
“Safer Births Bundle of Care” Implementation and Perinatal Impact at 30 Hospitals in Tanzania—Halfway Evaluation

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Organisation, Study Sites, and Population
2.2. Study Design and Timelines
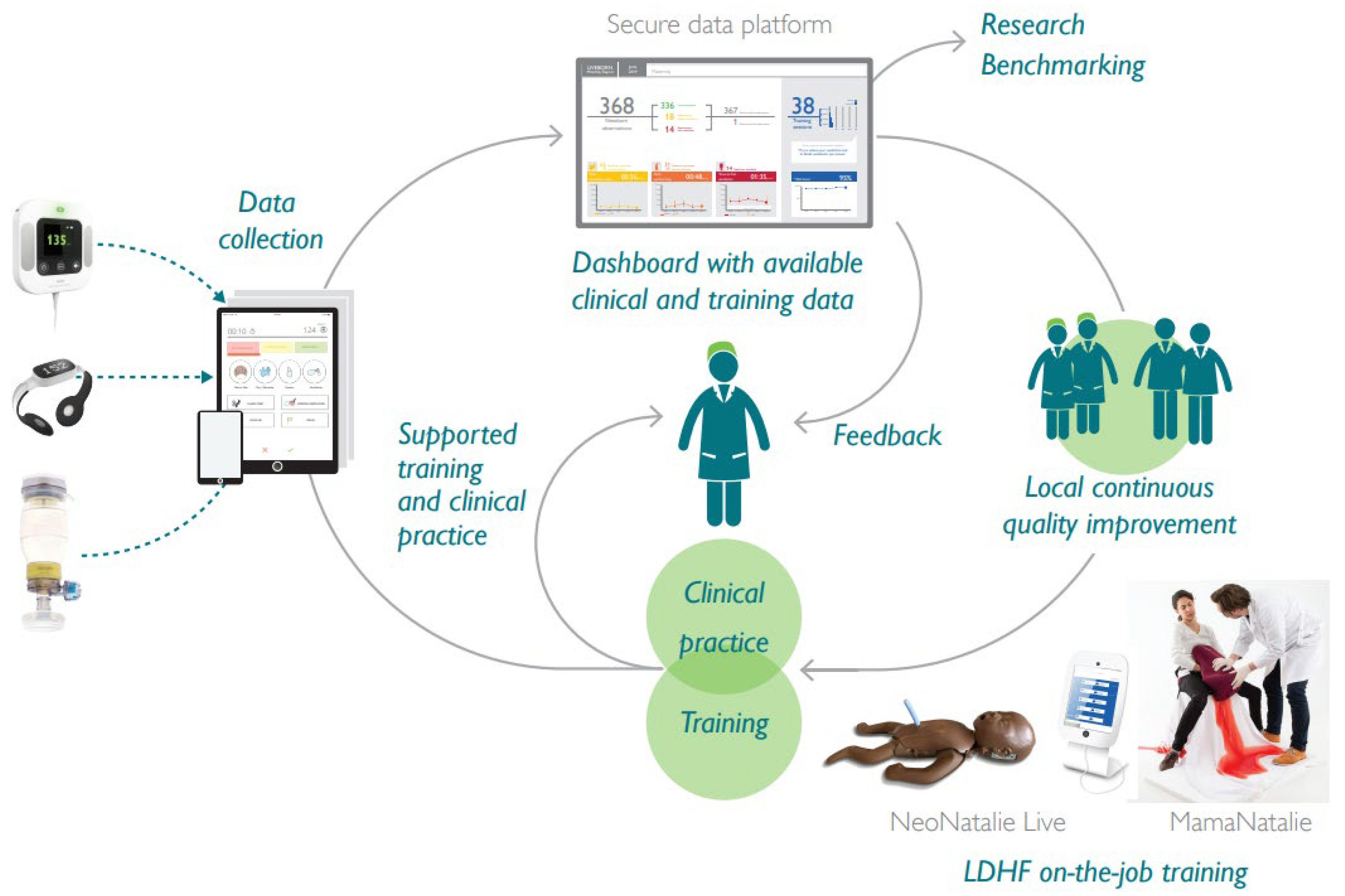
