
The Development and Usability of a Mobile App for Parents of Children with ADHD

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
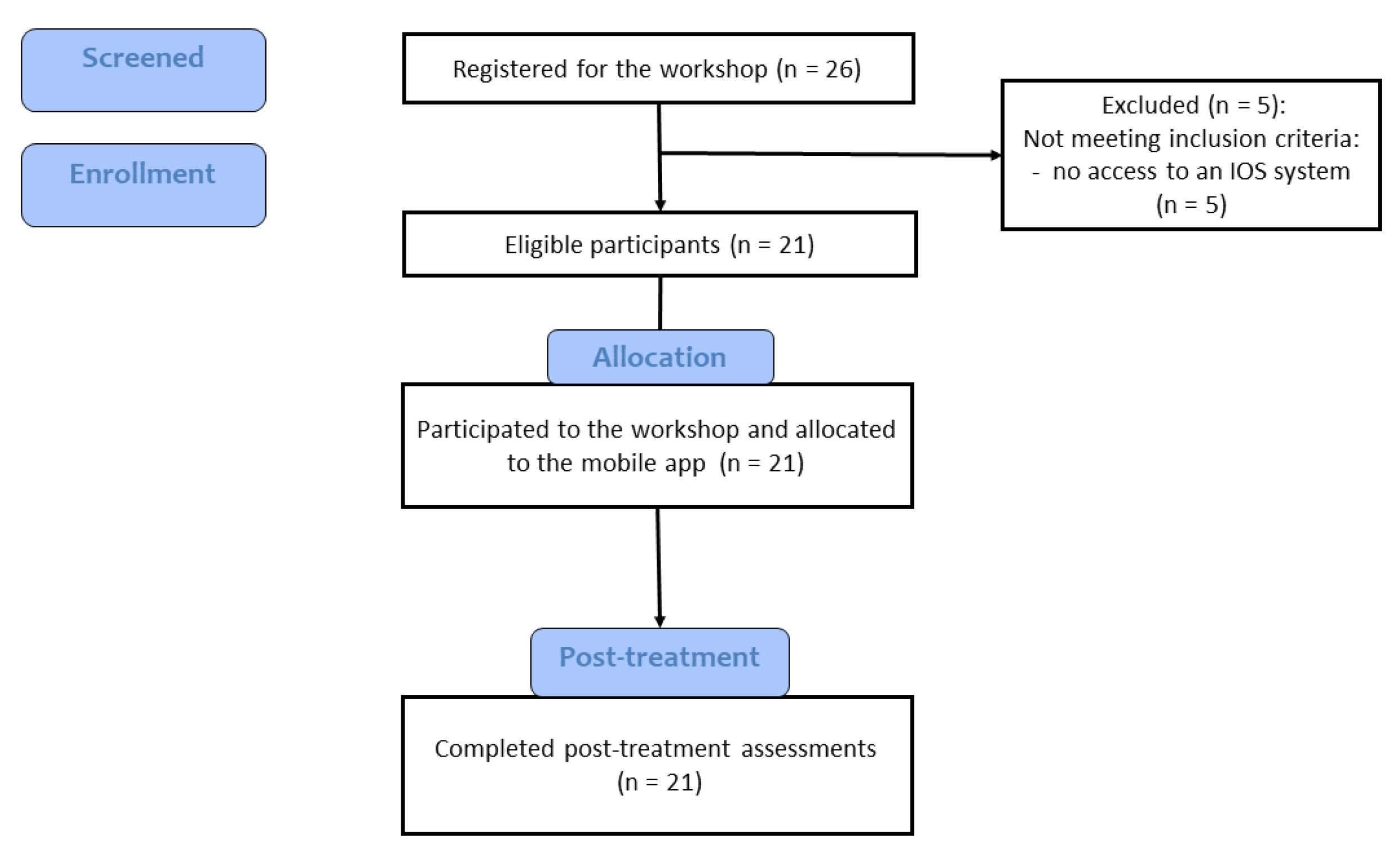
2.2. Participants
2.3. Description of the ADHD Coping Card App
2.3.1. The Psychoeducation Module
2.3.2. The Activities Section
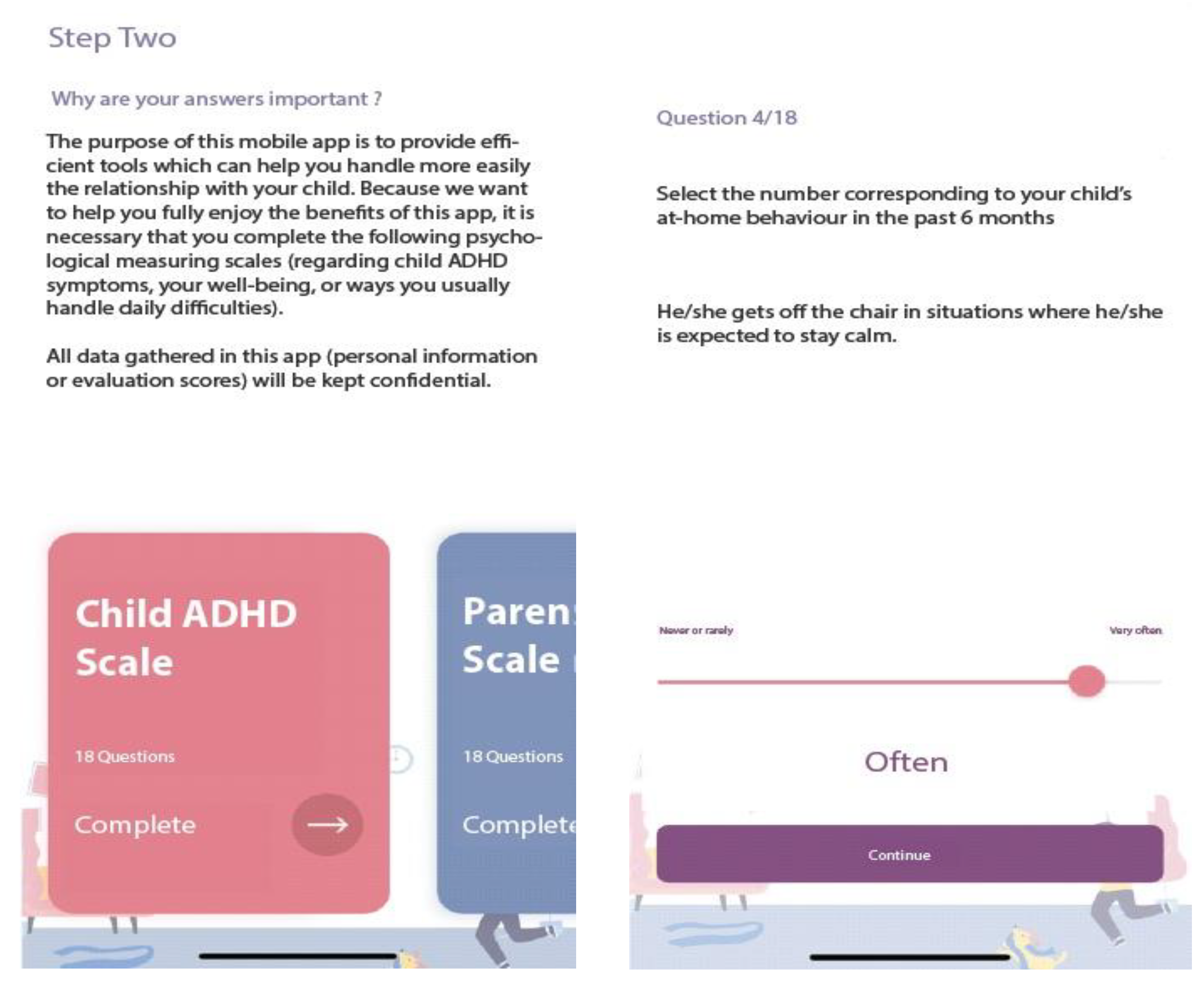
- ADHD symptoms. The Romanian version of the ADHD Rating Scale–IV [34] is used to measure child ADHD symptoms as reported by parents. The scale consists of 18 items, rated on a 4-point Likert scale using never or rarely, sometimes, often, or very often as responses. Scores can be computed for each dimension of ADHD (inattention, hyperactivity/impulsivity). Higher scores indicated higher ADHD symptoms. In the app, the results are presented in percentile scores (derived from the total score), indicating if this could be relevant for further investigation by a mental health specialist. Sample items: “Fails to give close attention to details or makes careless mistakes in schoolwork.”, “Is forgetful in daily activities.”
- Parenting. The Romanian version of the Alabama Parenting Questionnaire Short Form -9 [35] allows the assessment of parenting practices on three subscales: positive parenting, inconsistent discipline and poor supervision. It consists of 9 items (three items for each subscale), rated on a 5-point Likert scale, with responses rated from 1 (Never) to 5 (Always). Sample items: “You let your child know when he/she is doing a good job with something”, “You compliment your child after he/she has done something well”.
- Parental Burden. The Caregiving Burden Scale [36] is used to measure parents’ burden of taking care of children who have physical, emotional, and behavioral problems. It consists of 6 items, each rated on a 4-point Likert scale ranging from 0 (Never) to 3 (Almost everytime), higher total scores indicating more caregiving burden. Sample items: “During the past year, how much worry or concern did [CHILD]’s emotions, behavior, or learning abilities cause you?”, “During the past year, how often have you missed work because of [CHILD]’s emotional, behavioral, or learning problems?”
