
Influence of Child’s Temperament on Behaviour Management Problems in the Dental Office: A Literature Review
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Collected
3. Results
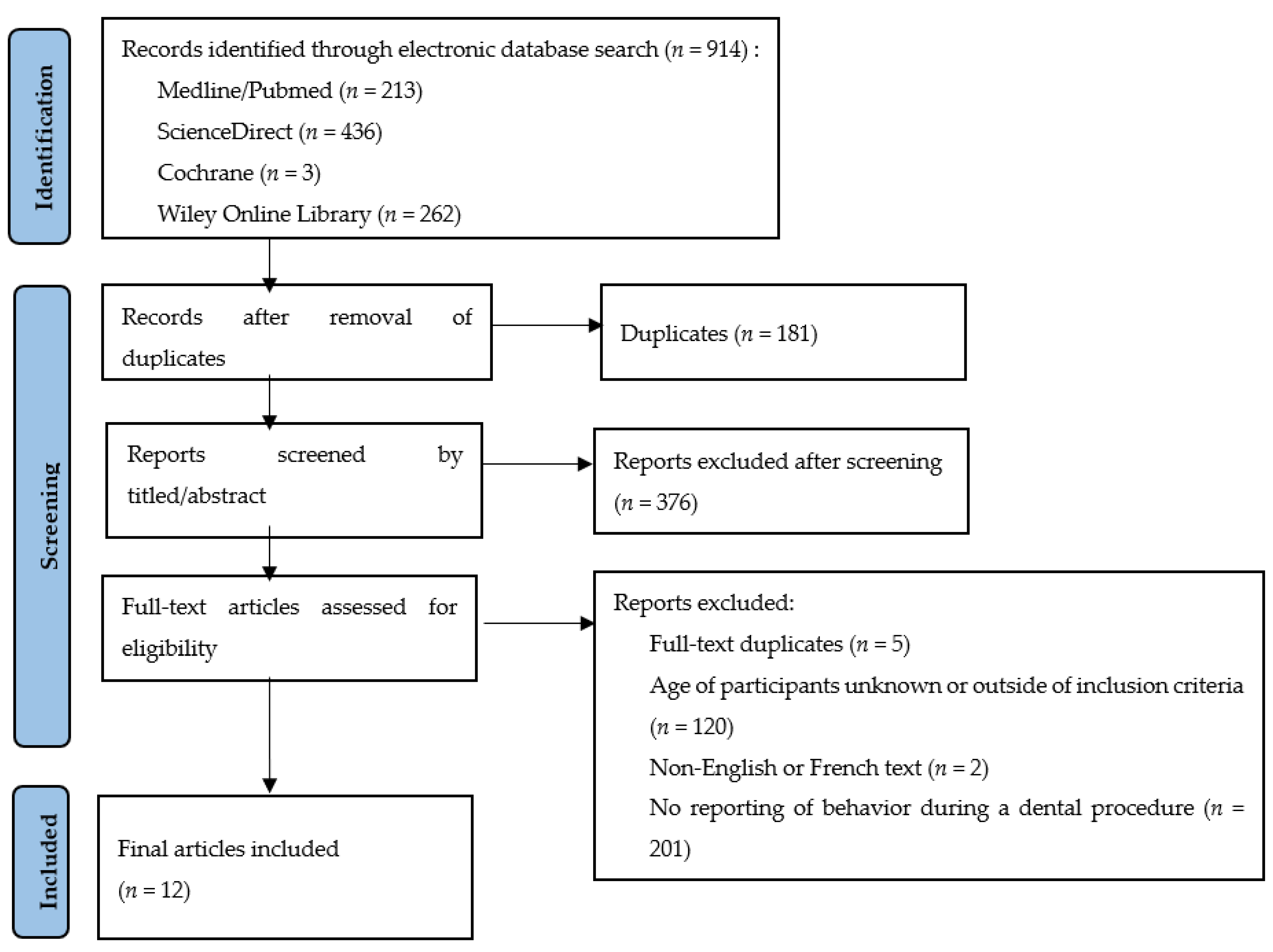
3.1. Literature Search
3.2. Descriptive Analysis
3.2.1. The Behaviour Style Questionnaire (BSQ) Scale
- Activity: the level of motor activity and the amount of time the child is active.
