
Characterization of MRI White Matter Signal Abnormalities in the Pediatric Population
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Preparation
- Autoimmune disorders (Group 1);
- Non-genetic hypoxic and ischemic insults (Group 2);
- Traumatic white matter injuries (Group 3);
- Patients with no final diagnosis due to insufficient clinical information (Group 4; mostly patients referred by other hospitals requesting a second opinion on a prior imaging exam);
- Non-specific WMSAs (Group 5);
- Infectious white matter damage (Group 6);
- Leukodystrophies (Group 7);
- Toxic white matter injuries (Group 8);
- Inborn errors of metabolism (Group 9);
- White matter damage caused by tumor infiltration/cancer-like disease (Group 10).
2.2. Magnetic Resonance Imaging
2.3. Statistics
3. Results
3.1. Patient Characteristics
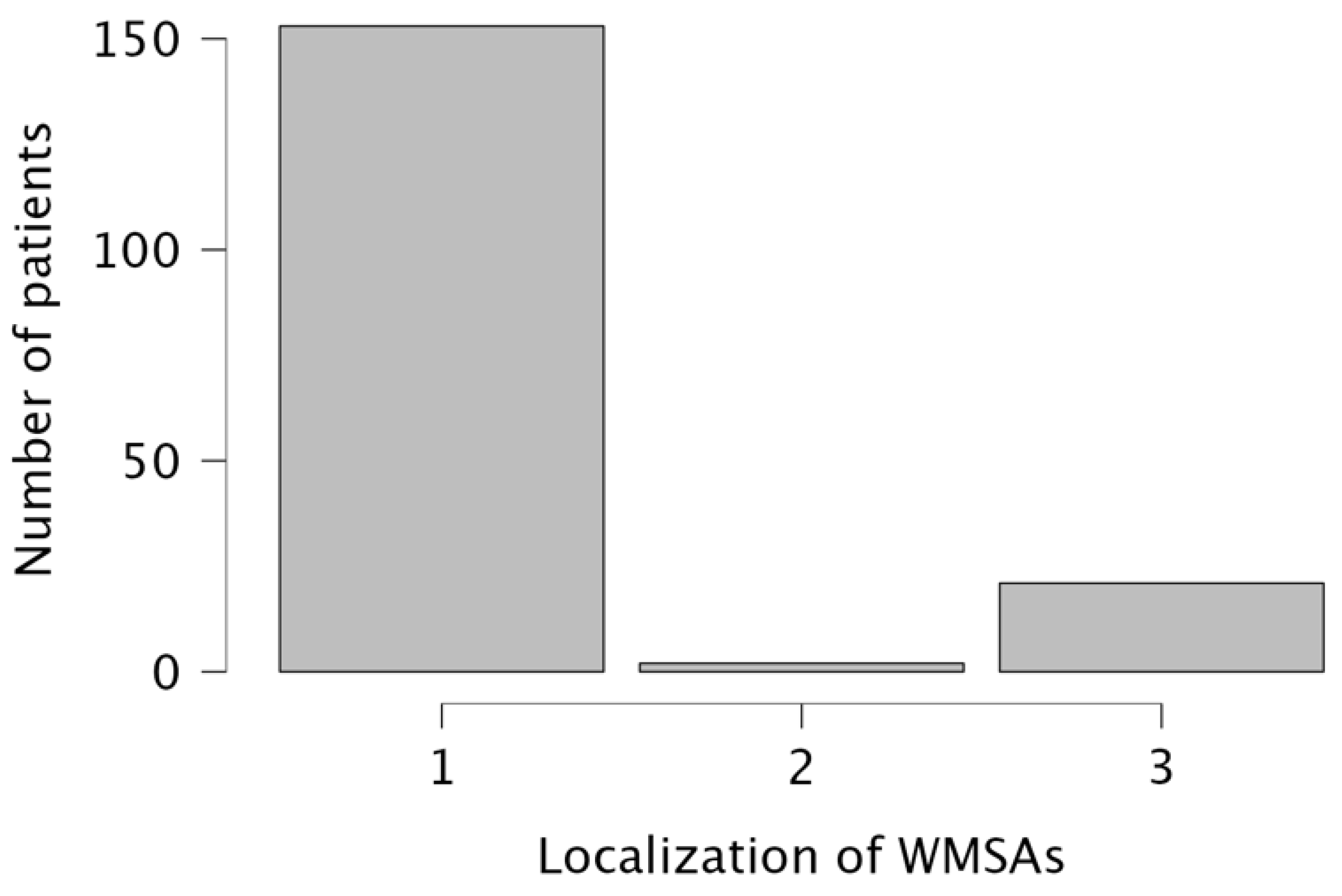
3.2. General Imaging Characteristics
3.3. Etiology-Based Classification of WMSAs
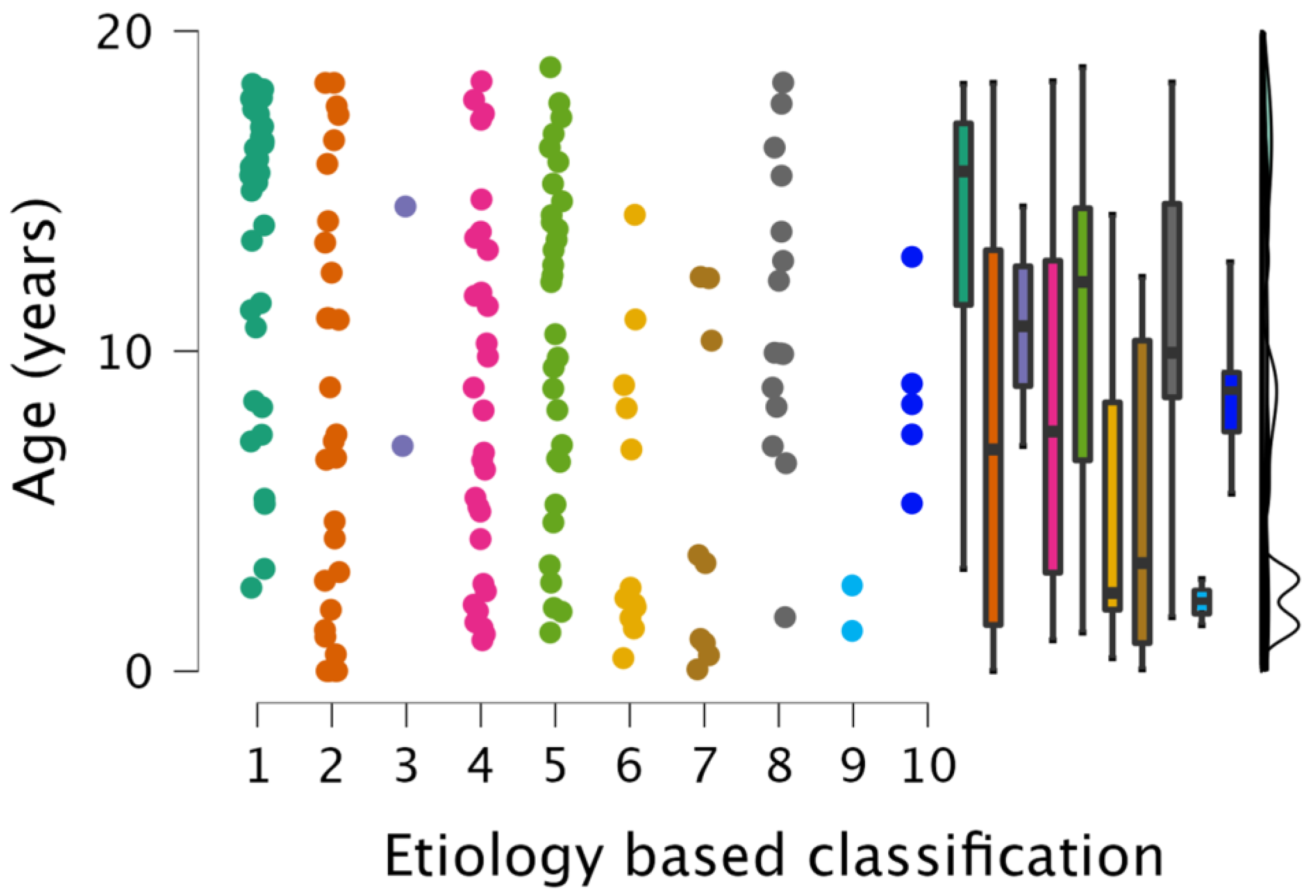
3.4. Age and Gender Distribution of WMSAs
3.5. Individual Group Characteristics
3.5.1. Autoimmune Disease (Group 1)
3.5.2. Non-Genetic Hypoxic and Ischemic Insults (Group 2)
3.5.3. Traumatic White Matter Injuries (Group 3)
3.5.4. Patients with No Final Diagnosis Due to Insufficient Clinical Information (Group 4)
3.5.5. Non-Specific WMSAs (Group 5)
3.5.6. Infectious White Matter Damage (Group 6)
3.5.7. Leukodystrophies (Group 7)
3.5.8. Toxic White Matter Injuries (Group 8)
3.5.9. Inborn Errors of Metabolism (Group 9)
3.5.10. White Matter Damage Caused by Tumor Infiltration/Cancer-like Disease (Group 10)
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviation
| ADEM | acute demyelinating encephalomyelitis |
| ADC | apparent diffusion coefficient |
| APS | antiphospholipid syndrome |
| CIS | clinical information system |
| DNET | dysembryoplastic neuroepithelial tumor |
| DTI | diffusion tensor imaging |
| DWI | diffusion-weighted imaging |
| WMSA | white matter signal abnormality |
| FA | fractional anisotropy |
| FLAIR | fluid-attenuated inversion recovery |
| FSE | fast spin echo |
| IRB | institutional review board |
| IVH | intraventricular hemorrhage |
| MS | multiple sclerosis |
| PRES | posterior reversible encephalopathy syndrome |
| SE | spin echo |
| RIS | radiological information system |