- Parental distress. The Ultra-Brief Screening Scale for Anxiety and Depression (PHQ-4; [37]) is used to measure parental psychological distress. The scale consists of 4 items (two measuring anxiety, two measuring depressive symptoms), rated on a 4-point Likert scale. PHQ-4 begins with the stem-question, “Over the last two weeks, how often have you been bothered by the following problems?” and responses are rated from 0 (“not at all”) to 3 (“nearly every day”). Sample items: “Feeling nervous, anxious or on edge”, “Little interest or pleasure in doing things”. In this app, we compute a total score on PHQ-4, indicating no-, low-, moderate-, or high-level of psychological distress.
- Satisfaction with the intervention scale. A scale with four questions previously used in another research [38] was used to measure parents’ satisfaction with the mobile app. The scale consists of four questions rated on a 4 point-Likert scale from 0 (Not at all) to 4 (Very much). Sample items: “How satisfied are you with the intervention?”, “Would you recommend this app to a friend?”
- Parental distress section
- Relaxation section
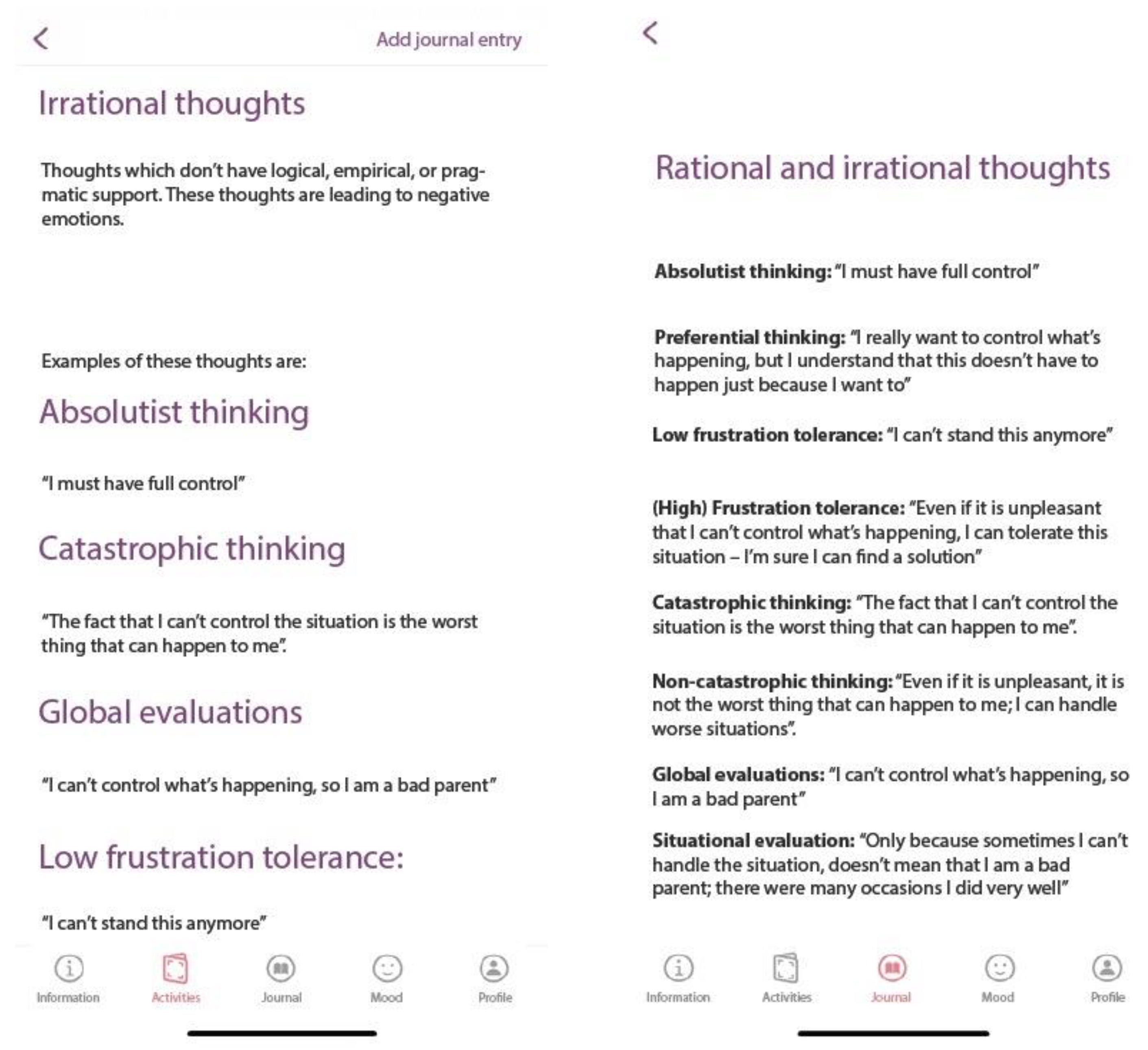
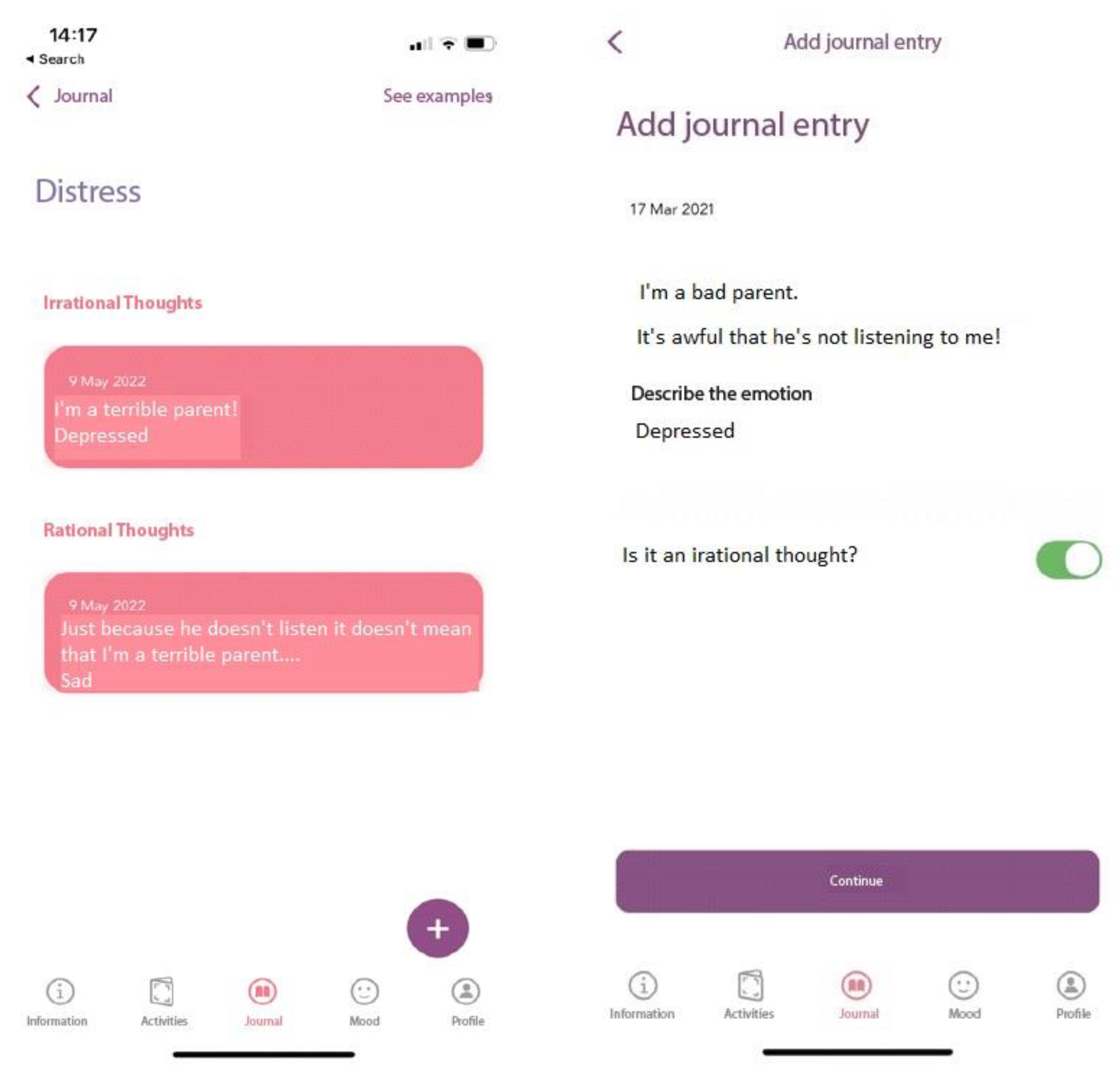
2.3.3. Journal Section
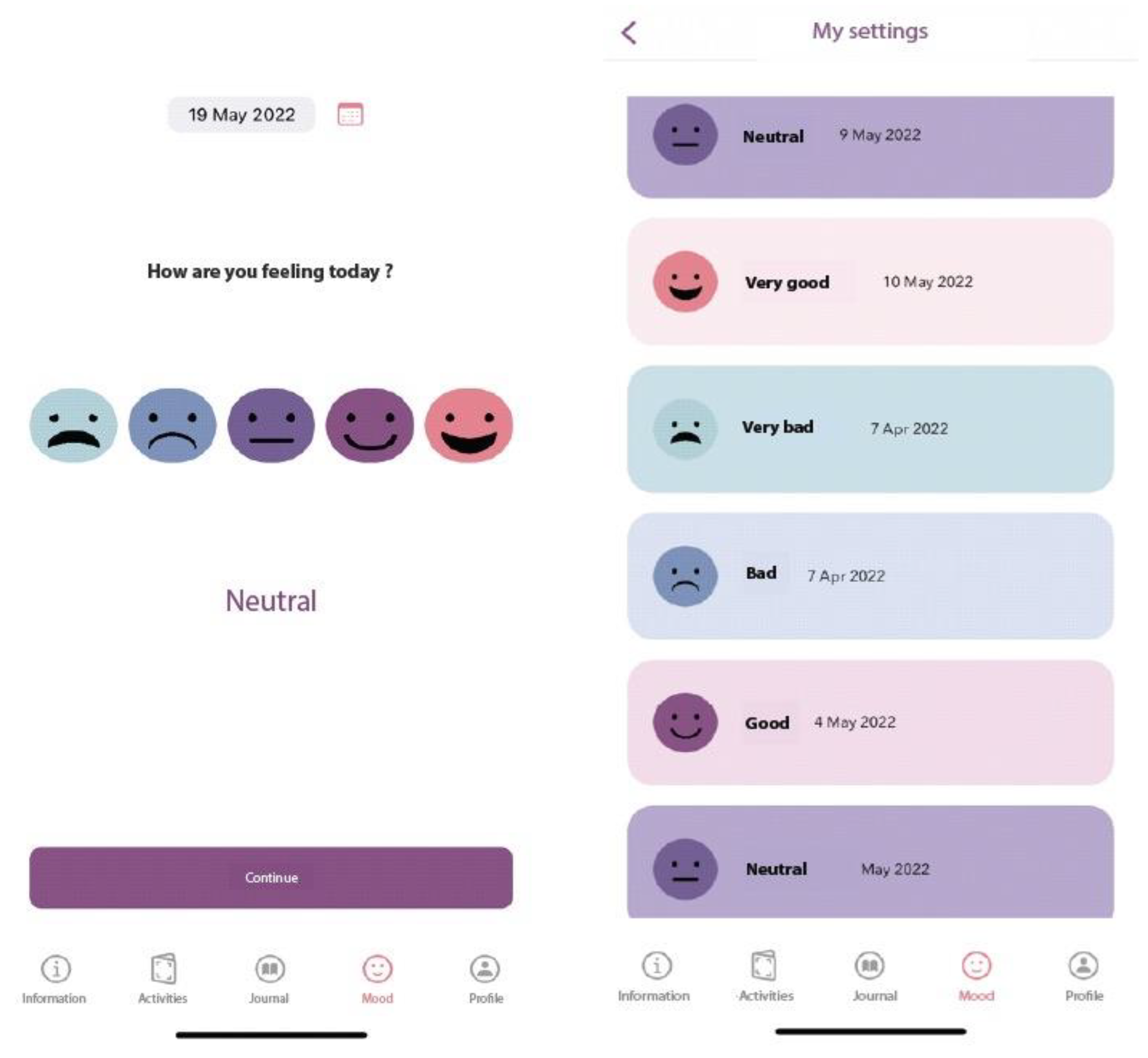
2.3.4. The Mood Monitoring Section
2.4. Measures
2.4.1. Demographic Information
2.4.2. Technology Use
2.4.3. Parents’ Attitudes Regarding Online Platforms
2.4.4. App Usability
2.4.5. User-Friendliness
2.4.6. Qualitative Feedback
2.5. Procedure
2.6. Statistical Analysis
3. Results
3.1. Parents’ Attitudes Regarding the Use of Digital Mental Health Applications
3.2. ADHD Coping Card Usability as Rated by Parents
3.3. User Friendly
3.4. Qualitative Feedback Regarding App and Future Improvements
4. Discussion
Limitations and Future Research Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Polanczyk, G.V.; Willcutt, E.G.; Salum, G.A.; Kieling, C.; Rohde, L.A. ADHD Prevalence Estimates across Three Decades: An Updated Systematic Review and Meta-Regression Analysis. Int. J. Epidemiol. 2014, 43, 434–442. [Google Scholar] [CrossRef]
- Di Lorenzo, R.; Balducci, J.; Poppi, C.; Arcolin, E.; Cutino, A.; Ferri, P.; D’Amico, R.; Filippini, T. Children and Adolescents with ADHD Followed up to Adulthood: A Systematic Review of Long-Term Outcomes. Acta Neuropsychiatr. 2021, 33, 283–298. [Google Scholar] [CrossRef]
