
Respiratory Syncytial Virus Outbreak in Infants and Young Children during COVID-19 Pandemic in Taiwan


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
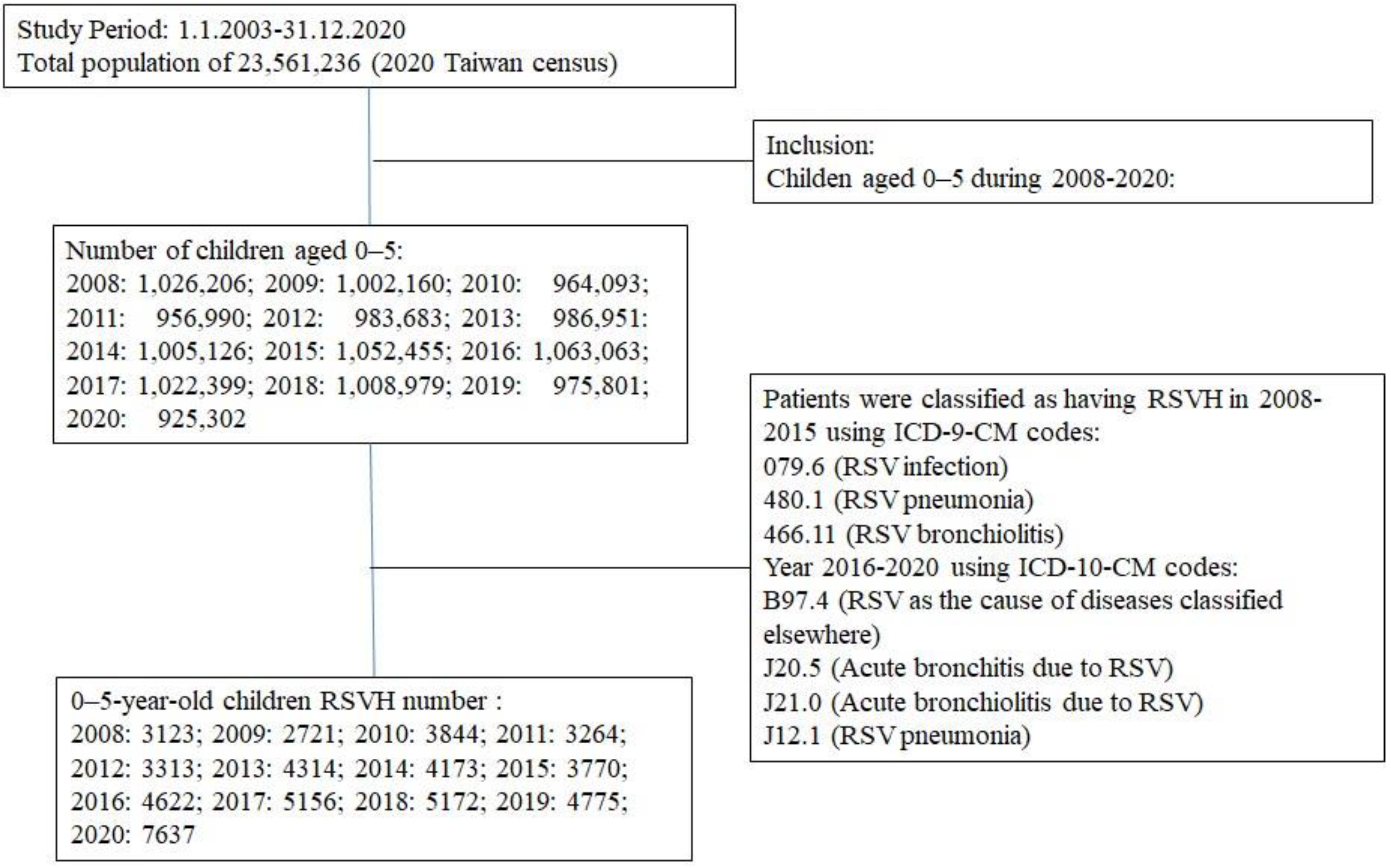
2.1. Data Source
2.2. Patient Selection
2.3. Data Analyses
3. Results
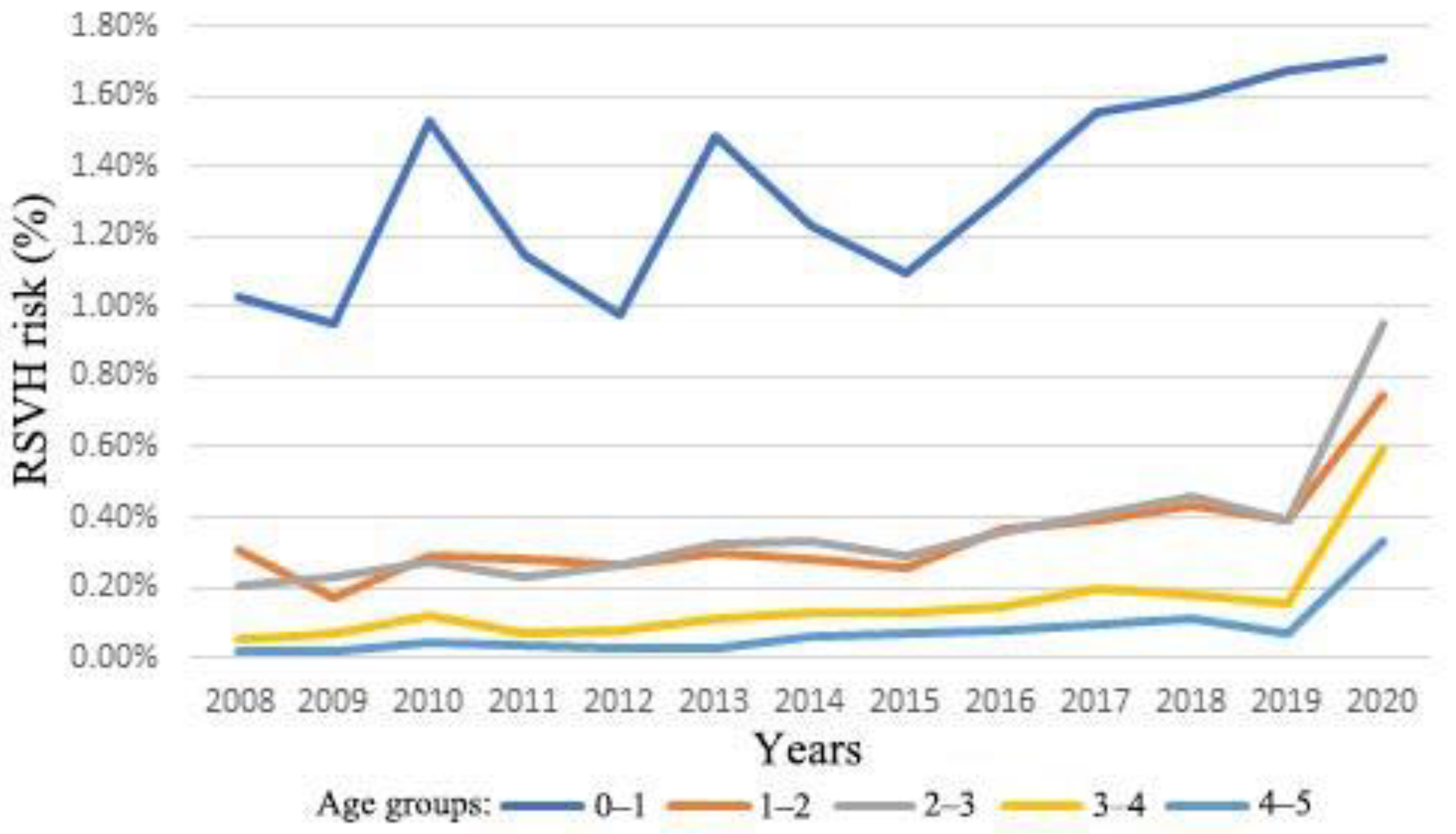
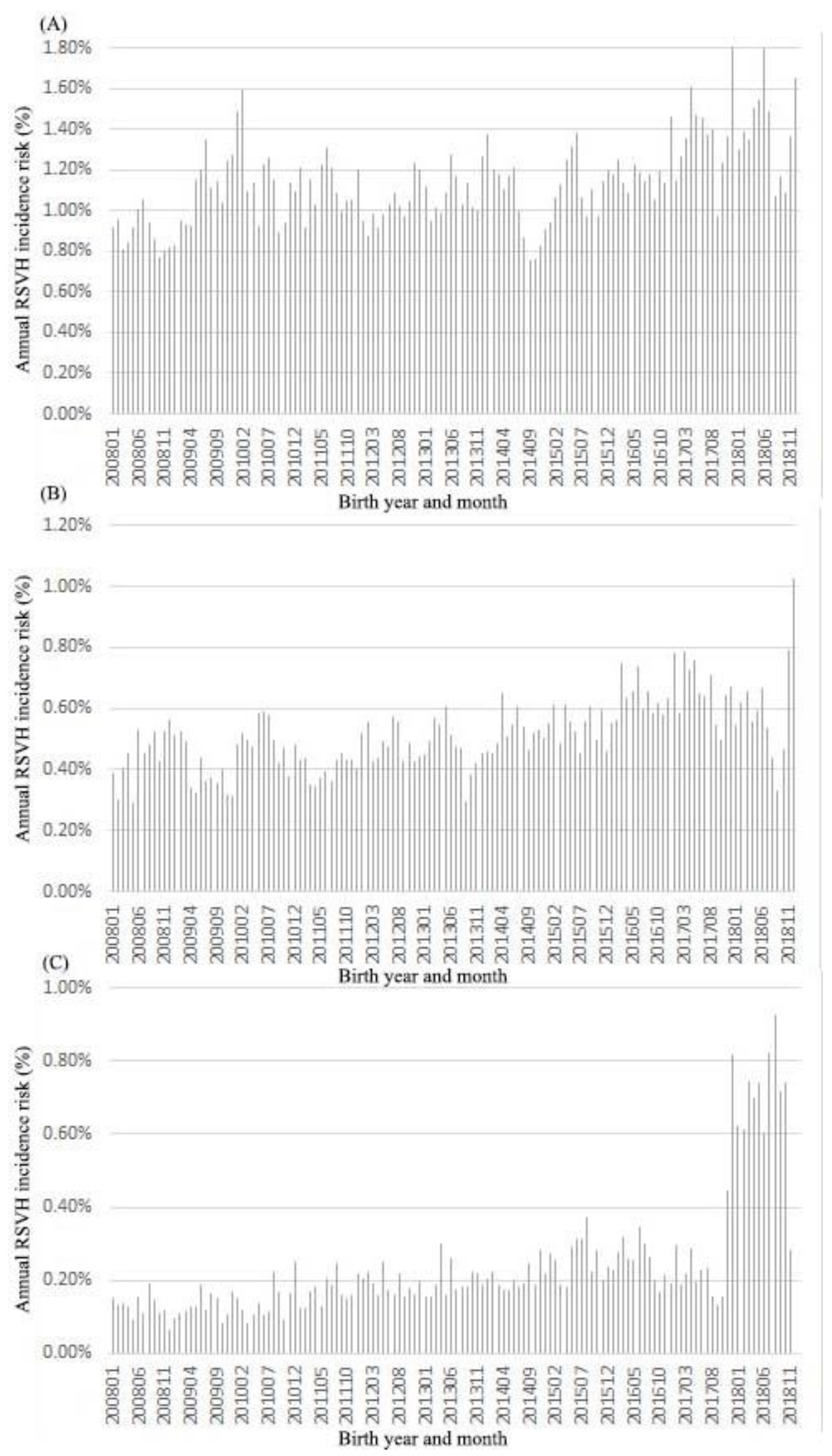
3.1. Annual Incidence of RSVH
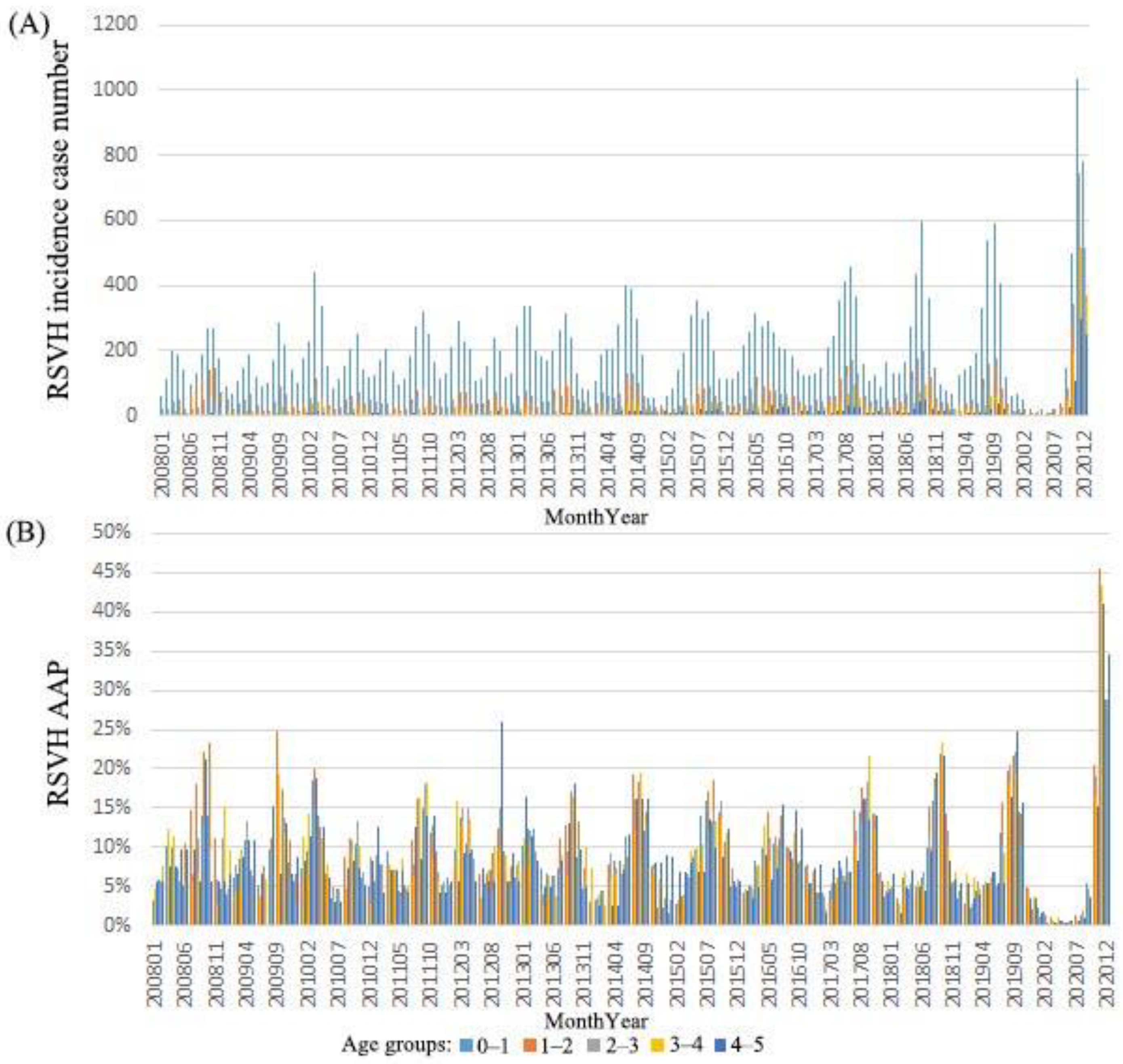
3.2. Monthly Case Number and AAP of RSVH in 2008–2020
3.3. RSVH Risk among Different Birth Months
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shi, T.; McAllister, D.A.; O’Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: A systematic review and modelling study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvajal, J.J.; Avellaneda, A.M.; Salazar-Ardiles, C.; Maya, J.E.; Kalergis, A.M.; Lay, M.K. Host Components Contributing to Respiratory Syncytial Virus Pathogenesis. Front. Immunol. 2019, 10, 2152. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Abu Raya, B.; Baraldi, E.; Flanagan, K.; Martinon Torres, F.; Tsolia, M.; Zielen, S. RSV Prevention in All Infants: Which Is the Most Preferable Strategy? Front. Immunol. 2022, 13, 880368. [Google Scholar] [CrossRef]
- Piedimonte, G.; Perez, M.K. Respiratory syncytial virus infection and bronchiolitis. Pediatr. Rev. 2014, 35, 519–530. [Google Scholar] [CrossRef]
- Meissner, H.C. More on Viral Bronchiolitis in Children. N. Engl. J. Med. 2016, 375, 1200. [Google Scholar] [CrossRef]
