
Risk Factors of Language Delay at Two Years of Corrected Age among Very-Low-Birth-Weight Preterm Infants: A Population-Based Study
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Outcome Evaluation
2.3. Statistical Analysis
3. Results
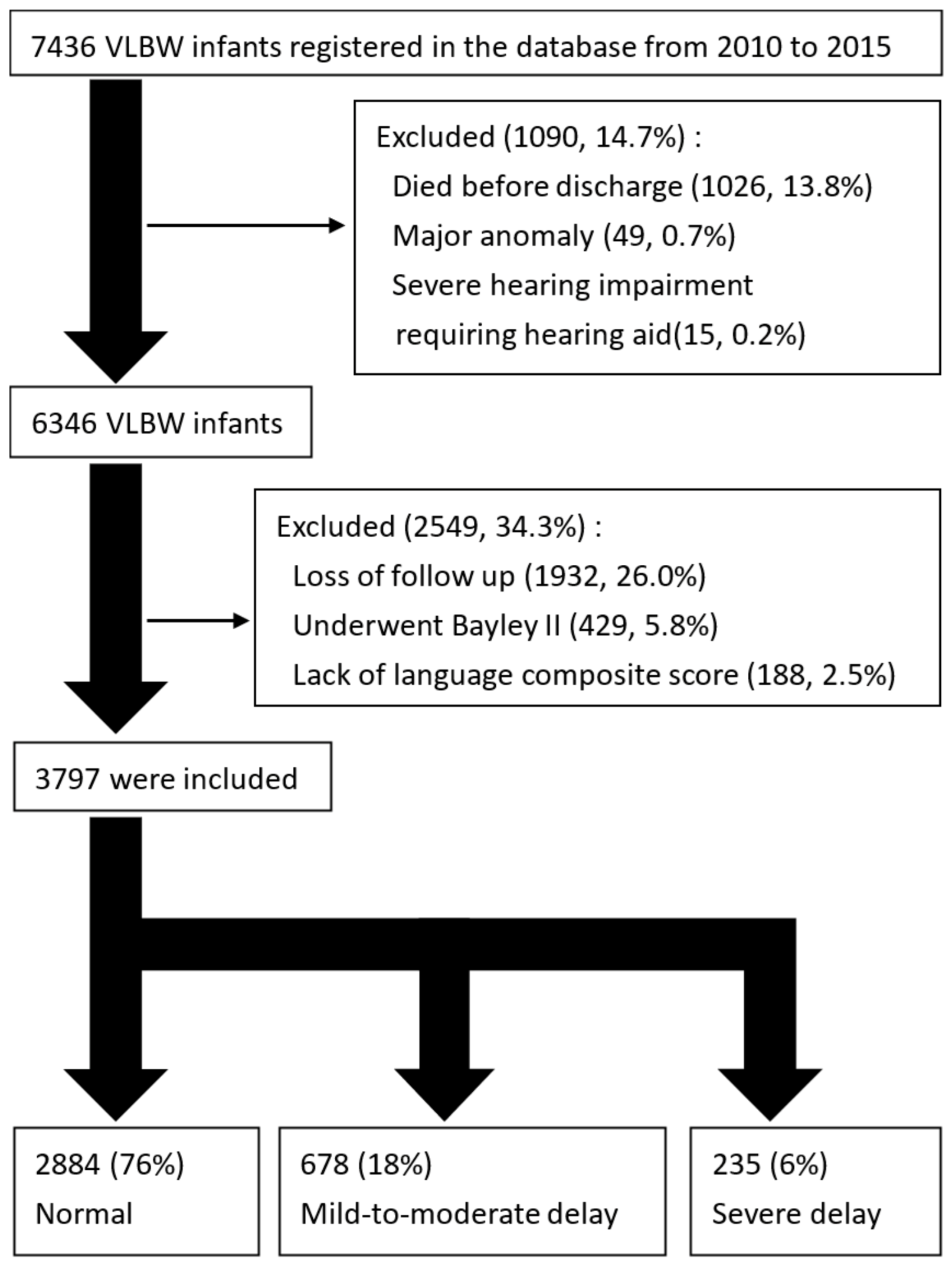
3.1. Participant Selection and Recruitment Period
3.2. Risk Factors of Mild to Moderate or Severe Language Delay
3.3. Logistic Regression Model for Risk Factors
3.4. Linear Regression Model for Language Raw Scores
3.5. Correlation of Language Delay with GA and BW
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chang, J.H.; Hsu, C.H.; Tsou, K.I.; Jim, W.T.; Taiwan Premature Infant Developmental Collaborative Study Group. Outcomes and related factors in a cohort of infants born in Taiwan over a period of five years (2007–2011) with borderline viability. J. Formos. Med. Assoc. 2018, 117, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.-Y.; Wang, S.-H.; Chou, H.-C.; Chen, C.-Y.; Hsieh, W.-S.; Tsao, P.-N.; Tsou, K.-I.; Hsu, C.-H.; Mu, S.-C.; Lin, H.-C.; et al. Morbidity and mortality of very low birth weight infants in Taiwan—Changes in 15 years: A population based study. J. Formos. Med. Assoc. 2016, 115, 1039–1045. [Google Scholar] [CrossRef] [PubMed]
- Su, B.-H.; Hsieh, W.-S.; Hsu, C.-H.; Chang, J.-H.; Lien, R.; Lin, C.-H.; Premature Baby Foundation of Taiwan (PBFT). Neonatal outcomes of extremely preterm infants from Taiwan: Comparison with Canada, Japan, and the USA. Pediatr. Neonatol. 2015, 56, 46–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.-Y.; Hsu, C.-H.; Chang, J.-H.; Taiwan Premature Infant Follow-up Network. Neurodevelopmental outcomes at 2 and 5 years of age in very-low-birth-weight preterm infants born between 2002 and 2009: A prospective cohort study in Taiwan. Pediatr. Neonatol. 2020, 61, 36–44. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.-S.; Jeng, S.-F.; Tsou, K.-I.; Taipei Long-Term Developmental Follow-Up Group for Preterm Infants. Developmental function of very-low-birth-weight infants and full-term infants in early childhood. J. Formos. Med. Assoc. 2004, 103, 23–31. [Google Scholar]
- Conti-Ramsden, G.; Mok, P.L.; Pickles, A.; Durkin, K. Adolescents with a history of specific language impairment (SLI): Strengths and difficulties in social, emotional and behavioral functioning. Res. Dev. Disabil. 2013, 34, 4161–4169. [Google Scholar] [CrossRef]
- Law, J.; Rush, R.; Schoon, I.; Parsons, S. Modeling Developmental Language Difficulties from School Entry into Adulthood: Literacy, Mental Health, and Employment Outcomes. J. Speech Lang. Hear. Res. 2009, 52, 1401–1416. [Google Scholar] [CrossRef] [Green Version]
