
Randomized Trial of 21% versus 100% Oxygen during Chest Compressions Followed by Gradual versus Abrupt Oxygen Titration after Return of Spontaneous Circulation in Neonatal Lambs
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Instrumentation in Utero
2.2. Asphyxial Cardiac Arrest and Resuscitation
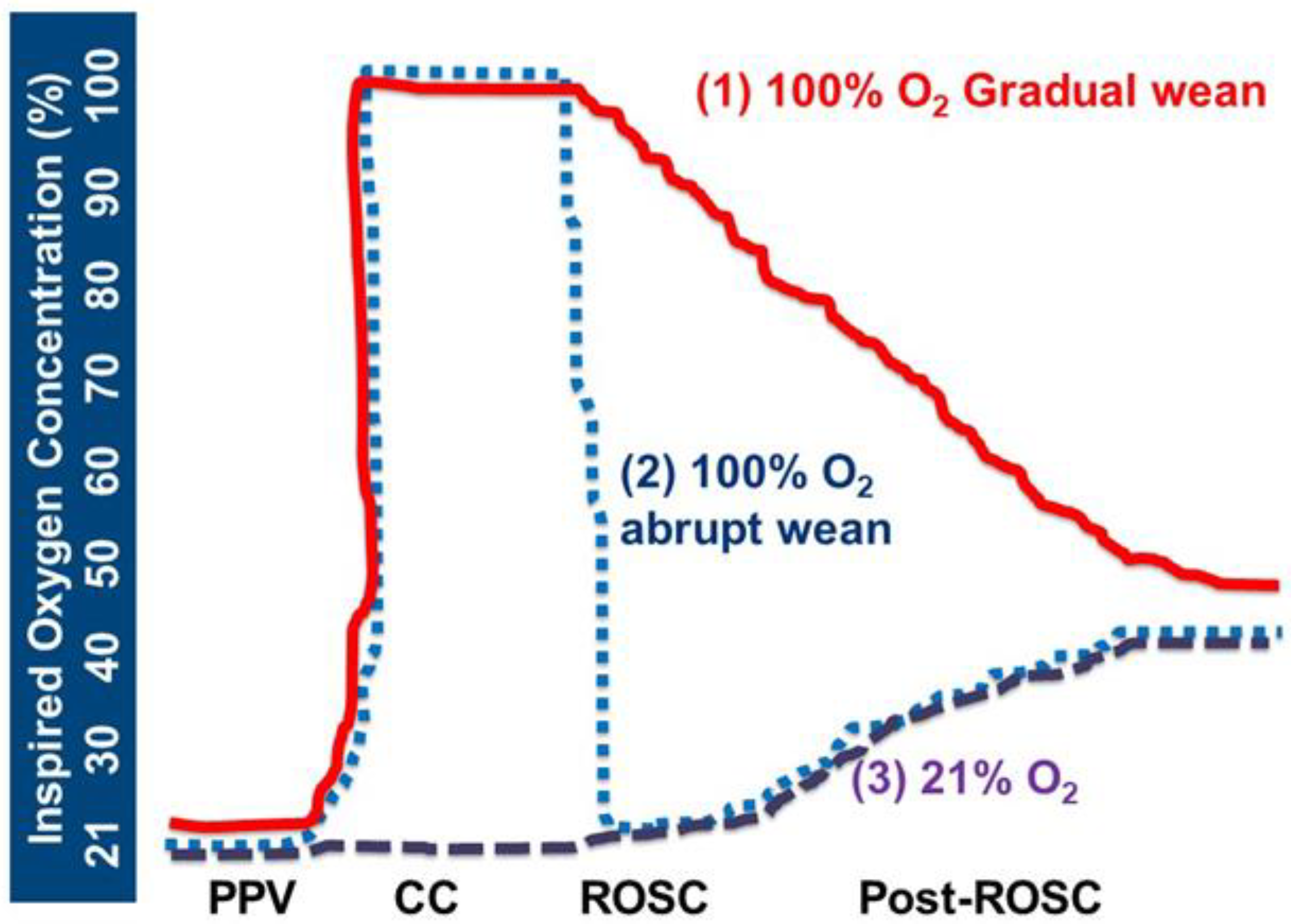
- Group 1: 100% O2 CC—Gradual wean: Inspired oxygen was increased to 100% during CC and resuscitation was continued per AAP-NRP guidelines. Following ROSC, attempts were made to adjust inspired oxygen down from 100% O2 by 5–10% every 30 sec to achieve preductal SpO2 per NRP guidelines. After the first 10 min, we targeted 85–95% SpO2 in lambs that achieved ROSC during the first 30 min after ROSC, and 90–95% beyond 30 min after ROSC until 60 min for all the study lambs.