- The Pneumonia Etiology Research for Child Health Study Group. Causes of severe pneumonia requiring hospital admission in children without HIV infection from Africa and Asia: The PERCH multi-country case-control study. Lancet 2019, 394, 757–779. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.C.; Lin, T.Y.; Chang, L.Y.; Wong, K.S.; Ning, S.C. Epidemiology of respiratory syncytial virus infection among paediatric inpatients in northern Taiwan. Eur. J. Pediatr. 2001, 160, 581–582. [Google Scholar] [CrossRef] [PubMed]
- Chi, H.; Huang, Y.C.; Liu, C.C.; Chang, K.Y.; Huang, Y.C.; Lin, H.C.; Chang, L.Y.; Ho, Y.H.; Tsao, K.C.; Mu, J.J.; et al. Characteristics and etiology of hospitalized pediatric community-acquired pneumonia in Taiwan. J. Formos. Med. Assoc. 2020, 119, 1490–1499. [Google Scholar] [CrossRef]
- Leader, S.; Kohlhase, K. Recent trends in severe respiratory syncytial virus (RSV) among US infants, 1997 to 2000. J. Pediatr. 2003, 143, S127–S132. [Google Scholar] [CrossRef] [PubMed]
- Thompson, W.W.; Shay, D.K.; Weintraub, E.; Brammer, L.; Cox, N.; Anderson, L.J.; Fukuda, K. Mortality associated with influenza and respiratory syncytial virus in the United States. JAMA 2003, 289, 179–186. [Google Scholar] [CrossRef]
- Boyce, T.G.; Mellen, B.G.; Mitchel, E.F., Jr.; Wright, P.F.; Griffin, M.R. Rates of hospitalization for respiratory syncytial virus infection among children in medicaid. J. Pediatr. 2000, 137, 865–870. [Google Scholar] [CrossRef]