2.3. Safer Births Bundle of Care Components and Interventions
2.4. Data Collection and Management
2.5. Statistical Methods
2.6. Ethical Considerations
3. Results
3.1. Patient Characteristics and Key Performance Indicators
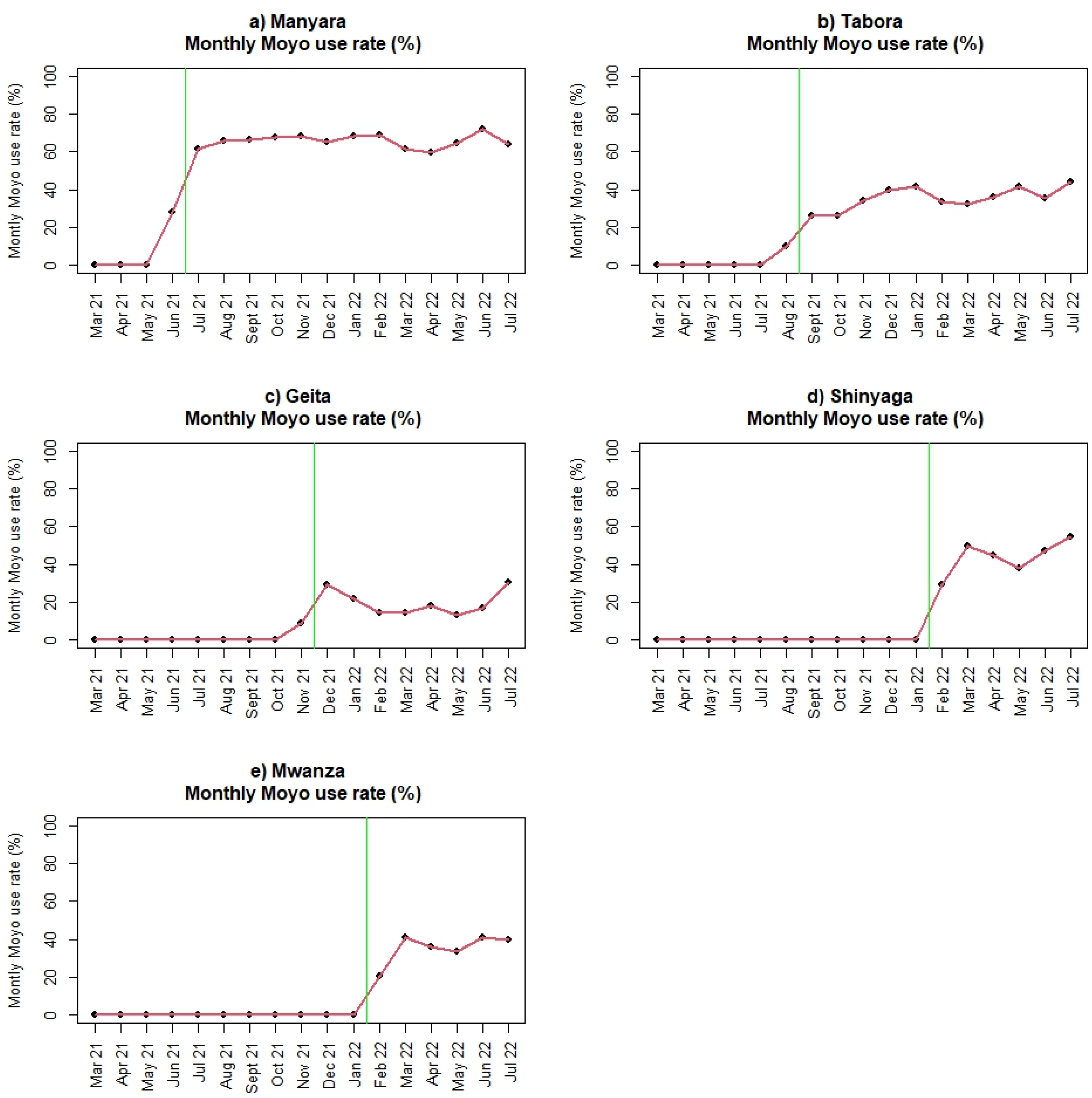
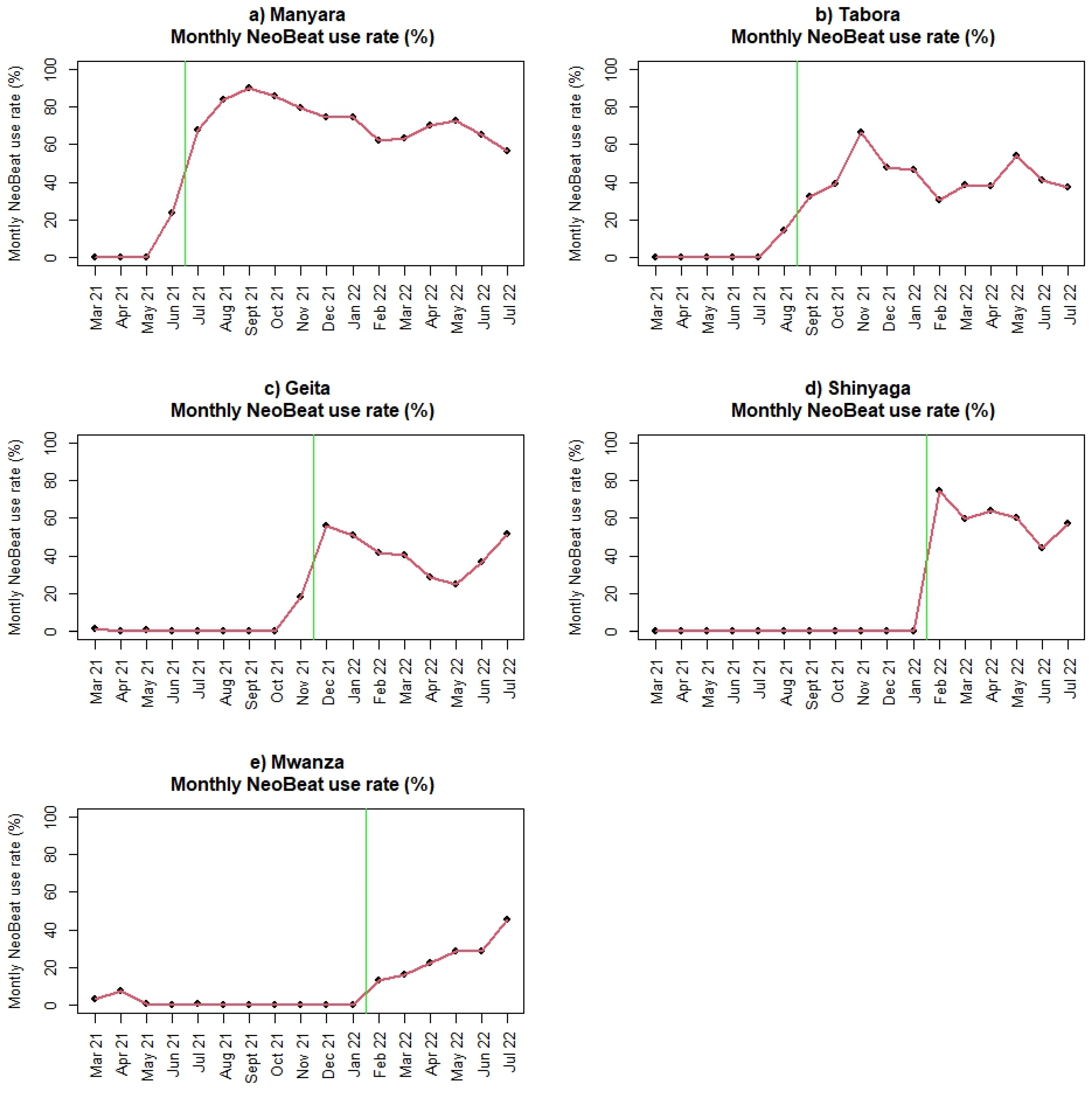
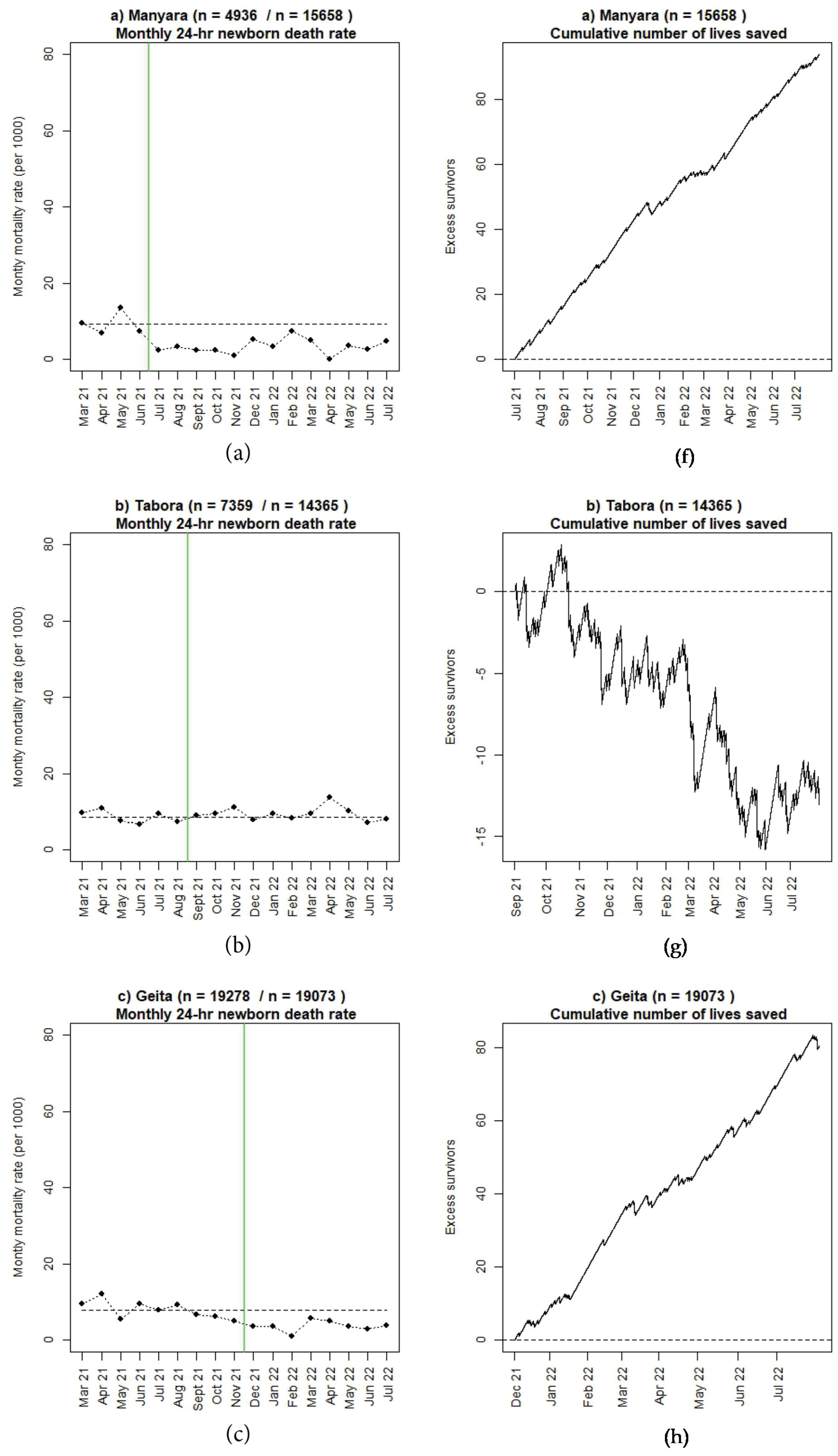