- Group 2: 100% O2 CC—Abrupt wean: Inspired oxygen was increased to 100% during CC, and resuscitation was continued per NRP. After ROSC, the inspired oxygen was rapidly decreased to 21% and attempts were made to adjust inspired oxygen up by 5–10% every 30 sec to maintain preductal SpO2 as described above.
- Group 3: 21% O2 CC: Inspired oxygen of 21% was administered during chest compressions. Following ROSC, inspired oxygen was titrated up by 5–10% every 30 sec to achieve preductal SpO2 as described above.
2.3. Primary and Secondary Outcomes
2.4. Sample Size Calculation
2.5. Data Collection and Analysis
3. Results
3.1. Hemodynamic and Arterial Blood Gas Parameters during Chest Compressions and after ROSC
3.2. Comparison of Markers of Oxidative Stress in Plasma and Brain Tissue
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kumar, V.H.; Patel, A.; Swartz, D.D.; Wang, H.; Wynn, K.; Nielsen, L.C.; Ryan, R.M. Exposure to Supplemental Oxygen and Its Effects on Oxidative Stress and Antioxidant Enzyme Activity in Term Newborn Lambs. Pediatr. Res. 2010, 67, 66–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiner, G.M.; Zaichkin, J. American Academy of Pediatrics. American Heart Association; In Textbook of Neonatal Resuscitation, 8th ed.; American Heart Association: Chicago, IL, USA, 2021. [Google Scholar]
- Aziz, K.; Lee, H.C.; Escobedo, M.B.; Hoover, A.V.; Kamath-Rayne, B.D.; Kapadia, V.S.; Magid, D.J.; Niermeyer, S.; Schmölzer, G.M.; Szyld, E.; et al. Part 5: Neonatal Resuscitation: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S524–S550. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, A.A. Response of the cerebral circulation to hypocarbia in postasphyxia newborn lambs. Pediatr. Res. 1992, 32, 537–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pryds, O.; Greisen, G.; Lou, H.; Friis-Hansen, B. Vasoparalysis associated with brain damage in asphyxiated term infants. J. Pediatr. 1990, 117, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Rawat, M.; Chandrasekharan, P.; Gugino, S.; Koenigsknecht, C.; Helman, J.; Alsaleem, M.; Mathew, B.; Nair, J.; Berkelhamer, S.; Vali, P.; et al. Oxygenation and Hemodynamics during Chest Compressions in a Lamb Model of Perinatal Asphyxia Induced Cardiac Arrest. Children 2019, 6, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez, M.; Robbins, M.E.; Revhaug, C.; Saugstad, O.D. Oxygen radical disease in the newborn, revisited: Oxidative stress and disease in the newborn period. Free. Radic. Biol. Med. 2019, 142, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Sankaran, D.; Vali, P.; Chen, P.; Lesneski, A.L.; Hardie, M.E.; Alhassen, Z.; Wedgwood, S.; Wyckoff, M.H.; Lakshminrusimha, S. Randomized trial of oxygen weaning strategies following chest compressions during neonatal resuscitation. Pediatr. Res. 2021, 90, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Sankaran, D.; Chandrasekharan, P.K.; Gugino, S.F.; Koenigsknecht, C.; Helman, J.; Nair, J.; Mathew, B.; Rawat, M.; Vali, P.; Nielsen, L.; et al. Randomised trial of epinephrine dose and flush volume in term newborn lambs. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 106, 578–583. [Google Scholar] [CrossRef] [PubMed]
- du Sert, N.P.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The ARRIVE guidelines 2.0: Updated guidelines for reporting animal research. PLoS Biol. 2020, 18, e3000410. [Google Scholar]