- Chi, H.; Chang, I.S.; Tsai, F.Y.; Huang, L.M.; Shao, P.L.; Chiu, N.C.; Chang, L.Y.; Huang, F.Y. Epidemiological study of hospitalization associated with respiratory syncytial virus infection in Taiwanese children between 2004 and 2007. J. Formos. Med. Assoc. 2011, 110, 388–396. [Google Scholar] [CrossRef] [Green Version]
- Hall, C.B.; Weinberg, G.A.; Blumkin, A.K.; Edwards, K.M.; Staat, M.A.; Schultz, A.F.; Poehling, K.A.; Szilagyi, P.G.; Griffin, M.R.; Williams, J.V.; et al. Respiratory syncytial virus-associated hospitalizations among children less than 24 months of age. Pediatrics 2013, 132, e341–e348. [Google Scholar] [CrossRef] [PubMed]
- Chi, H.; Chung, C.H.; Lin, Y.J.; Lin, C.H. Seasonal peaks and risk factors of respiratory syncytial virus infections related hospitalization of preterm infants in Taiwan. PLoS ONE 2018, 13, e0197410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arriola, C.S.; Kim, L.; Langley, G.; Anderson, E.J.; Openo, K.; Martin, A.M.; Lynfield, R.; Bye, E.; Como-Sabetti, K.; Reingold, A.; et al. Estimated Burden of Community-Onset Respiratory Syncytial Virus-Associated Hospitalizations Among Children Aged < 2 Years in the United States, 2014–2015. J. Pediatric Infect. Dis. Soc. 2020, 9, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Rha, B.; Curns, A.T.; Lively, J.Y.; Campbell, A.P.; Englund, J.A.; Boom, J.A.; Azimi, P.H.; Weinberg, G.A.; Staat, M.A.; Selvarangan, R.; et al. Respiratory Syncytial Virus-Associated Hospitalizations among Young Children: 2015–2016. Pediatrics 2020, 146, e20193611. [Google Scholar] [CrossRef]
