
Not Every Dyspepsia Is Related to Helicobacter pylori—A Case of Esophageal Inlet Patch in a Female Teenager
 , ,
, , {kind=link}
Abstract
:1. Introduction
2. Case Report
2.1. Presenting Concerns
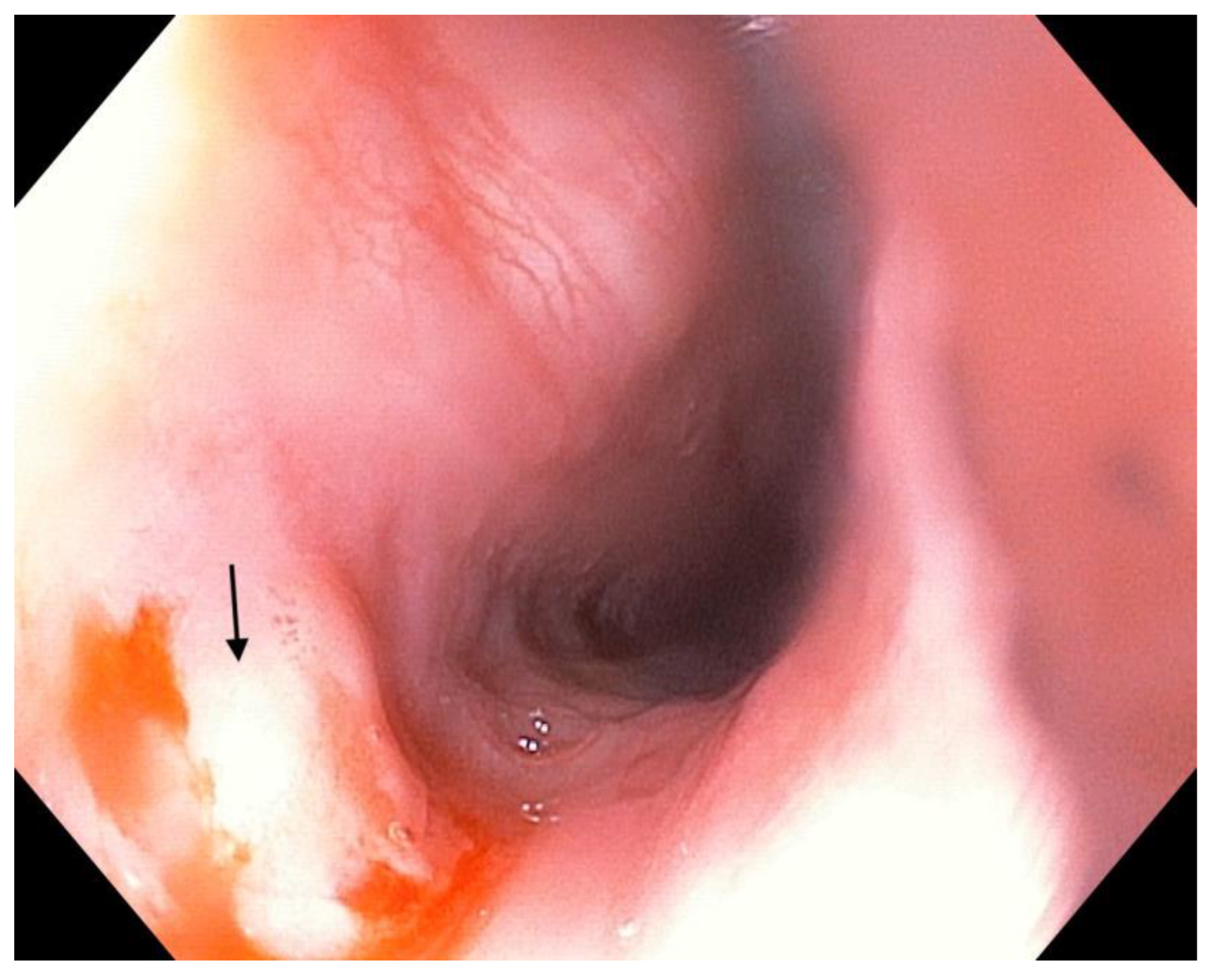
2.2. Clinical Findings
2.3. Diagnostic Focus and Assessment
2.4. Therapeutic Focus and Follow-Up
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mărginean, C.D.; Mărginean, C.O.; Meliț, L.E. Helicobacter Pylori-Related Extraintestinal Manifestations-Myth or Reality. Children 2022, 9, 1352. [Google Scholar] [CrossRef]
- McGuire, S. World Cancer Report 2014. Geneva, Switzerland: World Health Organization, International Agency for Research on Cancer, WHO Press, 2015. Adv. Nutr. 2016, 7, 418–419. [Google Scholar] [CrossRef] [Green Version]
- Robinson, K.; Atherton, J.C. The Spectrum of Helicobacter-Mediated Diseases. Annu. Rev. Pathol. 2021, 16, 123–144. [Google Scholar] [CrossRef]
- Meliţ, L.E.; Mărginean, M.O.; Mocan, S.; Mărginean, C.O. The Usefulness of Inflammatory Biomarkers in Diagnosing Child and Adolescent’s Gastritis: STROBE Compliant Article. Medicine 2019, 98, e16188. [Google Scholar] [CrossRef]
- Rosu, O.-M.; Gimiga, N.; Stefanescu, G.; Anton, C.; Paduraru, G.; Tataranu, E.; Balan, G.G.; Diaconescu, S. Helicobacter Pylori Infection in a Pediatric Population from Romania: Risk Factors, Clinical and Endoscopic Features and Treatment Compliance. J. Clin. Med. 2022, 11, 2432. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter Pylori Infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [Green Version]
- Săsăran, M.O.; Meliț, L.E.; Mocan, S.; Ghiga, D.V.; Dobru, E.D. Pediatric Gastritis and Its Impact on Hematologic Parameters. Medicine 2020, 99, e21985. [Google Scholar] [CrossRef]
- Keely, S.; Walker, M.M.; Marks, E.; Talley, N.J. Immune Dysregulation in the Functional Gastrointestinal Disorders. Eur. J. Clin. Investig. 2015, 45, 1350–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madisch, A.; Andresen, V.; Enck, P.; Labenz, J.; Frieling, T.; Schemann, M. The Diagnosis and Treatment of Functional Dyspepsia. Dtsch. Arztebl. Int. 2018, 115, 222–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, J.; Wang, J.; Wang, Y.; Zhang, C.; Hu, G.; Wang, Z. External Treatment of Traditional Chinese Medicine for Functional Dyspepsia in Children: Protocol for a Systematic Review and Network Meta-Analysis. Medicine 2022, 101, e31597. [Google Scholar] [CrossRef]
- Wei, Z.; Yang, X.; Xing, X.; Dong, L.; Wang, J.; Qin, B. Risk Factors Associated with Functional Dyspepsia in Chinese Children: A Cross-Sectional Study. BMC Gastroenterol. 2021, 21, 218. [Google Scholar] [CrossRef] [PubMed]
- Ciocalteu, A.; Popa, P.; Ionescu, M.; Gheonea, D.I. Issues and Controversies in Esophageal Inlet Patch. World J Gastroenterol. 2019, 25, 4061–4073. [Google Scholar] [CrossRef] [PubMed]