- Tseng, K.-T.; Peng, C.-C.; Chang, J.-H.; Hsu, C.-H.; Lin, C.-Y.; Jim, W.-T.; Chang, H.-Y. The impact of advanced maternal age on the outcomes of very low birth weight preterm infants. Medicine 2019, 98, e14336. [Google Scholar] [CrossRef]
- Sania, A.; Sudfeld, C.R.; Danaei, G.; Fink, G.; McCoy, D.C.; Zhu, Z.; Fawzi, M.C.S.; Akman, M.; Arifeen, S.E.; Barros, A.J.D.; et al. Early life risk factors of motor, cognitive and language development: A pooled analysis of studies from low/middle-income countries. BMJ Open 2019, 9, e026449. [Google Scholar] [CrossRef] [Green Version]
- El-Din, E.M.S.; Elabd, M.A.; Nassar, M.S.; Metwally, A.M.; Abdellatif, G.A.; Rabah, T.M.; Shalaan, A.; Shaaban, S.Y.; Kandeel, W.; El Etreby, L.A.; et al. The Interaction of Social, Physical and Nutritive Factors in Triggering Early Developmental Language Delay in a Sample of Egyptian Children. Open Access Maced. J. Med. Sci. 2019, 7, 2767–2774. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, P.K.; Shi, L.; Rajadurai, V.S.; Zheng, Q.; Yang, P.H.; Khoo, P.C.; Quek, B.H.; Daniel, L.M. Factors affecting neurodevelopmental outcome at 2 years in very preterm infants below 1250 grams: A prospective study. J. Perinatol. 2018, 38, 1093–1100. [Google Scholar] [CrossRef]
- Asztalos, E.V.; Church, P.T.; Riley, P.; Fajardo, C.; Shah, P.S.; Canadian Neonatal Network and Canadian Neonatal Follow-up Network Investigators. Association between primary caregiver education and cognitive and language development of preterm neonates. Am. J. Perinatol. 2017, 34, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Patra, K.; Greene, M.M.; Patel, A.L.; Meier, P. Maternal education level predicts cognitive, language, and motor outcome in preterm infants in the second year of life. Am. J. Perinatol. 2016, 33, 738–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishimura, T.; Takei, N.; Tsuchiya, K.; Asano, R.; Mori, N. Identification of neurodevelopmental trajectories in infancy and of risk factors affecting deviant development: A longitudinal birth cohort study. Int. J. Epidemiol. 2016, 45, 543–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korpilahti, P.; Kaljonen, A.; Jansson-Verkasalo, E. Identification of biological and environmental risk factors for language delay: The Let’s Talk STEPS study. Infant Behav. Dev. 2016, 42, 27–35. [Google Scholar] [CrossRef]
- Do, C.H.T.; Kruse, A.Y.; Wills, B.; Sabanathan, S.; Clapham, H.; Pedersen, F.K.; Pham, T.N.; Vu, P.M.; Børresen, M.L. Neurodevelopment at 2 years corrected age among Vietnamese preterm infants. Arch. Dis. Child. 2020, 105, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, K.; Spittle, A.J.; Cheong, J.L.; Thompson, D.; Doyle, L.W.; Anderson, P.J.; Morgan, A.T. Language in 2-year-old children born preterm and term: A cohort study. Arch. Dis. Child. 2019, 104, 647–652. [Google Scholar] [CrossRef]
