
Role of Maternal and Child Health Handbook on Improving Maternal, Newborn, and Child Health Outcomes: A Systematic Review and Meta-Analysis
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Criteria for Considering Studies in This Review
- (i)
- Participants
- (ii)
- Interventions
- (iii)
- Comparators
- (iv) Outcomes
- (v) Study designs
2.2. Outcomes of Interests
2.2.1. Primary Outcomes
- (i)
- Number of antenatal care (ANC) visits;
- (ii)
- Number of facility deliveries;
- (iii)
- Skilled birth attendance (SBA) at the time of delivery;
- (iv)
- Number of postnatal care (PNC) visits for mother;
- (v)
- Number of cesarean deliveries;
- (vi)
- Proportion of exclusive breastfeeding practices;
- (vii)
- Number of pregnant women who stopped or reduced cigarette smoking.
2.2.2. Secondary Outcomes
- (i)
- Maternal satisfaction and control
- (ii)
- Maternal and child vaccination coverage
- (iii)
- Partner involvement in the pregnancy, during labor, and after childbirth
- (iv)
- Maternal morbidity and mortality
- (v)
- Infant morbidity and mortality
- (vi)
- Administrative outcomes
2.3. Study Identification
2.4. Study Selection, Data Extraction and Quality Assessment
2.5. Data Synthesis and Analytical Approach
2.6. Assessment of the Certainty of the Evidence
2.7. Patient and Public Involvement
3. Results
3.1. Study Inclusion
3.2. Characteristics of the Included Studies
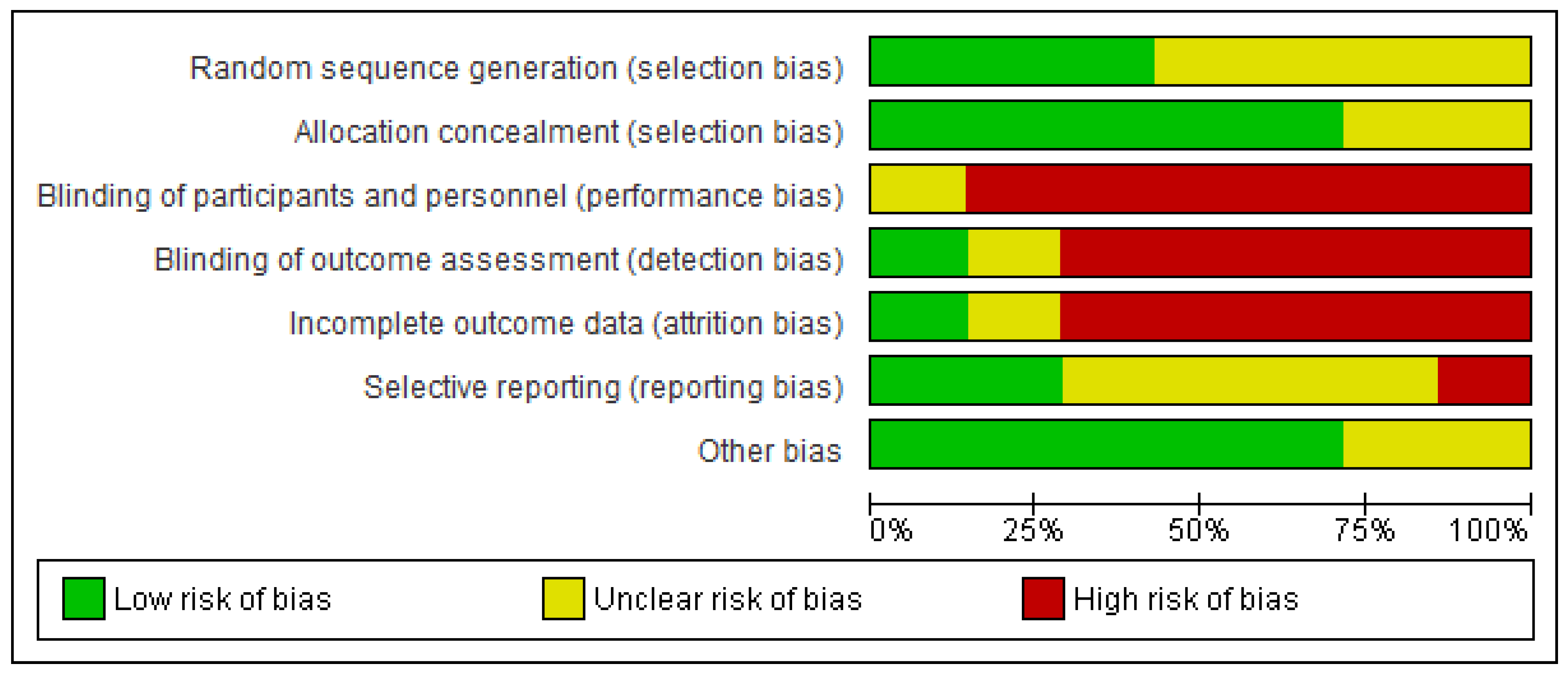
3.3. Overall Risk of Bias Assessment of the Included Studies
3.4. Pooled Effects of MCH Handbook Interventions on Improving Maternal, Newborn, and Child Health Outcomes
3.4.1. Number of ANC Visits
3.4.2. Skilled Birth Attendance at the Time of Delivery
3.4.3. Cesarean Delivery
3.4.4. Breastfeeding Practice
3.4.5. Maternal Smoking
3.4.6. Infant Morbidity and Mortality
3.4.7. Drinking during Pregnancy
3.4.8. Case Notes Lost or Left at Home
3.4.9. Women Satisfied with Antenatal or Maternity Care
3.4.10. Women Who Wanted to Carry Their Case Notes in Subsequent Pregnancy
3.4.11. Women Who Felt in Control during ANC
3.4.12. Support from Family during Pregnancy
3.4.13. Maternal Morbidity and Mortality
3.4.14. Certainty of the Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bhutta, Z.A.; Das, J.K.; Bahl, R.; Lawn, J.E.; Salam, R.A.; Paul, V.K.; Sankar, M.J.; Blencowe, H.; Rizvi, A.; Chou, V.B.; et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet 2014, 384, 347–370. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y. The role of maternal and child health (MCH) handbook in the era of sustainable development goals (SDGs). J. Glob. Health Sci. 2019, 1, e24. [Google Scholar] [CrossRef] [Green Version]
