Muscle Wasting among Hospitalized Children: A Narrative Review of the Feasibility and Accuracy of Diagnostic Methods

Abstract
:1. Introduction
- RQ1: What currently available evidence supports diagnostic methods, especially handgrip strength, in detecting muscle wasting among hospitalized children?
- RQ2: How feasible is it to use diagnostic methods, especially handgrip strength, to assess muscle wasting among hospitalized children?
- RQ3: What is the precision of diagnostic methods, especially handgrip strength, in detecting muscle wasting among hospitalized children?
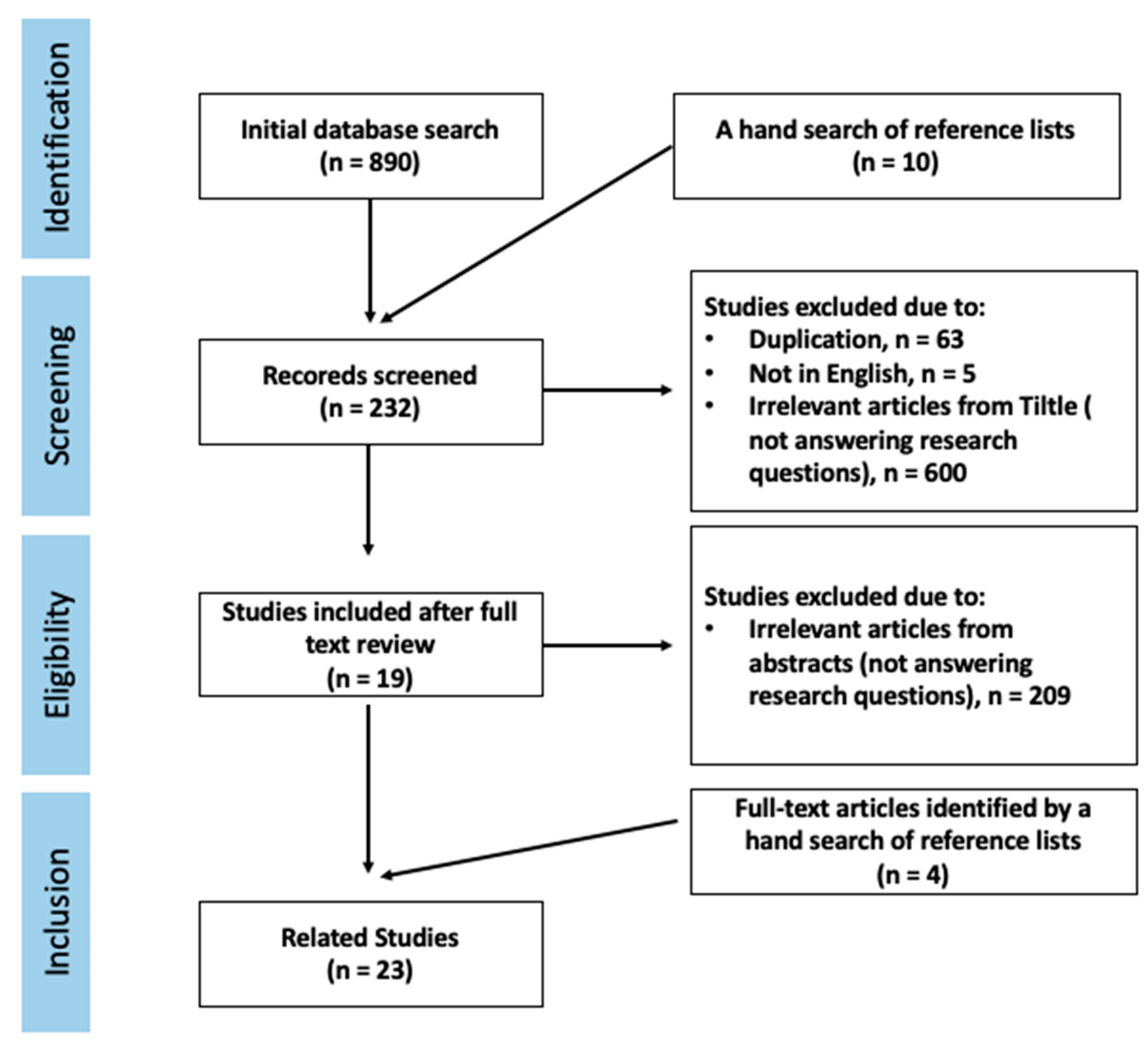
2. Materials and Methods
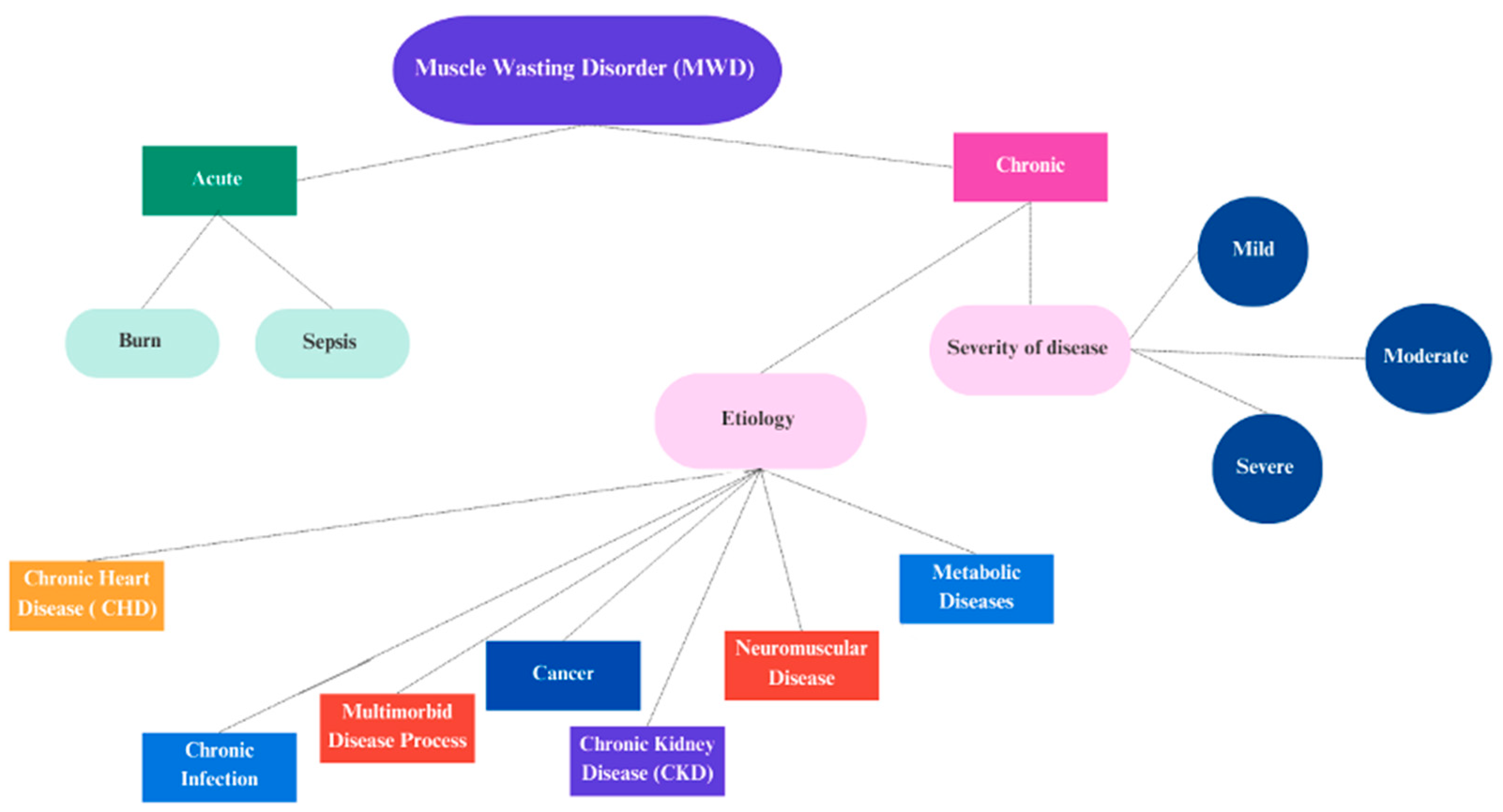
3. Diagnostic Methods to Detect Muscle-Wasting Disorder (MWD)
4. Feasibility and Accuracy of HGS in Detection MWD among Children
5. Feasibility and Accuracy of HGS in Detection MWD among Hospitalized Children
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- SCWD. Muscle Wasting. Society of Sarcopenia, Cachexia and Wasting Disorders 2022. Available online: https://society-scwd.org/muscle-wasting/ (accessed on 17 October 2022).