- Obando-Pacheco, P.; Justicia-Grande, A.J.; Rivero-Calle, I.; Rodriguez-Tenreiro, C.; Sly, P.; Ramilo, O.; Mejias, A.; Baraldi, E.; Papadopoulos, N.G.; Nair, H.; et al. Respiratory Syncytial Virus Seasonality: A Global Overview. J. Infect. Dis. 2018, 217, 1356–1364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.T.; Chang, L.Y.; Wang, L.C.; Kao, C.L.; Shao, P.L.; Lu, C.Y.; Lee, P.I.; Chen, J.M.; Lee, C.Y.; Huang, L.M. Epidemiology of respiratory syncytial virus infection in northern Taiwan, 2001–2005—Seasonality, clinical characteristics, and disease burden. J. Microbiol. Immunol. Infect. 2007, 40, 293–301. [Google Scholar]
- Hsu, C.H.; Lin, C.Y.; Chi, H.; Chang, J.H.; Hung, H.Y.; Kao, H.A.; Peng, C.C.; Jim, W.T. Prolonged seasonality of respiratory syncytial virus infection among preterm infants in a subtropical climate. PLoS ONE 2014, 9, e110166. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.T.; Huang, F.L.; Ting, P.J.; Chang, C.C.; Chen, P.Y. The epidemiological features of pediatric viral respiratory infection during the COVID-19 pandemic in Taiwan. J. Microbiol. Immunol. Infect. 2022, 55, 1101–1107. [Google Scholar] [CrossRef]
- Lin, T.Y.; Chi, H.; Kuo, C.Y.; Tsai, H.P.; Wang, J.R.; Liu, C.C.; Shen, C.F. Outbreak of respiratory syncytial virus subtype ON1 among children during COVID-19 pandemic in Southern Taiwan. J. Microbiol. Immunol. Infect. 2022, 55, 1168–1179. [Google Scholar] [CrossRef] [PubMed]