- Hooper, S.B.; Crossley, K.J.; Zahra, V.; van Vonderen, J.; Moxham, A.; Gill, A.W.; Kluckow, M.; Pas, A.B.T.; Wallace, E.M.; Polglase, G.R. Effect of body position and ventilation on umbilical artery and venous blood flows during delayed umbilical cord clamping in preterm lambs. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, F312–F319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nair, J.; Vali, P.; Gugino, S.F.; Koenigsknecht, C.; Helman, J.; Nielsen, L.C.; Chandrasekharan, P.; Rawat, M.; Berkelhamer, S.; Mathew, B.; et al. Bioavailability of endotracheal epinephrine in an ovine model of neonatal resuscitation. Early Hum. Dev. 2019, 130, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Vali, P.; Sankaran, D.; Rawat, M.; Berkelhamer, S.; Lakshminrusimha, S. Epinephrine in Neonatal Resuscitation. Children 2019, 6, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumagai, T.; Higuchi, R.; Higa, A.; Tsuno, Y.; Hiramatsu, C.; Sugimoto, T.; Booka, M.; Okutani, T.; Yoshikawa, N. Correlation between echocardiographic superior vena cava flow and short-term outcome in infants with asphyxia. Early Hum. Dev. 2013, 89, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Linner, R.; Werner, O.; Perez-De-Sa, V.; Cunha-Goncalves, D. Circulatory Recovery Is as Fast with Air Ventilation as with 100% Oxygen After Asphyxia-Induced Cardiac Arrest in Piglets. Pediatr. Res. 2009, 66, 391–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sankaran, D.; Rawat, M.; Lakshminrusimha, S. Optimal oxygen use in neonatal advanced cardiopulmonary resuscitation—A literature review. Pediatr. Med. 2022, 1–17. [Google Scholar] [CrossRef]
- Solevåg, A.L.; Schmölzer, G.M.; O’Reilly, M.; Lu, M.; Lee, T.-F.; Hornberger, L.K.; Nakstad, B.; Cheung, P.-Y. Myocardial perfusion and oxidative stress after 21% vs. 100% oxygen ventilation and uninterrupted chest compressions in severely asphyxiated piglets. Resuscitation 2016, 106, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Hidalgo, C.; Cheung, P.-Y.; Solevåg, A.L.; Vento, M.; O’Reilly, M.; Saugstad, O.; Schmölzer, G.M. A Review of Oxygen Use During Chest Compressions in Newborns—A Meta-Analysis of Animal Data. Front. Pediatr. 2018, 6, 400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saugstad, O.D.; Ramji, S.; Soll, R.F.; Vento, M. Resuscitation of Newborn Infants with 21% or 100% Oxygen: An Updated Systematic Review and Meta-Analysis. Neonatology 2008, 94, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Perez-De-Sa, V.; Cunha-Goncalves, D.; Nordh, A.; Hansson, S.; Larsson, A.; Ley, D.; Fellman, V.; Werner, O. High brain tissue oxygen tension during ventilation with 100% oxygen after fetal asphyxia in newborn sheep. Pediatr. Res. 2009, 65, 57–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koch, J.D.; Miles, D.K.; Gilley, J.; Yang, C.-P.; Kernie, S.G. brief exposure to hyperoxia depletes the glial progenitor pool and impairs functional recovery after hypoxic-ischemic brain injury. J. Cereb. Blood Flow Metab. 2008, 28, 1294–1306. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | 100% O2 CC—Gradual Wean (n = 7) | 100% O2 CC—Abrupt Wean (n = 6) | 21% O2 CC (n = 6) |
|---|---|---|---|
| Weight (kg) | 3.5 ± 0.6 | 3.6 ± 0.6 | 3.7 ± 0.6 |
| Gestational Age (days) | 140 ± 1.5 | 139.7 ± 0.5 | 139.7 ± 1.4 |