| T | Tesla |
| TIRM | turbo-inversion recovery-magnitude dark fluid |
| TSE | turbo spin echo |
| T1W | T1-weighted |
| T2W | T2-weighted |
References
- van der Knaap, M.S.; Breiter, S.N.; Naidu, S.; Hart, A.A.M.; Valk, J. Defining and Categorizing Leukoencephalopathies of Unknown Origin: MR Imaging Approach. Radiology 1999, 213, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Schiffmann, R.; van der Knaap, M.S. Invited Article: An MRI-Based Approach to the Diagnosis of White Matter Disorders. Neurology 2009, 72, 750–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nichtweiss, M.; Weidauer, S.; Treusch, N.; Hattingen, E. White Matter Lesions and Vascular Cognitive Impairment: Part 1: Typical and Unusual Causes. Clin. Neuroradiol. 2012, 22, 193–210. [Google Scholar] [CrossRef] [PubMed]
- Weidauer, S.; Nichtweiss, M.; Hattingen, E. Differential Diagnosis of White Matter Lesions: Nonvascular Causes-Part II. Clin. Neuroradiol. 2014, 24, 93–110. [Google Scholar] [CrossRef] [PubMed]
- Weidauer, S.; Wagner, M.; Hattingen, E. White Matter Lesions in Adults—A Differential Diagnostic Approach. Rofo 2020, 192, 1154–1173. [Google Scholar] [CrossRef] [PubMed]
- Kwok, P.L.; Lai, A.Y.T.; Lai, B.M.H.; Luk, S.Y.; Tang, K.Y.K.; Wong, W.W.C.; Khoo, J.L.S. Magnetic Resonance Imaging of Disorders with White Matter Changes in Children and Adolescents: A Pictorial Essay. Pediatr. Radiol. 2023. [CrossRef]
- Sarbu, N.; Shih, R.Y.; Jones, R.V.; Horkayne-Szakaly, I.; Oleaga, L.; Smirniotopoulos, J.G. White Matter Diseases with Radiologic-Pathologic Correlation. RadioGraphics 2016, 36, 1426–1447. [Google Scholar] [CrossRef] [Green Version]
- Sharma, R.; Sekhon, S.; Cascella, M. White Matter Lesions. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- van der Knaap, M.S.; Valk, J.; Barkhof, F.; van der Knaap, M.S. Magnetic Resonance of Myelination and Myelin Disorders, 3rd ed.; Springer: Berlin/Heidelberg, Germany; New York, NY, USA, 2005; ISBN 978-3-540-22286-6. [Google Scholar]
- Vanderver, A.; Prust, M.; Tonduti, D.; Mochel, F.; Hussey, H.M.; Helman, G.; Garbern, J.; Eichler, F.; Labauge, P.; Aubourg, P.; et al. Case Definition and Classification of Leukodystrophies and Leukoencephalopathies. Mol. Genet. Metab. 2015, 114, 494–500. [Google Scholar] [CrossRef] [Green Version]
