
Delta Neutrophil Index Does Not Differentiate Bacterial Infection without Bacteremia from Viral Infection in Pediatric Febrile Patients

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
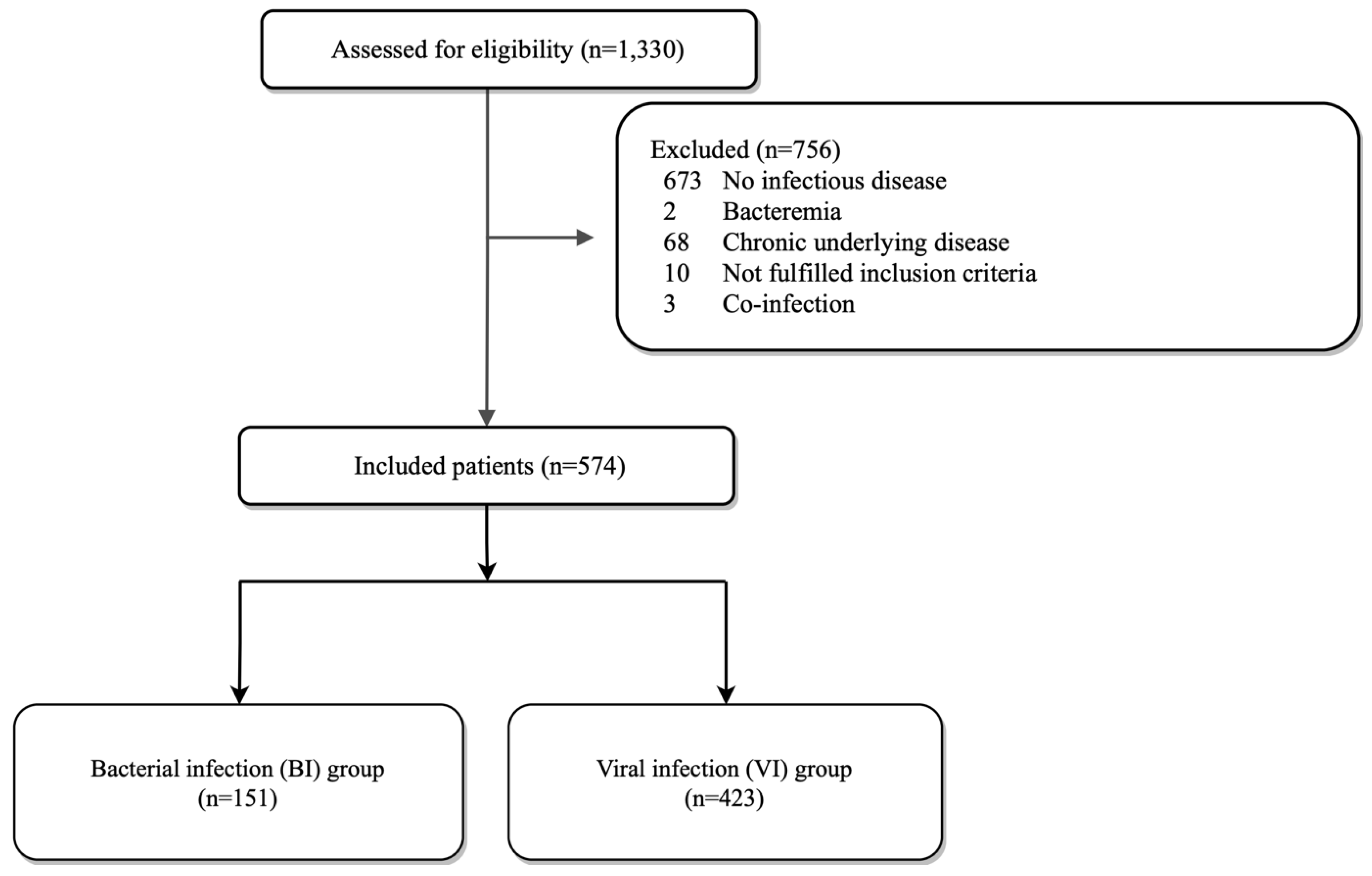
2.2. Participants
2.3. Outcome Measurement
2.4. Statistics
2.5. Ethics
2.6. Results
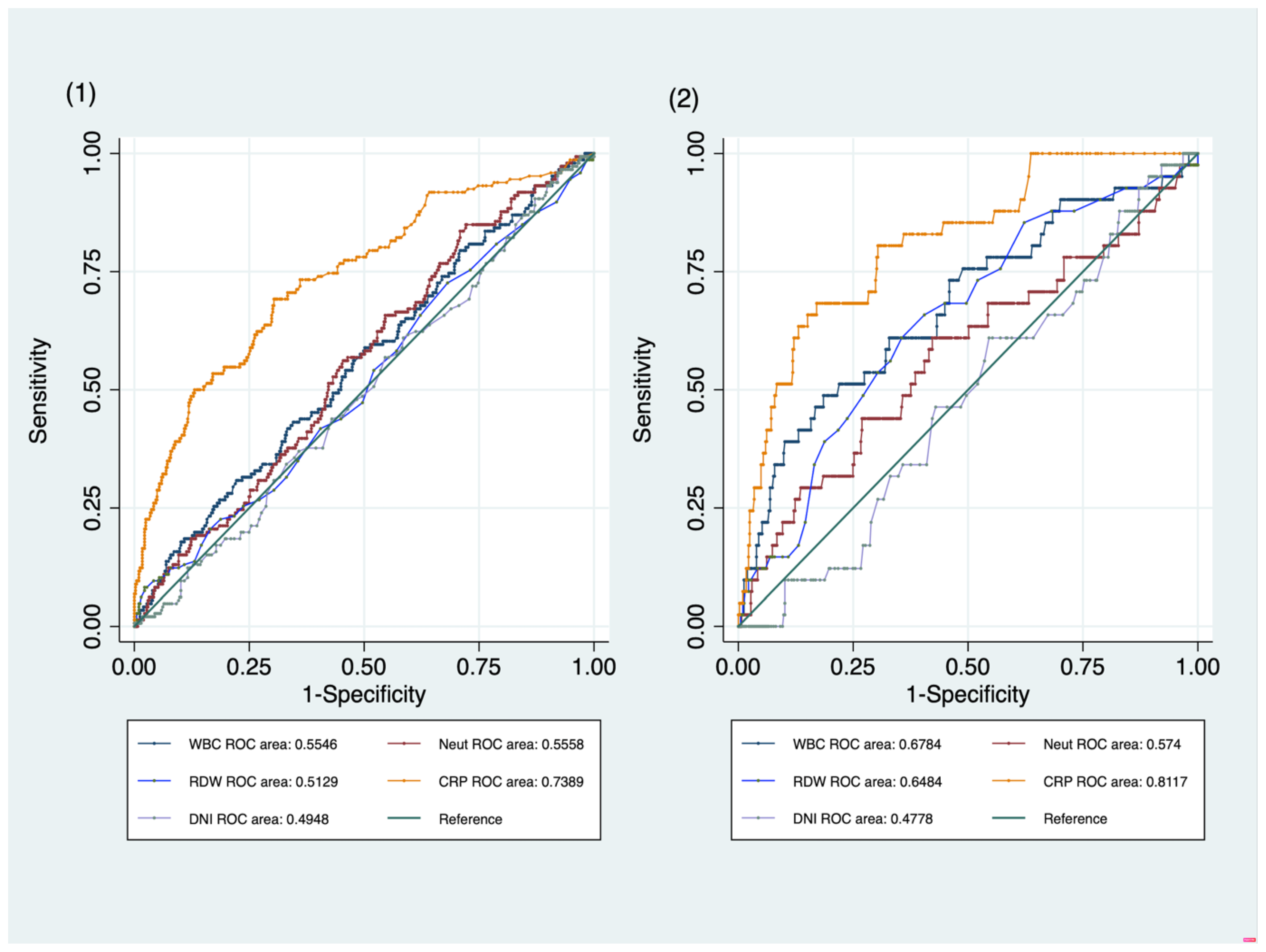
2.7. Primary Outcome
2.8. Secondary Outcome
2.9. Sensitivity Analysis
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AUROC | area under the ROC |
| BIWB | bacterial infection without bacteremia |
| CBC | complete blood count |
| CI | confidence interval |
| CRP | c-reactive protein |
| CSF | cerebrospinal fluid |
| DNI | delta neutrophil index |
| ED | emergency department |
| RDW | red cell distribution width |
| SBI | serious bacterial infection |
| UTI | urinary tract infection |
| VI | viral infection |
| WBC | white blood cell count |
References
- Poirier, M.P.; Davis, P.H.; Rey, J.A.G.D.; Monroe, K.W. Pediatric emergency department nurses’ perspectives on fever in children. Pediatr. Emerg. Care 2000, 16, 9–12. [Google Scholar] [CrossRef]
- Sands, R.; Shanmugavadivel, D.; Stephenson, T.; Wood, D. Medical problems presenting to paediatric emergency departments: 10 years on. Emerg. Med. J. 2012, 29, 379. [Google Scholar] [CrossRef]
- Kwak, Y.H.; Kim, D.K.; Jang, H.Y. Utilization of Emergency Department by Children in Korea. J. Korean Med. Sci. 2012, 27, 1222–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbi, E.; Marzuillo, P.; Neri, E.; Naviglio, S.; Krauss, B.S. Fever in Children: Pearls and Pitfalls. Children 2017, 4, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, K.K.; Lyman, J.A. Updated review of blood culture contamination. Clin. Microbiol. Rev. 2006, 19, 788–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstein, M.P. Blood culture contamination: Persisting problems and partial progress. J. Clin. Microbiol. 2003, 41, 2275–2278. [Google Scholar] [CrossRef] [Green Version]