- Rhythmicity/regularity: patterns of eating, sleeping and other bodily functions.
- Approach and the withdrawal: ease of approaching people and situations.
- Adaptability: the way the child responds to changes in his/her environment.
- Response: the energy levels and intensity of the child’s response.
- Disposition: predominant quality of mood.
- Sensitivity: the threshold for stimuli.
- Distractibility: how easily the child can be distracted from what he is doing.
- Attention span/persistence: the span of time for which the child will pay attention to one thing when left to his/her own devices and their persistence with an activity. [22]
3.2.2. The Emotionality–Activity–Sociability (EAS) Scale
- Emotionality, distress: in the face of a threatening event, variations on this dimension can range from a stoic lack of reaction to distress beyond the child’s emotional control.
- Activity: the pace and energy of the child.
- Sociability: the desire to interact with the social environment.
- Impulsiveness is replaced by Shyness due to its lower-than-expected level of heritability. Shyness refers to inhibiting behaviours in the presence of strangers and a tendency to shy away from social interactions.
3.3. Child Behaviour in a Dental Environment
3.3.1. During the First Session with the Dentist
3.3.2. During Invasive Procedures
3.3.3. Patients Referred for Sedations
4. Discussion
- The approach, the withdrawal and the inability to adapt the BSQ/CBQ correspond to the sociability of EAS.
- The intensity of the reactions corresponds to the emotionality.
- The level of motor activity, as well as distractibility, corresponds to hyperactivity.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Klingberg, G. Dental Anxiety and Behaviour Management Problems in Paediatric Dentistry—A Review of Background Factors and Diagnostics. Eur. Arch. Paediatr. Dent. 2008, 9, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Seligman, L.D.; Hovey, J.D.; Chacon, K.; Ollendick, T.H. Dental Anxiety: An Understudied Problem in Youth. Clin. Psychol. Rev. 2017, 55, 25–40. [Google Scholar] [CrossRef] [PubMed]
- Houpt, M. Project USAP 2000-Use of Sedative Agents by Pediatric Dentists: A 15-Year Follow-up Survey. Pediatr. Dent. 2002, 24, 289–294. [Google Scholar] [PubMed]
- Rettew, D.C.; Mclee, L. Temperament and its role in developmental psychopathology. Harv. Rev. Psychiatry 2005, 13, 14–27. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.; Prior, M. Temperament and Stress Resilience in School-Age Children: A Within-Families Study. J. Am. Acad. Child. Adolesc. Psychiatry 1995, 34, 168–179. [Google Scholar] [CrossRef]
- Mathiesen, K.S.; Prior, M. The Impact of Temperament Factors and Family Functioning on Resilience Processes from Infancy to School Age. Eur. J. Dev. Psychol. 2006, 3, 357–387. [Google Scholar] [CrossRef]
- Lewis, A.J.; Olsson, C.A. Early Life Stress and Child Temperament Style as Predictors of Childhood Anxiety and Depressive Symptoms: Findings from the Longitudinal Study of Australian Children. Depress. Res. Treat. 2011, 2011, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Buss, A.H.; Plomin, R. Early Developing Personality Traits; Psychology Press: New York, NY, USA, 1984; Volume 3, Chapter 5–7, pp. 45–102. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Lochary, M.E.; Wilson, S.; Griffen, A.L.; Coury, D.L. Temperaments a Predictor of Behavior for Conscious sedation in Dentistry. Pediatr. Dent. 1993, 15, 348–352. [Google Scholar]