- Tang, P.; McKinley, M.J.; Sporrer, M.; Kahn, E. Inlet Patch: Prevalence, Histologic Type, and Association with Esophagitis, Barrett Esophagus, and Antritis. Arch. Pathol. Lab. Med. 2004, 128, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Avidan, B.; Sonnenberg, A.; Chejfec, G.; Schnell, T.G.; Sontag, S.J. Is There a Link between Cervical Inlet Patch and Barrett’s Esophagus? Gastrointest. Endosc. 2001, 53, 717–721. [Google Scholar] [CrossRef]
- von Rahden, B.H.A.; Stein, H.J.; Becker, K.; Liebermann-Meffert, D.; Siewert, J.R. Heterotopic Gastric Mucosa of the Esophagus: Literature-Review and Proposal of a Clinicopathologic Classification. Am. J. Gastroenterol. 2004, 99, 543–551. [Google Scholar] [CrossRef]
- Truong, L.D.; Stroehlein, J.R.; McKechnie, J.C. Gastric Heterotopia of the Proximal Esophagus: A Report of Four Cases Detected by Endoscopy and Review of Literature. Am. J. Gastroenterol. 1986, 81, 1162–1166. [Google Scholar]
- Peitz, U.; Vieth, M.; Evert, M.; Arand, J.; Roessner, A.; Malfertheiner, P. The Prevalence of Gastric Heterotopia of the Proximal Esophagus Is Underestimated, but Preneoplasia Is Rare—Correlation with Barrett’s Esophagus. BMC Gastroenterol. 2017, 17, 87. [Google Scholar] [CrossRef]
- Chong, V.H. Clinical Significance of Heterotopic Gastric Mucosal Patch of the Proximal Esophagus. World J. Gastroenterol. 2013, 19, 331–338. [Google Scholar] [CrossRef]
- Mărginean, C.O.; Meliț, L.E.; Săsăran, M.O. Traditional and Modern Diagnostic Approaches in Diagnosing Pediatric Helicobacter Pylori Infection. Children 2022, 9, 994. [Google Scholar] [CrossRef]
- Özgür, T.; Özkan, T.B.; Erdemir, G.; Özakın, C.; Yerci, Ö. The Diagnostic Value of Endoscopic Narrow Band Imaging in Helicobacter Pylori Gastritis in Children. Turk. J. Gastroenterol. 2015, 26, 112–116. [Google Scholar] [CrossRef] [Green Version]
- Alaboudy, A.A.; Elbahrawy, A.; Matsumoto, S.; Yoshizawa, A. Conventional Narrow-Band Imaging Has Good Correlation with Histopathological Severity of Helicobacter Pylori Gastritis. Dig. Dis. Sci. 2011, 56, 1127–1130. [Google Scholar] [CrossRef]
- Maconi, G.; Pace, F.; Vago, L.; Carsana, L.; Bargiggia, S.; Bianchi Porro, G. Prevalence and Clinical Features of Heterotopic Gastric Mucosa in the Upper Oesophagus (Inlet Patch). Eur. J. Gastroenterol. Hepatol. 2000, 12, 745–749. [Google Scholar] [CrossRef]
- Feurle, G.E.; Helmstaedter, V.; Buehring, A.; Bettendorf, U.; Eckardt, V.F. Distinct Immunohistochemical Findings in Columnar Epithelium of Esophageal Inlet Patch and of Barrett’s Esophagus. Dig. Dis. Sci. 1990, 35, 86–92. [Google Scholar] [CrossRef]