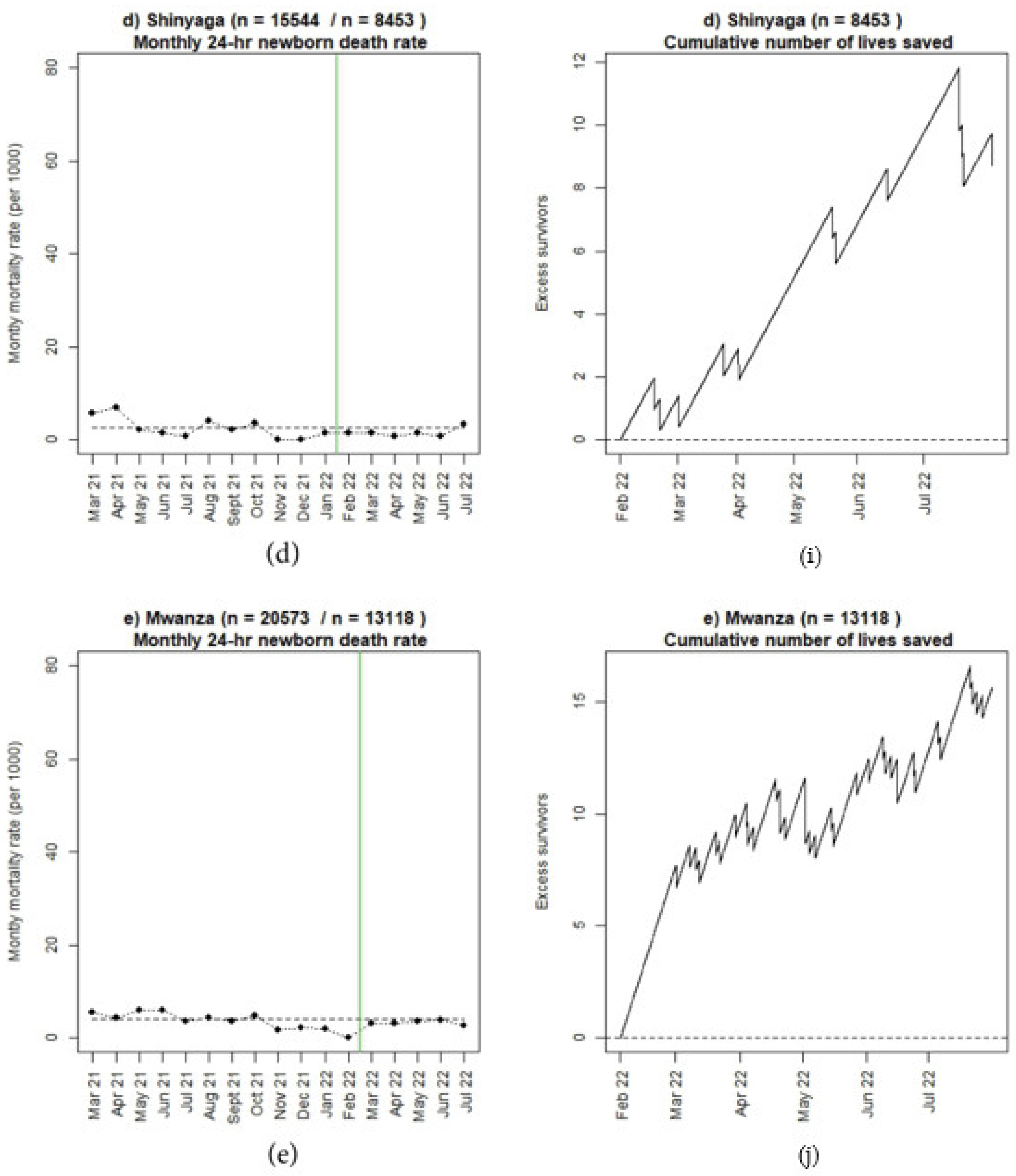
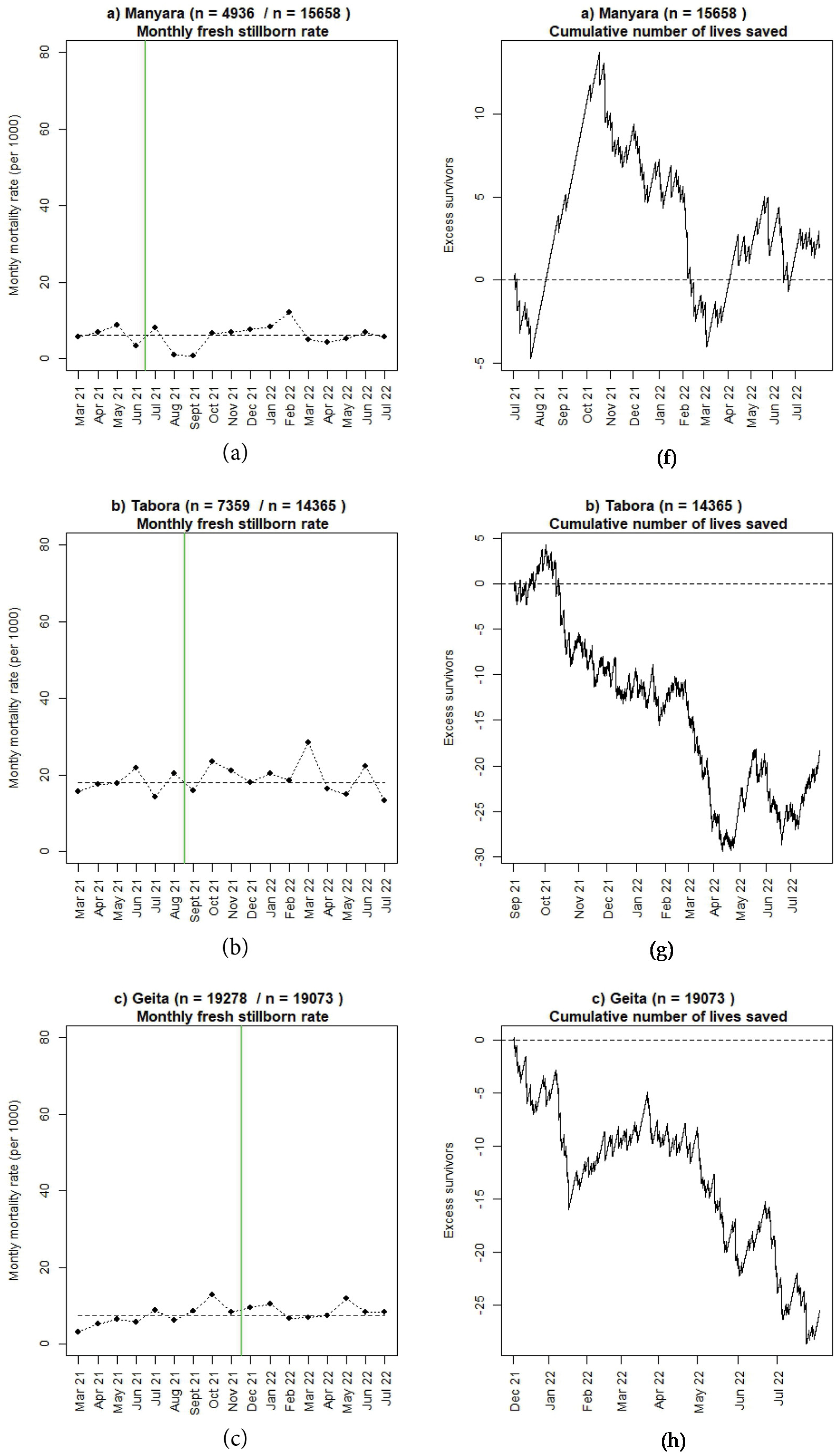
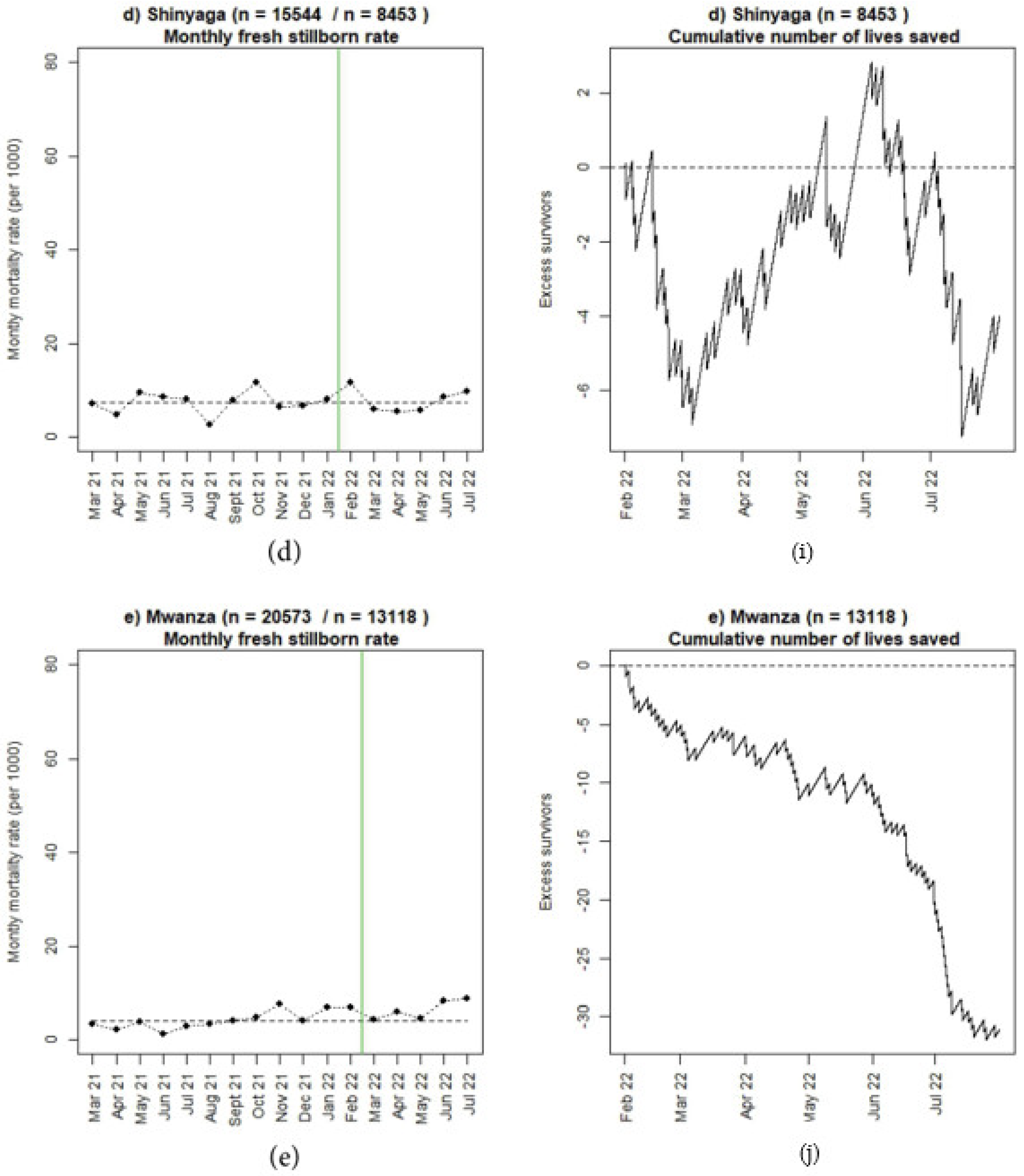
3.2. Perinatal Outcomes and Use of Moyo and NeoBeat
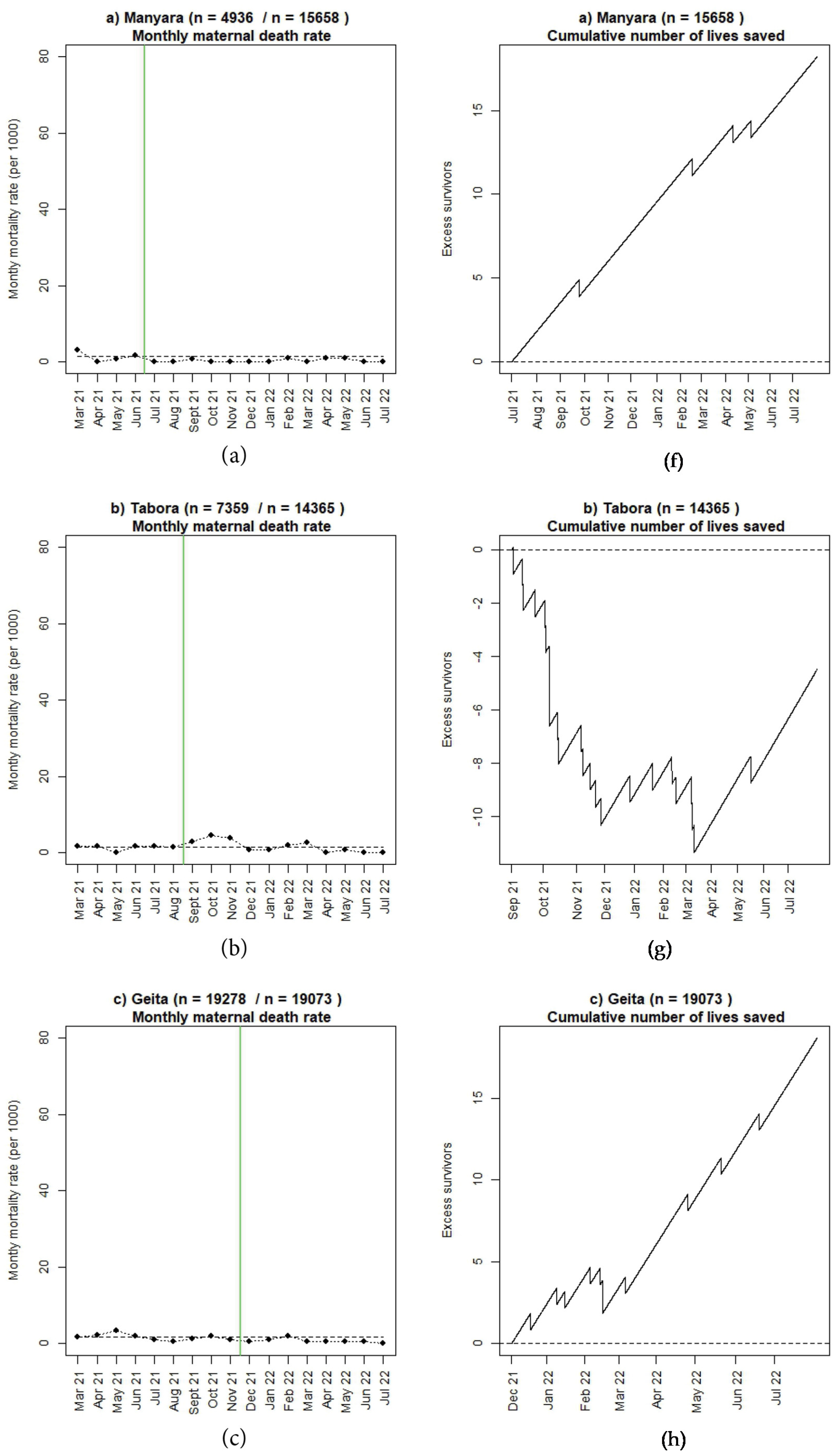
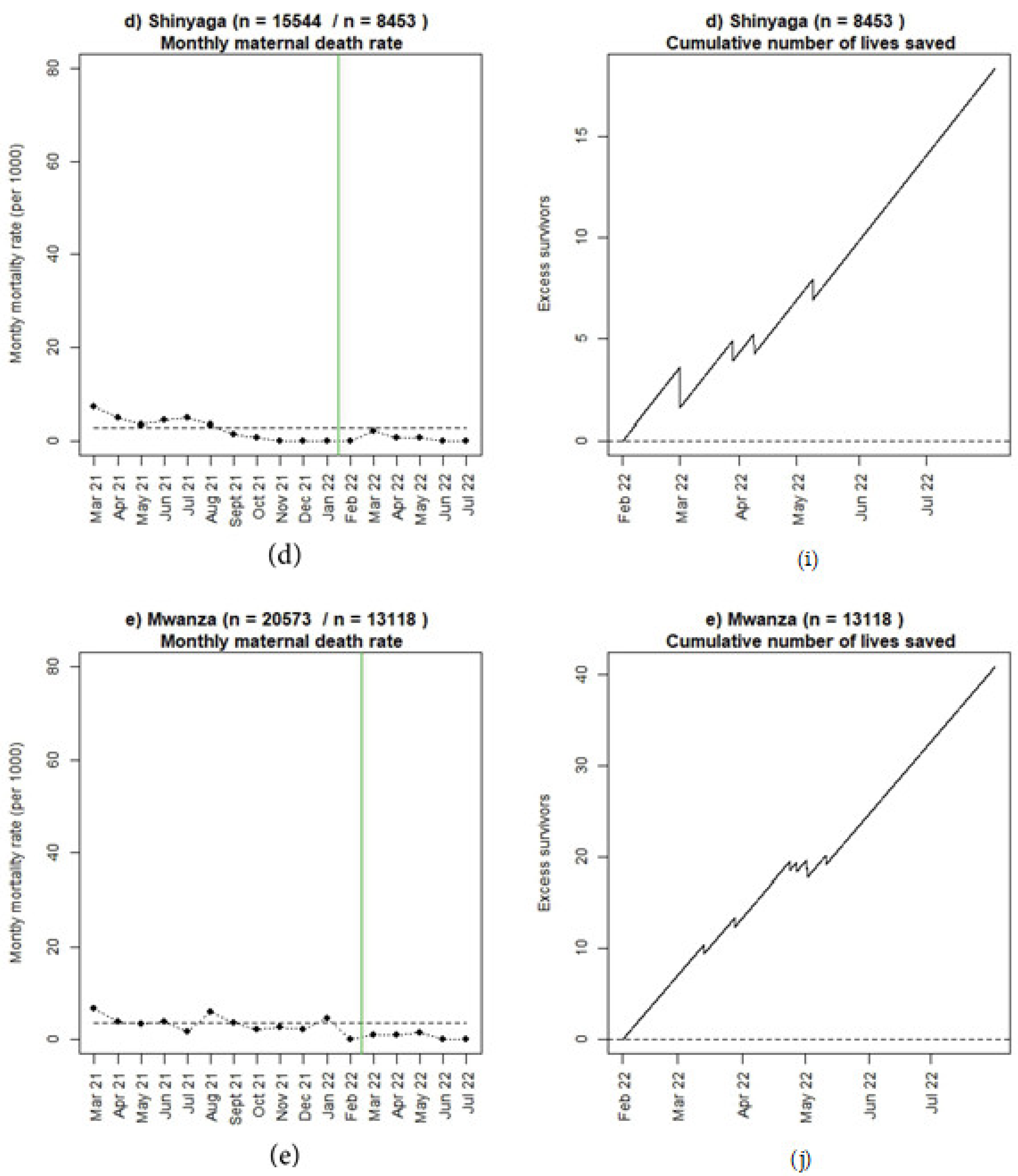
3.3. Maternal Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health (Dar es Salaam); Ministry of Health (Zanzibar); National Bureau of Statistics (Dar es Salaam); Office of the Chief Government Statistician (Zanzibar); ICF International (Rockville, Maryland, USA). Tanzania Demographic and Health Survey and Malaria Indicator Survey 2015–16—Key Indicators. 2016. Available online: http://www.nbs.go.tz/nbs/takwimu/dhs/2015-16_TDHS-MIS.pdf (accessed on 31 December 2022).
- Maternal Health. UNICEF. Maternal and Newborn Health. 2020. Available online: https://www.unicef.org/topics/maternal-health (accessed on 31 December 2022).