- Kousgaard, S.J.; Boldsen, S.K.; Mohr-Jensen, C.; Lauritsen, M.B. The Effect of Having a Child with ADHD or ASD on Family Separation. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 1391–1399. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Page, T.F.; Altszuler, A.R.; Pelham, W.E.; Kipp, H.; Gnagy, E.M.; Coxe, S.; Schatz, N.K.; Merrill, B.M.; Macphee, F.L.; et al. Family Burden of Raising a Child with ADHD. J. Abnorm. Child Psychol. 2019, 47, 1327–1338. [Google Scholar] [CrossRef] [PubMed]
- Jendreizik, L.T.; von Wirth, E.; Döpfner, M. Familial Factors Associated With Symptom Severity in Children and Adolescents With ADHD: A Meta-Analysis and Supplemental Review. J. Atten. Disord. 2023, 27, 124–144. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.; Theule, J. Parental Psychopathology in Families of Children with ADHD: A Meta-Analysis. J. Child Fam. Stud. 2016, 25, 3451–3461. [Google Scholar] [CrossRef]
- Cheung, K.; Aberdeen, K.; Ward, M.A.; Theule, J. Maternal Depression in Families of Children with ADHD: A Meta-Analysis. J. Child Fam. Stud. 2018, 27, 1015–1028. [Google Scholar] [CrossRef]
- Insa, I.; Alda, J.A.; Chamorro, M.; Espadas, M.; Huguet, A. Difference in Psychic Distress Lived by Parents With ADHD Children and Parents With Healthy Children: Focus on Gender Differences. J. Atten. Disord. 2021, 25, 332–339. [Google Scholar] [CrossRef] [Green Version]
- Piscitello, J.; Altszuler, A.R.; Mazzant, J.R.; Babinski, D.E.; Gnagy, E.M.; Page, T.F.; Molina, B.S.G.; Pelham, W.E. The Impact of ADHD on Maternal Quality of Life. Res. Child Adolesc. Psychopathol. 2022, 50, 1275–1288. [Google Scholar] [CrossRef]
- Harrison, C.; Sofronoff, K. ADHD and Parental Psychological Distress: Role of Demographics, Child Behavioral Characteristics, and Parental Cognitions. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 703–711. [Google Scholar] [CrossRef]
- Dobrean, A.; Păsărelu, C.R.; Döpfner, M. Varieties of Psychotherapy for Attention-Deficit Hyperactivity Disorder: An Evidence-Based Evaluation. In Evidence-Based Psychotherapy: The State of the Science and Practice; David, D., Lynn, S.Y., Montgomery, G.H., Eds.; Wiley-Blackwell: Hoboken, NJ, USA, 2018; pp. 435–463. ISBN 978-1-118-62552-1. [Google Scholar]
- National Institute for Clinical Excellence. Attention Deficit Hyperactivity Disorder: Diagnosis and Management. Available online: https://www.nice.org.uk/guidance/ng87 (accessed on 22 August 2022).
- Chacko, A.; Jensen, S.A.; Lowry, L.S.; Cornwell, M.; Chimklis, A.; Chan, E.; Lee, D.; Pulgarin, B. Engagement in Behavioral Parent Training: Review of the Literature and Implications for Practice. Clin. Child Fam. Psychol. Rev. 2016, 19, 204–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarke, A.T.; Marshall, S.A.; Mautone, J.A.; Soffer, S.L.; Jones, H.A.; Costigan, T.E.; Patterson, A.; Jawad, A.F.; Power, T.J. Parent Attendance and Homework Adherence Predict Response to a Family–School Intervention for Children With ADHD. J. Clin. Child Adolesc. Psychol. 