- Zambrana, I.M.; Vollrath, M.E.; Sengpiel, V.; Jacobsson, B.; Ystrom, E. Preterm delivery and risk for early language delays: A sibling-control cohort study. Int. J. Epidemiol. 2016, 45, 151–159. [Google Scholar] [CrossRef] [Green Version]
- Rechia, I.C.; Oliveira, L.D.; Crestani, A.H.; Biaggio, E.P.V.; De Souza, A.P.R. Effects of prematurity on language acquisition and auditory maturation: A systematic review. CoDAS 2016, 28, 843–854. [Google Scholar] [CrossRef]
- Dehghan, M.; Kuhi, M.; Rezvani, S.; Esmaeilzadeh, S.; Samadinezhad, H.; Basirat, Z.; Mir, F.N.; Khafri, S.; Ahmadi, A. Speech and language development of children born following assisted reproductive technologies. Int. J. Pediatr. Otorhinolaryngol. 2020, 134, 110060. [Google Scholar] [CrossRef]
- Ahn, S.H.; Kim, S.A. Assessment of preterm infants using the Bayley-III scales in Korea. Ann. Rehabil. Med. 2017, 41, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.K.; Shin, S.H.; Kim, E.-K.; Kim, H.-S. Developmental outcomes of preterm infants with bronchopulmonary dysplasia-associated pulmonary hypertension at 18–24 months of corrected age. BMC Pediatr. 2019, 19, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youn, Y.; Moon, C.-J.; Sung, I.K. Long-term postnatal steroid effect in very low birth weight infants. Steroids 2017, 125, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Ballot, D.E.; Ramdin, T.; Rakotsoane, D.; Agaba, F.; Chirwa, T.; Davies, V.A.; Cooper, P.A. Assessment of developmental outcome in very low birth weight infants in Southern Africa using the Bayley Scales of Infant Development (III). BMJ Paediatr. Open 2017, 1, e000091. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.-Y.; Chang, J.-H.; Peng, C.-C.; Hsu, C.-H.; Jim, W.-T.; Lin, J.-Y.; Chen, C.-H.; Li, S.-T.; Chang, H.-Y. Predictive Validity of the Bayley-III Cognitive Scores at 6 Months for Cognitive Outcomes at 24 Months in Very-Low-Birth-Weight Infants. Front. Pediatr. 2021, 9, 638449. [Google Scholar] [CrossRef]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary Dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef]
- Papile, L.-A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1,500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar] [CrossRef]
- Neu, J. Necrotizing Enterocolitis: The Search for a Unifying Pathogenic Theory Leading to Prevention. Pediatr. Clin. N. Am. 1996, 43, 409–432. [Google Scholar] [CrossRef]
- Fein, S.B.; Labiner-Wolfe, J.; Scanlon, K.S.; Grummer-Strawn, L.M. Selected Complementary Feeding Practices and Their Association with Maternal Education. Pediatrics 2008, 122, S91–S97. [Google Scholar] [CrossRef] [Green Version]