- Ministry of Health (Dar es Salaam); Ministry of Health (Zanzibar); National Bureau of Statistics (Dar es Salaam); Office of the Chief Government Statistician (Zanzibar); ICF (Rockville, Maryland, USA). Tanzania Demographic and Health Survey and Malaria Indicator Survey 2015–16. 2016. Available online: https://dhsprogram.com/pubs/pdf/FR321/FR321.pdf (accessed on 31 December 2022).
- United Nation Inter-Agency Group for Child Mortality Estimation Report. A Neglected Tragedy The global Burden of Stillbirths. 2020. Available online: https://www.unicef.org/media/84851/file/UN-IGME-the-global-burden-of-stillbirths-2020.pdf (accessed on 31 December 2022).
- United Nation Inter-Agency Group for Child Mortality Estimation Report. Levels and Trends in Child Mortality. 2021. Available online: https://data.unicef.org/resources/levels-and-trends-in-child-mortality/ (accessed on 31 December 2022).
- Ministry of Health and Social Welfare, Tanzania. The National Road Map Strategic Plan to Improve Reproductive, Maternal, Newborn, Child and Adolescent Health in Tanzania (2016–2020): One Plan II. 2016. Available online: https://www.prb.org/wp-content/uploads/2018/05/National-Road-Map-Strategic-Plan-to-Accelerate-Reduction-of-Maternal-Newborn-and-Child-Deaths-in-Tanzania-2016-2020-One-Plan-II.pdf (accessed on 31 December 2022).
- World Health Organization and UNICEF Report. Every Newborn: An Action Plan to End Preventable Deaths. 2014. Available online: https://www.healthynewbornnetwork.org/hnn-content/uploads/Every_Newborn_Action_Plan-ENGLISH_updated_July2014.pdf (accessed on 31 December 2022).
- Safer Births. Available online: https://saferbirths.com/ (accessed on 31 December 2022).
- Kamala, B.; Ersdal, H.L.; Mduma, E.R.; Moshiro, R.; Girnary, S.; Østrem, O.T.; Linde, J.; Dalen, I.; Søyland, E.; Bishanga, D.R.; et al. SaferBirths Bundle of Care Protocol: A stepped-wedge cluster implementation project in 30 public health-facilities in five regions, Tanzania. BMC Health Serv. Res. 2021, 21, 1117. [Google Scholar] [CrossRef] [PubMed]
- Lafontan, S.R.; Kidanto, H.L.; Ersdal, H.L.; Mbekenga, C.K.; Sundby, J. Perceptions and experiences of skilled birth attendants on using a newly developed strap-on electronic fetal heart rate monitor in Tanzania. BMC Pregnancy Childbirth 2019, 19, 165. [Google Scholar]
- Lafontan, S.R.; Sundby, J.; Ersdal, H.L.; Abeid, M.; Kidanto, H.L.; Mbekenga, C.K. “I was relieved to know that my baby was safe”: Women’s attitudes using an electronic fetal heart rate monitor during labor in Tanzania. A qualitative study. Int. J. Environ. Res. Public Health 2018, 15, 302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamala, B.A.; Kidanto, H.L.; Dalen, I.; Ngarina, M.N.; Abeid, M.S.; Perlman, J.M.; Ersdal, H.L. Effectiveness of a novel strap-on automatic Doppler (Moyo) versus intermittent Doppler in intrapartum detection of abnormal foetal heart rate: A randomized controlled study in Tanzania. Int. J. Environ. Res. Public Health 2019, 16, 315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rettedal, S.I.; Eilevstjønn, J.; Kibsgaard, A.; Kvaløy, J.T.; Ersdal, H.L. Comparison of heart rate feedback from dry-electrode ECG, 3-lead ECG and pulse oximetry during newborn resuscitation. Children 2021, 8, 1092. [Google Scholar] [CrossRef]
- Thallinger, M.; Ersdal, H.L.; Francis, F.; Yeconia, A.; Mduma, E.R.; Kidanto, H.L.; Linde, J.E.; Eilevstjønn, J.; Gunnes, N.; Størdal, K. Born not breathing: A randomised trial comparing two self-inflating bag-masks during newborn resuscitation in Tanzania. Resuscitation 2017, 116, 66–72. [Google Scholar] [CrossRef]
- Haynes, J.; Bjorland, P.; Gomo, Ø.; Ushakova, A.; Rettedal, S.; Perlman, J.M.; Ersdal, H.L. Novel neonatal simulator provides high-fidelity ventilation 2 training comparable to real-life newborn ventilation. Children 2021, 8, 940. [Google Scholar] [CrossRef]
- Chang, C.; Perlman, J.M.; Abramson, E. Use of Novel Manikin for Neonatal Resuscitation Ventilation Training. Children 2022, 9, 364. [Google Scholar] [CrossRef]
- Nelissen, E.; Ersdal, H.L.; Mduma, E.R.; Evjen-Olsen, B.; Twisk, J.; Broerse, J.; van Roosmalen, J.; Stekelenburg, J. Clinical performance and patient outcome after simulation-based training in prevention and management of postpartum haemorrhage: An educational intervention study in a low-resource setting. BMC Pregnancy Childbirth 2017, 17, 301. [Google Scholar] [CrossRef]
- Vadla, M.S.; Mdoe, P.; Moshiro, R.; Haug, I.A.; Gomo, Ø.; Kvaløy, J.T.; Oftedal, B.; Ersdal, H.L. Neonatal resuscitation skill-training using a new neonatal simulator, facilitated by local motivators; a 2-year prospective observational study of 9000 trainings. Children 2022, 9, 134. [Google Scholar] [CrossRef]
- Vadla, M.S.; Moshiro, R.; Mdoe, P.; Eilevstjønn, J.; Kvaløy, J.T.; Hhoki, B.H.; Ersdal, H.L. In-situ newborn resuscitation simulation-based skill-training and changes in clinical performance and perinatal outcomes: Clinical observational study of 10,481 births. Adv. Sim. 2022, 7, 38. [Google Scholar] [CrossRef]
- Mduma, E.R.; Kvaløy, J.T.; Søreide, E.; Svensen, E.; Mdoe, P.; Perlman, J.M.; Johnson, C.; Kidanto, H.L.; Ersdal, H.L. Frequent Refresher Newborn Resuscitation Training Improves Perinatal Outcome Over time in a rural Tanzanian hospital. BMJ Open 2019, 9, e030572. [Google Scholar] [CrossRef] [Green Version]
- Helping Mothers Survive Programs, Jhpiego. Available online: https://hms.jhpiego.org/bleeding-after-birth-complete/ (accessed on 31 December 2022).
- Helping Babies Survive Programs, American Academy of Pediatrics. Available online: https://www.aap.org/en/aap-global/helping-babies-survive/#:~:text=Helping%20Babies%20Survive%20is%20a,care%20to%20newborns%20after%20birth (accessed on 31 December 2022).
- Lovegrove, J.; Valencia, O.; Treasure, T.; Sherlaw-Johnsom, C.; Gallivan, S. Monitoring the results of cardiac surgery by variable life-adjusted display. Lancet 1997, 350, 1128–1130. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing, Version 4.2.2; R Foundation for Statistical Computing: Vienna, Austria, 2022. Available online: https://www.R-project.org/ (accessed on 31 December 2022).
