

A Prospective Evaluation of the Effects of the COVID-19 Pandemic on Youth with Primary Headache Disorders

Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure
2.2. Measures
2.3. Analyses
3. Results
3.1. Sample Characteristics
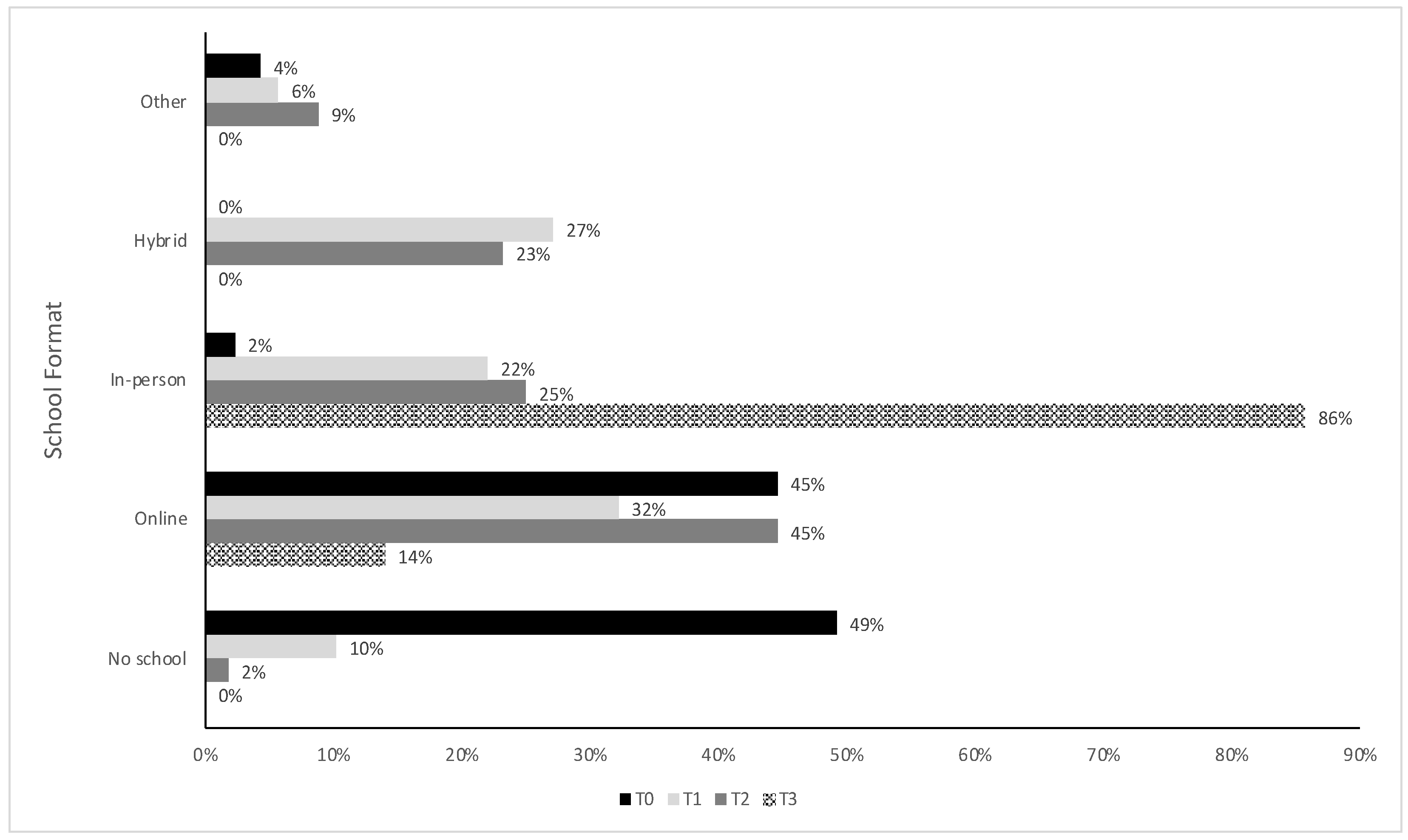
3.2. Changes in School Structure
3.3. Changes in Lifestyle Behaviors and Routines
3.4. Comparison of Recalled Pre-Pandemic Headache Characteristics to after Initial Pandemic Onset
3.5. Changes in Headache Characteristics over the Course of the Pandemic
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adhikari, S.P.; Meng, S.; Wu, Y.-J.; Mao, Y.-P.; Ye, R.-X.; Wang, Q.-Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 29. [Google Scholar] [CrossRef] [Green Version]
- De Bruin, Y.B.; Lequarre, A.; McCourt, J.; Clevestig, P.; Pigazzani, F.; Jeddi, M.Z.; Colosio, C.; Goulart, M. Initial impacts of global risk mitigation measures taken during the combatting of the COVID-19 pandemic. Saf. Sci. 2020, 128, 104773. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.A.; Ming, D.; Maslow, G.; Gifford, E.J. Mitigating the impacts of the COVID-19 pandemic response on at-risk children. Pediatrics 2020, 146, e20200973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.H.; Doan, S.N. Psychosocial stress contagion in children and families during the COVID-19 pandemic. Clin. Pediatr. 2020, 59, 853–855. [Google Scholar] [CrossRef]
- Panchal, U.; de Pablo, G.S.; Franco, M.; Moreno, C.; Parellada, M.; Arango, C.; Fusar-Poli, P. The impact of COVID-19 lockdown on child and adolescent mental health: Systematic review. Eur. Child. Adolesc. Psychiatry 2021, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Panda, P.K.; Gupta, J.; Chowdhury, S.R.; Kumar, R.; Meena, A.K.; Madaan, P.; Sharawat, I.K.; Gulati, S. Psychological and behavioral impact of lockdown and quarantine measures for COVID-19 pandemic on children, adolescents and caregivers: A systematic review and meta-analysis. J. Trop. Pediatr. 2021, 67, fmaa122. [Google Scholar] [CrossRef] [PubMed]
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: A meta-analysis. JAMA Pediatr. 2021, 175, 1142–1150. [Google Scholar] [CrossRef]
- Theberath, M.; Bauer, D.; Chen, W.; Salinas, M.; Mohabbat, A.B.; Yang, J.; Chon, T.Y.; A Bauer, B.; Wahner-Roedler, D.L. Effects of COVID-19 pandemic on mental health of children and adolescents: A systematic review of survey studies. SAGE Open Med. 2022, 10, 20503121221086712. [Google Scholar] [CrossRef]
- Jones, E.A.K.; Mitra, A.K.; Bhuiyan, A.R. Impact of COVID-19 on mental health in adolescents: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 2470. [Google Scholar] [CrossRef]