- Ujiie, M.; Tsuzuki, S.; Nakamoto, T.; Iwamoto, N. Resurgence of Respiratory Syncytial Virus Infections during COVID-19 Pandemic, Tokyo, Japan. Emerg. Infect. Dis. 2021, 27, 2969–2970. [Google Scholar] [CrossRef] [PubMed]
- Eden, J.S.; Sikazwe, C.; Xie, R.; Deng, Y.M.; Sullivan, S.G.; Michie, A.; Levy, A.; Cutmore, E.; Blyth, C.C.; Britton, P.N.; et al. Off-season RSV epidemics in Australia after easing of COVID-19 restrictions. Nat. Commun. 2022, 13, 2884. [Google Scholar] [CrossRef]
- Li, Y.; Reeves, R.M.; Wang, X.; Bassat, Q.; Brooks, W.A.; Cohen, C.; Moore, D.P.; Nunes, M.; Rath, B.; Campbell, H.; et al. Global patterns in monthly activity of influenza virus, respiratory syncytial virus, parainfluenza virus, and metapneumovirus: A systematic analysis. Lancet Glob. Health 2019, 7, e1031–e1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shay, D.K.; Holman, R.C.; Newman, R.D.; Liu, L.L.; Stout, J.W.; Anderson, L.J. Bronchiolitis-associated hospitalizations among US children, 1980-1996. JAMA 1999, 282, 1440–1446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cilla, G.; Sarasua, A.; Montes, M.; Arostegui, N.; Vicente, D.; Perez-Yarza, E.; Perez-Trallero, E. Risk factors for hospitalization due to respiratory syncytial virus infection among infants in the Basque Country, Spain. Epidemiol. Infect. 2006, 134, 506–513. [Google Scholar] [CrossRef]