- van der Knaap, M.S.; Bugiani, M. Leukodystrophies: A Proposed Classification System Based on Pathological Changes and Pathogenetic Mechanisms. Acta Neuropathol. 2017, 134, 351–382. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.S.; Illes, J.; Kaplan, R.T.; Reiss, A.; Atlas, S.W. Incidental Findings on Pediatric MR Images of the Brain. AJNR Am. J. Neuroradiol. 2002, 23, 1674–1677. [Google Scholar]
- Gupta, S.N.; Belay, B. Intracranial Incidental Findings on Brain MR Images in a Pediatric Neurology Practice: A Retrospective Study. J. Neurol. Sci. 2008, 264, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Kristjánsdóttir, R.; Uvebrant, P.; Wiklund, L.M. Clinical Characteristics of Children with Cerebral White Matter Abnormalities. Eur. J. Paediatr. Neurol. 2000, 4, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Dangouloff-Ros, V.; Roux, C.-J.; Boulouis, G.; Levy, R.; Nicolas, N.; Lozach, C.; Grevent, D.; Brunelle, F.; Boddaert, N.; Naggara, O. Incidental Brain MRI Findings in Children: A Systematic Review and Meta-Analysis. AJNR Am. J. Neuroradiol. 2019, 40, 1818–1823. [Google Scholar] [CrossRef]
- JASP Team JASP, Version 0.16.4; University of Amsterdam: Amsterdam, The Netherlands, 2022.
- Kolmogorov–Smirnov Test. In The Concise Encyclopedia of Statistics; Springer: New York, NY, USA, 2008; pp. 283–287. ISBN 978-0-387-31742-7.
- Dunn, O.J. Multiple Comparisons Using Rank Sums. Technometrics 1964, 6, 241–252. [Google Scholar] [CrossRef]
- Filippi, M.; Preziosa, P.; Banwell, B.L.; Barkhof, F.; Ciccarelli, O.; De Stefano, N.; Geurts, J.J.G.; Paul, F.; Reich, D.S.; Toosy, A.T.; et al. Assessment of Lesions on Magnetic Resonance Imaging in Multiple Sclerosis: Practical Guidelines. Brain 2019, 142, 1858–1875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swarte, R.; Lequin, M.; Cherian, P.; Zecic, A.; van Goudoever, J.; Govaert, P. Imaging Patterns of Brain Injury in Term-Birth Asphyxia. Acta Paediatr. 2009, 98, 586–592. [Google Scholar] [CrossRef]
- Boiko, A.; Vorobeychik, G.; Paty, D.; Devonshire, V.; Sadovnick, D. The UBC MS Clinic Neurologists Early Onset Multiple Sclerosis: A Longitudinal Study. Neurology 2002, 59, 1006–1010. [Google Scholar] [CrossRef]