- Nisar, N.; White, F. Factors affecting utilization of antenatal care among reproductive age group women (15-49 years) in an urban squatter settlement of Karachi. J. Pak. Med. Assoc. 2003, 53, 47–53. [Google Scholar]
- Makoka, D.; Masibo, P.K. Is there a threshold level of maternal education sufficient to reduce child undernutrition? Evidence from Malawi, Tanzania and Zimbabwe. BMC Pediatr. 2015, 15, 96. [Google Scholar] [CrossRef] [Green Version]
- Van Ryzin, M.J.; Carlson, E.A.; Sroufe, L.A. Attachment discontinuity in a high-risk sample. Attach. Hum. Dev. 2011, 13, 381–401. [Google Scholar] [CrossRef]
- Chittleborough, C.R.; Lawlor, D.A.; Lynch, J.W. Young Maternal Age and Poor Child Development: Predictive Validity from a Birth Cohort. Pediatrics 2011, 127, e1436–e1444. [Google Scholar] [CrossRef] [PubMed]
- Jaffari-Bimmel, N.; Juffer, F.; van Ijzendoorn, M.H.; Bakermans-Kranenburg, M.J.; Mooijaart, A. Social development from infancy to adolescence: Longitudinal and concurrent factors in an adoption sample. Dev. Psychol. 2006, 42, 1143–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Pereira, M.; Fernández, P.; Gómez-Taibo, M.L.; Resches, M. Language development of low risk preterm infants up to the age of 30months. Early Hum. Dev. 2014, 90, 649–656. [Google Scholar] [CrossRef]
- Pérez-Pereira, M.; Fernández, P.; Resches, M.; Gómez-Taibo, M.L. Determinants of early language and communication in preterm and full term infants: A comparative study. Enfance 2013, 2013, 59–76. [Google Scholar] [CrossRef]
- Madigan, S.; Wade, M.M.; Plamondon, A.; Browne, M.D.; Jenkins, J.M. Birth Weight Variability and Language Development: Risk, Resilience, and Responsive Parenting. J. Pediatr. Psychol. 2015, 40, 869–877. [Google Scholar] [CrossRef] [Green Version]
- Ball, G.; Seidlitz, J.; O’Muircheartaigh, J.; Dimitrova, R.; Fenchel, D.; Makropoulos, A.; Christiaens, D.; Schuh, A.; Passerat-Palmbach, J.; Hutter, J.; et al. Cortical morphology at birth reflects spatiotemporal patterns of gene expression in the fetal human brain. PLoS Biol. 2020, 18, e3000976. [Google Scholar] [CrossRef]
- Bouyssi-Kobar, M.; Brossard-Racine, M.; Jacobs, M.; Murnick, J.; Chang, T.; Limperopoulos, C. Regional microstructural organization of the cerebral cortex is affected by preterm birth. NeuroImage Clin. 2018, 18, 871–880. [Google Scholar] [CrossRef]
- Makropoulos, A.; Aljabar, P.; Wright, R.; Hüning, B.; Merchant, N.; Arichi, T.; Tusor, N.; Hajnal, J.V.; Edwards, A.D.; Counsell, S.J.; et al. Regional growth and atlasing of the developing human brain. NeuroImage 2016, 125, 456–478. [Google Scholar] [CrossRef] [Green Version]
