
Gentle Touch and Sucrose for Pain Relief during Suctioning in Preterm Newborns—A Randomized Clinical Trial

 , ,
, ,
Abstract
:1. Introduction
2. Methods
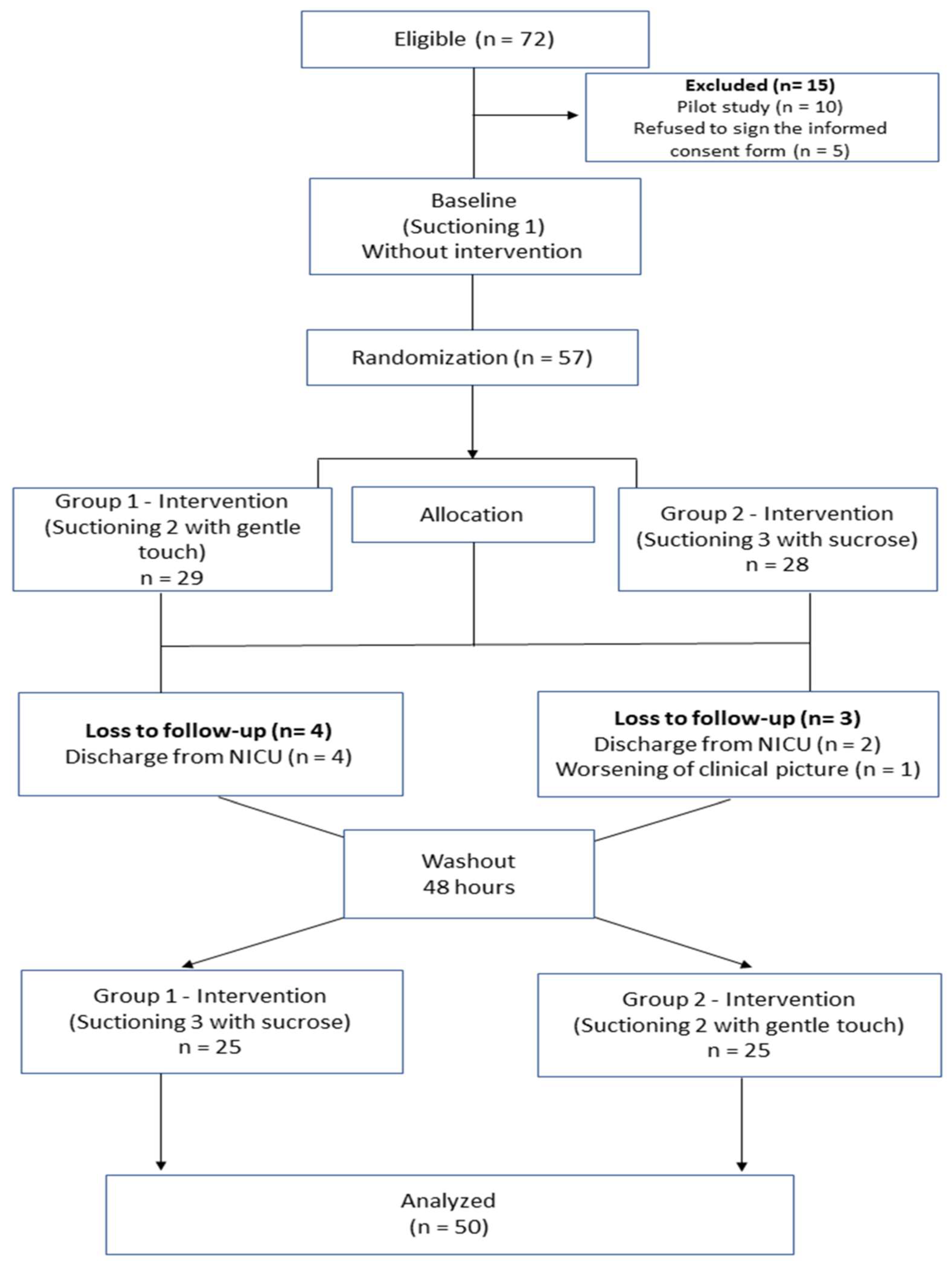
2.1. Randomization
2.2. Blinding
2.3. Variables
2.4. Interventions
2.5. Scales
2.6. Procedures
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Perry, M.; Tan, Z.; Chen, J.; Weidig, T.; Xu, W.; Cong, X.S. Neonatal Pain: Perceptions and Current Practice. Crit. Care Nurs Clin. N. Am. 2018, 30, 549–561. [Google Scholar] [CrossRef]
- Field, T. Preterm newborn pain research review. Infant Behav. Dev. 2017, 49, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Grupo de Trabajo de Doloren Neonatología, Comité de Estudios Feto—Neonatales (CEFEN). Manejo del dolor en Neonatología [Pain management in Neonatology]. Arch. Argent. Pediatr. 2019, 117, S180–S194. [Google Scholar] [CrossRef]
- Walker, S.M. Long term effects of Neonatal Pain. Semin. Fetal Neonatal Med. 2019, 24, 1–21. [Google Scholar] [CrossRef]
- Fitzgerald, M. What do we really know about newborn infant pain? Exp. Physiol. 2015, 100, 1451–1457. [Google Scholar] [CrossRef] [PubMed]
- Cordero, M.J.A.; García, L.B.; López, A.M.S.; Villar, N.M.; Castillo, R.F.; García, I.G. Procedimientos no farmacológicos para disminuir el dolor de los neonatos; Revisión sistemática. Nutr. Hosp. 2015, 32, 2496–2507. [Google Scholar] [CrossRef]
- Herrington, C.J.; Chiodo, L.M. Human touch effectively and safely reduces pain in the newborn intensive care unit. Pain ManagNurs. 2014, 15, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Stevens, B.; Yamada, J.; Ohlsson, A.; Haliburton, S.; Shorkey, A. Sucrose for analgesia in newborn infants undergoing painful procedures. Cochrane Database Syst. Rev. 2016, 7, CD001069. [Google Scholar] [CrossRef]
- Harrison, D.; Larocque, C.; Bueno, M.; Stokes, Y.; Turner, L.; Hutton, B.; Stevens, B. Sweet solutions to reduce procedural pain in neonates: A meta-analysis. Pediatrics 2017, 139, e20160955. [Google Scholar] [CrossRef] [Green Version]
- Manzotti, A.; Cerritelli, F.; Chiera, M.; Lombardi, E.; La Rocca, S.; Biasi, P.; Galli, M.; Esteves, J.; Lista, G. Neonatal Assessment Manual Score: Is There a Role of a Novel, Structured Touch-Based Evaluation in Neonatal Intensive Care Unit? Front. Pediatr. 2020, 8, 1–10. [Google Scholar] [CrossRef]