- Blakeley, C.E.; Van Rompay, M.I.; Schultz, N.S.; Sacheck, J.M. Relationship between muscle strength and dyslipidemia, serum 25(OH)D, and weight status among diverse schoolchildren: A cross-sectional analysis. BMC Pediatr. 2018, 18, 23. [Google Scholar] [CrossRef]
- Murphy, M.J.; Metcalf, B.S.; Jeffery, A.N.; Voss, L.D.; Wilkin, T.J. Does lean rather than fat mass provide the link between birth weight, BMI, and metabolic risk? EarlyBird 23. Pediatr. Diabetes 2006, 7, 211–214. [Google Scholar] [CrossRef]
- Kim, J.H.; Park, Y.S. Low muscle mass is associated with metabolic syndrome in Korean adolescents: The Korea National Health and Nutrition Examination Survey 2009–2011. Nutr. Res. 2016, 36, 1423–1428. [Google Scholar] [CrossRef]
- Peterson, M.D.; Zhang, P.; Saltarelli, W.A.; Visich, P.S.; Gordon, P.M. Low Muscle Strength Thresholds for the Detection of Cardiometabolic Risk in Adolescents. Am. J. Prev. Med. 2016, 50, 593–599. [Google Scholar] [CrossRef]
- Kim, S.; Valdez, R. Metabolic risk factors in U.S. youth with low relative muscle mass. Obes. Res. Clin. Pract. 2016, 9, 125–132. [Google Scholar] [CrossRef]
- Hulst, J.M.; van Goudoever, J.B.; Zimmermann, L.J.; Hop, W.C.; Albers, M.J.; Tibboel, D.; Joosten, K.F. The effect of cumulative energy and protein deficiency on anthropometric parameters in a pediatric ICU population. Clin. Nutr. 2004, 23, 1381–1389. [Google Scholar] [CrossRef]
- Banwell, B.L.; Mildner, R.J.; Hassall, A.C.; Becker, L.E.; Vajsar, J.; Shemie, S.D. Muscle weakness in critically ill children. Neurology 2003, 61, 1779–1782. [Google Scholar] [CrossRef]
- National Cancer Institute. Muscle Wasting. 2022. Available online: https://www.cancer.gov (accessed on 15 November 2022).
- WHO. Multicentre Growth Reference Study Group: WHO Child Growth Standards: Length/ Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; World Health Organization: Geneva, Switerland, 2006. [Google Scholar]
- WHO. Child Growth Standards. Arm Circumference for Age. Available online: http://www.who.int/childgrowth/standards/ac_for_age/en/index.html (accessed on 15 November 2022).
- Tostes, N.F.; Saraiva, D.D.C.A.; Martucci, R.B. Association between nutritional status and muscle strength in pediatric cancer patients. Clin. Nutr. ESPEN 2021, 43, 436–441. [Google Scholar] [CrossRef]
- Ooi, P.H.; Thompson-Hodgetts, S.; Pritchard-Wiart, L.; Gilmour, S.M.; Mager, D.R. Pediatric sarcopenia: A paradigm in the overall definition of malnutrition in children? J. Parenter. Enter. Nutr. 2020, 44, 407–418. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis.Report of the European Working Group on Sarcopenia in Older PeopleA. J. Cruz-Gentoft et al. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- Barbat-Artigas, S.; Rolland, Y.; Zamboni, M.; Aubertin-Leheudre, M. How to assess functional status: A new muscle quality index. J. Nutr. Health Aging 2012, 16, 67–77. [Google Scholar] [CrossRef]
- Anker, S.D.; Coats, A.J.; Morley, J.E.; Rosano, G.; Bernabei, R.; von Haehling, S.; Kalantar-Zadeh, K. Muscle wasting disease: A proposal for a new disease classification. J. Cachexia Sarcopenia Muscle 2014, 5, 1–3. [Google Scholar] [CrossRef]
- Pillen, S. Skeletal muscle ultrasound. Eur. J. Transl. Myol. 2010, 20, 145–156. [Google Scholar] [CrossRef]
- Pennati, F.; Arrigoni, F.; LoMauro, A.; Gandossini, S.; Russo, A.; D’Angelo, M.G.; Aliverti, A. Diaphragm involvement in Duchenne muscular dystrophy (DMD): An MRI study. J. Magn. Reson. Imaging 2020, 51, 461–471. [Google Scholar] [CrossRef]
- IJpma, I.; Lequin, M.H.; Nievelstein, R.A.; Fiocco, M.; Tissing, W.J. Body composition of patients with neuroblastoma using computed tomography. Pediatr. Blood Cancer 2021, 68, 29–37. [Google Scholar] [CrossRef]
- Kim, J.; Shen, W.; Gallagher, D.; Jones, A., Jr.; Wang, Z.; Wang, J.; Heshka, S.; Heymsfield, S.B. Total-body skeletal muscle mass: Estimation by dual-energy X-ray absorptiometry in children and adolescents. Am. J. Clin. Nutr. 2006, 84, 1014–1020. [Google Scholar] [CrossRef]
- Kushner, R.F. Bioelectrical impedance analysis: A review of principles and applications. J. Am. Coll. Nutr. 1992, 11, 199–209. [Google Scholar] [CrossRef]
- Casadei, K.; Kiel, J. Anthropometric Measurement; StatPearls Publishing: Treasure Island, FL, USA, 2019; Available online: https://europepmc.org/article/nbk/nbk537315 (accessed on 17 October 2022).
