
Exploring the Potential of Three-Dimensional Imaging, Printing, and Modeling in Pediatric Surgical Oncology: A New Era of Precision Surgery
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
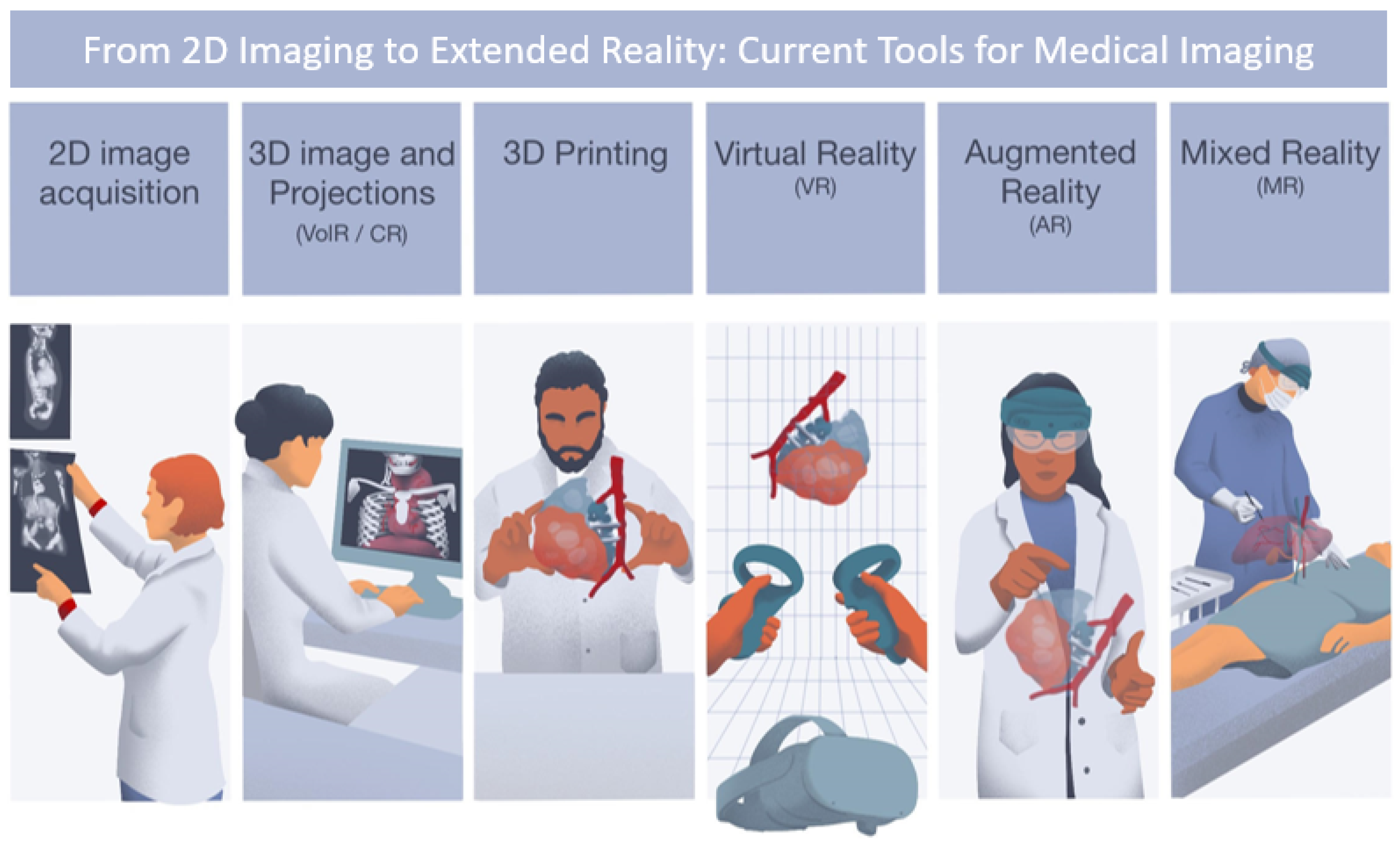
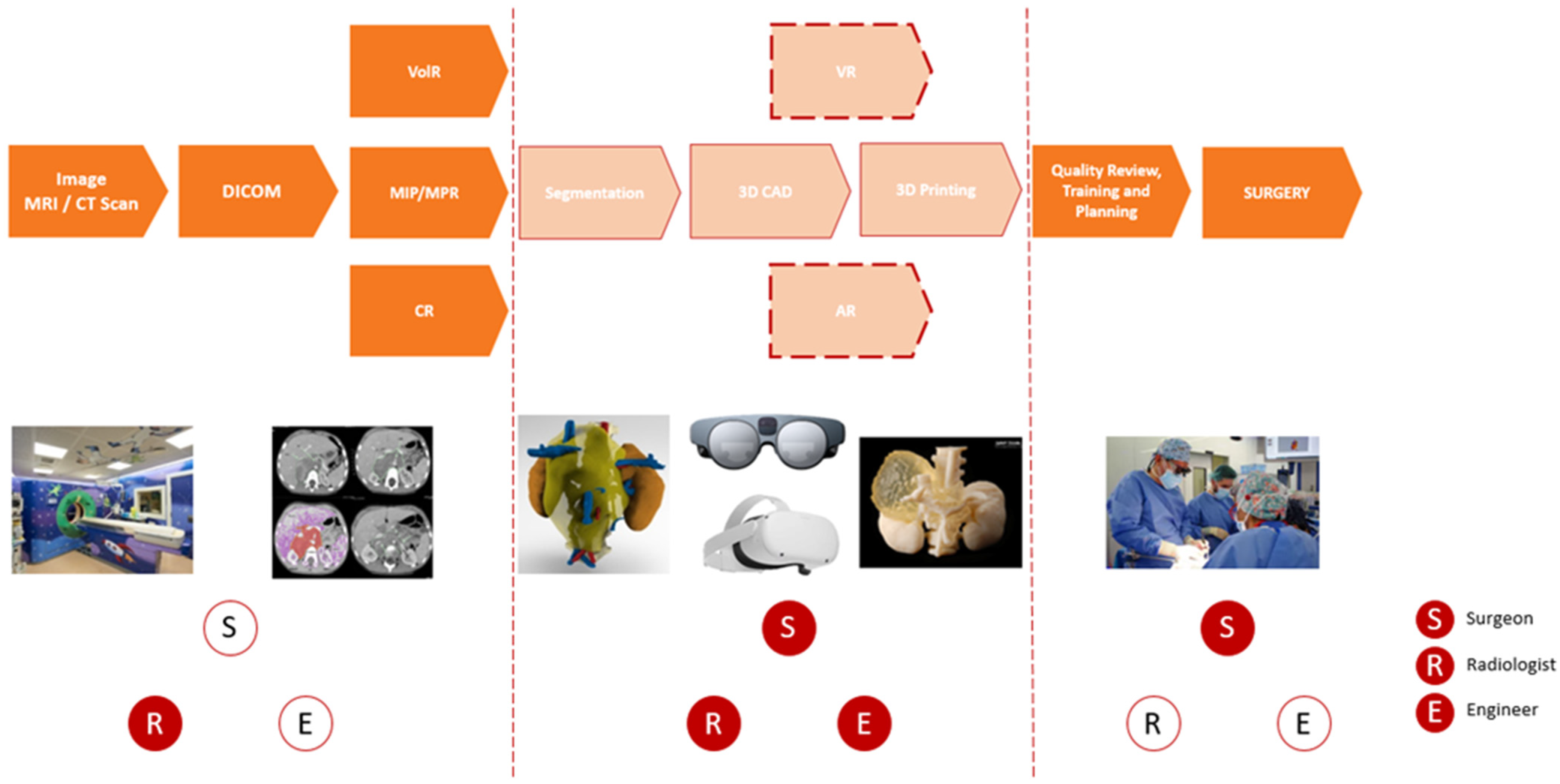
2.1. New Digital Workflow from Image Acquisition to Final Model Representation
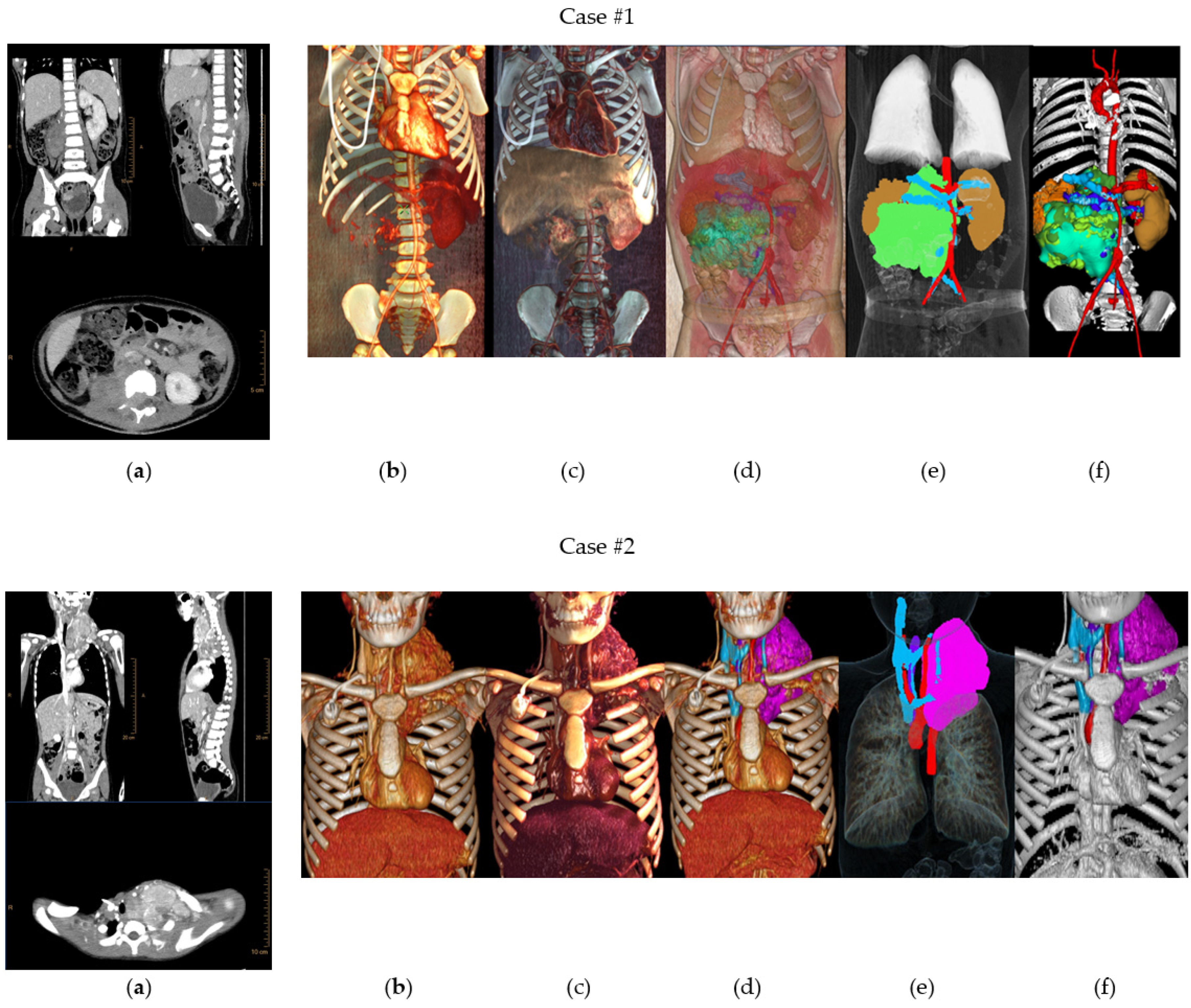
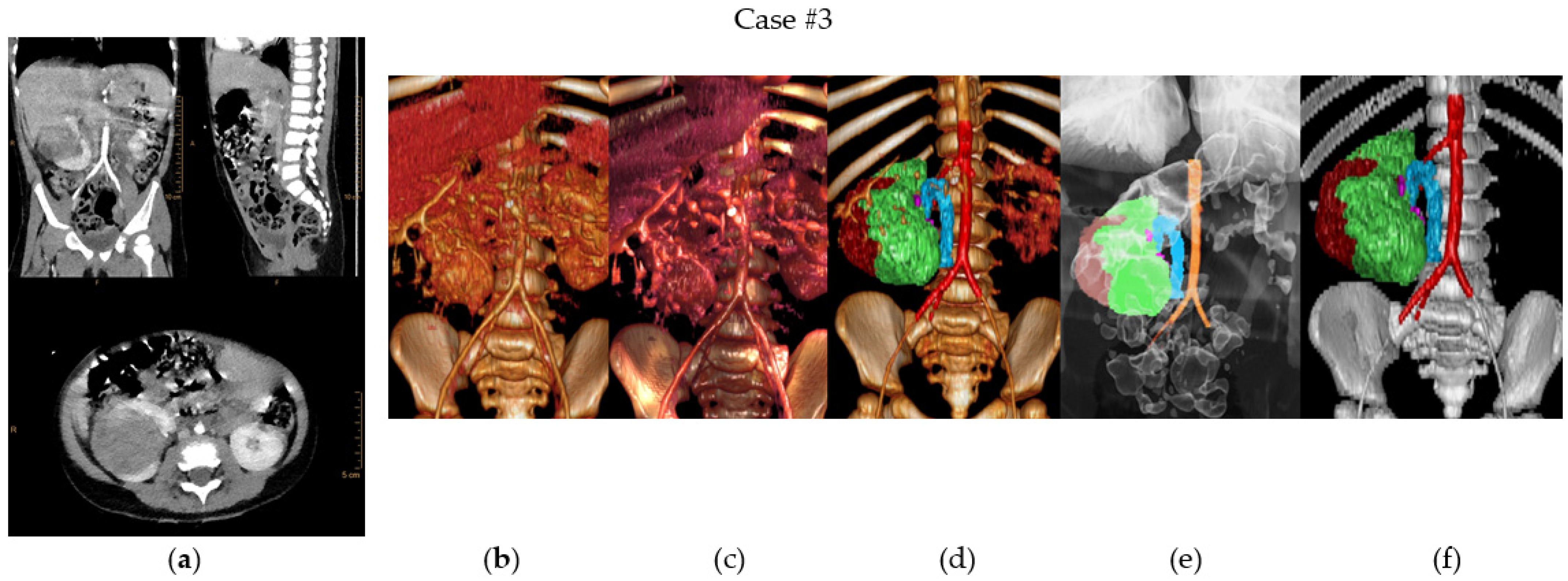
2.2. Case Presentation
2.3. Image Acquisition
2.4. Medical Imaging Projections
2.4.1. Multiplanar Reconstruction
2.4.2. Maximal Intensity Projection
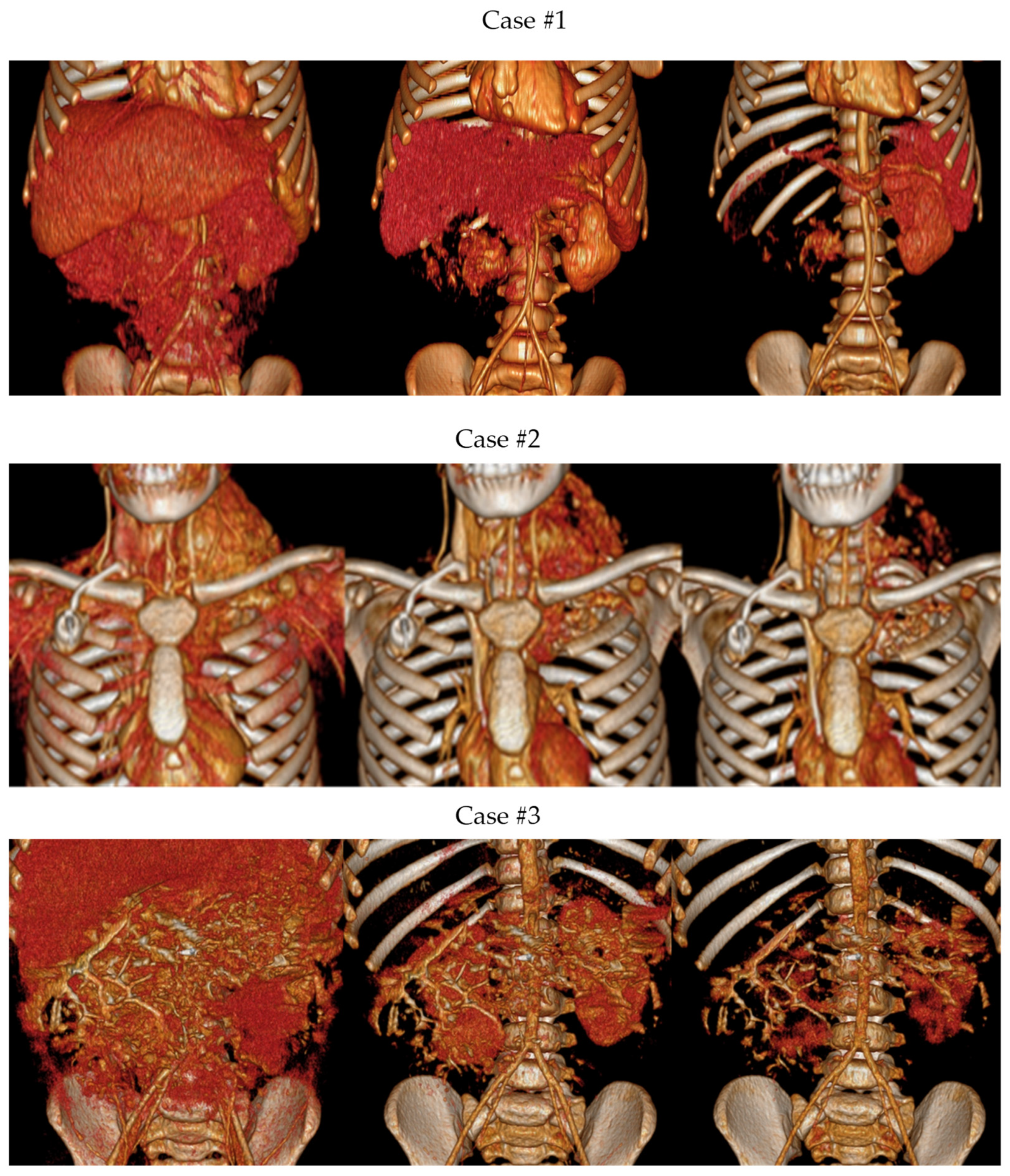
2.4.3. Volume Rendering
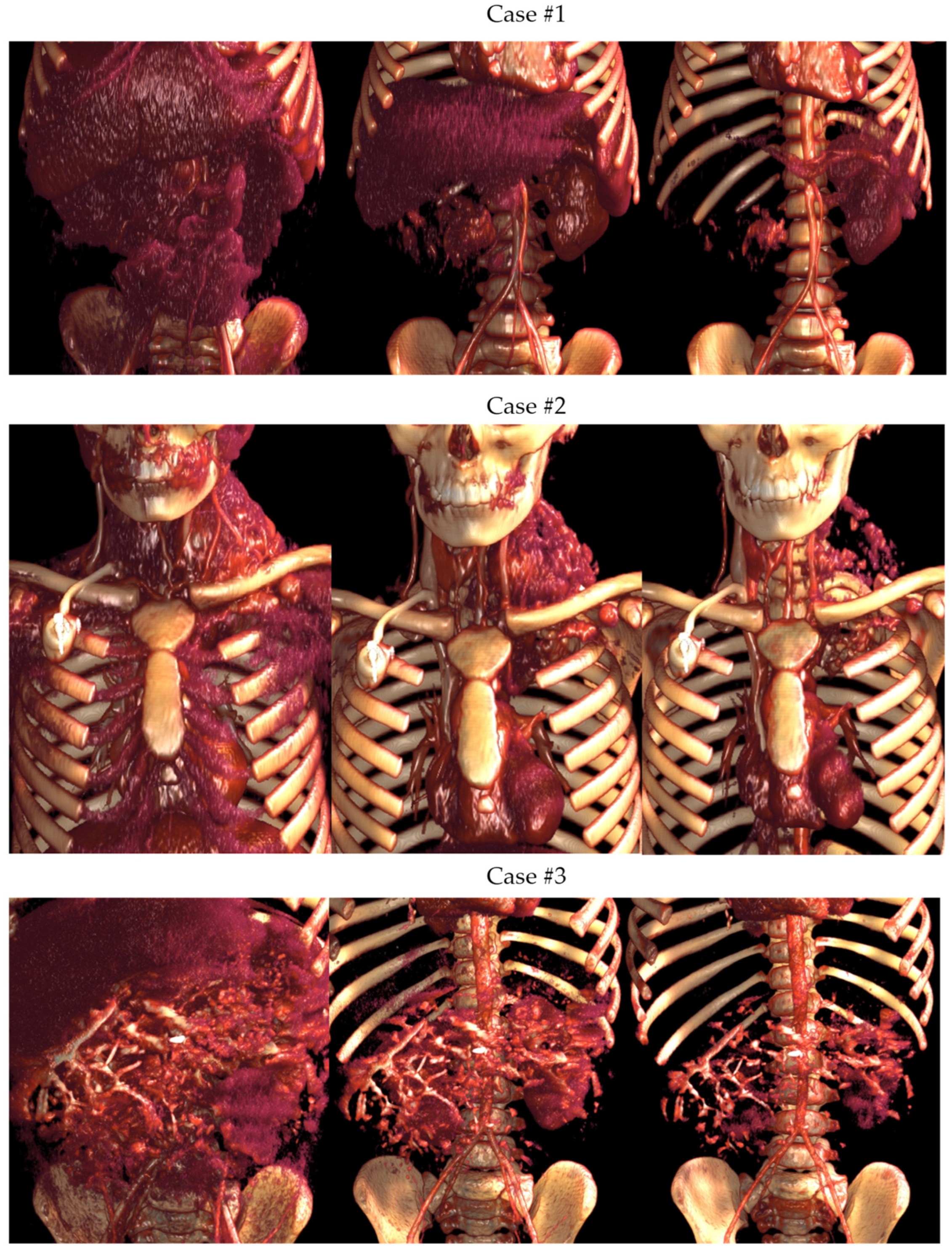
2.4.4. Cinematic Rendering
2.5. Image Segmentation
2.6. CAD Design and 3D Modeling
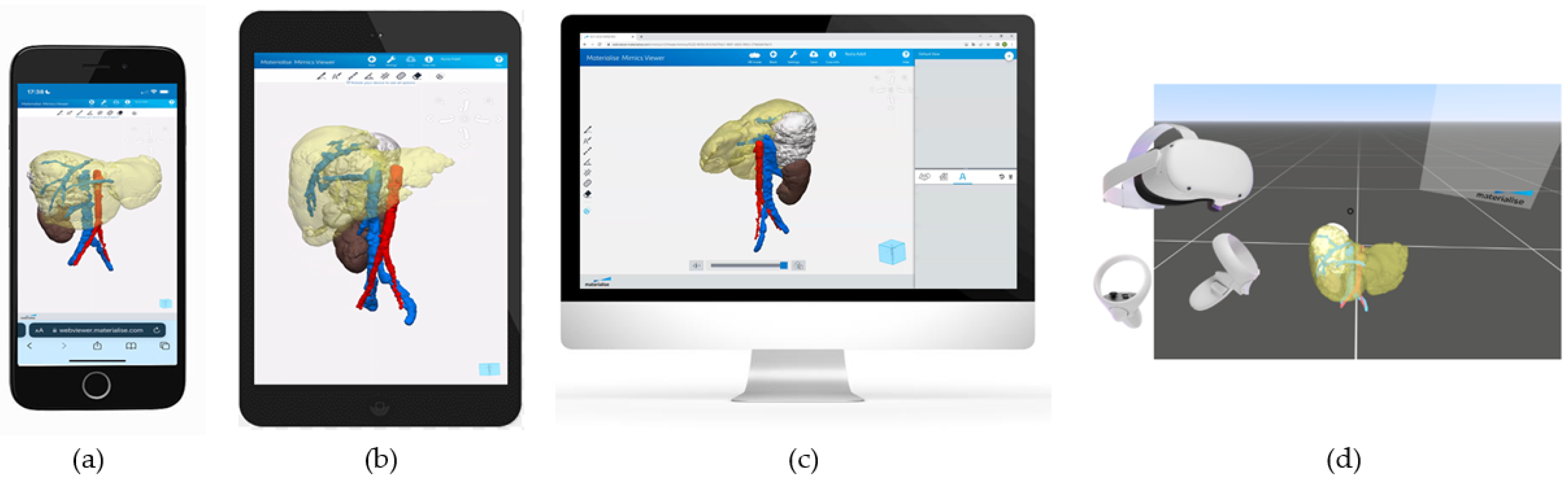