- Osaki, K.; Aiga, H. What Is Maternal and Child Health Handbook? Agency JIC: Tokyo, Japan, 2016. [Google Scholar]
- Osaki, K.; Aiga, H. Adapting home-based records for maternal and child health to users’ capacities. Bull. World Health Organ. 2019, 97, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Bhuiyan, S.U.; Nakamura, Y. Continuity of maternal, neonatal and child health care through MCH handbook for ensuring the quality of life. In MCH Handbook Conference Report; Osaka University: Suita, Japan, 2009. [Google Scholar]
- Osaki, K.; Hattori, T.; Kosen, S. The role of home-based records in the establishment of a continuum of care for mothers, newborns, and children in Indonesia. Glob. Health Action 2013, 6, 20429. [Google Scholar] [CrossRef]
- Brown, D.W.; Bosch-Capblanch, X.; Shimp, L. Where Do We Go From Here? Defining an Agenda for Home-Based Records Research and Action Considering the 2018 WHO Guidelines. Glob. Health Sci. Pract. 2019, 7, 6–11. [Google Scholar] [CrossRef] [Green Version]
- Magwood, O.; Kpadé, V.; Thavorn, K.; Oliver, S.; Mayhew, A.D.; Pottie, K. Correction: Effectiveness of home-based records on maternal, newborn and child health outcomes: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0212698. [Google Scholar] [CrossRef]
- Brown, H.C.; Smith, H.J.; Mori, R.; Noma, H. Giving women their own case notes to carry during pregnancy. Cochrane Database Syst. Rev. 2015, 2015, Cd002856. [Google Scholar] [CrossRef]
- Carandang, R.R.; Sakamoto, J.L.; Kunieda, M.K.; Shibanuma, A.; Yarotskaya, E.; Basargina, M.; Jimba, M. Roles of the Maternal and Child Health Handbook and Other Home-Based Records on Newborn and Child Health: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 7463. [Google Scholar] [CrossRef]
- Carandang, R.R.; Sakamoto, J.L.; Kunieda, M.K.; Shibanuma, A.; Yarotskaya, E.; Basargina, M.; Jimba, M. Effects of the maternal and child health handbook and other home-based records on mothers’ non-health outcomes: A systematic review. BMJ Open 2022, 12, e058155. [Google Scholar] [CrossRef]
- Chutiyami, M.; Wyver, S.; Amin, J. Are Parent-Held Child Health Records a Valuable Health Intervention? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 220. [Google Scholar] [CrossRef] [Green Version]
- Bhuiyan, S.; Begum, H.D.; Ehsan, S.; Jamal, S.S.; Shariff, R.; Linton, V.; Nafisa, T.; Bhuiyan, T.N. Maternal and child health (MCH) handbook and its effect on maternal and child health care: A systematic review and meta-analysis. J. Community Med. Public Health 2017, 1, CMPH-109. [Google Scholar] [CrossRef] [Green Version]