- Engelhardt, E.; Inder, T.E.; Alexopoulos, D.; Dierker, D.L.; Hill, J.; Van Essen, D.; Neil, J.J. Regional impairments of cortical folding in premature infants. Ann. Neurol. 2015, 77, 154–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ball, G.; Srinivasan, L.; Aljabar, P.; Counsell, S.J.; Durighel, G.; Hajnal, J.V.; Rutherford, M.A.; Edwards, A.D. Development of cortical microstructure in the preterm human brain. Proc. Natl. Acad. Sci. USA 2013, 110, 9541–9546. [Google Scholar] [CrossRef] [PubMed]
- Amaral, J.; Peixoto, S.; Faria, D.; Resende, C.; Taborda, A. Survival and neurodevelopmental outcomes of premature infants with severe peri-intraventricular hemorrhage at 24 months of age. Acta Med. Port. 2022, 35, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Cheong, J.L.Y.; Lee, K.J.; Boland, R.A.; Spittle, A.J.; Opie, G.F.; Burnett, A.C.; Hickey, L.M.; Roberts, G.; Anderson, P.J.; Doyle, L.W.; et al. Changes in long-term prognosis with increasing postnatal survival and the occurrence of postnatal morbidities in extremely preterm infants offered intensive care: A prospective observational study. Lancet Child Adolesc. Health 2018, 2, 872–879. [Google Scholar] [CrossRef]
- Radic, J.A.E.; Vincer, M.; McNeely, P.D. Outcomes of intraventricular hemorrhage and posthemorrhagic hydrocephalus in a population-based cohort of very preterm infants born to residents of Nova Scotia from 1993 to 2010. J. Neurosurg. Pediatr. 2015, 15, 580–588. [Google Scholar] [CrossRef] [Green Version]
- Humberg, A.; Spiegler, J.; Fortmann, M.I.; Zemlin, M.; Marissen, J.; Swoboda, I.; Rausch, T.K.; Herting, E.; Göpel, W.; Härtel, C.; et al. Surgical necrotizing enterocolitis but not spontaneous intestinal perforation is associated with adverse neurological outcome at school age. Sci. Rep. 2020, 10, 2373. [Google Scholar] [CrossRef] [Green Version]
- Moschopoulos, C.; Kratimenos, P.; Koutroulis, I.; Shah, B.V.; Möwes, A.; Bhandari, V. The Neurodevelopmental Perspective of Surgical Necrotizing Enterocolitis: The Role of the Gut-Brain Axis. Mediat. Inflamm. 2018, 2018, 7456857. [Google Scholar] [CrossRef]
- Sveinsdóttir, K.; Ley, D.; Hövel, H.; Fellman, V.; Hüppi, P.S.; Smith, L.E.; Hellström, A.; Pupp, I.H. Relation of Retinopathy of Prematurity to Brain Volumes at Term Equivalent Age and Developmental Outcome at 2 Years of Corrected Age in Very Preterm Infants. Neonatology 2018, 114, 46–52. [Google Scholar] [CrossRef] [Green Version]
- Glass, T.J.A.; Chau, V.; Gardiner, J.; Foong, J.; Vinall, J.; Zwicker, J.G.; Grunau, R.E.; Synnes, A.; Poskitt, K.J.; Miller, S.P. Severe retinopathy of prematurity predicts delayed white matter maturation and poorer neurodevelopment. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, F532–F537. [Google Scholar] [CrossRef]