2.7. Three-Dimensional Virtual Simulation and VR
2.8. VR and AR
2.9. Three-dimensional Printing
3. Results
3.1. Three-Dimensional Planning Models: From Imaging Projections to VR and 3D Printed Models
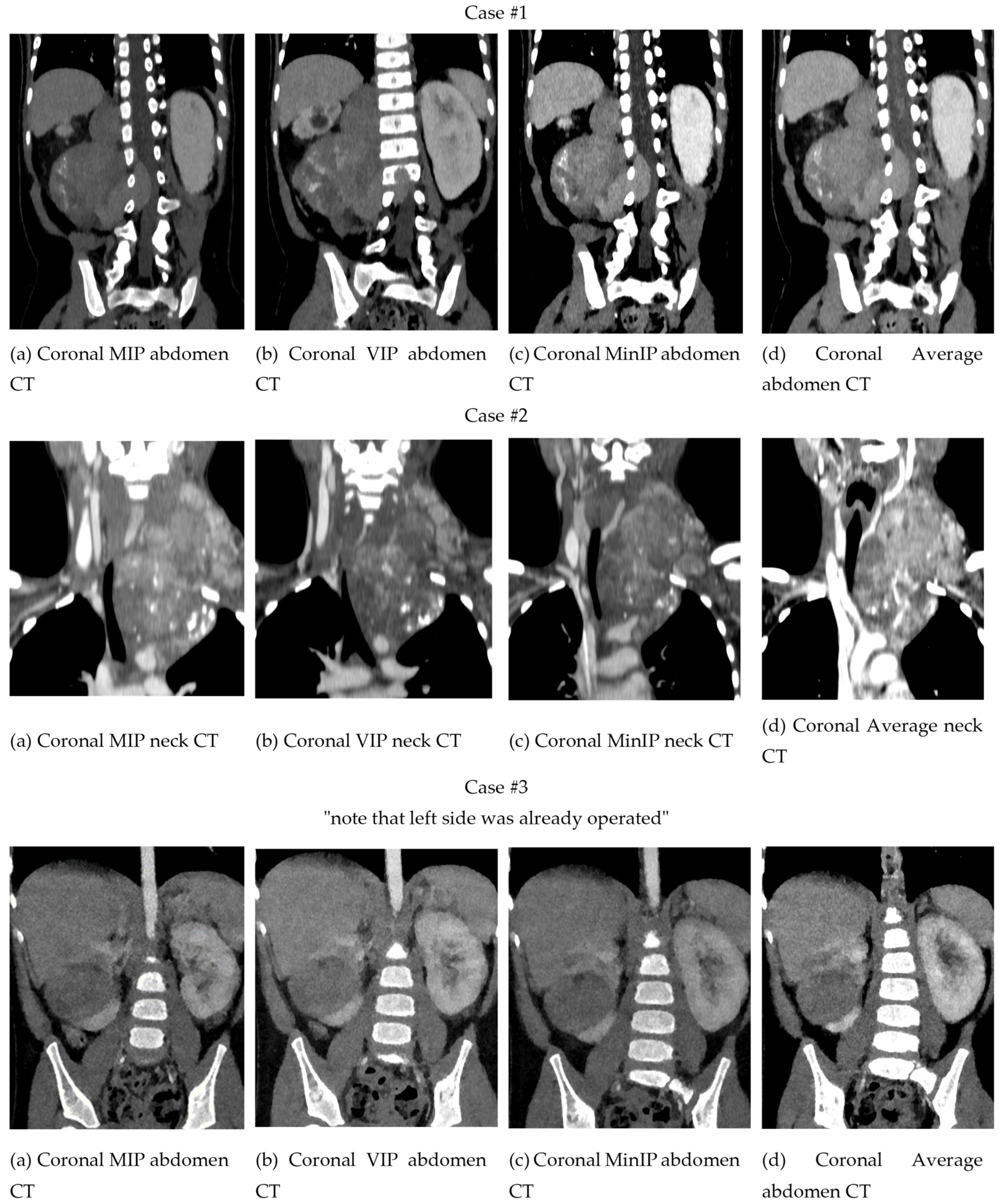
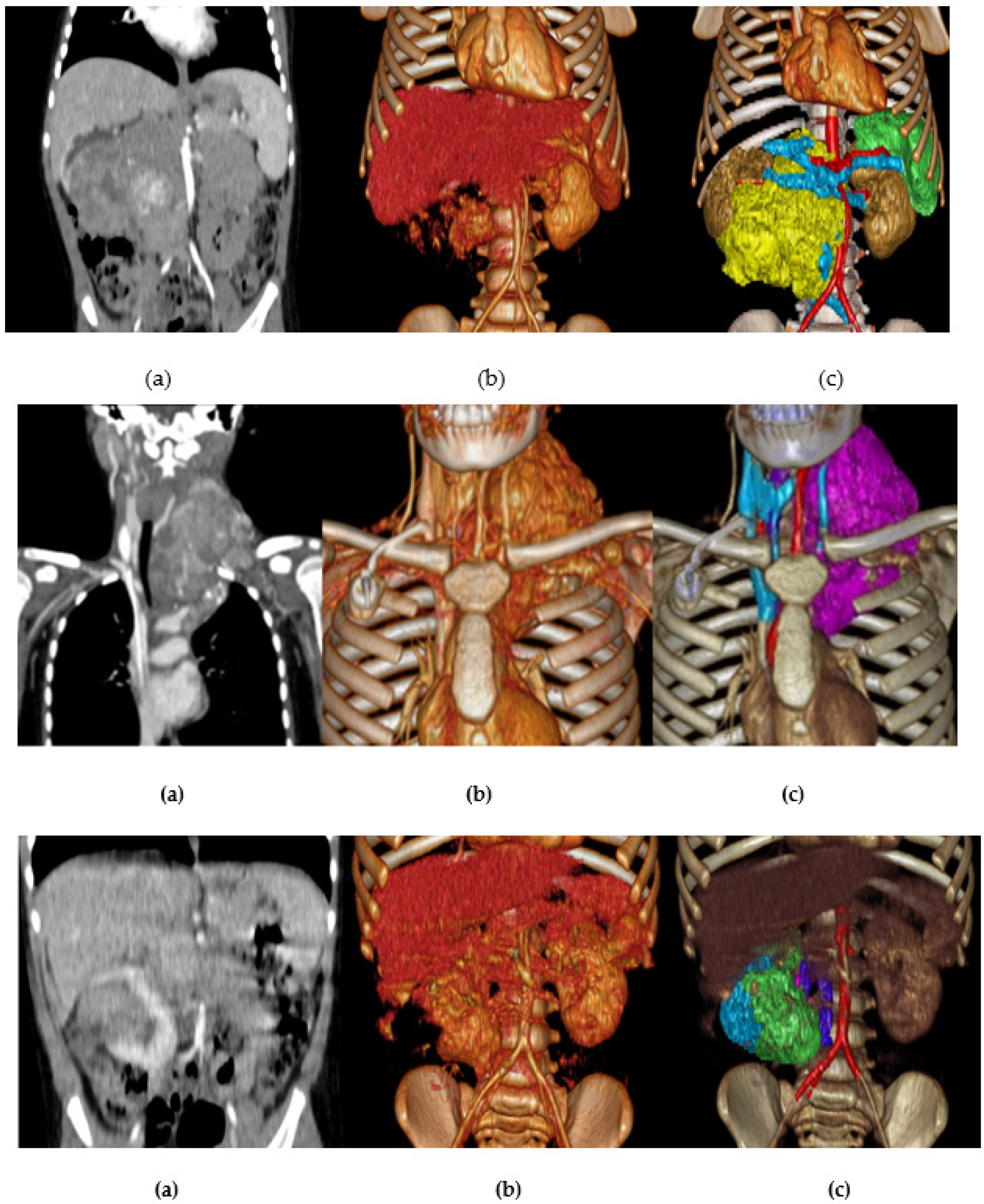
3.1.1. Two-Dimensional Projection Renderings
3.1.2. Volume Rendering and Cinematic Rendering
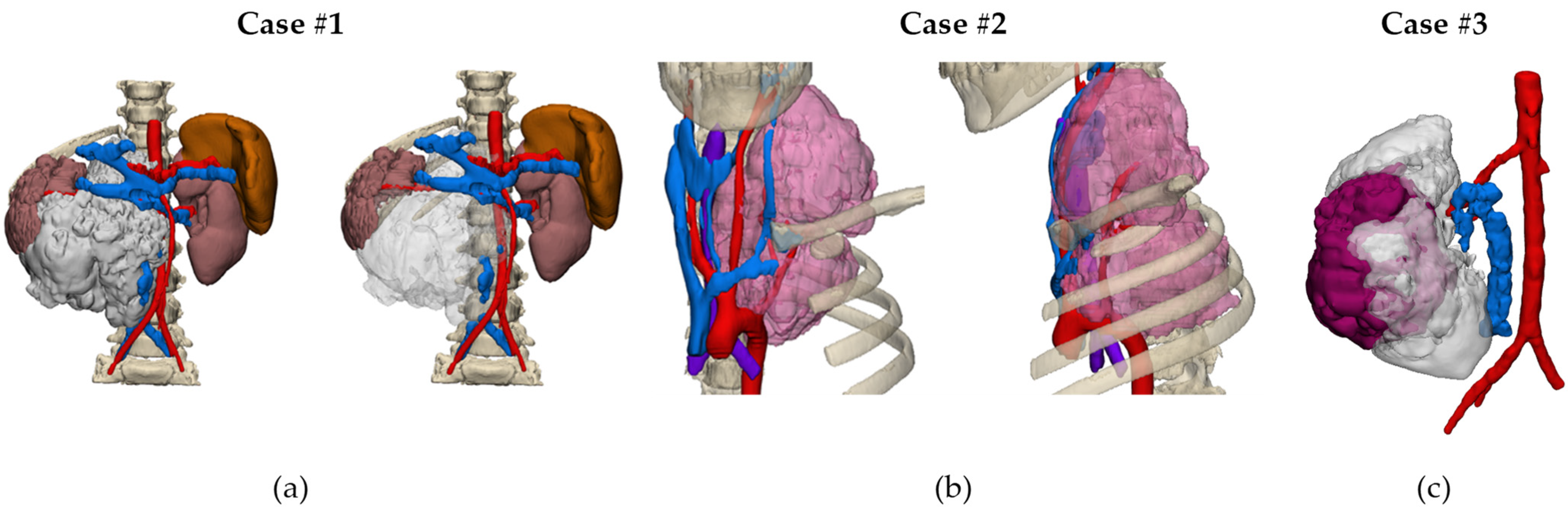
3.1.3. Three-Dimensional Virtual Simulations (CAD Models)
3.1.4. Virtual and Augmented Reality
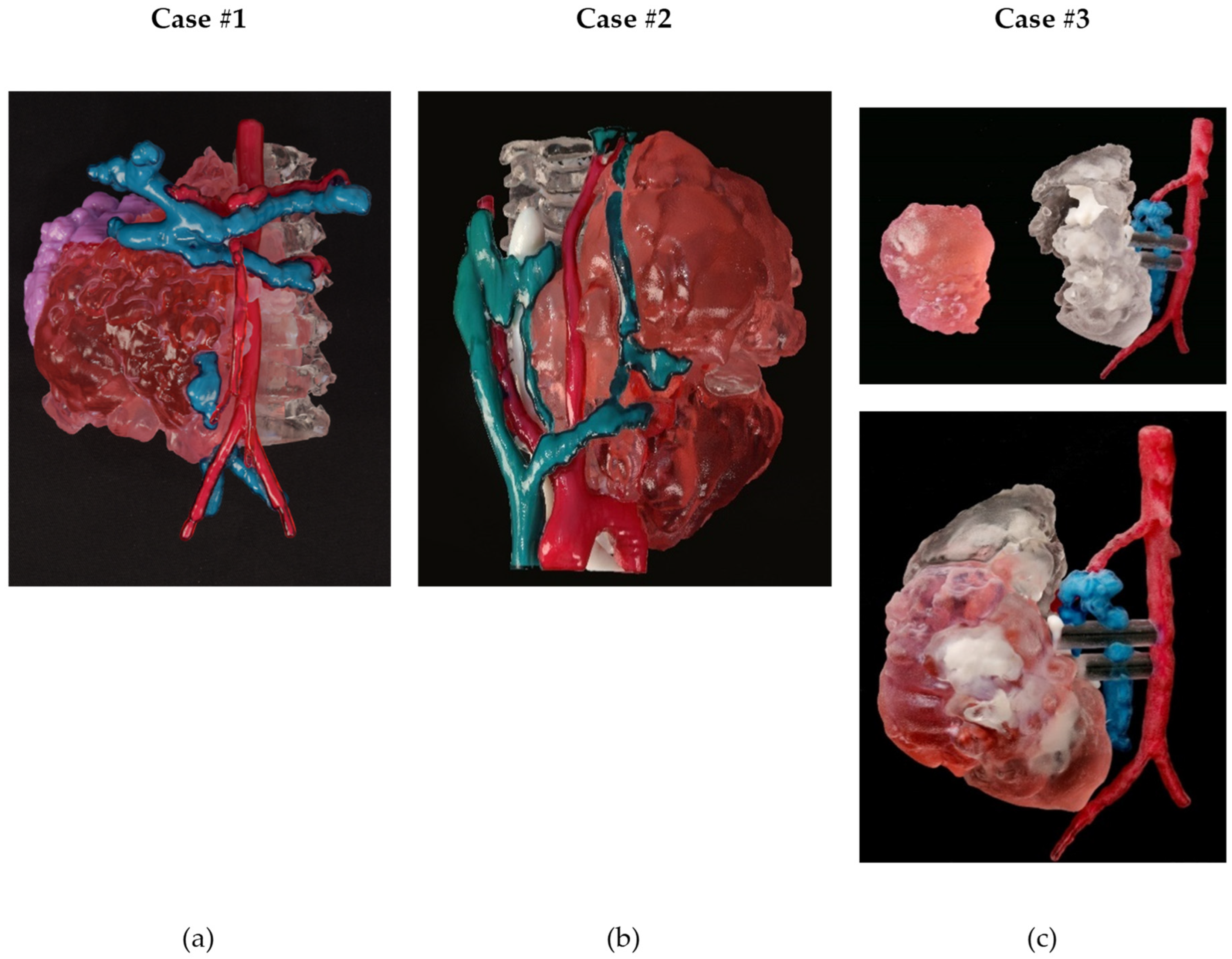
3.1.5. Three-Dimensional Printing
3.2. General Considerations
4. Discussion
4.1. Advantages and Pitfalls of Each Approach for the Differential Diagnosis and Treatment
4.2. Clinical Relevance
4.2.1. From a Surgical Point of View
4.2.2. From a Radiological Point of View
4.3. Limitations of the Technique
