
Mannitol Challenge to Assess Therapy Response in Asthmatic Children: An Interventional Cohort Study

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Ethical Permission
2.2. Study Design
2.3. Mannitol Dry Powder Challenge
2.4. Statistical Analysis
3. Results
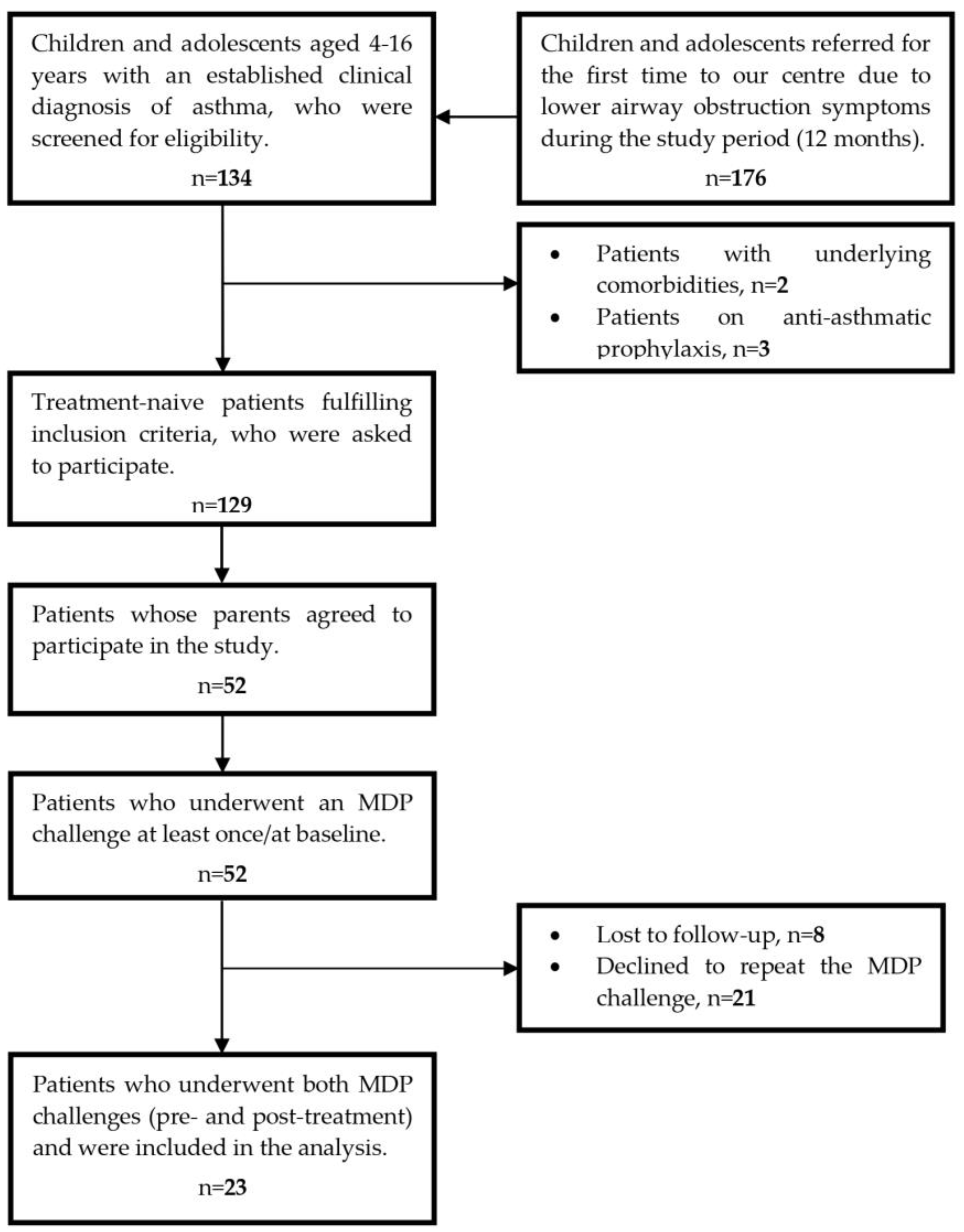
3.1. Subjects
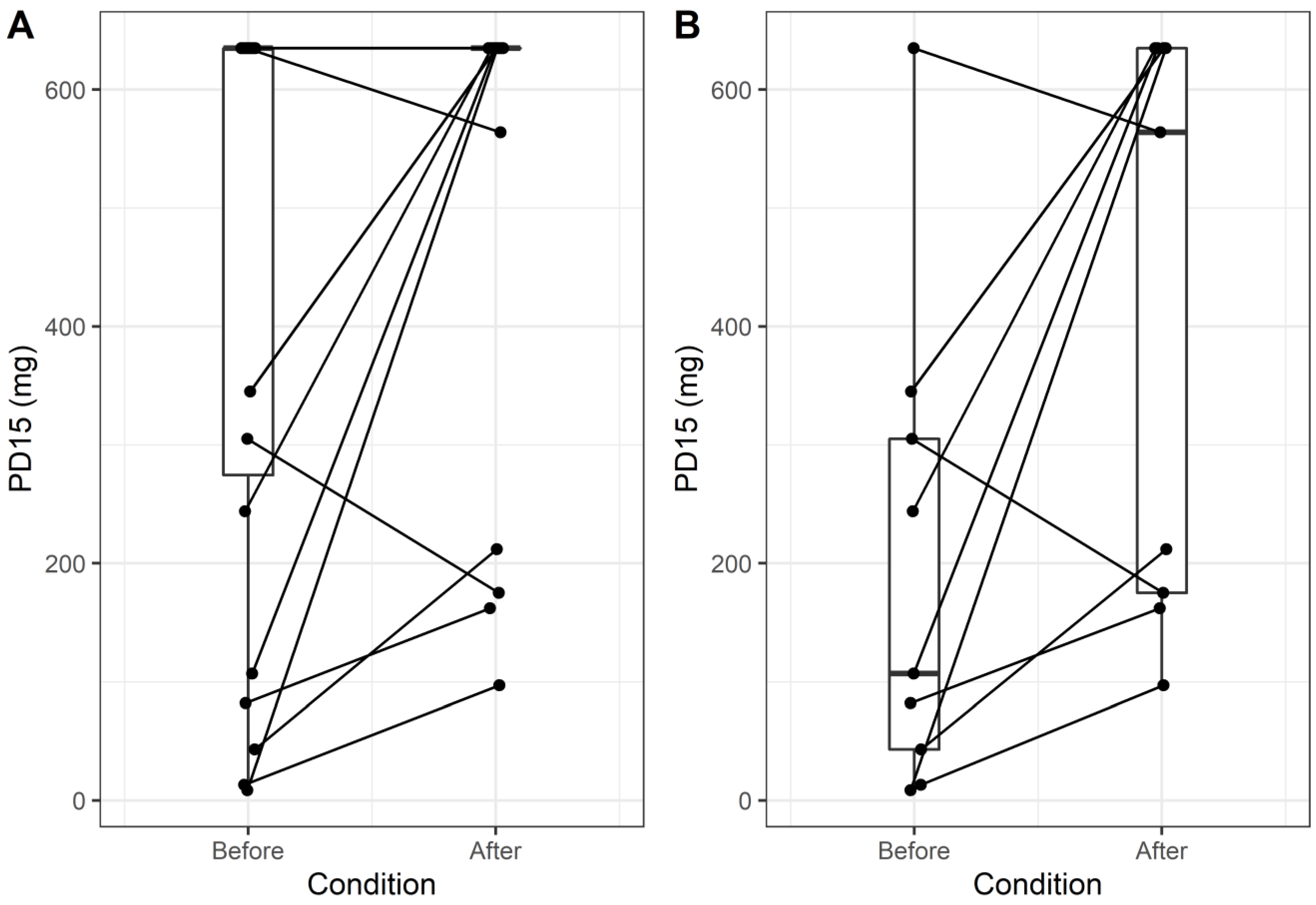
3.2. Effect of Asthma Prophylaxis on Clinical Outcomes and BHR to Mannitol
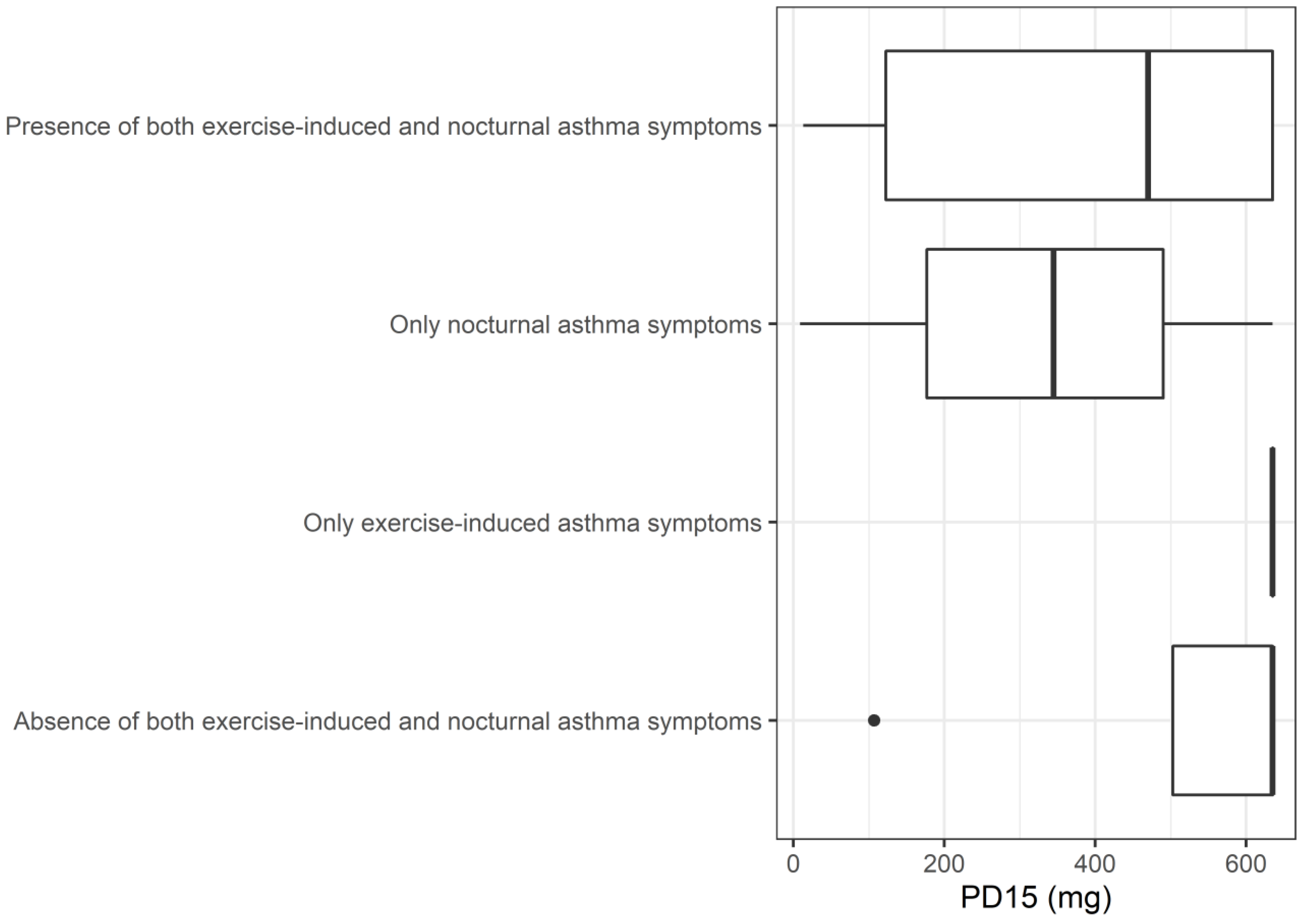
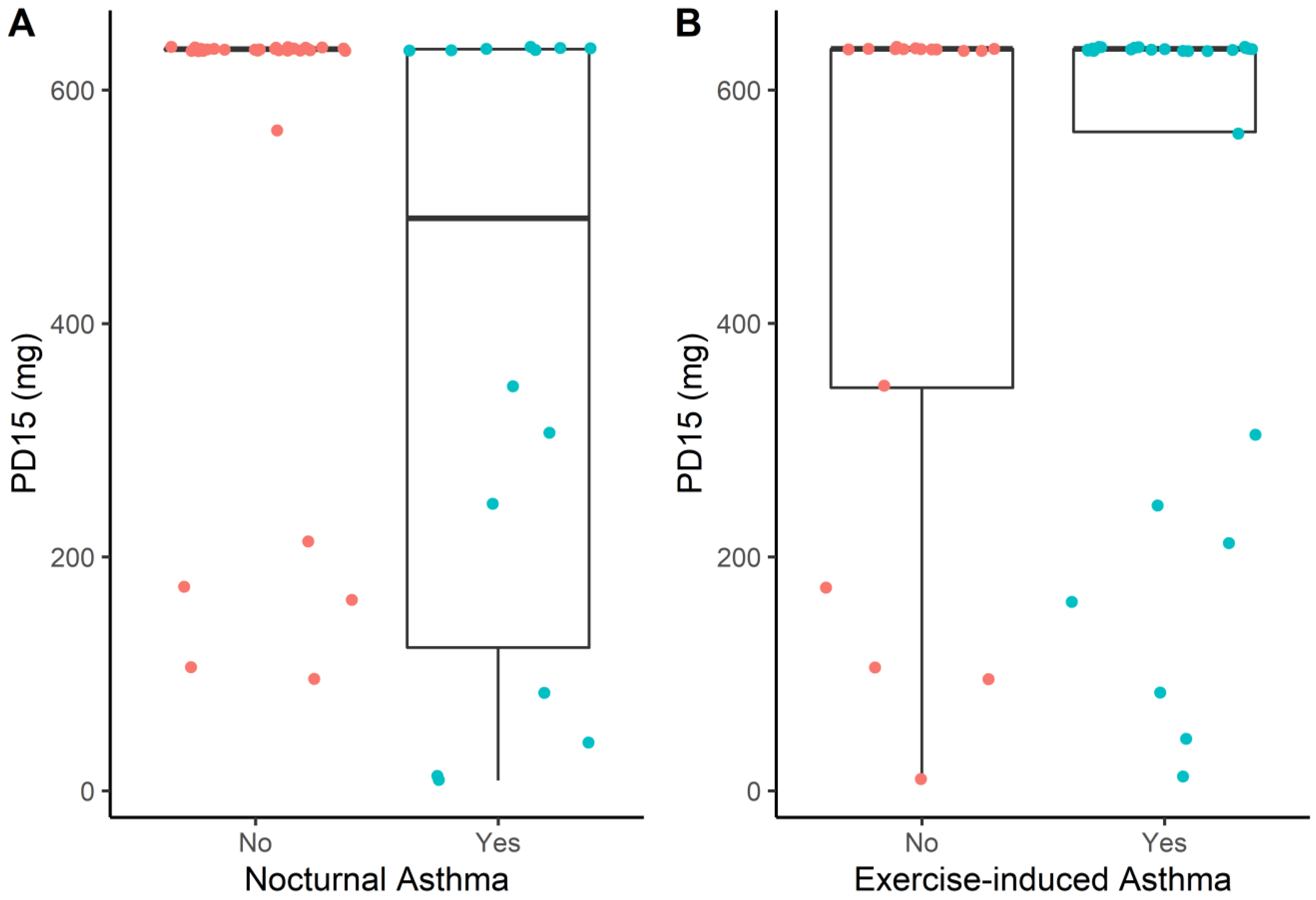
3.3. Associations between PD15 and Patient Characteristics
3.4. Safety, Tolerability and Adverse Events of the MDP Challenge
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferrante, G.; La Grutta, S. The Burden of Pediatric Asthma. Front. Pediatr. 2018, 6, 186. [Google Scholar] [CrossRef] [PubMed]
- Serebrisky, D.; Wiznia, A. Pediatric Asthma: A Global Epidemic. Ann. Glob. Health 2019, 85, 6. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. Available online: www.ginasthma.org (accessed on 23 February 2023).