2015, 44, 58–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, D.J.; Loiselle, R.; Zachary, C.; Georgeson, A.R.; Highlander, A.; Turner, P.; Youngstrom, J.K.; Khavjou, O.; Anton, M.T.; Gonzalez, M.; et al. Optimizing Engagement in Behavioral Parent Training: Progress Toward a Technology-Enhanced Treatment Model. Behav. Ther. 2021, 52, 508–521. [Google Scholar] [CrossRef]
- Andersson, G.; Titov, N. Advantages and Limitations of Internet-Based Interventions for Common Mental Disorders. World Psychiatry 2014, 13, 4–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, D.J.; Naslund, J.A.; Bantjes, J. COVID-19 and the Global Acceleration of Digital Psychiatry. Lancet Psychiatry 2022, 9, 8–9. [Google Scholar] [CrossRef]
- Lindhiem, O.; Bennett, C.B.; Rosen, D.; Silk, J. Mobile Technology Boosts the Effectiveness of Psychotherapy and Behavioral Interventions: A Meta-Analysis. Behav. Modif. 2015, 39, 785–804. [Google Scholar] [CrossRef] [PubMed]
- Powell, A.C.; Chen, M.; Thammachart, C. The Economic Benefits of Mobile Apps for Mental Health and Telepsychiatry Services When Used by Adolescents. Child Adolesc. Psychiatr. Clin. 2017, 26, 125–133. [Google Scholar] [CrossRef]
- Păsărelu, C.R.; Andersson, G.; Dobrean, A. Attention-Deficit/Hyperactivity Disorder Mobile Apps: A Systematic Review. Int. J. Med. Inform. 2020, 138, 104133. [Google Scholar] [CrossRef]
- Weisman, O.; Schonherz, Y.; Harel, T.; Efron, M.; Elazar, M.; Gothelf, D. Testing the Efficacy of a Smartphone Application in Improving Medication Adherence, Among Children with ADHD. Isr. J. Psychiatry 2018, 55, 59–64,67. [Google Scholar] [CrossRef]
- Schuck, S.; Emmerson, N.; Ziv, H.; Collins, P.; Arastoo, S.; Warschauer, M.; Crinella, F.; Lakes, K. Designing an IPad App to Monitor and Improve Classroom Behavior for Children with ADHD: ISelfControl Feasibility and Pilot Studies. PLoS ONE 2016, 11, e0164229. [Google Scholar] [CrossRef]
- Schoenfelder, E.; Moreno, M.; Wilner, M.; Whitlock, K.B.; Mendoza, J.A. Piloting a Mobile Health Intervention to Increase Physical Activity for Adolescents with ADHD. Prev. Med. Rep. 2017, 6, 210–213. [Google Scholar] [CrossRef] [PubMed]
- Selaskowski, B.; Steffens, M.; Schulze, M.; Lingen, M.; Aslan, B.; Rosen, H.; Kannen, K.; Wiebe, A.; Wallbaum, T.; Boll, S.; et al. Smartphone-Assisted Psychoeducation in Adult Attention-Deficit/Hyperactivity Disorder: A Randomized Controlled Trial. Psychiatry Res. 2022, 317, 114802. [Google Scholar] [CrossRef]