- Image Quality: The quality of the final rendering can be affected by the quality and resolution of the original imaging data, as well as the specific algorithms and techniques used in the rendering process.
- Patient Variability: Different patients can have different anatomies, tissue densities, and other factors that affect the accuracy and reliability of the renderings.
- Interobserver variability: Different radiologists or physicians may interpret the images differently, leading to variations in the diagnosis or treatment plan.
- Time-consuming: The rendering process can be time-consuming and may require specialized software and hardware, which can be costly.
- Limited applicability: The renderings may not be suitable for all types of medical imaging, such as nuclear medicine or ultrasound, which have different modalities.
- Training: Medical professionals need to be trained to use the software and interpret the images correctly.
- Costs: The procurement of 3D printing technologies such as 3D printer, VR or AR headsets, or software packages to implement advanced projection techniques (VolR or CR), as well as the resources needed for bioengineers and setting an in-house lab, may be a limitation for the adoption of the presented techniques.
- Regulation: Complying with local regulations to use these new technologies for surgical planning and treatment can be a barrier to their implementation, mainly due to the time and resources needed.
- Lack of Validation: Some of the techniques used in medical imaging rendering have still to be validated for clinical use.
- Privacy and security: Storing and sharing of medical imaging data can raise privacy and security concerns.
4.4. Limitations of This Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wijnen, M. Innovations in pediatric surgical oncology. J. Pediatr. Surg. 2022, 57, 967–969. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, S.D.; Heaton, T.E.; Bondoc, A.; Dasgupta, R.; Abdelhafeez, A.; Davidoff, A.M.; Lautz, T.B. Evolving applications of fluorescence guided surgery in pediatric surgical oncology: A practical guide for surgeons. J. Pediatr. Surg. 2021, 56, 215–223. [Google Scholar] [CrossRef]
- Jacobson, J.C.; Scrushy, M.G.; Gillory, L.A.; Pandya, S.R. Utilization of robotics in pediatric surgical oncology. Semin. Pediatr. Surg. 2023, 32, 151263. [Google Scholar] [CrossRef] [PubMed]
- Lazar, J.F.; Hwalek, A.E. A review of Robotic Thoracic Surgery Adoption and Future Innovations. Thorac. Surg. Clin. 2023, 33, 1–10. [Google Scholar] [CrossRef]
- Warmann, S.; Fuchs, J.; Jesch, N.K.; Schrappe, M.; Ure, B.M. A prospective study of minimally invasive techniques in pediatric surgical oncology: Preliminary report. Med. Pediatr. Oncol. 2003, 40, 155–157. [Google Scholar] [CrossRef]
- Tejo-Otero, A.; Buj-Corral, I.; Fenollosa-Artés, F. 3D Printing in Medicine for Preoperative Surgical Planning: A Review. Ann. Biomed. Eng. 2019, 48, 536–555. [Google Scholar] [CrossRef] [PubMed]
- Fox, M.; Peregrin, T. 3-D printing: Revolutionizing preoperative planning, resident training, and the future of surgical care. Bull. Am. Coll. Surg. 2016, 101, 9–18. Available online: https://bulletin.facs.org/2016/07/3-d-printing-revolutionizing-preoperative-planning-resident-training-and-the-future-of-surgical-care/ (accessed on 30 November 2022).