- Meherali, S.; Punjani, N.; Louie-Poon, S.; Abdul Rahim, K.; Das, J.K.; Salam, R.A.; Lassi, Z.S. Mental health of children and adolescents amidst COVID-19 and past pandemics: A rapid systematic review. Int. J. Environ. Res. Public Health 2021, 18, 3432. [Google Scholar] [CrossRef]
- Tang, S.; Xiang, M.; Cheung, T.; Xiang, Y.T. Mental health and its correlates among children and adolescents during COVID-19 school closure: The importance of parent-child discussion. J. Affect. Disord. 2021, 279, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Ford, T.; John, A.; Gunnell, D. Mental health of children and young people during pandemic. BMJ 2021, 372, n614. [Google Scholar] [CrossRef] [PubMed]
- Almeida, M.; Challa, M.; Ribeiro, M.; Harrison, A.M.; Castro, M.C. The mental health impact of school closures during the COVID-19 pandemic. J. Child Psychol. Psychiatry 2022, 63, 608–612. [Google Scholar] [CrossRef]
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 1985, 98, 310–357. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Kröner-Herwig, B.; Gassmann, J. Headache disorders in children and adolescents: Their association with psychological, behavioral, and socio-environmental factors. Headache 2012, 52, 1387–1401. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Bruno, A.; Trojsi, F.; Tessitore, A.; Tedeschi, G. Lifestyle factors and migraine in childhood. Curr. Pain Headache Rep. 2016, 20, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Papetti, L.; Loro, P.A.D.; Tarantino, S.; Grazzi, L.; Guidetti, V.; Parisi, P.; Raieli, V.; Sciruicchio, V.; Termine, C.; Toldo, I.; et al. I stay at home with headache. A survey to investigate how the lockdown for COVID-19 impacted on headache in Italian children. Cephalalgia 2020, 40, 1459–1473. [Google Scholar] [CrossRef] [PubMed]
- Dallavalle, G.; Pezzotti, E.; Provenzi, L.; Toni, F.; Carpani, A.; Borgatti, R. Migraine symptoms improvement during the COVID-19 lockdown in a cohort of children and adolescents. Front. Neurol. 2020, 11, 579047. [Google Scholar] [CrossRef]
- Law, E.F.; Zhou, C.; Seung, F.; Perry, F.; Palermo, T.M. Longitudinal study of early adaptation to the coronavirus disease pandemic among youth with chronic pain and their parents: Effects of direct exposures and economic stress. Pain 2021, 162, 2132–2144. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Kosinski, M.; Bayliss, M.S.; Bjorner, J.B., Jr.; Ware, J.E.; Garber, W.H.; Batenhorst, A.; Cady, R.; Dahlöf, C.G.; Dowson, A.; Tepper, S. A six-item short-form survey for measuring headache impact: The HIT-6. Qual. Life Res. 2003, 12, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Osika, W.; Friberg, P.; Wahrborg, P. A new short self-rating questionnaire to assess stress in children. Int. J. Behav. Med. 2007, 14, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Chesney, M.A.; Neilands, T.B.; Chambers, D.B.; Taylor, J.M.; Folkman, S. A validity and reliability study of the coping self-efficacy scale. Br. J. Health Psychol. 2006, 11 Pt 3, 421–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, J.D.; Willett, J.B. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence; Oxford University Press: Oxford, UK, 2003. [Google Scholar]
- Guidett, V.; Faedda, N.; Siniatchkin, M. Migraine in childhood: Biobehavioural or psychosomatic disorder? J. Headache Pain 2016, 17, 82. [Google Scholar] [CrossRef] [Green Version]
- Connelly, M.; Bickel, J. An electronic daily diary process study of stress and health behavior triggers of primary headaches in children. J. Pediatr. Psychol. 2011, 36, 852–862. [Google Scholar] [CrossRef] [Green Version]
- Jacoby, R.; Greenfeld Barsky, K.; Porat, T.; Harel, S.; Hanalis Miller, T.; Goldzweig, G. Individual stress response patterns: Preliminary findings and possible implications. PLoS ONE 2021, 16, e0255889. [Google Scholar] [CrossRef] [PubMed]
- Soriani, S.; Fiumana, E.; Manfredini, R.; Boari, B.; Battistella, P.A.; Canetta, E.; Pedretti, S.; Borgna-Pignatti, C. Circadian and seasonal variation of migraine attacks in children. Headache 2006, 46, 1571–1574. [Google Scholar] [CrossRef]
- Pakalnis, A.; Heyer, G.L. Seasonal variation in emergency department visits among pediatric headache patients. Headache 2016, 56, 1344–1347. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.J.Y.; Chan, A.C.Y.; Bharatendu, C.; Teoh, H.L.; Chan, Y.C.; Sharma, V.K. Headache related to PPE use during the COVID-19 pandemic. Curr. Pain Headache Rep. 2021, 25, 53. [Google Scholar] [CrossRef]
- Hawrilenko, M.; Kroshus, E.; Tandon, P.; Christakis, D. The association between school closures and child mental health during COVID-19. JAMA Netw. Open 2021, 4, e2124092. [Google Scholar] [CrossRef] [PubMed]
- Caffo, E.; Asta, L.; Scandroglio, F. Predictors of mental health worsening among children and adolescents during the coronavirus disease 2019 pandemic. Curr. Opin. Psychiatry 2021, 34, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Gazerani, P. Migraine and mood in children. Behav. Sci. 2021, 11, 52. [Google Scholar] [CrossRef]