- Banjari, M.; Kano, Y.; Almadani, S.; Basakran, A.; Al-Hindi, M.; Alahmadi, T. The Relation between Asthma Control and Quality of Life in Children. Int. J. Pediatr. 2018, 2018, 6517329. [Google Scholar] [CrossRef]
- Kaplan, A. The Myth of Mild: Severe Exacerbations in Mild Asthma: An Underappreciated, but Preventable Problem. Adv. Ther. 2021, 38, 1369–1381. [Google Scholar] [CrossRef]
- Busse, W.W.; Bateman, E.D.; Caplan, A.L.; Kelly, H.W.; O’Byrne, P.M.; Rabe, K.F.; Chinchilli, V.M. Combined Analysis of Asthma Safety Trials of Long-Acting β2-Agonists. N. Engl. J. Med. 2018, 378, 2497–2505. [Google Scholar] [CrossRef] [PubMed]
- Hopkin, J.M. The Diagnosis of Asthma, a Clinical Syndrome. Thorax 2012, 67, 660–662. [Google Scholar] [CrossRef]
- Martin, J.; Townshend, J.; Brodlie, M. Diagnosis and Management of Asthma in Children. BMJ Paediatr. Open 2022, 6, e001277. [Google Scholar] [CrossRef]
- Brannan, J.D.; Porsbjerg, C.; Anderson, S.D. Inhaled Mannitol as a Test for Bronchial Hyper-Responsiveness. Expert Rev. Respir. Med. 2009, 3, 457–468. [Google Scholar] [CrossRef]
- Leuppi, J.D. Bronchoprovocation Tests in Asthma. Curr. Opin. Pulm. Med. 2014, 20, 31–36. [Google Scholar] [CrossRef]
- Hallstrand, T.S.; Leuppi, J.D.; Joos, G.; Hall, G.L.; Carlsen, K.-H.; Kaminsky, D.A.; Coates, A.L.; Cockcroft, D.W.; Culver, B.H.; Diamant, Z.; et al. ERS Technical Standard on Bronchial Challenge Testing: Pathophysiology and Methodology of Indirect Airway Challenge Testing. Eur. Respir. J. 2018, 52, 1801033. [Google Scholar] [CrossRef]
- Sverrild, A.; Porsbjerg, C.; Backer, V. The Use of Inhaled Mannitol in the Diagnosis and Management of Asthma. Expert Opin. Pharmacother. 2012, 13, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Brannan, J.D.; Anderson, S.D.; Perry, C.P.; Freed-Martens, R.; Lassig, A.R.; Charlton, B. The Safety and Efficacy of Inhaled Dry Powder Mannitol as a Bronchial Provocation Test for Airway Hyperresponsiveness: A Phase 3 Comparison Study with Hypertonic (4.5%) Saline. Respir. Res. 2005, 6, 144. [Google Scholar] [CrossRef] [PubMed]
- Porsbjerg, C.; Sverrild, A.; Backer, V. The Usefulness of the Mannitol Challenge Test for Asthma. Expert Rev. Respir. Med. 2013, 7, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Knag Pedersen, S.; Ustrup, A.S.; Baarnes, C.B.; Suppli Ulrik, C. Usefulness of Mannitol Challenge Testing for Diagnosing Asthma in Everyday Clinical Practice. J. Asthma 2020, 57, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Attanasi, M.; Consilvio, N.P.; Rapino, D.; Nicola, M.D.; Scaparrotta, A.; Cingolani, A.; Petrosino, M.I.; Filippo, P.D.; Pillo, S.D.; Chiarelli, F. Bronchial Hyperresponsiveness to Mannitol, Airway Inflammation and Asthma Control Test in Atopic Asthmatic Children. Arch. Med. Sci. 2016, 1, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Brannan, J.D.; Kippelen, P. Bronchial Provocation Testing for the Identification of Exercise-Induced Bronchoconstriction. J. Allergy Clin. Immunol. Pract. 2020, 8, 2156–2164. [Google Scholar] [CrossRef]
- Kersten, E.T.G.; Driessen, J.M.M.; Duiverman, E.J.; Thio, B.J. The Effect of Stepping down Combination Therapy on Airway Hyperresponsiveness to Mannitol. Respir. Med. 2011, 105, 691–697. [Google Scholar] [CrossRef]
- Török, S.S.; Mueller, T.; Miedinger, D.; Jochmann, A.; Zellweger, L.J.; Sauter, S.; Goll, A.; Chhajed, P.N.; Taegtmeyer, A.B.; Knöpfli, B.; et al. An Open-Label Study Examining the Effect of Pharmacological Treatment on Mannitol- and Exercise-Induced Airway Hyperresponsiveness in Asthmatic Children and Adolescents with Exercise-Induced Bronchoconstriction. BMC Pediatr. 2014, 14, 196. [Google Scholar] [CrossRef]