- Meining, A.; Bajbouj, M. Erupted Cysts in the Cervical Esophagus Result in Gastric Inlet Patches. Gastrointest. Endosc. 2010, 72, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Alagozlu, H.; Simsek, Z.; Unal, S.; Cindoruk, M.; Dumlu, S.; Dursun, A. Is There an Association between Helicobacter Pylori in the Inlet Patch and Globus Sensation? World J. Gastroenterol. 2010, 16, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Neumann, W.L.; Luján, G.M.; Genta, R.M. Gastric Heterotopia in the Proximal Oesophagus (“inlet Patch”): Association with Adenocarcinomas Arising in Barrett Mucosa. Dig. Liver Dis. 2012, 44, 292–296. [Google Scholar] [CrossRef]
- Takeji, H.; Ueno, J.; Nishitani, H. Ectopic Gastric Mucosa in the Upper Esophagus: Prevalence and Radiologic Findings. AJR Am. J. Roentgenol. 1995, 164, 901–904. [Google Scholar] [CrossRef] [Green Version]
- Hori, K.; Kim, Y.; Sakurai, J.; Watari, J.; Tomita, T.; Oshima, T.; Kondo, C.; Matsumoto, T.; Miwa, H. Non-Erosive Reflux Disease Rather than Cervical Inlet Patch Involves Globus. J. Gastroenterol. 2010, 45, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Wlaź, J.; Mądro, A.; Kaźmierak, W.; Celiński, K.; Słomka, M. Pancreatic and Gastric Heterotopy in the Gastrointestinal Tract. Postepy Hig. Med. Dosw. 2014, 68, 1069–1075. [Google Scholar] [CrossRef]
- Polat, F.R.; Polat, S. The Effect of Helicobacter Pylori on Gastroesophageal Reflux Disease. JSLS 2012, 16, 260–263. [Google Scholar] [CrossRef] [Green Version]
- Ghoshal, U.C.; Chourasia, D. Gastroesophageal Reflux Disease and Helicobacter Pylori: What May Be the Relationship? J. Neurogastroenterol. Motil. 2010, 16, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Wüppenhorst, N.; Viebahn, B.; Theile, A.; Radü, H.J.; Kist, M. Culture and Successful Eradication of Helicobacter Pylori from Heterotopic Gastric Mucosa. Z. Gastroenterol. 2012, 50, 677–679. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, O.; Akamatsu, T.; Cardona, H.; Graham, D.Y.; El-Zimaity, H.M.T. Helicobacter Pylori and Hetertopic Gastric Mucosa in the Upper Esophagus (the Inlet Patch). Am. J. Gastroenterol. 2003, 98, 1266–1270. [Google Scholar] [CrossRef] [PubMed]
- Lauwers, G.Y.; Mino, M.; Ban, S.; Forcione, D.; Eatherton, D.E.; Shimizu, M.; Sevestre, H. Cytokeratins 7 and 20 and Mucin Core Protein Expression in Esophageal Cervical Inlet Patch. Am. J. Surg. Pathol. 2005, 29, 437–442. [Google Scholar] [CrossRef]
- Korkut, E.; Bektaş, M.; Alkan, M.; Ustün, Y.; Meco, C.; Ozden, A.; Soykan, I. Esophageal Motility and 24-h PH Profiles of Patients with Heterotopic Gastric Mucosa in the Cervical Esophagus. Eur. J. Intern. Med. 2010, 21, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Rosztóczy, A.; Izbéki, F.; Németh, I.B.; Dulic, S.; Vadászi, K.; Róka, R.; Gecse, K.; Gyökeres, T.; Lázár, G.; Tiszlavicz, L.; et al. Detailed Esophageal Function and Morphological Analysis Shows High Prevalence of Gastroesophageal Reflux Disease and Barrett’s Esophagus in Patients with Cervical Inlet Patch. Dis. Esophagus 2012, 25, 498–504. [Google Scholar] [CrossRef] [Green Version]
- Talih, T.; Arslan, E.; Talih, G.; Sipahi, M. Inlet Patch Mimicking Unstable Angina Pectoris. Turk. J. Surg. 2020, 36, 229–232. [Google Scholar] [CrossRef]