- Karlson, C.W.; Litzenburg, C.C.; Sampilo, M.L.; Rapoff, M.A.; Connelly, M.; Bickel, J.L.; Hershey, A.D.; Powers, S.W. Relationship between daily mood and migraine in children. Headache 2013, 53, 1624–1634. [Google Scholar] [CrossRef] [Green Version]
- Neut, D.; Fily, A.; Cuvellier, J.C.; Vallée, L. The prevalence of triggers in paediatric migraine: A questionnaire study in 102 children and adolescents. J. Headache Pain 2012, 13, 61–65. [Google Scholar] [CrossRef] [Green Version]
- Milde-Busch, A.; Blaschek, A.; Heinen, F.; Borggräfe, I.; Koerte, I.; Straube, A.; Schankin, C.; Von Kries, R. Associations between stress and migraine and tension-type headache: Results from a school-based study in adolescents from grammar schools in Germany. Cephalalgia 2011, 31, 774–785. [Google Scholar] [CrossRef] [Green Version]
- Gross, E.C.; Lisicki, M.; Fischer, D.; Sándor, P.S.; Schoenen, J. The metabolic face of migraine—From pathophysiology to treatment. Nat. Rev. Neurol. 2019, 15, 627–643. [Google Scholar] [CrossRef]
- Lin, J.E.; Asfour, A.; Sewell, T.B.; Hooe, B.; Pryce, P.; Earley, C.; Shen, M.Y.; Kerner-Rossi, M.; Thakur, K.T.; Vargas, W.S.; et al. Neurological issues in children with COVID-19. Neurosci. Lett. 2021, 743, 135567. [Google Scholar] [CrossRef]
- Straburzyński, M.; Nowaczewska, M.; Budrewicz, S.; Waliszewska-Prosół, M. COVID-19-related headache and sinonasal inflammation: A longitudinal study analysing the role of acute rhinosinusitis and ICHD-3 classification difficulties in SARS-CoV-2 infection. Cephalalgia 2022, 42, 218–228. [Google Scholar] [CrossRef]
- Castaldo, M.; Waliszewska-Prosół, M.; Koutsokera, M.; Robotti, M.; Straburzyński, M.; Apostolakopoulou, L.; Capizzi, M.; Çibuku, O.; Ambat, F.D.F.; Frattale, I.; et al. Headache onset after vaccination against SARS-CoV-2: A systematic literature review and meta-analysis. J. Headache Pain 2022, 23, 41. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Baseline (T0) | T1 | T2 | T3 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lifestyle/Routines Item 1 | M (SD) | Mdn | Min/ Max | M (SD) | Mdn | Min/ Max | M (SD) | Mdn | Min/ Max | M (SD) | Mdn | Min/ Max |
| I am using the computer more now than is usual for me | 3.45 (1.42) | 4.0 | 1/5 | 4.02 (1.17) | 4.0 | 1/5 | 4.13 (1.22) | 5.0 | 1/5 | 2.67 * (1.02) | 3.0 | 1/4 |
| School is less stressful for me now | 3.13 (1.45) | 3.0 | 1/5 | 2.73 (1.28) | 3.0 | 1/5 | 2.52 (1.38) | 2.5 | 1/5 | 2.21 (1.35) | 1.5 | 1/5 |
| Being at home more with family has been stressful | 2.68 (1.37) | 3.0 | 1/5 | 2.77 (1.31) | 3.0 | 1/5 | 2.94 (1.19) | 3.0 | 1/5 | 2.53 (1.25) | 2.0 | 1/5 |