- Krauel, L.; Fenollosa, F.; Riaza, L.; Pérez, M.; Tarrado, X.; Morales, A.; Gomà, J.; Mora, J. Use of 3D Prototypes for Complex Surgical Oncologic Cases. World J. Surg. 2015, 40, 889–894. [Google Scholar] [CrossRef]
- Tack, P.; Victor, J.; Gemmel, P.; Annemans, L. 3D-printing techniques in a medical setting: A systematic literature review. Biomed. Eng. Online 2016, 15, 115. [Google Scholar] [CrossRef]
- Krauel, L.; Valls-Esteve, A.; Tejo-Otero, A.; Fenollosa-Artés, F. 3D-Printing in surgery: Beyond bone structures. A review. Ann. 3D Print. Med. 2021, 4, 100039, ISSN 2666-964. [Google Scholar] [CrossRef]
- Privitera, L.; Paraboschi, I.; Dixit, D.; Arthurs, O.J.; Giuliani, S. Image-guided surgery and novel intraoperative devices for enhanced visualisation in general and paediatric surgery: A Review. Innov. Surg. Sci. 2021, 6, 161–172. [Google Scholar] [CrossRef]
- Aimar, A.; Palermo, A.; Innocenti, B. The Role of 3D Printing in Medical Applications: A State of the Art. J. Healthc. Eng. 2019, 2019, 5340616. [Google Scholar] [CrossRef]
- Wake, N.; Nussbaum, J.E.; Elias, M.I.; Nikas, C.V.; Bjurlin, M.A. 3D printing, augmented reality, and virtual reality for the assessment and management of kidney and prostate cancer: A systematic review. Urology 2020, 143, 20–32. [Google Scholar] [CrossRef]
- Calhoun, P.S.; Kuszyk, B.S.; Heath, D.G.; Carley, J.C.; Fishman, E.K. Three-dimensional volume rendering of spiral CT data: Theory and method. Radiographics 1999, 19, 745–764. [Google Scholar] [CrossRef] [PubMed]
- Eid, M.; De Cecco, C.N.; Nance, J.W., Jr.; Caruso, D.; Albrecht, M.H.; Spandorfer, A.J.; De Santis, D.; Varga-Szemes, A.; Schoepf, U.J. Cinematic rendering in CT: A novel, lifelike 3D visualization technique. Am. J. Roentgenol. 2017, 209, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Dappa, E.; Higashigaito, K.; Fornaro, J.; Leschka, S.; Wildermuth, S.; Alkadhi, H. Cinematic rendering—An alternative to volume rendering for 3D computed tomography imaging. Insights Imaging 2016, 7, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, M.E.; Pena, I.R.; Castillo, R.E.B.; Sufianov, A.; Goncharov, E.; Sanchez, J.A.S.; Colome-Hidalgo, M.; Nurmukhametov, R.; Céspedes, J.R.C.; Montemurro, N. Development of a 3D Printed Brain Model with Vasculature for Neurosurgical Procedure Visualisation and Training. Biomedicines 2023, 11, 330. [Google Scholar] [CrossRef]
- Prunoiu, V.-M.; Popa, D.; Serbulea, M.-S.; Bratucu, E.; Simion, L.; Bratucu, M.N. Augmented Reality in Surgical Oncology. A Literature Review. Chirurgia 2022, 117, 517–525. [Google Scholar] [CrossRef]
- Fitski, M.; Meulstee, J.W.; Littooij, A.S.; van de Ven, C.P.; van der Steeg, A.F.W.; Wijnen, M.H. MRI-based 3-dimensional visualization workflow for the preoperative planning of nephron-sparing surgery in wilms’ tumor surgery: A pilot study. J. Healthc. Eng. 2020, 2020, 8899049. [Google Scholar] [CrossRef]
- Elshafei, M.; Binder, J.; Baecker, J.; Brunner, M.; Uder, M.; Weber, G.F.; Grützmann, R.; Krautz, C. Comparison of Cinematic Rendering and Computed Tomography for Speed and Comprehension of Surgical Anatomy. JAMA Surg. 2019, 154, 738–744. [Google Scholar] [CrossRef]
- Pereira, H.R.; Barzegar, M.; Hamadelseed, O.; Esteve, A.V.; Munuera, J. 3D surgical planning of pediatric tumors: A review. Int. J. Comput. Assist. Radiol. Surg. 2022, 17, 805–816. [Google Scholar] [CrossRef]
- Capellini, K.; Tripicchio, P.; Vignali, E.; Gasparotti, E.; Ali, L.A.; Cantinotti, M.; Federici, D.; Santoro, G.; Alfonzetti, F.; Evangelista, C.; et al. 3D Printing and 3D Virtual Models for Surgical and Percutaneous Planning of Congenital Heart Diseases. In Proceedings of the 15th International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications (VISIGRAPP 2020), Valletta, Malta, 27–29 February 2020; Volume 3, pp. 81–287. [Google Scholar] [CrossRef]
- Eijlers, R.; Utens, E.M.W.J.; Staals, L.M.; de Nijs, P.F.A.; Berghmans, J.M.; Wijnen, R.M.H.; Hillegers, M.H.J.; Dierckx, B.; Legerstee, J.S. Meta-analysis: Systematic review and meta-analysis of virtual reality in pediatrics: Effects on pain and anxiety. Anesth. Analg. 2019, 129, 1344. [Google Scholar] [CrossRef]
- Yeung, A.W.K.; Tosevska, A.; Klager, E.; Eibensteiner, F.; Laxar, D.; Stoyanov, J.; Glisic, M.; Zeiner, S.; Kulnik, S.T.; Crutzen, R.; et al. Virtual and Augmented Reality Applications in Medicine: Analysis of the Scientific Literature. J. Med. Internet Res. 2021, 23, e25499. [Google Scholar] [CrossRef] [PubMed]
- Lewis, T.; Aggarwal, R.; Rajaretnam, N.; Grantcharov, T.; Darzi, A. Training in surgical oncology—The role of VR simulation. Surg. Oncol. 2011, 20, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Souzaki, R.; Ieiri, S.; Uemura, M.; Ohuchida, K.; Tomikawa, M.; Kinoshita, Y.; Koga, Y.; Suminoe, A.; Kohashi, K.; Oda, Y.; et al. An augmented reality navigation system for pediatric oncologic surgery based on preoperative CT and MRI images. J. Pediatr. Surg. 2013, 48, 2479–2483. [Google Scholar] [CrossRef] [PubMed]
- Barteit, S.; Lanfermann, L.; Bärnighausen, T.; Neuhann, F.; Beiersmann, C. Augmented, mixed, and virtual reality-based head-mounted devices for medical education: Systematic review. JMIR Serious Games 2021, 9, e29080. [Google Scholar] [CrossRef]
- Quero, G.; Lapergola, A.; Soler, L.; Shahbaz, M.; Hostettler, A.; Collins, T.; Marescaux, J.; Mutter, D.; Diana, M.; Pessaux, P. Virtual and Augmented Reality in Oncologic Liver Surgery. Surg. Oncol. Clin. N. Am. 2019, 28, 31–44. [Google Scholar] [CrossRef]
- Vervoorn, M.T.; Wulfse, M.; Van Doormaal, T.P.C.; Ruurda, J.P.; Van der Kaaij, N.P.; De Heer, L.M. Mixed Reality in Modern Surgical and Interventional Practice: Narrative Review of the Literature. JMIR Serious Games 2023, 11, e41297. [Google Scholar] [CrossRef] [PubMed]
- Wellens, L.M.; Meulstee, J.; van de Ven, C.P.; van Scheltinga, C.E.J.T.; Littooij, A.S.; van den Heuvel-Eibrink, M.M.; Fiocco, M.; Rios, A.C.; Maal, T.; Wijnen, M.H.W.A. Comparison of 3-Dimensional and Augmented Reality Kidney Models with Conventional Imaging Data in the Preoperative Assessment of Children with Wilms Tumors. JAMA Netw. Open 2019, 2, e192633. [Google Scholar] [CrossRef]
- Arjomandi Rad, A.; Vardanyan, R.; Thavarajasingam, S.G.; Zubarevich, A.; Van den Eynde, J.; Pompeu B O Sá, M.; Zhigalov, K.; Nia, P.S.; Ruhparwar, A.; Weymann, A. Extended, virtual and augmented reality in thoracic surgery: A systematic review. Interact. CardioVascular Thorac. Surg. 2022, 34, 201–211. [Google Scholar] [CrossRef]