- Belman, A.L.; Krupp, L.B.; Olsen, C.S.; Rose, J.W.; Aaen, G.; Benson, L.; Chitnis, T.; Gorman, M.; Graves, J.; Harris, Y.; et al. Characteristics of Children and Adolescents With Multiple Sclerosis. Pediatrics 2016, 138, e20160120. [Google Scholar] [CrossRef] [Green Version]
- Chitnis, T.; Glanz, B.; Jaffin, S.; Healy, B. Demographics of Pediatric-Onset Multiple Sclerosis in an MS Center Population from the Northeastern United States. Mult. Scler. 2009, 15, 627–631. [Google Scholar] [CrossRef]
- Bonkowsky, J.L.; Keller, S.; Capal, J.K.; Lotze, T.; Shellhaas, R.A.; Urion, D.K.; Chen, E.; Trotter, T.L.; Berry, S.A.; Burke, L.W.; et al. Leukodystrophies in Children: Diagnosis, Care, and Treatment. Pediatrics 2021, 148, e2021053126. [Google Scholar] [CrossRef]
- Tenembaum, S.; Chitnis, T.; Ness, J.; Hahn, J.S. International Pediatric MS Study Group Acute Disseminated Encephalomyelitis. Neurology 2007, 68, S23–S36. [Google Scholar] [CrossRef] [PubMed]
- Durá-Travé, T.; Yoldi-Petri, M.E.; Esparza-Estaún, J.; Gallinas-Victoriano, F.; Aguilera-Albesa, S.; Sagastibelza-Zabaleta, A. Magnetic Resonance Imaging Abnormalities in Children with Epilepsy. Eur. J. Neurol. 2012, 19, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Widjaja, E.; Kis, A.; Go, C.; Snead, O.C.; Smith, M.L. Bilateral White Matter Abnormality in Children with Frontal Lobe Epilepsy. Epilepsy Res. 2014, 108, 289–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hintz, S.R.; Barnes, P.D.; Bulas, D.; Slovis, T.L.; Finer, N.N.; Wrage, L.A.; Das, A.; Tyson, J.E.; Stevenson, D.K.; Carlo, W.A.; et al. Neuroimaging and Neurodevelopmental Outcome in Extremely Preterm Infants. Pediatrics 2015, 135, e32–e42. [Google Scholar] [CrossRef] [Green Version]
- Longoni, G.; Brown, R.A.; MomayyezSiahkal, P.; Elliott, C.; Narayanan, S.; Bar-Or, A.; Marrie, R.A.; Yeh, E.A.; Filippi, M.; Banwell, B.; et al. White Matter Changes in Paediatric Multiple Sclerosis and Monophasic Demyelinating Disorders. Brain 2017, 140, 1300–1315. [Google Scholar] [CrossRef] [Green Version]
- Matsuda-Abedini, M.; Fitzpatrick, K.; Harrell, W.R.; Gipson, D.S.; Hooper, S.R.; Belger, A.; Poskitt, K.; Miller, S.P.; Bjornson, B.H. Brain Abnormalities in Children and Adolescents with Chronic Kidney Disease. Pediatr. Res. 2018, 84, 387–392. [Google Scholar] [CrossRef]