- Lamy, B. Blood culture time-to-positivity: Making use of the hidden information. Clin. Microbiol. Infect. 2019, 25, 268–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stol, K.; Nijman, R.G.; van Herk, W.; van Rossum, A.M.C. Biomarkers for Infection in Children: Current Clinical Practice and Future Perspectives. Pediatr. Infect. Dis. J. 2019, 38 (Suppl. S1), S7–S13. [Google Scholar] [CrossRef]
- Miller, J.M.; Binnicker, M.J.; Campbell, S.; Carroll, K.C.; Chapin, K.C.; Gilligan, P.H.; Gonzalez, M.D.; Jerris, R.C.; Kehl, S.C.; Patel, R.; et al. A Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2018 Update by the Infectious Diseases Society of America and the American Society for Microbiology. Clin. Infect. Dis. 2018, 67, 813–816. [Google Scholar] [CrossRef] [Green Version]
- Nahm, C.H.; Choi, J.W.; Lee, J. Delta neutrophil index in automated immature granulocyte counts for assessing disease severity of patients with sepsis. Ann. Clin. Lab. Sci. 2008, 38, 241–246. [Google Scholar] [PubMed]
- Ansari-Lari, M.A.; Kickler, T.S.; Borowitz, M.J. Immature granulocyte measurement using the Sysmex XE-2100. Relationship to infection and sepsis. Am. J. Clin. Pathol. 2003, 120, 795–799. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.W.; Yoon, J.H.; Jin, S.J.; Kim, S.B.; Ku, N.S.; Jeong, S.J.; Han, S.H.; Choi, J.Y.; Kim, J.M.; Song, Y.G. Delta Neutrophil Index as a Prognostic Marker of Early Mortality in Gram Negative Bacteremia. Infect. Chemother. 2014, 46, 94–102. [Google Scholar] [CrossRef] [Green Version]
- Hwang, Y.J.; Chung, S.P.; Park, Y.S.; Chung, H.S.; Lee, H.S.; Park, J.W.; Lee, J.W.; Hong, J.H.; You, J.S.; Park, I. Newly designed delta neutrophil index–to–serum albumin ratio prognosis of early mortality in severe sepsis. Am. J. Emerg. Med. 2015, 33, 1577–1582. [Google Scholar] [CrossRef] [PubMed]