- Bozzola, E.; Barni, S.; Villani, A. Respiratory Syncytial Virus Pediatric Hospitalization in the COVID-19 Era. Int. J. Environ. Res. Public. Health 2022, 19, 5455. [Google Scholar] [CrossRef]
- Clinciu, D.L.; Chen, C.H.; Wang, J.Y.; Huang, G. Letter to the Editor: Impact of COVID-19 Prevention Methods on Influenza and Other Respiratory Infections in Taiwan. Popul. Health Manag. 2021, 24, 631–632. [Google Scholar] [CrossRef]
- Qiu, W.; Zheng, C.; Huang, S.; Zhang, Y.; Chen, Z. Epidemiological Trend of RSV Infection Before and During COVID-19 Pandemic: A Three-Year Consecutive Study in China. Infect. Drug. Resist. 2022, 15, 6829–6837. [Google Scholar] [CrossRef]
- Bardsley, M.; Morbey, R.A.; Hughes, H.E.; Beck, C.R.; Watson, C.H.; Zhao, H.; Ellis, J.; Smith, G.E.; Elliot, A.J. Epidemiology of respiratory syncytial virus in children younger than 5 years in England during the COVID-19 pandemic, measured by laboratory, clinical, and syndromic surveillance: A retrospective observational study. Lancet Infect. Dis. 2023, 23, 56–66. [Google Scholar] [CrossRef]
- Mira-Iglesias, A.; Demont, C.; Lopez-Labrador, F.X.; Mengual-Chulia, B.; Garcia-Rubio, J.; Carballido-Fernandez, M.; Tortajada-Girbes, M.; Mollar-Maseres, J.; Schwarz-Chavarri, G.; Puig-Barbera, J.; et al. Role of age and birth month in infants hospitalized with RSV-confirmed disease in the Valencia Region, Spain. Influenza Other Respir. Viruses 2022, 16, 328–339. [Google Scholar] [CrossRef]