- Benninger, K.L.; Maitre, N.L.; Ruess, L.; Rusin, J.A. MR Imaging Scoring System for White Matter Injury after Deep Medullary Vein Thrombosis and Infarction in Neonates. AJNR Am. J. Neuroradiol. 2019, 40, 347–352. [Google Scholar] [CrossRef]
- Widjaja, E.; Nilsson, D.; Blaser, S.; Raybaud, C. White Matter Abnormalities in Children with Idiopathic Developmental Delay. Acta Radiol. 2008, 49, 589–595. [Google Scholar] [CrossRef]
- Mar, S.; Kelly, J.E.; Isbell, S.; Aung, W.Y.; Lenox, J.; Prensky, A. Prevalence of White Matter Lesions and Stroke in Children with Migraine. Neurology 2013, 81, 1387–1391. [Google Scholar] [CrossRef]
- Bayram, E.; Topcu, Y.; Karaoglu, P.; Yis, U.; Guleryuz, H.C.; Kurul, S.H. Incidental White Matter Lesions in Children Presentıng With Headache. Headache J. Head Face Pain 2013, 53, 970–976. [Google Scholar] [CrossRef]
- Kristjánsdóttir, R.; Uvebrant, P.; Hagberg, B.; Kyllerman, M.; Wiklund, L.M.; Blennow, G.; Flodmark, O.; Gustavsson, L.; Ekholm, S.; Månsson, J.E. Disorders of the Cerebral White Matter in Children. The Spectrum of Lesions. Neuropediatrics 1996, 27, 295–298. [Google Scholar] [CrossRef] [PubMed]
- Eikermann-Haerter, K.; Huang, S.Y. White Matter Lesions in Migraine. Am. J. Pathol. 2021, 191, 1955–1962. [Google Scholar] [CrossRef] [PubMed]
- Kjos, B.O.; Umansky, R.; Barkovich, A.J. Brain MR Imaging in Children with Developmental Retardation of Unknown Cause: Results in 76 Cases. AJNR Am. J. Neuroradiol. 1990, 11, 1035–1040. [Google Scholar]
- Kalnin, A.J.; Fastenau, P.S.; deGrauw, T.J.; Musick, B.S.; Perkins, S.M.; Johnson, C.S.; Mathews, V.P.; Egelhoff, J.C.; Dunn, D.W.; Austin, J.K. Magnetic Resonance Imaging Findings in Children with a First Recognized Seizure. Pediatr. Neurol. 2008, 39, 404–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Chen, M.; Wang, J.; Illapani, V.S.P.; Parikh, N.A.; He, L. Automatic Segmentation of Diffuse White Matter Abnormality on T2-Weighted Brain MR Images Using Deep Learning in Very Preterm Infants. Radiol. Artif. Intell. 2021, 3, e200166. [Google Scholar] [CrossRef]
- Joo, L.; Shim, W.H.; Suh, C.H.; Lim, S.J.; Heo, H.; Kim, W.S.; Hong, E.; Lee, D.; Sung, J.; Lim, J.-S.; et al. Diagnostic Performance of Deep Learning-Based Automatic White Matter Hyperintensity Segmentation for Classification of the Fazekas Scale and Differentiation of Subcortical Vascular Dementia. PLoS ONE 2022, 17, e0274562. [Google Scholar] [CrossRef]