- Schiavo, J.H. PROSPERO: An International Register of Systematic Review Protocols. Med. Ref. Serv. Q. 2019, 38, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A.e. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022): Cochrane. 2022. Available online: www.training.cochrane.org/handbook (accessed on 26 December 2020).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mori, R.; Yonemoto, N.; Noma, H.; Ochirbat, T.; Barber, E.; Soyolgerel, G.; Nakamura, Y.; Lkhagvasuren, O. The Maternal and Child Health (MCH) handbook in Mongolia: A cluster-randomized, controlled trial. PLoS ONE 2015, 10, e0119772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osaki, K.; Hattori, T.; Toda, A.; Mulati, E.; Hermawan, L.; Pritasari, K.; Bardosono, S.; Kosen, S. Maternal and Child Health Handbook use for maternal and child care: A cluster randomized controlled study in rural Java, Indonesia. J. Public Health (Oxf) 2019, 41, 170–182. [Google Scholar] [CrossRef]
- Beigi, M.; Javanmardi, Z.; Khani, B.; Safdari, F. The effect of using maternal care log book on pregnancy outcome in clients referred to private gynecologists and midwives offices. Iran J. Nurs. Midwifery Res. 2011, 16, 222–226. [Google Scholar]
- Lovell, A.; Zander, L.I.; James, C.E.; Foot, S.; Swan, A.V.; Reynolds, A. The St. Thomas’s Hospital maternity case notes study: A randomised controlled trial to assess the effects of giving expectant mothers their own maternity case notes. Paediatr. Perinat. Epidemiol. 1987, 1, 57–66. [Google Scholar] [CrossRef]
- Dagvadorj, A.; Nakayama, T.; Inoue, E.; Sumya, N.; Mori, R. Cluster randomised controlled trial showed that maternal and child health handbook was effective for child cognitive development in Mongolia. Acta Paediatr. 2017, 106, 1360–1361. [Google Scholar] [CrossRef]
- Homer, C.S.; Davis, G.K.; Everitt, L.S. The introduction of a woman-held record into a hospital antenatal clinic: The bring your own records study. Aust. N. Z. J. Obstet. Gynaecol. 1999, 39, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Elbourne, D.; Richardson, M.; Chalmers, I.; Waterhouse, I.; Holt, E. The Newbury Maternity Care Study: A randomized controlled trial to assess a policy of women holding their own obstetric records. Br. J. Obstet. Gynaecol. 1987, 94, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dowswell, T.; Carroli, G.; Duley, L.; Gates, S.; Gulmezoglu, A.M.; Khan-Neelofur, D.; Piaggio, G. Alternative versus standard packages of antenatal care for low-risk pregnancy. Cochrane Database Syst. Rev. 2015, 2015, CD000934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. Available online: https://www.who.int/publications/i/item/9789241549912 (accessed on 26 January 2022).