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; Madhi, S.A.; Omer, S.B.; Simoes, E.A.F.; Campbell, H.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: A systematic analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef] [PubMed]
- Bozzola, E.; Ciarlitto, C.; Guolo, S.; Brusco, C.; Cerone, G.; Antilici, L.; Schettini, L.; Piscitelli, A.L.; Chiara Vittucci, A.; Cutrera, R.; et al. Respiratory Syncytial Virus Bronchiolitis in Infancy: The Acute Hospitalization Cost. Front. Pediatr. 2020, 8, 594898. [Google Scholar] [CrossRef] [PubMed]
- Hammitt, L.L.; Dagan, R.; Yuan, Y.; Baca Cots, M.; Bosheva, M.; Madhi, S.A.; Muller, W.J.; Zar, H.J.; Brooks, D.; Grenham, A.; et al. Nirsevimab for Prevention of RSV in Healthy Late-Preterm and Term Infants. N. Engl. J. Med. 2022, 386, 837–846. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chi, H.; Chung, C.-H. Respiratory Syncytial Virus Outbreak in Infants and Young Children during COVID-19 Pandemic in Taiwan. Children 2023, 10, 629. https://doi.org/10.3390/children10040629
Chi H, Chung C-H. Respiratory Syncytial Virus Outbreak in Infants and Young Children during COVID-19 Pandemic in Taiwan. Children. 2023; 10(4):629. https://doi.org/10.3390/children10040629
Chicago/Turabian StyleChi, Hsin, and Ching-Hu Chung. 2023. "Respiratory Syncytial Virus Outbreak in Infants and Young Children during COVID-19 Pandemic in Taiwan" Children 10, no. 4: 629. https://doi.org/10.3390/children10040629