- Silva, C.; Amaral, T.F.; Silva, D.; Oliveira, B.M.; Guerra, A. Handgrip strength and nutrition status in hospitalized pediatric patients. Nutr. Clin. Pract. 2014, 29, 380–385. [Google Scholar] [CrossRef]
- Toledo, D.O.; Silva, D.C.D.L.; Santos, D.M.D.; Freitas, B.J.D.; Dib, R.; Cordioli, R.L.; Figueiredo, E.J.D.A.; Piovacari, S.M.F.; Silva, J.M. Ultrassom à beira do leito como ferramenta prática para avaliação da massa muscular. Rev. Bras. Ter. Intensiv. 2017, 29, 476–480. [Google Scholar] [CrossRef]
- Tillquist, M.; Kutsogiannis, D.J.; Wischmeyer, P.E.; Kummerlen, C.; Leung, R.; Stollery, D.; Karvellas, C.J.; Preiser, J.C.; Bird, N.; Kozar, R.; et al. Bedside ultrasound is a practical and reliable measurement tool for assessing quadriceps muscle layer thickness. J. Parenter. Enter. Nutr. 2014, 38, 886–890. [Google Scholar] [CrossRef]
- Bertini, G.; Elia, S.; Dani, C. Using ultrasound to examine muscle mass in preterm infants at term-equivalent age. Eur. J. Pediatr. 2021, 180, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Pitcher, C.A.; Elliott, C.M.; Panizzolo, F.A.; Valentine, J.P.; Stannage, K.; Reid, S.L. Ultrasound characterization of medial gastrocnemius tissue composition in children with spastic cerebral palsy. Muscle Nerve 2015, 52, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.; Lee, J.H.; Leow, M.K.; Puthucheary, Z.A. Skeletal muscle ultrasonography in nutrition and functional outcome assessment of critically ill children: Experience and insights from pediatric disease and adult critical care studies. J. Parenter. Enter. Nutr. 2017, 41, 1091–1099. [Google Scholar] [CrossRef] [PubMed]
- Lecouvet, F.E. Whole-body MR imaging: Musculoskeletal applications. Radiology 2016, 279, 345–365. [Google Scholar] [CrossRef]
- RSNA. Pediatric MRI. Radiological Society of North America. 2022. Available online: https://www.radiologyinfo.org/en/info/pediatric-mri (accessed on 17 October 2022).
- Chavhan, G.B.; Babyn, P.S. Whole-body MR imaging in children: Principles, technique, current applications, and future directions. Radiographics 2011, 31, 1757–1772. [Google Scholar] [CrossRef]
- Eutsler, E.P.; Khanna, G. Whole-body magnetic resonance imaging in children: Technique and clinical applications. Pediatr. Radiol. 2016, 46, 858–872. [Google Scholar] [CrossRef]
- Yodoshi, T.; Orkin, S.; Clachar, A.C.A.; Bramlage, K.; Sun, Q.; Fei, L.; Beck, A.F.; Xanthakos, S.A.; Trout, A.T.; Mouzaki, M. Muscle mass is linked to liver disease severity in pediatric nonalcoholic fatty liver disease. J. Pediatr. 2020, 223, 93–99. [Google Scholar] [CrossRef]
- RSNA. Pediatric CT. Radiological Society of North America. 2021. Available online: https://www.radiologyinfo.org/en/info/pedia-ct (accessed on 17 October 2022).
- Prado, C.M.; Birdsell, L.A.; Baracos, V.E. The emerging role of computerized tomography in assessing cancer cachexia. Curr. Opin. Support. Palliat. Care 2009, 3, 269–275. [Google Scholar] [CrossRef]
- Yip, C.; Dinkel, C.; Mahajan, A.; Siddique, M.; Cook, G.J.; Goh, V. Imaging body composition in cancer patients: Visceral obesity, sarcopenia and sarcopenic obesity may impact on clinical outcome. Insights Imaging 2015, 6, 489–497. [Google Scholar] [CrossRef]
- RSNA. Bone Density Scan (DEXA or DXA). Radiological Society of North America. 2022. Available online: https://www.radiologyinfo.org/en/info/dexa (accessed on 17 October 2022).
