.302:−0.075 | −2.556 | <0.001 ** | −3.903:−1.432 |
| Abdominal obesity based on the SST ratio | −2.897 | <0.001 ** | −4.331:−1.629 | −2.718 | <0.001 ** | −4.165:−1.501 |
| Abdominal obesity based on the SSTB ratio | −3.088 | <0.001 ** | −4.573:−1.828 | −2.506 | <0.001 ** | −3.885:−1.346 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mulaudzi, L.; Mkhatshwa, T.N.; Makhubedu, M.M.; Matshipi, M.; Lebelo, S.L.; Monyeki, K.D. Investigation of the Seasonal Variation in Fat Patterning of Ellisras Rural Children and Adolescents, in the Limpopo Province, South Africa. Children 2023, 10, 1113. https://doi.org/10.3390/children10071113
Mulaudzi L, Mkhatshwa TN, Makhubedu MM, Matshipi M, Lebelo SL, Monyeki KD. Investigation of the Seasonal Variation in Fat Patterning of Ellisras Rural Children and Adolescents, in the Limpopo Province, South Africa. Children. 2023; 10(7):1113. https://doi.org/10.3390/children10071113
Chicago/Turabian StyleMulaudzi, Lusani, Thandiwe N. Mkhatshwa, Mankopodi M. Makhubedu, Moloko Matshipi, Sogolo L. Lebelo, and Kotsedi D. Monyeki. 2023. "Investigation of the Seasonal Variation in Fat Patterning of Ellisras Rural Children and Adolescents, in the Limpopo Province, South Africa" Children 10, no. 7: 1113. https://doi.org/10.3390/children10071113