- Koh, I.D.; Jeon, I.S.; Kim, H.M. Diagnostic Significance of the Delta Neutrophil Index and Other Conventional Parameters in Neonatal Bacteremia. Pediatr. Infect. Vaccine 2017, 24, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Dagys, A.; Laucaitytė, G.; Volkevičiūtė, A.; Abramavičius, S.; Kėvalas, R.; Vitkauskienė, A.; Jankauskaitė, L. Blood biomarkers in early bacterial infection and sepsis diagnostics in feverish young children. Int. J. Med. Sci. 2022, 19, 753–761. [Google Scholar] [CrossRef]
- Marom, R.; Sakran, W.; Antonelli, J.; Horovitz, Y.; Zarfin, Y.; Koren, A.; Miron, D. Quick identification of febrile neonates with low risk for serious bacterial infection: An observational study. Arch. Dis. Child-Fetal Neonatal Ed. 2007, 92, F15. [Google Scholar]
- Shaikh, K.J.; Osio, V.A.; Leeflang, M.M.; Shaikh, N. Procalcitonin, C-reactive protein, and erythrocyte sedimentation rate for the diagnosis of acute pyelonephritis in children. Cochrane Databade Syst. Rev. 2020, 9, CD009185. [Google Scholar]
- Yang, X.; Zhang, Y.; Lin, H.; Zhong, H.; Wu, Z. Diagnostic Value of the Triple Combination of Serum Heparin-Binding Protein, Procalcitonin, and C-Reactive Protein in Children with Acute Bacterial Upper Respiratory Tract Infection. J. Healthc. Eng. 2022, 2022, 1877960. [Google Scholar] [CrossRef]
- Yo, C.H.; Hsieh, P.S.; Lee, S.H.; Wu, J.Y.; Chang, S.S.; Tasi, K.C.; Lee, C.C. Comparison of the Test Characteristics of Procalcitonin to C-Reactive Protein and Leukocytosis for the Detection of Serious Bacterial Infections in Children Presenting with Fever without Source: A Systematic Review and Meta-analysis. Ann. Emerg. Med. 2012, 60, 591–600. [Google Scholar] [CrossRef]
- Den Bruel, A.V.; Thompson, M.J.; Haj-Hassan, T.; Stevens, R.; Moll, H.; Lakhanpaul, M.; Mant, D. Diagnostic value of laboratory tests in identifying serious infections in febrile children: Systematic review. Bmj 2011, 342, d3082. [Google Scholar] [CrossRef] [Green Version]