- Ersdal, H.L.; Eilevstjønn, J.; Linde, J.; Yeconia, A.; Mduma, E.R.; Kidanto, H.L.; Perlman, J.M. Fresh Stillbirths and Severely Asphyxiated Neonates Represent a Common Hypoxic-ischemic Pathway. Int. J. Gynecol. Obstet. 2018, 141, 171–180. [Google Scholar] [CrossRef]
- Moshiro, R.; Perlman, J.M.; Kidanto, H.-L.; Kvaloy, J.T.; Mdoe, P.; Ersdal, H.L. Predictors of death including quality of positive pressure ventilation during newborn resuscitation and the relationship to outcome at seven days in a rural Tanzanian hospital. PLoS ONE 2018, 13, e0202641. [Google Scholar]
- Ersdal, H.L.; Mduma, E.R.; Svensen, E.; Sundby, J.; Perlman, J.M. Intermittent Detection of Fetal Heart Rate Abnormalities Identify Infants at Greatest Risk for Fresh Stillbirths, Birth Asphyxia, Neonatal Resuscitation, and Early Neonatal Deaths in a Resource Limited Setting. Neonatology 2012, 102, 235–242. [Google Scholar] [CrossRef]
- Bogren, M.; Denovan, A.; Kent, F.; Berg, M.; Linden, K. Impact of the Helping Mothers Survive Bleeding After Birth learning programme on care provider skills and maternal health outcomes in low-income countries—An integrative review. Women Birth 2021, 34, 425–434. [Google Scholar] [CrossRef]
- Litorp, H.; Mgaya, A.; Mbekenga, C.K.; Kidanto, H.L.; Johnsdotter, S.; Essén, B. Fear, blame and transparency: Obstetric caregivers’ rationales for high caesarean section rates in a low-resource setting. Soc. Sci. Med. 2015, 143, 232–240. [Google Scholar] [CrossRef]
- Rumisha, S.F.; Lyimo, E.P.; Mremi, I.R.; Tungu, P.K.; Mwingira, V.S.; Mbata, D.; Malekia, S.E.; Joachim, C.; Mboera, L.E.G. Data quality of the routine health management information system at the primary healthcare facility and district levels in Tanzania. BMC Med. Inform. Decis. Mak. 2020, 20, 340. [Google Scholar] [CrossRef]
- Målqvist, M.; Eriksson, L.; Nga, N.T.; Fagerland, L.I.; Hoa, D.P.; Wallin, L.; Ewald, U.; Persson, L.-Å. Unreported births and deaths, a severe obstacle for improved neonatal survival in low-income countries. BMC Int. Health Hum. Rights 2008, 8, 4. [Google Scholar] [CrossRef] [Green Version]
- Estifanos, A.S.; Gezahegn, R.; Keraga, D.W.; Kifle, A.; Procureur, F.; Hill, Z. ‘The false reporter will get a praise and the one who reported truth will be discouraged’: A qualitative study on intentional data falsification by frontline maternal and newborn healthcare workers in two regions in Ethiopia. BMJ Glob. Health 2022, 7, e008260. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Manyara | Tabora | Geita | Shinyanga | Mwanza | |
|---|---|---|---|---|---|
| Time period | 01.03.21– 30.06.21 | 01.03.21– 31.08.21 | 01.03.21– 30.11.21 | 01.03.21– 31.01.22 | 01.03.21– 31.02.22 |
| Months of baseline | 4 | 6 | 9 | 11 | 12 |
| Deliveries (n) | 4 936 | 7 359 | 19 278 | 15 544 | 20 573 |
| Referred in labour from other facility | 2.1 (104) | 12.7 (935) | 0.8 (162) | 6.8 (1053) | 1.8 (367) |
| Maternal age (years) | 24 (20,30) | 24 (20,30) | 24 (20,30) | 24 (20,30) | 25 (21,30) |
| Parity (n) | 1 (0,3) | 2 (0,4) | 2 (1,4) | 1 (0,3) | 1 (0,3) |
| Newborn birthweight (grams) | 3100 (2900,3500) | 3100 (2800,3500) | 3200 (2900,3500) | 3200 (2900,3500) | 3000 (2700,3300) |
| Fetal heart rate on admission | |||||
| Abnormal (<110/>160 bpm) | 0.9 (46) | 0.9 (64) | 0.2 (30) | 0.3 (46) | 0.2 (49) |
| Not detectable | 1.2 (59) | 3.2 (238) | 1.3 (245) | 1.4 (220) | 1.6 (332) |
| Not recorded | 9.9 (488) | 9.2 (678) | 16.2 (3113) | 10.2 (1590) | 19.3 (3957) |
| Fetal heart rate during labour | |||||
| Abnormal (<110/>160 bpm) | 0.5 (25) | 0.9 (64) | 0.1 (28) | 0.1 (21) | 0.4 (71) |
| Not detectable | 0.9 (44) | 2.4 (178) | 1.0 (187) | 1.2 (186) | 1.0 (201) |
| Not measured/recorded | 34.9 (1726) | 27.1 (1991) | 25.9 (4993) | 13.9 (2155) | 26.5 (5461) |
| Moyo used | 7.1 (348) | 1.9 (138) | 1.0 (201) | 0 (0) | 0 (6) |
| Newborn Resuscitation | |||||
| Stimulation/suction | 13.7 (677) | 22.0 (1625) | 9.1 (1760) | 10.8 (1673) | 19.9 (4096) |
| Bag-mask ventilation | 4.2 (204) | 9.0 (671) | 2.5 (490) | 4.3 (675) | 4.7 (972) |
| NeoBeat used | 0.7 (37) | 0.5 (37) | 0.2 (38) | 0 (0) | 0.2 (49) |
| Perinatal outcomes | |||||
| Newborn deaths (24-h) | 0.9 (46) | 0.9 (63) | 0.8 (151) | 0.3 (40) | 0.4 (81) |
| Fresh stillbirths | 0.6 (30) | 1.8 (132) | 0.7 (141) | 0.7 (114) | 0.4 (83) |
| Maternal deaths | 0.1 (7) | 0.1 (10) | 0.2 (30) | 0.3 (43) | 0.4 (75) |
| Maternal near miss | 0.1 (4) | 0.1 (9) | 0.1 (13) | 0.1 (18) | 0.2 (34) |
| Manyara | Tabora | Geita | Shinyanga | Mwanza | |
|---|---|---|---|---|---|
| Time period | 01.07.21– 31.07.22 | 01.09.21– 31.07.22 | 01.12.21– 31.07.22 | 01.02.22– 31.07.22 | 01.03.22– 31.07.22 |
| Months of implementation | 13 | 11 | 8 | 6 | 5 |
| Deliveries (n) | 15 658 | 14 365 | 19 073 | 8 453 | 13 118 |
| Referred in labour from other facility | 1.8 (277) | 12.9 (1859) | 1.0 (195) | 4.5 (384) | 1.6 (211) |