- Radis, F.G.; Wilson, S.; Griffen, A.L.; Coury, D.L. Temperament as a Predictor of Behavior during Initial Dental Examination in Children. Pediatr. Dent. 1994, 16, 121–127. [Google Scholar]
- Arnrup, K.; Broberg, A.G.; Berggren, U.; Bodin, L. Lack of Cooperation in Pediatric Dentistry—The Role of Child Personality Characteristics. Pediatr. Dent. 2002, 24, 119–128. [Google Scholar] [PubMed]
- Jensen, B.; Stjernqvist, K. Temperament and Acceptance of Dental Treatment under Sedation in Preschool Children. Acta Odontol. Scand. 2002, 60, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Isik, B.; Baygin, O.; Kapci, E.G.; Bodur, H. The Effects of Temperament and Behaviour Problems on Sedation Failure in Anxious Children after Midazolam Premedication. Eur. J. Anaesthesiol. 2010, 27, 336–340. [Google Scholar] [CrossRef] [PubMed]
- Aminabadi, N.A.; Puralibaba, F.; Erfanparast, L.; Najafpour, E.; Jamali, Z.; Adhami, S.E. Impact of Temperament on Child Behavior in the Dental Setting. J. Dent. Res. Dent. Clin. Dent. Prospects 2011, 5, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Lane, K.J.; Nelson, T.M.; Thikkurissy, S.; Scott, J.M. Assessing Temperament as a Predictor of Oral Sedation Success Using the Children’s Behavior Questionnaire Short Form. Pediatr. Dent. 2015, 37, 7. [Google Scholar]
- Pai, R.; Mandroli, P.; Benni, D.; Pujar, P. Prospective Analysis of Factors Associated with Dental Behavior Management Problems, in Children Aged 7–11 Years. J. Indian. Soc. Pedod. Prev. Dent. 2015, 33, 312–318. [Google Scholar] [CrossRef]
- Nelson, T.M.; Griffith, T.M.; Lane, K.J.; Thikkurissy, S.; Scott, J.M. Temperament as a Predictor of Nitrous Oxide Inhalation Sedation Success. Anesth. Prog. 2017, 64, 17–21. [Google Scholar] [CrossRef] [Green Version]
- Tsoi, A.K.; Wilson, S.; Thikkurissy, S. A Study of the Relationship of Parenting Styles, Child Temperament, and Operatory Behavior in Healthy Children. J. Clin. Pediatr. Dent. 2018, 42, 273–278. [Google Scholar] [CrossRef]
- Jain, A.; Suprabha, B.S.; Shenoy, R.; Rao, A. Association of Temperament with Dental Anxiety and Behaviour of the Preschool Child during the Initial Dental Visit. Eur. J. Oral Sci. 2019, 127, 147–155. [Google Scholar] [CrossRef]
- Janeshin, A.; Habibi, M. The Relationship between Temperament and Behavior in 3-7-Year-Old Children during Dental Treatment. Dent. Res. J. 2021, 18, 12. [Google Scholar] [CrossRef]
- Chess, S.; Thomas, A. The New York Longitudinal Study (NYLS): The Young Adult Periods. Can. J. Psychiatry 1990, 35, 557–561. [Google Scholar] [CrossRef] [PubMed]
- Gasman, L.; Purper-Ouakil, D.; Michel, G.; Mouren-Siméoni, M.C.; Bouvard, M.; Perez-Diaz, F.; Jouvent, R. Cross-Cultural Assessment of Childhood Temperament. A Confirmatory Factor Analysis of the French Emotionality Activity and Sociability (EAS) Questionnaire. Eur. Child. Adolesc. Psychiatry 2002, 11, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Rouxel, G.; Briec, J.; Juhel, J.; Le Maner-Idrissi, G. Analyse de la structure factorielle du questionnaire de tempérament EAS (version parents) auprès de deux échantillons d’enfants âgés de deux à cinq ans et de six à neuf ans. Eur. Rev. Appl. Psychol. 2013, 63, 173–183. [Google Scholar] [CrossRef]