- Meglioli, M.; Naveau, A.; Macaluso, G.M.; Catros, S. 3D printed bone models in oral and cranio-maxillofacial surgery: A systematic review. 3D Print. Med. 2020, 6, 30. [Google Scholar] [CrossRef] [PubMed]
- Gehrsitz, P.; Rompel, O.; Schöber, M.; Cesnjevar, R.; Purbojo, A.; Uder, M.; Dittrich, S.; Alkassar, M. Cinematic Rendering in Mixed-Reality Holograms: A New 3D Preoperative Planning Tool in Pediatric Heart Surgery. Front. Cardiovasc. Med. 2021, 8, 633611. [Google Scholar] [CrossRef] [PubMed]
- Brun, H.; Bugge, R.A.B.; Suther, K.R.; Birkeland, S.; Kumar, R.; Pelanis, E.; Elle, O.J. Mixed reality holograms for heart surgery planning: First user experience in congenital heart disease. Eur. Heart J. Cardiovasc. Imaging 2018, 20, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Lau, I.; Gupta, A.; Ihdayhid, A.; Sun, Z. Clinical Applications of Mixed Reality and 3D Printing in Congenital Heart Disease. Biomolecules 2022, 12, 1548. [Google Scholar] [CrossRef]
- Ruggiero, F.; Cercenelli, L.; Emiliani, N.; Badiali, G.; Bevini, M.; Zucchelli, M.; Marcelli, E.; Tarsitano, A. Preclinical Application of Augmented Reality in Pediatric Craniofacial Surgery: An Accuracy Study. J. Clin. Med. 2023, 12, 2693. [Google Scholar] [CrossRef]
- Barcali, E.; Iadanza, E.; Manetti, L.; Francia, P.; Nardi, C.; Bocchi, L. Augmented Reality in Surgery: A Scoping Review. Appl. Sci. 2022, 12, 6890. [Google Scholar] [CrossRef]
- Byrd, C.T.; Lui, N.S.; Guo, H.H. Applications of Three-Dimensional Printing in Surgical Oncology. Surg. Oncol. Clin. N. Am. 2022, 31, 673–684. [Google Scholar] [CrossRef]
- Wijnen, M.W.; Davidoff, A.M. Minimally Invasive Techniques in Pediatric Surgical Oncology. Surg. Oncol. Clin. N. Am. 2021, 30, 417–430. [Google Scholar] [CrossRef]
- Souzaki, R.; Taguchi, T. Navigational Techniques in Pediatric Surgical Oncology. In Pediatric Surgical Oncology; CRC Press: Boca Raton, FL, USA, 2022; pp. 439–445. [Google Scholar] [CrossRef]
- Schima, W.; Böhm, G.; Rösch, C.S.; Klaus, A.; Függer, R.; Kopf, H. Mass-forming pancreatitis versus pancreatic ductal adenocarcinoma: CT and MR imaging for differentiation. Cancer Imaging 2020, 20, 52. [Google Scholar] [CrossRef]
- Pandey, P.; Lewis, H.; Pandey, A.; Schmidt, C.; Dillhoff, M.; Kamel, I.R.; Pawlik, T.M. Updates in hepatic oncology imaging. Surg. Oncol. 2017, 26, 195–206. [Google Scholar] [CrossRef]
- Montemurro, N.; Condino, S.; Carbone, M.; Cattari, N.; D’amato, R.; Cutolo, F.; Ferrari, V. Brain Tumor and Augmented Reality: New Technologies for the Future. Int. J. Environ. Res. Public Health 2022, 19, 6347. [Google Scholar] [CrossRef] [PubMed]
- Langdon, C.; Hinojosa-Bernal, J.; Munuera, J.; Gomez-Chiari, M.; Haag, O.; Veneri, A.; Valldeperes, A.; Valls, A.; Adell, N.; Santamaria, V.; et al. 3D printing as surgical planning and training in pediatric endoscopic skull base surgery—Systematic review and practical example. Int. J. Pediatr. Otorhinolaryngol. 2023, 168, 111543. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Li, C.; Xiao, C.; Zhang, Z.; Ma, J.; Gao, J.; Shao, P.; Valerio, I.; Pawlik, T.M.; Ding, C.; et al. A Wearable Augmented Reality Navigation System for Surgical Telementoring Based on Microsoft HoloLens. Ann. Biomed. Eng. 2020, 49, 287–298. [Google Scholar] [CrossRef] [PubMed]
- Romao, R.L.P.; van der Steeg, A.F.W.; Malek, M.; Irtan, S.; Gow, K.; Ghandour, K.; Biasoni, D.; Davidoff, A.; Pachl, M. Technical advances in the surgical management of Wilms tumors in children. Pediatr. Blood Cancer 2023, 70, e30267. [Google Scholar] [CrossRef] [PubMed]
- Paraboschi, I.; Mantica, G.; Minoli, D.G.; De Marco, E.A.; Gnech, M.; Bebi, C.; Manzoni, G.; Berrettini, A. Fluorescence-Guided Surgery and Novel Innovative Technologies for Improved Visualization in Pediatric Urology. Int. J. Environ. Res. Public Health 2022, 19, 11194. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | Sex | Diagnosis | Surgical Approach | |
|---|---|---|---|---|
| Case #1 | 3 | F | Abdominal neuroblastoma | Laparotomy |
| Case #2 | 11 | F | Thoracic Inlet neuroblastoma | Trap Door |
| Case #3 | 2 | F | Bilateral Wilms tumor (nephron-sparing surgery) | Bilateral Transverse Laparotomy |
| Case | Technology | Printer | Printing Time | Cost | Model Materials | Support Material |
|---|---|---|---|---|---|---|
| 1 | Material Jetting | J5 MediJet© | 1 day 12 h 36 min | EUR 486,70 | VeroCyan™V for veins, VeroMagenta™V for arteries, Med610 for bone; tumor was printed with a combination of VeroMagenta™V + Elastico Clear with 60A shore hardness | SUP710™ (Water removable) |
| 2 | Material Jetting | J5 MediJet© | 24 h 21 min | EUR 435,51 | VeroCyan™V for veins, VeroMagenta™V for arteries, Med610 for bone, DraftWhite for airway; tumor was printed with a combination of VeroMagenta™V + Elastico Clear with 60A shore hardness | SUP710™ (Water removable) |
| 3 | Material Jetting | J5 MediJet© | 10 h 56 min | EUR 130,33 | VeroCyan™V for veins, VeroMagenta™V for arteries, Med610 for the kidney, DraftWhite for calyces; tumor was printed with a combination of VeroMagenta™V + Elastico Clear with 60A shore hardness | SUP710™ (Water removable) |
| Image Post-Processing | Cost | Time | Virtual Visualization | Tactile Planning | Main Advantages | Recommended Indication |
|---|---|---|---|---|---|---|
| MIP/MPR | Low | Low (10 min) | Yes | No |
|
|
| VolR | Low | Low (10 min) | Yes | No |
|
|
| CR | Low | Low (10 min) | Yes | No |
|
|
| 3D CAD | Mid | Mid (1 h) | Yes | No |
|
|
| 3D PRINT | High | High (from 11 h to 1 day and 12 h) | Yes | Yes |
|
|
| VR | Mid | Mid (1 h 15 min) | Yes | Yes |
|
|
| AR | Mid | Mid (1 h 15 min) | Yes | Yes |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valls-Esteve, A.; Adell-Gómez, N.; Pasten, A.; Barber, I.; Munuera, J.; Krauel, L. Exploring the Potential of Three-Dimensional Imaging, Printing, and Modeling in Pediatric Surgical Oncology: A New Era of Precision Surgery. Children 2023, 10, 832. https://doi.org/10.3390/children10050832
Valls-Esteve A, Adell-Gómez N, Pasten A, Barber I, Munuera J, Krauel L. Exploring the Potential of Three-Dimensional Imaging, Printing, and Modeling in Pediatric Surgical Oncology: A New Era of Precision Surgery. Children. 2023; 10(5):832. https://doi.org/10.3390/children10050832
Chicago/Turabian StyleValls-Esteve, Arnau, Núria Adell-Gómez, Albert Pasten, Ignasi Barber, Josep Munuera, and Lucas Krauel. 2023. "Exploring the Potential of Three-Dimensional Imaging, Printing, and Modeling in Pediatric Surgical Oncology: A New Era of Precision Surgery" Children 10, no. 5: 832. https://doi.org/10.3390/children10050832