- Heymsfield, S.B.; Smith, R.; Aulet, M.; Bensen, B.; Lichtman, S.; Wang, J.P.R.J.; Pierson, R.N., Jr. Appendicular skeletal muscle mass: Measurement by dual-photon absorptiometry. Am. J. Clin. Nutr. 1990, 52, 214–218. [Google Scholar] [CrossRef]
- Tavoian, D.; Ampomah, K.; Amano, S.; Law, T.D.; Clark, B.C. Changes in DXA-derived lean mass and MRI-derived cross-sectional area of the thigh are modestly associated. Sci. Rep. 2019, 9, 10028. [Google Scholar] [CrossRef] [PubMed]
- Earthman, C.P. Body composition tools for assessment of adult malnutrition at the bedside: A tutorial on research considerations and clinical applications. J. Parenter. Enter. Nutr. 2015, 39, 787–822. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gomez, J.M. ESPEN guidelines for the use of BIA measurements-part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Fors, H.; Gelander, L.; Bjarnason, R.; Albertsson-Wikland, K.; Bosaeus, I. Body composition, as assessed by bioelectrical impedance spectroscopy and dual-energy X-ray absorptiometry, in a healthy paediatric population. Acta Paediatr. 2002, 91, 755–760. [Google Scholar] [CrossRef]
- Poortmans, J.R.; Boisseau, N.; Moraine, J.J.; Moreno-Reyes, R.; Goldman, S. Estimation of total-body skeletal muscle mass in children and adolescents. Med. Sci. Sport. Exerc. 2005, 37, 316–322. [Google Scholar] [CrossRef]
- Mendoza, M.; Miller, R.G. Muscle Strength, Assessment. In Encyclopedia of the Neurological Sciences; Academic Press: Cambridge, MA, USA, 2003; pp. 279–285. [Google Scholar] [CrossRef]
- Kolber, M.J.; Cleland, J.A. Strength testing using hand-held dynamometry. Phys. Ther. Rev. 2005, 10, 99–112. [Google Scholar] [CrossRef]
- Hebert, L.J.; Remec, J.F.; Saulnier, J.; Vial, C.; Puymirat, J. The use of muscle strength assessed with handheld dynamometers as a non-invasive biological marker in myotonic dystrophy type 1 patients: A multicenter study. BMC Musculoskelet. Disord. 2010, 11, 72. [Google Scholar] [CrossRef]
- Mathiowetz, V. Comparison of Rolyan and Jamar dynamometers for measuring grip strength. Occup. Ther. Int. 2002, 9, 201–209. [Google Scholar] [CrossRef]
- Buck, R.; Lambert, M.I. Getting a Grip on Strength Measurement in Children (6–13 Y): Impact of Typical Error of Measurement. Pediatr. Exerc. Sci. 2022, 34, 141–147. [Google Scholar] [CrossRef]
- Svensson, E.; Waling, K.; Hager-Ross, C. Grip strength in children: Test–retest reliability using Grippit. Acta Paediatr. 2008, 97, 1226–1231. [Google Scholar] [CrossRef]
- Gasior, J.S.; Pawłowski, M.; Jelen, P.J.; Rameckers, E.A.; Williams, C.A.; Makuch, R.; Werner, B. Test–retest reliability of handgrip strength measurement in children and preadolescents. Int. J. Environ. Res. Public Health 2020, 17, 8026. [Google Scholar] [CrossRef] [PubMed]
- Mckirdy, S.; Nichols, B.; Williamson, S.; Gerasimidis, K. Handgrip strength as a surrogate marker of lean mass and risk of malnutrition in paediatric patients. Clin. Nutr. 2021, 40, 5189–5195. [Google Scholar] [CrossRef] [PubMed]
- Jensen, K.C.; Bellini, S.G.; Derrick, J.W.; Fullmer, S.; Eggett, D. Handgrip strength and malnutrition (undernutrition) in hospitalized versus nonhospitalized children aged 6–14 years. Nutr. Clin. Pract. 2017, 32, 687–693. [Google Scholar] [CrossRef]
- Gibson, H.T.; McDonald, C.M.; Derrick, J.W.; Eggett, D.L.; Bellini, S.G. Evaluating Changes in Handgrip Strength in Children With Cystic Fibrosis: A Pilot Study. Nutr. Clin. Pract. 2018, 33, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Bulut, N.; Gurbuz, I.; Yilmaz, O.; Aydin, G.; Karaduman, A. The association of hand grip strength with functional measures in non-ambulatory children with Duchenne muscular dystrophy. Arq. Neuro-Psiquiatr. 2019, 77, 792–796. [Google Scholar] [CrossRef]
- Iyob-Tessema, H.; Wang, C.S.; Kennedy, S.; Reyes, L.; Shin, S.; Greenbaum, L.A.; Hogan, J. Grip Strength in Adults and Children with Cystinosis. Kidney Int. Rep. 2021, 6, 389–395. [Google Scholar] [CrossRef]
- Bouma, S.; Peterson, M.; Gatza, E.; Choi, S.W. Nutritional status and weakness following pediatric hematopoietic cell transplantation. Pediatr. Transplant. 2016, 20, 1125–1131. [Google Scholar] [CrossRef]
- Bouma, S.F.; Iwanicki, C.; McCaffery, H.; Nasr, S.Z. The association of grip strength, body mass index, and lung function in youth with cystic fibrosis. Nutr. Clin. Pract. 2020, 35, 1110–1118. [Google Scholar] [CrossRef]