- Garmezy, N.; Masten, A.S.; Tellegen, A. The Study of Stress and Competence in Children: A Building Block for Developmental Psychopathology. Child Dev. 1984, 55, 97. [Google Scholar] [CrossRef] [PubMed]
- Scaini, S.; Caputi, M.; Giani, L.; Forresi, B. Temperament Profiles to Differentiate between Stress-Resilient and Stress-Affected Children during COVID-19 Pandemic. Psychol. Hub 2022, 38, 7–16. [Google Scholar] [CrossRef]
- Kyrios, M.; Prior, M. Temperament, Stress and Family Factors in Behavioural Adjustment of 3–5-Year-Old Children. Int. J. Behav. Dev. 1990, 13, 67–93. [Google Scholar] [CrossRef]
- Wachs, T.D. Contributions of Temperament to Buffering and Sensitization Processes in Children’s Development. Ann. N. Y. Acad. Sci. 2006, 1094, 28–39. [Google Scholar] [CrossRef]
- Quinonez, R.; Santos, R.G.; Boyar, R.; Cross, H. Temperament and Trait Anxiety as Predictors of Child Behavior Prior to General Anesthesia for Dental Surgery. Pediatr. Dent. 1997, 19, 427–431. [Google Scholar]
- Kain, Z.N.; MacLaren, J.; McClain, B.C.; Saadat, H.; Wang, S.-M.; Mayes, L.C.; Anderson, G.M. Effects of Age and Emotionality on the Effectiveness of Midazolam Administered Preoperatively to Children. Anesthesiology 2007, 107, 545–552. [Google Scholar] [CrossRef]


{kind=link}
| # | Search Term |
|---|---|
| 1 | temperament [All Fields] AND dent [All Fields] |
| 2 | temperament [MeSH Terms] AND child [All Fields] AND dent [All Fields] |
| 3 | child’s temperament [All Fields] AND dent [All Fields] |
| 4 | toddler [All Fields] AND temperament [All Fields] AND dent [All Fields] |
| 5 | toddler [All Fields] AND temperament [All Fields] AND dent [All Fields] |
| 6 | dental behavior [All Fields] AND temperament [All Fields] |
| 7 | dental behavior [All Fields] AND temperament [All Fields] AND child [All Fields] |
| 8 | behavior [All Fields] AND child [All Fields] AND temperament [All Fields] |
| Author and Year of Publication | Age (Years) | N | Temperament Scale Used | Type of Procedure | Sedation Used | Behaviour Rating Scale | Results: Temperament Statistically Associated with DBMP |
|---|---|---|---|---|---|---|---|
| Lochary 1993 [10] | 18–36 months | 29 | TTS | Invasive: restoration under local anaesthesia | 2 mg/kg oral Hydroxyzine + 2 mg/kg submucosal Meperidine | Ohio State university Behavior Rating Scale (4 items) | Approach/withdrawal (p = 0.0015) Adaptability (p = 0.009) |
| Radis 1994 [11] | 3–5 | 50 | BSQ | Non-invasive: initial dental examination + X-rays + prophylaxis | None | Ohio State University Behavior Rating Scale | Low Approach/withdrawal (p = 0.0023) Low adaptability: (p = 0.0022) Intensity/crying: (p = 0.0351) Activity: (p = 0.0157) |
| Arnrup 2002 [12] | 4–13 | 203 | EASI + Rutter scale | Assessment of factors that influence children cooperation. No information found about the disruptive behaviour nor the dental procedure leading to this disruptive behaviour. | Emotionality (p < 0.001) Impulsivity (p < 0.001) | ||