- Arima, M.; Akiyama, M.; Fujiwara, K.; Mori, Y.; Inoue, H.; Seki, E.; Nakama, T.; Tsukamoto, S.; Ochiai, M.; Ohga, S.; et al. Neurodevelopmental outcomes following intravitreal bevacizumab injection in Japanese preterm infants with type 1 retinopathy of prematurity. PLoS ONE 2020, 15, e0230678. [Google Scholar] [CrossRef]
- Mosca, R.; Kritzinger, A.; van der Linde, J. Language and communication development in preschool children with visual impairment: A systematic review. S. Afr. J. Commun. Disord. 2015, 62, e1–e10. [Google Scholar] [CrossRef] [Green Version]
- Nagayoshi, M.; Hirose, T.; Toju, K.; Suzuki, S.; Okamitsu, M.; Teramoto, T.; Omori, T.; Kawamura, A.; Takeo, N. Related visual impairment to mother-infant interaction and development in infants with bilateral retinoblastoma. Eur. J. Oncol. Nurs. 2017, 28, 28–34. [Google Scholar] [CrossRef]
- Nagayoshi, M.; Hirose, T.; Omori, T.; Toju, K.; Suzuki, S.; Okamitsu, M.; Kawamura, A.; Takeo, N. A Prospective Study of Factors Related to Mother-Infant Interaction in One-year-old Infants with Retinoblastoma. J. Med. Dent. Sci. 2015, 62, 103–113. [Google Scholar] [CrossRef]
- Schneider, J.; Miller, S.P. Preterm brain Injury: White matter injury. Handb. Clin. Neurol. 2019, 162, 155–172. [Google Scholar] [CrossRef]
- Twilhaar, E.S.; Wade, R.M.; de Kieviet, J.F.; van Goudoever, J.B.; van Elburg, R.M.; Oosterlaan, J. Cognitive Outcomes of Children Born Extremely or Very preterm since the 1990s and Associated Risk Factors: A Meta-analysis and Meta-regression. JAMA Pediatr. 2018, 172, 361–367. [Google Scholar] [CrossRef]
- Loeb, D.F.; Imgrund, C.M.; Lee, J.; Barlow, S.M. Language, motor, and cognitive outcomes of toddlers who were born preterm. Am. J. Speech Lang. Pathol. 2020, 29, 625–637. [Google Scholar] [CrossRef]
- Bello, A.; Onofrio, D.; Remi, L.; Caselli, C. Prediction and persistence of late talking: A study of Italian toddlers at 29 and 34 months. Res. Dev. Disabil. 2018, 75, 40–48. [Google Scholar] [CrossRef]
- Sansavini, A.; Pentimonti, J.; Justice, L.; Guarini, A.; Savini, S.; Alessandroni, R.; Faldella, G. Language, motor and cognitive development of extremely preterm children: Modeling individual growth trajectories over the first three years of life. J. Commun. Disord. 2014, 49, 55–68. [Google Scholar] [CrossRef]
- McMahon, G.E.; Spencer-Smith, M.; Pace, C.C.; Spittle, A.J.; Stedall, P.; Richardson, K.; Cheong, J.L.; Doyle, L.W.; Anderson, P.J.; Treyvaud, K. Influence of Fathers’ Early Parenting on the Development of Children Born Very Preterm and Full Term. J. Pediatr. 2019, 205, 195–201. [Google Scholar] [CrossRef]
- Pancsofar, N.; Vernon-Feagans, L. Fathers’ early contributions to children’s language development in families from low-income rural communities. Early Child. Res. Q. 2010, 25, 450–463. [Google Scholar] [CrossRef]


{kind=link}