- Jang, S.; Kim, J.-J.; Kim, S.-J.; Hong, J.; Kim, S.; Kim, E. Mobile App-Based Chatbot to Deliver Cognitive Behavioral Therapy and Psychoeducation for Adults with Attention Deficit: A Development and Feasibility/Usability Study. Int. J. Med. Inform. 2021, 150, 104440. [Google Scholar] [CrossRef] [PubMed]
- Powell, L.; Parker, J.; Harpin, V. ADHD: Is There an App for That? A Suitability Assessment of Apps for the Parents of Children and Young People With ADHD. JMIR mHealth uHealth 2017, 5, e7941. [Google Scholar] [CrossRef] [Green Version]
- Mirri, S.; Roccetti, M.; Salomoni, P. Collaborative Design of Software Applications: The Role of Users. Hum. Centric Comput. Inf. Sci. 2018, 8, 6. [Google Scholar] [CrossRef] [Green Version]
- Virzi, R.A. Refining the Test Phase of Usability Evaluation: How Many Subjects Is Enough? Hum. Factors 1992, 34, 457–468. [Google Scholar] [CrossRef]
- Macefield, R. How To Specify the Participant Group Size for Usability Studies: A Practitioner’s Guide. J. User Exp. 2009, 5, 34–45. [Google Scholar]
- Döpfner, M.; Schürmann, S.; Frölich, J. Program Psihoterapeutic Pentru Copii Cu Tulburare Hiperchinetică Şi Comportamente de Tip Opoziţional (THOP); RTS 2010: Cluj-Napoca, Romania, 2006. [Google Scholar]
- David, D.; Dobrean, A.; Păsărelu, C.R.; Iftene, F.; Lupu, V.; Predescu, E.; Döpfner, M. Psychotherapy, Atomoxetine or Both? Preliminary Evidence from a Comparative Study of Three Types of Treatment for Attention-Deficit/Hyperactivity Disorder in Children. Cogn. Ther. Res. 2021, 45, 149–165. [Google Scholar] [CrossRef]
- Ellis, A. Reason and Emotion in Psychotherapy: Revised and Updated; Carol Publishing Group: Secaucus, NJ, USA, 1994. [Google Scholar]
- Faraone, S.V.; Banaschewski, T.; Coghill, D.; Zheng, Y.; Biederman, J.; Bellgrove, M.A.; Newcorn, J.H.; Gignac, M.; Al Saud, N.M.; Manor, I.; et al. The World Federation of ADHD International Consensus Statement: 208 Evidence-Based Conclusions about the Disorder. Neurosci. Biobehav. Rev. 2021, 128, 789–818. [Google Scholar] [CrossRef] [PubMed]
- Dobrean, A.; Păsărelu, C.-R.; Balazsi, R.; Predescu, E. Measurement Invariance of the ADHD Rating Scale–IV Home and School Versions Across Age, Gender, Clinical Status, and Informant. Assessment 2021, 28, 86–99. [Google Scholar] [CrossRef] [PubMed]