| Jensen 2002 [13] | 17–51 months (4,5 years) | 50 | EAS + Shyness | Invasive: avulsion under local anaesthesia | 0.3 mg/kg intra-rectal Midazolam | Level of sedation (Wilton) + Child’s acceptance of procedure according to Host | Shyness (p = 0.05) Emotionality (p = 0.01) Mood changing |
| Isik 2010 [14] | 4–8 | 60 | STSC (30 items) + CPRS-R (80 items) | Invasive: treatment under local anaesthesia | 0.75 mg/kg oral Midazolam + N2O/O2 40/60% | Houpt Sedation Rating Scale (HSRS) | Inflexibility (p = 0.033) |
| Aminabadi 2011 [15] | 1–7 | 196 | ECBQ for 18–36 months and CBQ for 3–7 years old | Invasive: restoration under local anaesthesia | None | Frankl | Anger, irritability, fear, reaction, reactivity, shyness. (correlation coefficient = 0.33 p < 0.05) |
| Lane 2015 [16] | 36–95 months (7,9 years) | 61 | CBQ SF | Invasive: restoration under local anaesthesia | 0.3 mg/kg Midazolam + 1 mg/kg hydroxyzine + 1.5 mg/kg Meperidine (50 min latency) + MEOPA | Houpt Sedation Rating Scale (HSRS) | Impulsivity (p = 0.04) |
| Pai 2015 [17] | 7–11 | 165 | Standardized multi-factor questionnaire including personality | -Non-invasive -Moderately-invasive -Highly invasive (with local anaesthesia) | None | Venham | Sociability Interaction with siblings (p = 0.00001) Interaction with other children (p = 0.00001) Conduct towards parents (p = 0.00001) School performance (p = 0.0004) |
| Nelson 2017 [18] | 3–5,5 5,5–8 | 48 | CBQ-SF: 3 groups with 15 subgroups, 94 items | Invasive: restoration + tooth extraction under local anaesthesia | N2O/O2 50% | Frankl | Effortful control (p = 0.001): Attention control (p = 0.002), Inhibitory control (p = 0.001) Negativity Affectivity (p = 0.006): frustration (p = 0.006) sadness (p = 0.011) soothability (p = 0.006) Extraversion/surgency: activity (p = 0.004), impulsivity (p = 0.018) |
| Tsoi 2018 [19] | 4–12 | 113 | EAS | No information | No sedation reported | Frankl | Emotionality (r = 0.497 p < 0.001) Activity (r = 0.196 p < 0.03) Shyness (r = 0.281 p < 0.003) |
| Jain 2019 [20] | 3–5 | 100 | EAS | Non-invasive: initial dental examination + X-rays + prophylaxis | None | Frankl (score of 1–4) | Emotionality a(Spearman’s correlation coefficient rs = 0.28) (p = 0.046) Shyness associated with dental anxiety (rs = 0.28) (p = 0.897) Activity (p = 0.012) |
| Janeshin 2021 [21] | 3–7 | 215 | CBQ | Invasive: dental pulp treatment with local anaesthesia | None | Frankl | Mean scores of fear (p = 0.004) and perceptual sensitivity (p = 0.001) were higher in completely negative behaviour than other temperament traits |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Do, N.M.; Clauss, F.; Schmitt, M.; Manière, M.-C. Influence of Child’s Temperament on Behaviour Management Problems in the Dental Office: A Literature Review. Children 2023, 10, 90. https://doi.org/10.3390/children10010090
Do NM, Clauss F, Schmitt M, Manière M-C. Influence of Child’s Temperament on Behaviour Management Problems in the Dental Office: A Literature Review. Children. 2023; 10(1):90. https://doi.org/10.3390/children10010090
Chicago/Turabian StyleDo, Nhat Minh, François Clauss, Margot Schmitt, and Marie-Cécile Manière. 2023. "Influence of Child’s Temperament on Behaviour Management Problems in the Dental Office: A Literature Review" Children 10, no. 1: 90. https://doi.org/10.3390/children10010090