| Maternal age (years) | 25 (21,30) | 24 (20,30) | 24 (20,30) | 25 (20,30) | 25 (21,30) |
| Parity (n) | 1 (0,3) | 2 (0,4) | 2 (0,4) | 1 (0,3) | 1 (0,3) |
| Newborn birthweight (grams) | 3200 (2900,3500) | 3200 (2900,3500) | 3200 (2800,3500) | 3200 (2900,3500) | 3000 (2700,3400) |
| Fetal heart rate on admission | |||||
| Abnormal (<110/>160 bpm) | 1.8 (285) | 1.6 (223) | 0.3 (64) | 0.5 (42) | 0.7 (94) |
| Not detectable | 1.0 (152) | 3.0 (436) | 1.5 (287) | 1.6 (137) | 1.6 (210) |
| Not recorded | 5.7 (900) | 8.7 (1260) | 19.2 (3653) | 17.8 (1502) | 10.9 (1432) |
| Fetal heart rate during labour | |||||
| Abnormal (<110/>160 bpm) | 1.0 (154) | 1.1 (152) | 0.2 (44) | 0.4 (32) | 0.5 (70) |
| Not detectable | 0.8 (131) | 2.2 (320) | 1.3 (252) | 1.7 (144) | 1.2 (155) |
| Not recorded | 23.1 (3615) | 15.9 (2283) | 27.6 (5275) | 11.4 (963) | 12.3 (1617) |
| Moyo used | 65.7 (10,280) | 35.5 (5094) | 20.0 (3814) | 44.2 (3732) | 35.9 (4712) |
| Newborn Resuscitation | |||||
| Stimulation/suction | 12.9 (2022) | 10.5 (1506) | 6.6 (1268) | 8.8 (744) | 12.8 (1678) |
| Bag-mask ventilation | 3.9 (622) | 6.0 (861) | 3.6 (687) | 5.0 (426) | 4.7 (621) |
| NeoBeat used | 9.6 (1498) | 4.6 (683) | 2.9 (555) | 5.6 (471) | 4.2 (556) |
| Perinatal outcomes | |||||
| Newborn deaths (24-h) | 0.3 (52) | 0.9 (136) | 0.4 (69) | 0.2 (13) | 0.3 (36) |
| Fresh stillbirths | 0.6 (93) | 1.9 (276) | 0.9 (165) | 0.8 (66) | 0.6 (84) |
| Maternal deaths | 0 (4) | 0.2 (24) | 0.1 (11) | 0.1 (5) | 0.1 (7) |
| Maternal near miss | 0.1 (18) | 0.6 (80) | 0.1 (14) | 0.3 (28) | 0.3 (37) |
| Manyara | Baseline n = 4936 | After start SBBC n = 15,658 | ||||
|---|---|---|---|---|---|---|
| Alive n = 4860 | Dead n = 46 | FSB n = 30 | Alive n = 15,513 | Dead n = 52 | FSB n = 93 | |
| Source of admission | ||||||
| From antenatal care/maternity ward | 1.4 (69) | 2.2 (1) | 3.3 (1) | 5.2 (811) | 9.6 (5) | 4.3 (4) |
| From home | 82.0 (3986) | 73.9 (34) | 73.3 (22) | 79.4 (12,318) | 75.0 (39) | 76.3 (71) |
| Referred from other facility | 2.0 (99) | 8.7 (4) | 3.3 (1) | 1.7 (266) | 0 (0) | 11.8 (11) |
| Not recorded | 14.5 (706) | 15.2 (7) | 20.0 (6) | 13.7 (2118) | 15.4 (8) | 7.5 (7) |
| Fetal heart rate on admission | ||||||
| Abnormal (<110/>160 bpm) | 0.9 (45) | 2.2 (1) | 0 (0) | 1.7 (268) | 9.6 (5) | 12.9 (12) |
| Not detectable | 0.7 (35) | 21.7 (10) | 46.7 (14) | 0.8 (121) | 3.8 (2) | 31.2 (29) |
| Not measured and/or recorded | 9.8 (476) | 19.6 (9) | 10.0 (3) | 5.7 (883) | 11.5 (6) | 11.9 (11) |
| Use of new devices | ||||||
| Moyo | 7.1 (346) | 2.2 (1) | 3.3 (1) | 65.7 (10,193) | 63.5 (33) | 58.1 (54) |
| NeoBeat | 0.7 (35) | 4.3 (2) | 0 (0) | 9.4 (1456) | 69.2 (36) | 6.5 (6) |
| Bag-mask ventilation | 3.8 (185) | 34.8 (16) | 10.0 (3) | 3.7 (575) | 78.8 (41) | 6.5 (6) |
| Tabora | Baseline n = 7359 | After start SBBC n = 14,365 | ||||
| Alive n = 7164 | Dead n = 63 | FSB n = 132 | Alive n = 13,953 | Dead n = 136 | FSB n = 276 | |
| Source of admission | ||||||
| From antenatal care/maternity ward | 5.1 (362) | 1.6 (1) | 3.0 (4) | 1.0 (139) | 0.7 (1) | 0.7 (1) |
| From home | 82.2 (5890) | 74.6 (47) | 55.3 (73) | 86.1 (12,015) | 80.1 (109) | 57.6 (159) |
| Referred from other facility | 12.1 (867) | 23.8 (15) | 40.2 (53) | 12.3 (1721) | 17.6 (24) | 41.3 (114) |
| Not recorded | 0.6 (45) | 0 (0) | 1.5 (2) | 0.6 (78) | 1.5 (2) | 0.4 (1) |
| Fetal heart rate on admission | ||||||
| Abnormal (<110/>160 bpm) | 0.9 (62) | 1.6 (1) | 0.8 (1) | 1.4 (196) | 5.9 (8) | 6.9 (19) |
| Not detectable | 2.2 (159) | 19.0 (12) | 50.8 (67) | 2.2 (305) | 6.6 (9) | 44.2 (122) |
| Not measured and/or recorded | 8.9 (634) | 14.3 (9) | 9.9 (13) | 8.7 (1218) | 10.3 (14) | 10.1 (28) |
| Use of new devices | ||||||
| Moyo | 1.9 (135) | 3.2 (2) | 0.8 (1) | 35.4 (4946) | 27.2 (37) | 40.2 (111) |
| NeoBeat | 0.5 (34) | 3.2 (2) | 0.8 (1) | 4.1 (568) | 72.1 (98) | 6.2 (17) |
| Bag-mask ventilation | 8.6 (613) | 63.5 (40) | 12.9 (17) | 5.2 (721) | 83.8 (114) | 9.4 (26) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ersdal, H.; Mdoe, P.; Mduma, E.; Moshiro, R.; Guga, G.; Kvaløy, J.T.; Bundala, F.; Marwa, B.; Kamala, B. “Safer Births Bundle of Care” Implementation and Perinatal Impact at 30 Hospitals in Tanzania—Halfway Evaluation. Children 2023, 10, 255. https://doi.org/10.3390/children10020255
Ersdal H, Mdoe P, Mduma E, Moshiro R, Guga G, Kvaløy JT, Bundala F, Marwa B, Kamala B. “Safer Births Bundle of Care” Implementation and Perinatal Impact at 30 Hospitals in Tanzania—Halfway Evaluation. Children. 2023; 10(2):255. https://doi.org/10.3390/children10020255
Chicago/Turabian StyleErsdal, Hege, Paschal Mdoe, Estomih Mduma, Robert Moshiro, Godfrey Guga, Jan Terje Kvaløy, Felix Bundala, Boniphace Marwa, and Benjamin Kamala. 2023. "“Safer Births Bundle of Care” Implementation and Perinatal Impact at 30 Hospitals in Tanzania—Halfway Evaluation" Children 10, no. 2: 255. https://doi.org/10.3390/children10020255