| N (%) or Mean (SD) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Normal (N = 2884) | Mild to Moderate (N = 678) | p Value # | Severe (N = 235) | p Value # | ||||
| Mother age ≥ 35 | 406 | 14.1% | 113 | 16.7% | 0.09 | 28 | 11.9% | 0.36 |
| Low maternal education level | 760 | 26.4% | 297 | 43.8% | <0.01 * | 107 | 45.5% | <0.01 * |
| Low maternal socioeconomic status | 855 | 29.6% | 319 | 47.1% | <0.01 * | 122 | 51.9% | <0.01 * |
| Preeclampsia | 591 | 20.5% | 137 | 20.2% | 0.87 | 45 | 19.1% | 0.62 |
| PPROM | 917 | 31.8% | 215 | 31.7% | 0.97 | 62 | 26.4% | 0.09 |
| Chorioamnionitis | 136 | 4.7% | 22 | 3.2% | 0.09 | 13 | 5.5% | 0.57 |
| IUGR | 332 | 11.5% | 79 | 11.7% | 0.92 | 33 | 14.0% | 0.25 |
| 2 doses of prenatal steroid | 1661 | 57.6% | 381 | 56.2% | 0.51 | 130 | 55.3% | 0.50 |
| GA | 29.1 | (2.7) | 28.3 | (2.8) | <0.01 * | 27.9 | (2.9) | <0.01 * |
| GA < 28 weeks | 813 | 28.2% | 266 | 39.2% | <0.01 * | 118 | 50.2% | <0.01 * |
| BW | 1135.5 | (248.6) | 1035.2 | (266.5) | <0.01 * | 988.5 | (289.1) | <0.01 * |
| BW < 1000 g | 864 | 30.0% | 299 | 44.1% | <0.01 * | 124 | 52.8% | <0.01 * |
| SGA | 957 | 33.2% | 222 | 32.7% | 0.83 | 75 | 31.9% | 0.69 |
| Sex (male) | 1335 | 46.3% | 410 | 60.5% | <0.01 * | 153 | 65.1% | <0.01 * |
| Singleton | 1953 | 67.7% | 466 | 68.7% | 0.51 | 160 | 68.1% | 0.91 |
| Resuscitation at delivery | 1748 | 60.6% | 473 | 69.8% | <0.01 * | 181 | 77.0% | <0.01 * |
| Sepsis | 468 | 16.2% | 124 | 18.3% | 0.19 | 66 | 28.1% | <0.01 * |
| NEC | 33 | 1.1% | 9 | 1.3% | 0.69 | 12 | 5.1% | <0.01 * |
| PDA ligation | 427 | 14.8% | 152 | 22.4% | <0.01 * | 69 | 29.4% | <0.01 * |
| ROP needed treatment | 225 | 7.8% | 103 | 15.2% | <0.01 * | 46 | 19.6% | <0.01 * |
| BPD | 1851 | 64.2% | 516 | 76.1% | <0.01 * | 185 | 78.7% | <0.01 * |
| Severe IVH and/or PVL | 171 | 5.9% | 82 | 12.1% | <0.01 * | 52 | 22.1% | <0.01 * |
| Mild To Moderate Delay | Severe Delay | |||||||
|---|---|---|---|---|---|---|---|---|
| Wald χ2 | OR | 95% CI | p Value | Wald χ2 | OR | 95% CI | p Value | |
| Low maternal education level | 14.836 | 1.579 | 1.251–1.992 | < 0.01 * | 6.390 | 1.598 | 1.111–2.298 | 0.01 * |
| Low maternal socioeconomic status | 16.481 | 1.605 | 1.277–2.017 | < 0.01 * | 11.673 | 1.872 | 1.306–2.681 | <0.01 * |
| GA < 28 weeks | 1.086 | 1.141 | 0.890–1.463 | 0.30 | 0.065 | 1.052 | 0.712–1.556 | 0.80 |
| BW < 1000 g | 11.028 | 1.478 | 1.174–1.861 | <0.01 * | 7.774 | 1.681 | 1.167–2.421 | <0.01 * |
| Gender (male) | 44.904 | 1.834 | 1.536–2.190 | <0.01 * | 27.631 | 2.181 | 1.631–2.917 | <0.01 * |
| resuscitation at delivery | 3.086 | 1.197 | 0.979–1.462 | 0.08 | 5.330 | 1.501 | 1.063–2.120 | 0.02 * |
| Sepsis | 2.119 | 1.292 | 0.922–1.811 | 0.14 | ||||
| NEC | 7.182 | 2.763 | 1.314–5.809 | <0.01 * | ||||