- Malhi-Chowla, N.; Ringley, R.K.; Wolfsen, H.C. Gastric Metaplasia of the Proximal Esophagus Associated with Esophageal Adenocarcinoma and Barrett’s Esophagus: What Is the Connection? Inlet Patch Revisited. Dig Dis 2000, 18, 183–185. [Google Scholar] [CrossRef]
- Rusu, R.; Ishaq, S.; Wong, T.; Dunn, J.M. Cervical Inlet Patch: New Insights into Diagnosis and Endoscopic Therapy. Frontline Gastroenterol. 2018, 9, 214–220. [Google Scholar] [CrossRef]
- Meining, A.; Bajbouj, M. Gastric Inlet Patches in the Cervical Esophagus: What They Are, What They Cause, and How They Can Be Treated. Gastrointest. Endosc. 2016, 84, 1027–1029. [Google Scholar] [CrossRef] [Green Version]
- Bajbouj, M.; Becker, V.; Eckel, F.; Miehlke, S.; Pech, O.; Prinz, C.; Schmid, R.M.; Meining, A. Argon Plasma Coagulation of Cervical Heterotopic Gastric Mucosa as an Alternative Treatment for Globus Sensations. Gastroenterology 2009, 137, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Klare, P.; Meining, A.; von Delius, S.; Wolf, P.; Konukiewitz, B.; Schmid, R.M.; Bajbouj, M. Argon Plasma Coagulation of Gastric Inlet Patches for the Treatment of Globus Sensation: It Is an Effective Therapy in the Long Term. Digestion 2013, 88, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Kadota, T.; Fujii, S.; Oono, Y.; Imajoh, M.; Yano, T.; Kaneko, K. Adenocarcinoma Arising from Heterotopic Gastric Mucosa in the Cervical Esophagus and Upper Thoracic Esophagus: Two Case Reports and Literature Review. Expert Rev. Gastroenterol. Hepatol. 2016, 10, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Cartabuke, R.H.; Thota, P.N. High-Grade Dysplasia in Thoracic Inlet Patch Treated by Focal Endoscopic Mucosal Resection and Radiofrequency Ablation. Gastrointest. Endosc. 2015, 81, 1297–1298. [Google Scholar] [CrossRef] [PubMed]
- Dunn, J.M.; Sui, G.; Anggiansah, A.; Wong, T. Radiofrequency Ablation of Symptomatic Cervical Inlet Patch Using a Through-the-Scope Device: A Pilot Study. Gastrointest. Endosc. 2016, 84, 1022–1026.e2. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meliț, L.E.; Dincă, A.L.; Borka Balas, R.; Mocanu, S.; Mărginean, C.O. Not Every Dyspepsia Is Related to Helicobacter pylori—A Case of Esophageal Inlet Patch in a Female Teenager. Children 2023, 10, 229. https://doi.org/10.3390/children10020229
Meliț LE, Dincă AL, Borka Balas R, Mocanu S, Mărginean CO. Not Every Dyspepsia Is Related to Helicobacter pylori—A Case of Esophageal Inlet Patch in a Female Teenager. Children. 2023; 10(2):229. https://doi.org/10.3390/children10020229
Chicago/Turabian StyleMeliț, Lorena Elena, Andreea Ligia Dincă, Reka Borka Balas, Simona Mocanu, and Cristina Oana Mărginean. 2023. "Not Every Dyspepsia Is Related to Helicobacter pylori—A Case of Esophageal Inlet Patch in a Female Teenager" Children 10, no. 2: 229. https://doi.org/10.3390/children10020229