- Anderson, S.D.; Brannan, J.; Spring, J.; Spalding, N.; Rodwell, L.T.; Chan, K.; Gonda, I.; Walsh, A.; Clark, A.R. A New Method For Bronchial-Provocation Testing in Asthmatic Subjects Using a Dry Powder of Mannitol. Am. J. Respir. Crit. Care Med. 1997, 156, 758–765. [Google Scholar] [CrossRef]
- Chan, B.K.C. Data Analysis Using R Programming. Adv. Exp. Med. Biol. 2018, 1082, 47–122. [Google Scholar] [CrossRef]
- Kersten, E.T.G.; Driessen, J.M.M.; van der Berg, J.D.; Thio, B.J. Mannitol and Exercise Challenge Tests in Asthmatic Children. Pediatr. Pulmonol. 2009, 44, 655–661. [Google Scholar] [CrossRef] [PubMed]
- Kharitonov, S.A.; Yates, D.H.; Barnes, P.J. Inhaled Glucocorticoids Decrease Nitric Oxide in Exhaled Air of Asthmatic Patients. Am. J. Respir. Crit. Care Med. 1996, 153, 454–457. [Google Scholar] [CrossRef]
- Lehtimäki, L.; Kankaanranta, H.; Saarelainen, S.; Turjanmaa, V.; Moilanen, E. Increased Alveolar Nitric Oxide Concentration in Asthmatic Patients with Nocturnal Symptoms. Eur. Respir. J. 2002, 20, 841–845. [Google Scholar] [CrossRef] [PubMed]
- Sverrild, A.; Porsbjerg, C.; Thomsen, S.F.; Backer, V. Airway Hyperresponsiveness to Mannitol and Methacholine and Exhaled Nitric Oxide: A Random-Sample Population Study. J. Allergy Clin. Immunol. 2010, 126, 952–958. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.A.; Park, H.B.; Kim, Y.H.; Sul, I.S.; Yoon, S.H.; Kim, H.R.; Kim, K.W.; Kim, K.-E.; Sohn, M.H. Airway Hyperresponsiveness to Mannitol and Methacholine and Exhaled Nitric Oxide in Children with Asthma. J. Asthma 2017, 54, 644–651. [Google Scholar] [CrossRef]
- Barben, J.; Kuehni, C.E.; Strippoli, M.-P.F.; Schiller, B.; Hammer, J.; Trachsel, D. Mannitol Dry Powder Challenge in Comparison with Exercise Testing in Children. Pediatr. Pulmonol. 2011, 46, 842–848. [Google Scholar] [CrossRef]
- Anderson, S.D.; Charlton, B.; Weiler, J.M.; Nichols, S.; Spector, S.L.; Pearlman, D.S. Comparison of Mannitol and Methacholine to Predict Exercise-Induced Bronchoconstriction and a Clinical Diagnosis of Asthma. Respir. Res. 2009, 10, 4. [Google Scholar] [CrossRef]
- Alblooshi, A.S.; Simpson, S.J.; Stick, S.M.; Hall, G.L. The Safety and Feasibility of the Inhaled Mannitol Challenge Test in Young Children. Eur. Respir. J. 2013, 42, 1420–1423. [Google Scholar] [CrossRef]
- Barben, J.; Roberts, M.; Chew, N.; Carlin, J.B.; Robertson, C.F. Repeatability of Bronchial Responsiveness to Mannitol Dry Powder in Children with Asthma. Pediatr. Pulmonol. 2003, 36, 490–494. [Google Scholar] [CrossRef]
- Decimo, F.; Capristo, C.; Amelio, R.; Maiello, N.; Capristo, A.F.; Del Giudice, M.M. Evaluation of Bronchial Hyperreactivity with Mannitol Dry Powder Challenge Test in a Paediatric Population with Intermittent Allergic Asthma or Allergic Rhinitis. Int. J. Immunopathol. Pharmacol. 2011, 24, 1069–1074. [Google Scholar] [CrossRef]
- Subbarao, P.; Brannan, J.D.; Ho, B.; Anderson, S.D.; Chan, H.K.; Coates, A.L. Inhaled Mannitol Identifies Methacholine-Responsive Children with Active Asthma. Pediatr. Pulmonol. 2000, 29, 291–298. [Google Scholar] [CrossRef]
- Świebocka, E.M.; Siergiejko, G.; Siergiejko, Z. Mannitol Challenge Does Not Confirm Bronchial Hyperreactivity in Some Histamine-Responsive Asthmatic Children. J. Asthma 2012, 49, 817–821. [Google Scholar] [CrossRef] [PubMed]