- Celik, I.H.; Arifoglu, I.; Arslan, Z.; Aksu, G.; Bas, A.Y.; Demirel, N. The value of delta neutrophil index in neonatal sepsis diagnosis, follow-up and mortality prediction. Early Hum. Dev. 2019, 131, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Byeon, H.J.; Lee, K.H.; Lee, J.W.; Kronbichler, A.; Eisenhut, M.; Shin, J.I. Delta neutrophil index (DNI) as a novel diagnostic and prognostic marker of infection: A systematic review and meta-analysis. Inflamm. Res. 2017, 66, 863–870. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | VI Group N = 423 | BIWB Group N = 151 | Odd Ratio | 95% CI | p Value |
|---|---|---|---|---|---|
| Male, N (%) | 251 (59.3) | 84 (55.6) | 1.55 | 0.92~2.63 | 0.098 |
| Age (years), median (IQR) | 2.83 (1.00~6.25) | 3.92 (1.00~8.50) | 1.04 | 0.97~1.11 | 0.227 |
| Body temperature, mean ± SD | 37.9 ± 0.1 | 38.1 ± 0.1 | 1.11 | 0.87~1.42 | 0.386 |
| Symptom duration (days). mean ± SD | 3.36 ± 0.13 | 4.02 ± 0.24 | 1.00 | 0.86~1.16 | 0.953 |
| Hospital stays (days). median (IQR) | 0 (0~1) | 1 (0~3) | 1.35 | 1.16~1.57 | <0.05 |
| White blood cell count, N/uL, mean ± SD | 10,832 ± 5115 | 11,760 ± 5188 | 1.00 | 0.99~1.00 | 0.091 |
| Neutrophil, N/uL median (IQR) | 5770 (3580~9840) | 6740 (4390~10,210) | 0.99 | 0.99~1.00 | 0.129 |
| RDW, %, mean ± SD | 13.12 ± 0.98 | 13.20 ± 1.54 | 1.02 | 0.82~1.28 | 0.840 |
| Delta neutrophil index, % | 3.07 ± 5.82 | 3.51 ± 6.90 | 0.97 | 0.93~1.01 | 0.146 |
| C-Reactive protein, mg/dL | 1.39 ± 2.12 | 4.56 ± 5.45 | 1.28 | 1.17~1.41 | <0.05 |
| Diagnosis at ED, N (%) | <0.05 | ||||
| Upper respiratory infection | 166 (39.2) | 19 (12.6) | |||
| Lower respiratory infection | 43 (10.2) | 43 (28.5) | |||
| Gastrointestinal infection | 131 (31.0) | 37 (24.5) | |||
| Genitourinary infection | 0 (0.0) | 42 (27.8) | |||
| CNS infection | 24 (5.7) | 0 (0.0) | |||
| Soft tissue infection | 0 (0.0) | 3 (2.0) | |||
| Neonatal sepsis | 12 (2.8) | 0 (0.0) | |||
| Other infection | 47 (11.1) | 7 (4.6) |
| Characteristics | VI Group (N= 423) | UTI Group (N = 42) | Odd Ratio | 95% CI | p Value |