- Florean, I.S.; Dobrean, A.; Balazsi, R.; Roșan, A.; Păsărelu, C.R.; Predescu, E.; Rad, F. Measurement Invariance of Alabama Parenting Questionnaire Across Age, Gender, Clinical Status, and Informant. Assessment 2022. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Wagner, K.M.; Valdez, C.R. The Relationship Between Maternal Depression, Externalizing and Internalizing Problems in Children, and Caregiving Burden in Urban Low-Income Ethnic and Racial Minority Families. Child Psychiatry Hum. Dev. 2020, 51, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Löwe, B. An Ultra-Brief Screening Scale for Anxiety and Depression: The PHQ–4. Psychosomatics 2009, 50, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Păsărelu, C.-R.; Dobrean, A.; Andersson, G.; Zaharie, G.C. Feasibility and Clinical Utility of a Transdiagnostic Internet-Delivered Rational Emotive and Behavioral Intervention for Adolescents with Anxiety and Depressive Disorders. Internet Interv. 2021, 26, 100479. [Google Scholar] [CrossRef]
- Döpfner, M.; Wähnke, L.; Klemp, M.-T.; Mühlenmeister, J.; Schürmann, S.; Hellmich, M.; Plück, J. Efficacy of Web-Assisted Self-Help for Parents of Children with ADHD (WASH)—A Three-Arm Randomized Trial under Field/Routine Care Conditions in Germany. BMC Psychiatry 2020, 20, 76. [Google Scholar] [CrossRef] [Green Version]
- Bangor, A.; Kortum, P.T.; Miller, J.T. An Empirical Evaluation of the System Usability Scale. Int. J. Hum. Comput. Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- Brooke, J. SUS: A “Quick and Dirty” Usability Scale. In Usability Evaluation in Industry; Jordan, P.W., Thomas, B., McClelland, I.L., Weerdmeester, B., Eds.; CRC Press: Boca Raton, FL, USA, 1996; ISBN 978-0-429-15701-1. [Google Scholar]
- Lewis, J.R. The System Usability Scale: Past, Present, and Future. Int. J. Hum. Comput. Interact. 2018, 34, 577–590. [Google Scholar] [CrossRef]
- Florean, I.S.; Dobrean, A.; Păsărelu, C.R.; Georgescu, R.D.; Milea, I. The Efficacy of Internet-Based Parenting Programs for Children and Adolescents with Behavior Problems: A Meta-Analysis of Randomized Clinical Trials. Clin. Child Fam. Psychol. Rev. 2020, 23, 510–528. [Google Scholar] [CrossRef] [PubMed]
- Faraone, S.V.; Larsson, H. Genetics of Attention Deficit Hyperactivity Disorder. Mol. Psychiatry 2019, 24, 562–575. [Google Scholar] [CrossRef] [Green Version]
- Friedman, L.M.; Dvorsky, M.R.; McBurnett, K.; Pfiffner, L.J. Do Parents’ ADHD Symptoms Affect Treatment for Their Children? The Impact of Parental ADHD on Adherence to Behavioral Parent Training for Childhood ADHD. J. Abnorm. Child Psychol. 2020, 48, 1425–1437. [Google Scholar] [CrossRef]
- Sonuga-barke, E.J.S.; Daley, D.; Thompson, M. Does Maternal ADHD Reduce the Effectiveness of Parent Training for Preschool Children’s ADHD? J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Dekkers, T.J.; Hornstra, R.; van der Oord, S.; Luman, M.; Hoekstra, P.J.; Groenman, A.P.; van den Hoofdakker, B.J. Meta-Analysis: Which Components of Parent Training Work for Children With Attention-Deficit/Hyperactivity Disorder? J. Am. Acad. Child Adolesc. Psychiatry 2022, 61, 478–494. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Theme 1 | Theme 2 | Theme 3 | Theme 4 | Theme 5 | Theme 6 | Theme 7 | |