- Holzer, K.; Anderson, S.D.; Chan, H.-K.; Douglass, J. Mannitol as a Challenge Test to Identify Exercise-Induced Bronchoconstriction in Elite Athletes. Am. J. Respir. Crit. Care Med. 2003, 167, 534–537. [Google Scholar] [CrossRef] [PubMed]
- Sue-Chu, M.; Brannan, J.D.; Anderson, S.D.; Chew, N.; Bjermer, L. Airway Hyperresponsiveness to Methacholine, Adenosine 5-Monophosphate, Mannitol, Eucapnic Voluntary Hyperpnoea and Field Exercise Challenge in Elite Cross-Country Skiers. Br. J. Sports Med. 2010, 44, 827–832. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean (SD) | |
|---|---|
| Age (years) | 9.98 (2.10) |
| Height (cm) | 143.26 (12.44) |
| Weight (kg) | 42.22 (13.33) * |
| BMI Z-score | 1.25 (1.46) |
| FEV1 (% predicted) | 110.66 (19.15) |
| N (%) | |
| Sex (Male) | 16 (69.57) |
| Exercise-induced asthma symptoms | 16 (69.57) |
| Nocturnal asthma symptoms | 13 (56.52) |
| Prophylactic treatment-naive | 23 (100.00) |
| Initiated asthma prophylaxis | |
| ICS | 2 (8.70) |
| ICS + LABA | 21 (91.30) |
| Pre-Treatment | Post-Treatment | Difference (95% CI) | p-Value | |
|---|---|---|---|---|
| PD15 (mg) * | 635.00 (259.25–635.00) | 635.00 (635.00–635.00) | 228.50 (4.50, 458.15) | 0.04 |
| RDR (mg/mL) | 1.70 (0.50–3.20) | 0.70 (0.30–0.90) | −1.22 (−2.85, −0.20) | 0.02 |
| FEV1 (% predicted) | 113.93 (17.10) | 107.14 (12.56) | −6.01 (−15.50, 3.48) | 0.20 |
| Exercise-induced asthma symptoms | 16 (69.57) | 13 (56.52) | 0.26 | |
| Nocturnal asthma symptoms | 13 (56.52) | 1 (4.35) | <0.01 | |
| Completed mannitol challenge | 16 (69.57) | 20 (86.96) | 0.16 | |
| Positive mannitol challenge ** | 8 (34.78) | 5 (21.74) | 0.18 |
| Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|
| Independent Variable | Coefficient (95% CI) | p | Coefficient (95% CI) | p | |
| Pre-treatment (adj. R2 = 0.41) | BMI-for-age (Z-score) | 89.92 (23.62 to 156.21) | 0.01 | 92.10 (33.61 to 150.59) | <0.01 |
| Nocturnal Asthma (Yes) | −209.05 (−412.91 to −5.20) | 0.04 | −216.78 (−385.73 to −47.83) | 0.01 | |
| Exercise-induced Asthma (Yes) | 50.84 (−190.30 to 291.99) | 0.67 | Not included * | ||
| FEV1 (% predicted) | −2.26 (−8.84 to 4.32) | 0.48 | Not included * | ||
| Post-treatment (adj. R2 = 0.22) | BMI-for-age (Z-score) | 63.91 (14.98 to 112.85) | 0.01 | 63.91 (14.98 to 112.85) | 0.01 |
| Nocturnal Asthma (Yes) | 89.32 (−308.01 to 486.64) | 0.64 | Not included * | ||
| Exercise-induced Asthma (Yes) | 25.42 (−138.48 to 189.31) | 0.75 | Not included * | ||
| FEV1 (% predicted) | −0.18 (−7.82 to 7.47) | 0.96 | Not included * | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karantaglis, N.; Kirvassilis, F.; Hatziagorou, E.; Gkantaras, A.; Kontouli, K.; Tsanakas, J.; Emporiadou, M. Mannitol Challenge to Assess Therapy Response in Asthmatic Children: An Interventional Cohort Study. Children 2023, 10, 802. https://doi.org/10.3390/children10050802
Karantaglis N, Kirvassilis F, Hatziagorou E, Gkantaras A, Kontouli K, Tsanakas J, Emporiadou M. Mannitol Challenge to Assess Therapy Response in Asthmatic Children: An Interventional Cohort Study. Children. 2023; 10(5):802. https://doi.org/10.3390/children10050802
Chicago/Turabian StyleKarantaglis, Nikolaos, Fotios Kirvassilis, Elpis Hatziagorou, Antonios Gkantaras, Kalliopi Kontouli, John Tsanakas, and Maria Emporiadou. 2023. "Mannitol Challenge to Assess Therapy Response in Asthmatic Children: An Interventional Cohort Study" Children 10, no. 5: 802. https://doi.org/10.3390/children10050802