|---|---|---|---|---|---|
| Male, N (%) | 251 (59.3) | 26 (61.9) | 1.55 | 0.92~2.63 | 0.098 |
| Age (years), median (IQR) | 2.83 (1.00~6.25) | 0.38 (0.17~1.00) | 1.04 | 0.97~1.11 | 0.227 |
| Body temperature, mean ± SD | 37.9 ± 0.1 | 38.5 ± 1.1 | 1.11 | 0.87~1.42 | 0.386 |
| Symptom duration (days). mean ± SD | 3.36 ± 0.13 | 2.55 ± 1.58 | 1.00 | 0.86~1.16 | 0.953 |
| Hospital stays (days). median (IQR) | 0 (0~1) | 2 (1~3) | 1.35 | 1.16~1.57 | <0.05 |
| White blood cell count, N/uL, mean ± SD | 10,832 ± 5115 | 14,198 ± 6158 | 1.00 | 1.00~1.00 | <0.05 |
| Neutrophil, N/uL, median (IQR) | 5770 (3580~9840) | 7505 (3820~11,910) | 0.99 | 0.99~0.99 | <0.05 |
| RDW, %, mean ± SD | 13.12 ± 0.98 | 13.45 ± 2.07 | 1.01 | 0.80~1.48 | 0.599 |
| Delta neutrophil index, % | 3.07 ± 5.82 | 2.91 ± 3.19 | 0.97 | 0.91~1.03 | 0.278 |
| C-Reactive protein, mg/dL | 1.39 ± 2.12 | 4.40 ± 3.64 | 1.27 | 1.11~1.45 | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.; Lee, J.H.; Kwak, Y.H.; Kim, H.K.; Kwon, H.; Suh, D.; Kim, D.K.; Lee, H.N.; Kim, J.H.; Jue, J.H.; et al. Delta Neutrophil Index Does Not Differentiate Bacterial Infection without Bacteremia from Viral Infection in Pediatric Febrile Patients. Children 2023, 10, 161. https://doi.org/10.3390/children10010161
Kim M, Lee JH, Kwak YH, Kim HK, Kwon H, Suh D, Kim DK, Lee HN, Kim JH, Jue JH, et al. Delta Neutrophil Index Does Not Differentiate Bacterial Infection without Bacteremia from Viral Infection in Pediatric Febrile Patients. Children. 2023; 10(1):161. https://doi.org/10.3390/children10010161
Chicago/Turabian StyleKim, Maro, Jin Hee Lee, Young Ho Kwak, Hyun Kyung Kim, Hyuksool Kwon, Dongbum Suh, Do Kyun Kim, Ha Ni Lee, Jin Hee Kim, Jie Hee Jue, and et al. 2023. "Delta Neutrophil Index Does Not Differentiate Bacterial Infection without Bacteremia from Viral Infection in Pediatric Febrile Patients" Children 10, no. 1: 161. https://doi.org/10.3390/children10010161