- Yanagisawa, S.; Soyano, A.; Igarashi, H.; Ura, M.; Nakamura, Y. Effect of a maternal and child health handbook on maternal knowledge and behaviour: A community-based controlled trial in rural Cambodia. Health Policy Plan. 2015, 30, 1184–1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, J.; Vesel, L.; Bahl, R.; Martines, J.C. Timing of breastfeeding initiation and exclusivity of breastfeeding during the first month of life: Effects on neonatal mortality and morbidity--a systematic review and meta-analysis. Matern. Child Health J. 2015, 19, 468–479. [Google Scholar] [CrossRef] [PubMed]
- Phipps, H. Carrying their own medical records: The perspective of pregnant women. Aust. N. Z. J. Obstet. Gynaecol. 2001, 41, 398–401. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcomes | Anticipated Absolute Effects * (95% CI) | Relative Effect (95% CI) | No. of Participants (Studies) | Certainty of the Evidence (GRADE) | Comments | |
|---|---|---|---|---|---|---|
| Risk with Standard Care or No MCH Handbook | Risk with MCH Handbook | |||||
| ≥6 ANC visits | 549 per 1000 | 653 per 1000 (599 to 714) | RR 1.19 (1.09 to 1.30) | 955 (2 RCTs) | ⨁⨁⨁◯ MODERATE | Inverse variance |
| Cesarean delivery | 0 per 1000 | 0 per 1000 (0 to 0) | RR 1.07 (0.55 to 2.07) | 681 (2 RCTs) | ⨁◯◯◯ VERY LOW | Inverse variance |
| Early breastfeeding | 844 per 1000 | 903 per 1000 (853 to 954) | RR 1.07 (1.01 to 1.13) | 704 (2 RCTs) | ⨁⨁⨁◯ MODERATE | Inverse variance |
| Women who wanted to carry their case notes in subsequent pregnancy | 493 per 1000 | 887 per 1000 (704 to 1000) | RR 1.80 (1.43 to 2.25) | 553 (3 RCTs) | ⨁⨁◯◯ LOW | Inverse variance |
| Women felt in control during ANC | 235 per 1000 | 360 per 1000 (273 to 475) | RR 1.53 (1.16 to 2.02) | 450 (2 RCTs) | ⨁⨁⨁◯ MODERATE | Inverse variance |
| Family support during pregnancy | 531 per 1000 | 653 per 1000 (595 to 722) | RR 1.23 (1.12 to 1.36) | 651 (2 RCTs) | ⨁⨁◯◯ LOW | Inverse variance |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishimura, E.; Rahman, M.O.; Ota, E.; Toyama, N.; Nakamura, Y. Role of Maternal and Child Health Handbook on Improving Maternal, Newborn, and Child Health Outcomes: A Systematic Review and Meta-Analysis. Children 2023, 10, 435. https://doi.org/10.3390/children10030435
Nishimura E, Rahman MO, Ota E, Toyama N, Nakamura Y. Role of Maternal and Child Health Handbook on Improving Maternal, Newborn, and Child Health Outcomes: A Systematic Review and Meta-Analysis. Children. 2023; 10(3):435. https://doi.org/10.3390/children10030435
Chicago/Turabian StyleNishimura, Etsuko, Md Obaidur Rahman, Erika Ota, Noriko Toyama, and Yasuhide Nakamura. 2023. "Role of Maternal and Child Health Handbook on Improving Maternal, Newborn, and Child Health Outcomes: A Systematic Review and Meta-Analysis" Children 10, no. 3: 435. https://doi.org/10.3390/children10030435