| Sex (F:M) | 4:3 | 5:1 | 5:1 |
| Hemoglobin, g/dL | 12.0 ± 1.4 | 11.4 ± 1.0 | 13.4 ± 2 |
| pH | 7.24 ± 0.10 | 7.18 ± 0.08 | 7.19 ± 0.10 |
| PaCO2 (mm Hg) | 66 ± 14 | 71 ± 11 | 76 ± 16 |
| PaO2 (mm Hg) | 22 ± 6 | 25 ± 3 | 20 ± 8 |
| Cerebral oxygen delivery (mL/kg/min) | 3.0 ± 1.3 | 2.9 ± 0.7 | 2.7 ± 1.1 |
| Lactate (mmol/L) | 3.5 ± 2.2 | 2.5 ± 1.7 | 3.1 ± 2.6 |
| Mean Carotid Artery Blood Flow (mL/kg/min) | 31.3 ± 8.0 | 30.1 ± 6.4 | 29.7 ± 9.0 |
| Duration of Asphyxia until Asystole (min) | 12.5 ± 2.9 | 15.1 ± 2.3 | 16.5 ± 4.4 |
| Incidence of ROSC n (%) | 7 (100) | 6 (100) | 5 (83.3) |
| Number of epinephrine doses n (ROSC or not) | 1 dose in 7 lambs (ROSC) | 1 dose in 6 lambs (ROSC) | 1 dose in 5 lambs ROSC) 4 doses in 1 lamb (ROSC followed by rearrest) |
| Parameter | 100% O2 CC—Gradual Wean (n = 7) | 100% O2 CC—Abrupt Wean (n = 6) | 21% O2 CC (n = 6) |
|---|---|---|---|
| PaO2 (mm Hg) | 18.5 ± 5.5 | 13.7 ± 11.0 | 10.7 ± 4.3 |
| Mean Carotid Artery Blood Flow (QCA, mL/kg/min) | 3.1 ± 0.9 | 3.6 ± 1.8 | 2.8 ± 0.8 |
| Cerebral oxygen delivery (mL/kg/min) | 0.07 ± 0.07 | 0.08 ± 0.07 | 0.06 ± 0.02 |
| Parameter | 100% O2 CC—Gradual Wean (n = 7) | 100% O2 CC—Abrupt Wean (n = 6) | 21% O2 CC (n = 6) |
|---|---|---|---|
| Plasma markers | |||
| Hypoxanthine/xanthine ratio Fetal Baseline | 26 ± 16 | 26 ± 14 | 17 ± 12 |
| 5 min after ROSC | 40 * ± 8 | 25 ± 6 | 24 ± 10 |
| 10 min after ROSC | 31 ± 16 | 28 ± 15 | 24 ± 8 |
| Methionine sulfoxide/methionine ratio | |||
| Fetal baseline | 5.5 ± 1.5 | 5.2 ± 0.1 | 5.4 ± 1.2 |
| 5 min after ROSC | 6.7 ± 1.2 | 5.5 ± 1.1 | 5.8 ± 1.6 |
| 10 min after ROSC | 6.6 ± 2.0 | 8.7 ± 1.0 | 7.6 ± 2.5 |
| Lactic acid (×105) | |||
| Fetal baseline | 8.7 ± 0.9 | 8.5 ± 2.2 | 13.9 ± 11.4 |
| 5 min after ROSC | 39.4 ± 5.2 | 29.6 ± 9.4 | 32.4 ± 8.4 |
| 10 min after ROSC | 37.5 ± 7.5 | 33.2 ± 2.6 | 30.6 ± 12.3 |
| Brain markers | |||
| Brain hypoxanthine/xanthine ratio | 24.2 ± 35.2 | 9.2 ± 1.9 | 10.6 ± 2.1 |
| Brain methionine sulfoxide/methionine ratio | 2.2 ± 1.1 | 1.3 ± 0.1 | 1.2 ± 0.3 |
| Brain lactic acid (×105) | 7.3 ± 1.7 | 6.3 ± 0.7 | 9.3 * ± 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sankaran, D.; Giusto, E.M.; Lesneski, A.L.; Hardie, M.E.; Joudi, H.M.; Lane, E.C.A.; Hammitt, V.L.; Tully, K.C.; Vali, P.; Lakshminrusimha, S. Randomized Trial of 21% versus 100% Oxygen during Chest Compressions Followed by Gradual versus Abrupt Oxygen Titration after Return of Spontaneous Circulation in Neonatal Lambs. Children 2023, 10, 575. https://doi.org/10.3390/children10030575
Sankaran D, Giusto EM, Lesneski AL, Hardie ME, Joudi HM, Lane ECA, Hammitt VL, Tully KC, Vali P, Lakshminrusimha S. Randomized Trial of 21% versus 100% Oxygen during Chest Compressions Followed by Gradual versus Abrupt Oxygen Titration after Return of Spontaneous Circulation in Neonatal Lambs. Children. 2023; 10(3):575. https://doi.org/10.3390/children10030575
Chicago/Turabian StyleSankaran, Deepika, Evan M. Giusto, Amy L. Lesneski, Morgan E. Hardie, Houssam M. Joudi, Emily C. A. Lane, Victoria L. Hammitt, Kirstie C. Tully, Payam Vali, and Satyan Lakshminrusimha. 2023. "Randomized Trial of 21% versus 100% Oxygen during Chest Compressions Followed by Gradual versus Abrupt Oxygen Titration after Return of Spontaneous Circulation in Neonatal Lambs" Children 10, no. 3: 575. https://doi.org/10.3390/children10030575