- Hogrel, J.Y.; Decostre, V.; Ledoux, I.; de Antonio, M.; Niks, E.H.; de Groot, I.; Straub, V.; Muntoni, F.; Ricotti, V.; Voit, T.; et al. Normalized grip strength is a sensitive outcome measure through all stages of Duchenne muscular dystrophy. J. Neurol. 2020, 267, 2022–2028. [Google Scholar] [CrossRef]
- Hogan, J.; Schneider, M.F.; Pai, R.; Denburg, M.R.; Kogon, A.; Brooks, E.R.; Kaskel, F.J.; Reidy, K.J.; Saland, J.M.; Warady, B.A.; et al. Grip strength in children with chronic kidney disease. Pediatr. Nephrol. 2020, 35, 891–899. [Google Scholar] [CrossRef]
- Abd El Basset Bakr, A.M.; Hasaneen, B.M.; Bassiouni, D.A.H. Assessment of Nutritional Status in Children with Chronic Kidney Disease Using Hand Grip Strength Tool. J. Ren. Nutr. 2018, 28, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.D.; Gordon, P.M.; Smeding, S.; Visich, P. Grip strength is associated with longitudinal health maintenance and improvement in adolescents. J. Pediatr. 2018, 202, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Bellini, S.G.; Chapman, P.; Szendre, K.; McDonald, C.; Williams, N.; Hopkin, L.; Eggett, D.; Dean, A. Changes in handgrip strength in children with cystic fibrosis compared to children without cystic fibrosis. Clin. Nutr. ESPEN 2021, 42, 206–211. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Definition | Advantage | Disadvantage | |
|---|---|---|---|
| Muscle Mass | |||
| Ultrasonography | A noninvasive and real-time tool for visualizing normal and diseased muscle tissue. | No radiation exposure or sedation, cost-effective, easily applicable, and safe. | Ultrasound equipment required. Restricted for some subjects with fluid–electrolyte imbalance. |
| Magnetic resonance imaging (MRI) | A noninvasive technique for identifying the muscle-wasting disorder. Provides precise images of internal body structures. | The gold standard, no radiation, precise, and accurate. | Cost-restricted, equipment required, may require sedation. |
| Computed tomography (CT) | Generates several images or images of the interior of the body including muscle mass | The gold standard, precise, accurate. | Cost-restricted, equipment required, radiation, may require sedation. |
| Dual-energy X-ray (DXA) | Produces images of the inside of the body, often the hips and lower body. Estimates skeletal muscle. | Simple, quick, no anesthesia required given a total amount of skeletal muscle. | May require sedation, and the radiation dose for this procedure varies; not able to directly measure the amount of skeletal muscle. |
| Bioelectrical impedance analysis (BIA) | Allows the determination of the fat-free mass and total body water in subjects without significant fluid and electrolyte abnormalities. | Simple, quick, cost-effective, no sedation required, safe. | Restricted for some subjects with fluid–electrolyte imbalance, equipment required, underestimates fat mass, and overestimates fat-free mass. |
| Anthropometry | Noninvasive method. Elements of anthropometry are height, weight, head circumference, body mass index (BMI), body circumferences to assess for adiposity (waist, hip, and limbs), and skinfold thickness. | Quantitative measurements, simple, and quick. | Restricted for some subjects with fluid–electrolyte imbalance |
| Muscle Strength | |||
| Handheld dynamometer (HHD) | A small portable device can be used to test both proximal and distal muscles in all extremities. | An efficient, objective, quick, easy, affordable alternative for strength quantitation. | May be difficult when testing large muscles or muscle groups in the lower extremities, sensitive. |
| Study | Study Design | Population | Sample Size | Age, Year | Control Group and Sample Size | Body Composition/Methodology | Clinical Outcome | |
|---|---|---|---|---|---|---|---|---|
| Muscle Mass | ||||||||
| Ultrasonography | [26] | Prospective, observational | Preterm infants | N = 44 | Term-equivalent age | Healthy full-term infants, N = 44 | Examined the muscle thickness and subcutaneous fat thickness in three different muscles and muscle groups: two proximal (biceps brachii and quadriceps femoris) and one distal (anterior tibial). |
|
| [27] | Case–control | SCP | N = 40 | Ages 4–14 years | TD children | Ultrasound scans were taken of the medial gastrocnemius. |
| |