| PDA ligation | 3.016 | 1.236 | 0.973–1.571 | 0.08 | 6.606 | 1.580 | 1.115–2.239 | 0.01 * |
| ROP needed treatment | 6.521 | 1.456 | 1.091–1.942 | 0.01 * | 0.979 | 1.237 | 0.812–1.885 | 0.32 |
| BPD | 3.049 | 1.227 | 0.975–1.544 | 0.08 | 0.449 | 0.873 | 0.586–1.300 | 0.50 |
| Severe IVH and/or PVL | 13.064 | 1.728 | 1.284–2.324 | <0.01 * | 34.369 | 3.102 | 2.125–4.529 | <0.01 * |
| Receptive Raw Score | Expressive Raw Score | |||||||
|---|---|---|---|---|---|---|---|---|
| B | SE | β | p Value | B | SE | β | p Value | |
| Low maternal education level | −1.40 | 0.22 | −0.13 | <0.01 * | −1.43 | 0.35 | −0.08 | <0.01 * |
| Low maternal socioeconomic status | −1.26 | 0.21 | −0.12 | <0.01 * | −1.46 | 0.34 | −0.09 | <0.01 * |
| GA < 28 weeks | −0.11 | 0.23 | −0.01 | 0.64 | −0.49 | 0.37 | −0.03 | 0.18 |
| BW < 1000 g | −0.71 | 0.21 | −0.07 | <0.01 * | −0.56 | 0.34 | −0.03 | 0.10 |
| Sex, (male) | 1.32 | 0.15 | 0.13 | <0.01 * | 1.72 | 0.25 | 0.11 | 0.01 * |
| Resuscitation at delivery | −0.34 | 0.17 | −0.03 | 0.05 * | −0.07 | 0.28 | 0.00 | 0.81 |
| Sepsis | −0.14 | 0.21 | −0.01 | 0.50 | −0.50 | 0.34 | −0.02 | 0.14 |
| NEC | −1.75 | 0.66 | −0.04 | <0.01 * | −0.26 | 1.06 | 0.00 | 0.81 |
| PDA ligation | −0.19 | 0.23 | −0.01 | 0.40 | −1.28 | 0.37 | −0.06 | <0.01 * |
| ROP needed treatment | −0.68 | 0.29 | −0.04 | 0.02 * | −1.33 | 0.46 | −0.05 | <0.01 * |
| BPD | 0.22 | 0.19 | 0.02 | 0.26 | 0.31 | 0.31 | 0.02 | 0.32 |
| Severe IVH and/or cystic PVL | −2.07 | 0.29 | −0.11 | <0.01 * | −2.55 | 0.47 | −0.09 | <0.01 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tseng, W.-L.; Chen, C.-H.; Chang, J.-H.; Peng, C.-C.; Jim, W.-T.; Lin, C.-Y.; Hsu, C.-H.; Liu, T.-Y.; Chang, H.-Y.; on behalf of the Taiwan Premature Infant Follow-up Network. Risk Factors of Language Delay at Two Years of Corrected Age among Very-Low-Birth-Weight Preterm Infants: A Population-Based Study. Children 2023, 10, 189. https://doi.org/10.3390/children10020189
Tseng W-L, Chen C-H, Chang J-H, Peng C-C, Jim W-T, Lin C-Y, Hsu C-H, Liu T-Y, Chang H-Y, on behalf of the Taiwan Premature Infant Follow-up Network. Risk Factors of Language Delay at Two Years of Corrected Age among Very-Low-Birth-Weight Preterm Infants: A Population-Based Study. Children. 2023; 10(2):189. https://doi.org/10.3390/children10020189
Chicago/Turabian StyleTseng, Wei-Lun, Chia-Huei Chen, Jui-Hsing Chang, Chun-Chih Peng, Wai-Tim Jim, Chia-Ying Lin, Chyong-Hsin Hsu, Tzu-Yu Liu, Hung-Yang Chang, and on behalf of the Taiwan Premature Infant Follow-up Network. 2023. "Risk Factors of Language Delay at Two Years of Corrected Age among Very-Low-Birth-Weight Preterm Infants: A Population-Based Study" Children 10, no. 2: 189. https://doi.org/10.3390/children10020189