|---|---|---|---|---|---|---|---|
| 1. What characteristics should a mobile app have in order to be useful to parents? | Simple information (3 parents) | Relevant and valid information (10 parents) | User friendly (5 parents) | To be able to use it with children (2 parents) | |||
| 2. What did you liked about this mobile application? | The design (8 parents) | User friendly and simple information (9 parents) | Activities that target parent-child relationship (8 parents) | Relaxation module (6 parents) | Mood monitoring module (6 parents) | The journals (3 parents) | Parental distress module (3 parents) |
| 3. What didn’t you like about this mobile application? | The delivery form of the information (7 parents) | Psychological assessments (3 parents) | The difficulty level of the information (2 parents) | The small number of parent-child activities (2 parents) | |||
| 4. Which functionalities would you eliminate from the app? | Psychological assessments (6 parents) | Psychoeducation module (1 parent) | The relaxation module (2 parents) | ||||
| 5. What functionalities would you add to the app? | Information about other psychological difficulties (5 parents) | Video and audio recordings rather than text information (4 parents) | More parent-child activities (3 parents) | ||||
| 6. App improvement suggestions | A simpler way to deliver the content (6 parents) | To remove mandatory activities (1 parent) | To replace the text content with video/ audio recording (2 parents) | ||||
| 7. Barriers identified for using of this mobile app | Age (1 parent) | Time resources (6 parents) | Financial barriers (3 parents) | Technical knowledge (1 parent) | Parents’ patience (3 parents) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Păsărelu, C.-R.; Kertesz, R.; Dobrean, A. The Development and Usability of a Mobile App for Parents of Children with ADHD. Children 2023, 10, 164. https://doi.org/10.3390/children10010164
Păsărelu C-R, Kertesz R, Dobrean A. The Development and Usability of a Mobile App for Parents of Children with ADHD. Children. 2023; 10(1):164. https://doi.org/10.3390/children10010164
Chicago/Turabian StylePăsărelu, Costina-Ruxandra, Reka Kertesz, and Anca Dobrean. 2023. "The Development and Usability of a Mobile App for Parents of Children with ADHD" Children 10, no. 1: 164. https://doi.org/10.3390/children10010164