| MRI | [18] | Cross-sectional | DMD | N = 26 | Ages 6–32 years | N = 12 | Spirometry was performed in DMD patients on the same day as MRI. Patients and controls were scanned with a 3-time MRI system. |
|
| [33] | Retrospective cohorts | NAFLD | N = 100 | Age < 20 years | MRI evidence of hepatic steatosis, N = 236. | Muscle mass was estimated in all patients by measuring MRI-based tPMSA and correcting for height (tPMSA index = tPMSA/height2). |
| |
| CT | [19] | Retrospective | Neuroblastoma | N = 29 | Ages 0–18 years | N/A | Cross-sectional areas of skeletal muscle, IMAT, VAT, SAT, and skeletal muscle density at the level of the third lumbar vertebra were examined. |
|
| DXA | [20] | Retrospective | Varied in the pubertal maturation stage. | N = 99 | Ages 5–17 years | SM estimated using whole-body MRI was used as the reference. The adult SM model was not accurate for subjects below Tanner stage 5 (N = 65; ages 5–14 years). New pediatric SM prediction models were therefore developed and validated in a separate group (N = 18). |
| |
| BIA | [42] | Tool evaluation | Healthy children | N = 61 | Ages 8–11 years | N/A | Level of agreement between body composition measurements using DXA, BIA, and multifrequency BIS. FFM, body fat mass, and body fatness (percentage fat) were measured using DXA, BIA, and BIS. |
|
| Anthropometry | [43] | Cross-sectional | Healthy, nonobese subjects | N = 39 | Ages 7–16 years | N = 20 adults ages 20–24 years | Total-body SM was assessed using DXA and UCrn determination and anthropometric measurements of weight, height, skinfold thickness, and circumference measurements of the mid-upper arm, mid-thigh, and mid-calf. |
|
| Study | Study Design | Population | Age, Year | Sample Size | Control Group and Sample Size | Body Composition Methodology | Definition of Malnutrition/Muscle Wasting | Clinical Outcome |
|---|---|---|---|---|---|---|---|---|
| [49] | Test–retest study | Healthy children | 6-, 10-, and 14-year-olds | N = 58 | Compared reliability for 3 groups: N = 19 (6 years), N = 20 (10 years), N = 19 (14 years). | HGS | Test–retest reliability | HGS ↑ More reliable in 6- and 14-year-olds than 10-year-olds. ↑ Reliability was good for both peak and sustained grip strength. |
| [61] | 2-year longitudinal cohort study | Students | Age = 9.2 years: 54% female; 83% white) | N = 474 | N/A | HGS, BMI, CVD health | HGS, BMI | Low HGS had a significant association with a high prevalence of health decline or poor health persistence. Adolescents who were strong had odds for health maintenance (OR 3.54; 95% CI 1.80–6.97) and health improvement (OR 1.30; 95% CI 1.05–1.60), even after adjustment for baseline fat-free mass index, cardiorespiratory fitness, and objectively measured physical activity. |
| [50] | Test–retest study | Healthy children | Ages 7–13 years | N = 338 | Divided into two groups based on age: children (7–9 years old) and preadolescents (10–13 years old). | HGS | Test–retest reliability | Childhood age influences the difference between the test and retest of the HGS measurement. ↓ HGS measurement using a digital handgrip dynamometer is less reliable among preadolescents than children. |
| [48] | Evaluation tools study | Healthy | Ages 6–13 years | N = 290 | N/A | TE, coefficient of variation, and SWC were calculated. | HGS testing protocol 3 times within a 7-day period. | Changes in HGS were greater than in the TE and SWC, which can be considered real changes of practical significance. |
| [51] | Retrospective cohort | SC | ages 5–16 years | N = 595 [53] | HC, N = 535 for the development of HGS centile charts | HGS z-scores for age | Using PYMS score | High PYMS scores were significantly associated with low HGS z-scores for age. HGS z-scores were significantly inversely related to plasma CRP. |
| [52] | Cross-sectional nonequivalent control group design study | Hospitalized patients | Ages 6–14 years | N = 109 | Nonhospitalized patients = 110 | BMI, MUAC, and HGS z-scores | Nutrition screening tool | HGS did not differ significantly between hospitalized and nonhospitalized. A significant association between HGS and age and height, and a nonsignificant association with MUAC. |
| [23] | Longitudinal cohort study | Hospitalized patients | ≥6 years | N = 89 | On admission vs. on discharge | HGS | BMI z-scores | ↓ HGS marker of undernutrition |