| It has been difficult for me to be out of my usual activities | 3.68 (1.31) | 4.0 | 1/5 | 3.80 (1.2) | 4.0 | 1/5 | 3.79 (1.26) | 4.0 | 1/5 | 3.25 (1.38) | 3.0 | 1/5 |
| I am having frequent worrisome thoughts about my family’s health and safety | 2.98 (1.42) | 3.0 | 1/5 | 2.97 (1.39) | 3.0 | 1/5 | 2.89 (1.42) | 3.0 | 1/5 | 2.69 (1.53) | 2.5 | 1/5 |
| I am getting more sleep now than is usual for me | 3.36 (1.36) | 4.0 | 1/5 | 3.02 (1.14) | 3.0 | 1/5 | 2.79 (1.21) | 3.0 | 1/5 | 2.58 (1.53) | 2.0 | 1/5 |
| Timepoint | Mean ± SD | Median | Minimum–Maximum |
|---|---|---|---|
| Baseline/T0 (n = 130) | 60.21 ± 8.55 | 62.00 | 38–78 |
| T1 (n = 59) | 59.49 ± 7.70 | 61.00 | 40–73 |
| T2 (n = 58) | 59.45 ± 7.88 | 60.00 | 42–78 |
| T3 (n = 41) | 58.44 ± 9.52 | 59.50 | 36–74 |
| Timepoint | Little to No Impact (%, n/N) | Some Impact (%, n/N) | Substantial Impact (%, n/N) | Severe Impact (%, n/N) |
|---|---|---|---|---|
| Baseline/T0 | 15.4% (20/130) | 11.5% (5/130) | 10.8% (14/130) | 62.3% (81/130) |
| T1 | 10.2% (6/59) | 20.3% (12/59) | 13.6% (8/59) | 55.9% (33/59) |
| T2 | 10.3% (6/58) | 17.2% (10/58) | 15.5% (9/58) | 56.9% (33/58) |
| T3 | 12.2% (4/41) | 14.6% (6/41) | 34.1% (14/41) | 41.4% (17/41) |
| Timepoint | Mean 1 ± Standard Deviation | Median | Minimum– Maximum |
|---|---|---|---|
| Baseline/T0 | 3.96 ± 1.82 | 4.00 | 1–7 |
| Recalled prior to pandemic 2 | 3.85 ± 1.74 | 3.00 | 1–7 |
| T1 | 3.93 ± 1.91 | 4.00 | 1–7 |
| T2 | 4.22 ± 1.75 | 4.00 | 1–7 |
| T3 | 3.97 ± 1.99 | 4.00 | 1–7 |
| Timepoint | Mean 1 ± Standard Deviation | Median | Minimum– Maximum |
|---|---|---|---|
| Baseline/T0 | 56.48 ± 21.00 | 61.00 | 0–100 |
| Recalled prior to pandemic 2 | 59.51 ± 20.23 | 62.00 | 3–100 |
| T1 | 56.00 ± 14.52 | 56.00 | 22–87 |
| T2 | 54.34 ± 19.83 | 58.50 | 8–91 |
| T3 | 52.49 ± 22.22 | 54.00 | 2–100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Connelly, M.; Dilts, J.; Boorigie, M.; Gerson, T. A Prospective Evaluation of the Effects of the COVID-19 Pandemic on Youth with Primary Headache Disorders. Children 2023, 10, 184. https://doi.org/10.3390/children10020184
Connelly M, Dilts J, Boorigie M, Gerson T. A Prospective Evaluation of the Effects of the COVID-19 Pandemic on Youth with Primary Headache Disorders. Children. 2023; 10(2):184. https://doi.org/10.3390/children10020184
Chicago/Turabian StyleConnelly, Mark, Jennifer Dilts, Madeline Boorigie, and Trevor Gerson. 2023. "A Prospective Evaluation of the Effects of the COVID-19 Pandemic on Youth with Primary Headache Disorders" Children 10, no. 2: 184. https://doi.org/10.3390/children10020184