- Zhang, Y.; Duan, Y.; Wang, X.; Zhuo, Z.; Haller, S.; Barkhof, F.; Liu, Y. A Deep Learning Algorithm for White Matter Hyperintensity Lesion Detection and Segmentation. Neuroradiology 2022, 64, 727–734. [Google Scholar] [CrossRef]
- Grosu, S.; Rospleszcz, S.; Hartmann, F.; Habes, M.; Bamberg, F.; Schlett, C.L.; Galie, F.; Lorbeer, R.; Auweter, S.; Selder, S.; et al. Associated Factors of White Matter Hyperintensity Volume: A Machine-Learning Approach. Sci. Rep. 2021, 11, 2325. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sequence | Plane | Comment |
|---|---|---|
| 2D T1W SE or FSE (3D MPRAGE in a subset of patients) | axial | pre- and, if clinically indicated, post-contrast (Gadolinium-based contrast agents) |
| 2D T2W TSE | axial | |
| FLAIR or TIRM df | axial | |
| DWI/ADC | axial | b-values 0, 1000 |
| Etiology of WMSAs | Number of Study Patients (n) | Percentage of Study Population |
|---|---|---|
| Autoimmune disease (Group 1) | 40 | 23% |
| Non-genetic hypoxic and ischemic insults (Group 2) | 30 | 17% |
| Traumatic white matter injuries (Group 3) | 2 | 1% |
| Patients with no final diagnosis due to insufficient clinical information (Group 4) | 30 | 17% |
| Non-specific WMSAs (Group 5) | 31 | 18% |
| Infectious and post-infectious white matter damage (Group 6) | 12 | 7% |
| Leukodystrophies (Group 7) | 9 | 5% |
| Toxic white matter injuries (Group 8) | 15 | 9% |
| Inborn errors of metabolism (Group 9) | 2 | 1% |
| White matter damage caused by tumor infiltration/cancer-like disease (Group 10) | 5 | 3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wenger, K.J.; Koldijk, C.E.; Hattingen, E.; Porto, L.; Kurre, W. Characterization of MRI White Matter Signal Abnormalities in the Pediatric Population. Children 2023, 10, 206. https://doi.org/10.3390/children10020206
Wenger KJ, Koldijk CE, Hattingen E, Porto L, Kurre W. Characterization of MRI White Matter Signal Abnormalities in the Pediatric Population. Children. 2023; 10(2):206. https://doi.org/10.3390/children10020206
Chicago/Turabian StyleWenger, Katharina J., Caroline E. Koldijk, Elke Hattingen, Luciana Porto, and Wiebke Kurre. 2023. "Characterization of MRI White Matter Signal Abnormalities in the Pediatric Population" Children 10, no. 2: 206. https://doi.org/10.3390/children10020206