| [53] | Longitudinal pilot study | Children with CF | Ages 6–18 years | N = 23 | 5 months pre-hospitalization, 5–7 days post-hospitalization, and 6 weeks during hospitalization | HGS z-scores and arm anthropometrics | Nutrition screening tool and BMI z-scores | No significant relationship was observed between HGS and nutrition status (BMI z-scores and nutrition risk scores). HGS z-scores at hospitalization were much lower than the standard even though mean BMI z-scores classified participants as having normal nutrition status. |
| [57] | Cohort study | Medically stable youth with CF | Ages 6–21 years | N = 201 | HGS reference tables were created by merging data from the NHANES 2011–2012 and 2013–2014 survey cycles, resulting in HGS measurements from 4672 individuals, ages 6–19 years. | HGS, BMI, body composition (lean body mass and fat-free mass) | HGS and BMI | HGS is reliable, less expensive, and clinically feasible for body composition measurements in monitoring nutrition status. |
| [62] | Prospective longitudinal study | Children with CF | Ages 6–18 years | N = 75 | Non-CF group (N= 76) | MUAC, tricep skinfold, and HGS | Nutrition screening tool | The rate of change in HGS z-scores in both groups was not significant (p = 0.15). HGS z-scores significantly decreased over time in children with CFRD versus children without CFRD. |
| [56] | Descriptive cross-sectional study | Pediatric HCT | Ages 2–25 years | N = 36 | HGS, nutrition-focused physical examination, and online food and activity surveys | BMI, nutrition-focused physical examination, divided into undernutrition, normal, and overnutrition groups | ↓ HGS measurements in the undernutrition group was significantly more than those in the normal and overnutrition groups. Comprehensive nutritional assessments and HGS measurements are feasible, noninvasive, easy to perform, and inform both under- and overnutrition in pediatric HCT survivors. | |
| [54] | Cross-sectional study | DMD in children | Ages 5–18 years | N = 38 | N/A | HGS, the Turkish version of EK2 for global functional capacity, PUL for upper limb functional performance and the ABILHAND-Kids for hand ability. | Accuracy | HGS was found to be correlated with the EK2 (p < 0.05). HGS may be used in clinical practice as a practical assessment tool to gain immediate insight into the global functional capacity of nonambulatory DMD children. |
| [58] | Cohort | DMD patients | Ages 5.0–28.7 years | N = 202 | 92 patients were ambulatory and 110 were nonambulatory | Test–retest reliability of HGS measurements, MyoGrip device | HGS | HGS in ambulatory patients was higher than in nonambulatory patients. |
| [55] | Cohort | Pt with CKD with cystinosis | All patients > 6 years of age including adults | N = 76 | Healthy control subjects, similar CKD stage without cystinosis. | HGS z-score, eGFR | HGS z-score | No significant correlation was observed between eGFR and grip strength z-score. CKD with cystinosis exhibited a mean HGS z-score of −2.1 (SD, 1.1), which is lower ↓ than that found in patients with CKD without cystinosis. |
| [59] | Prospective cohort | Pt with CKD | 1 to 16 years | N = 411 | Healthy control subjects | HGS z-score, eGFR | HGS z-score | HGS z-score among CKD patients with CKD stages 2 through 5 was significantly lower than ↓ HGS z-scores for CKD stage 1. Compared with healthy controls, CKD participants had a ↓ Lower HGS z-score |
| [12] | A cross-sectional study | Cancer patients | Ages 6–19 years | N = 63 | The sample was stratified by age group: 6–9 years, 10–14 years, and 15–19 years. | Anthropometric (body weight, height, MUAC, and TSF), BMI, MAMC, and HGS | Anthropometric (body weight, height, MUAC, and TSF), BMI, MAMC, and HGS | A strong positive correlation was observed between HGS and MAMC and weight. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlQahtani, S.; Aldisi, D. Muscle Wasting among Hospitalized Children: A Narrative Review of the Feasibility and Accuracy of Diagnostic Methods. Children 2023, 10, 795. https://doi.org/10.3390/children10050795
AlQahtani S, Aldisi D. Muscle Wasting among Hospitalized Children: A Narrative Review of the Feasibility and Accuracy of Diagnostic Methods. Children. 2023; 10(5):795. https://doi.org/10.3390/children10050795
Chicago/Turabian StyleAlQahtani, Sheikha, and Dara Aldisi. 2023. "Muscle Wasting among Hospitalized Children: A Narrative Review of the Feasibility and Accuracy of Diagnostic Methods" Children 10, no. 5: 795. https://doi.org/10.3390/children10050795