- Manzotti, A.; Cerritelli, F.; Esteves, J.E.; Lista, G.; Lombardi, E.; La Rocca, S.; Gallace, A.; McGlone, F.P.; Walker, S.C. Dynamic touch reduces physiological arousal in preterm infants: A role for c-tactile afferents? Dev. Cogn. Neurosci. 2019, 39, 1–7. [Google Scholar] [CrossRef]
- Fatollahzade, M.; Parvizi, S.; Kashaki, M.; Haghani, H.; Alinejad-Naeini, M. The effect of gentle human touch during endotracheal suctioning on procedural pain response in preterm infant admitted to neonatal intensive care units: A randomized controlled crossover study. J. Matern. Neonatal. Med. 2020, 35, 1370–1376. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Jiang Y fei Li, F.; Tong Q hong Rong, H.; Cheng, R. Effect of combined music and touch intervention on pain response and β- endorphin and cortisol concentrations in late preterm infants. BMC Pediatr. 2017, 17, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moultrie, F.; Slater, R.; Hartley, C. Improving the treatment of infant pain. CurrOpin. Support Palliat. Care 2017, 11, 112–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavoie, P.M.; Stritzke, A.; Ting, J.; Jabr, M.; Jain, A.; Kwan, E.; Chakkarapani, E.; Brooks, P.; Brant, R.; McNamara, P.J.; et al. A randomized controlled trial of the use of oral glucose with or without gentle facilitated tucking of infants during neonatal echocardiography. PLoS ONE 2015, 10, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beatriz, M.; Linhares, M. Dor em neonatos e crianças: Avaliação e intervenções não farmacológicas. Temas Psicol. 2010, 18, 307–325. [Google Scholar]
- Ribeiro, L.M. O Leite Humano e Sacarose 25% no Alívio da dor em Prematuros Submetidos ao Exame de Fundo de Olho: Ensaio Clínico Randomizado. Ph.D. Thesis, Escola de Enfermagem de Ribeirão Preto, Ribeirão Preto, Brazil, 2012. [Google Scholar]
- Da Motta, G.D.C.P. Adaptação Transcultural e Validação Clínica da Neonatal Infant Pain Scale para o Uso no Brasil. Master’s Thesis, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil, 2013. [Google Scholar]
- Da Batalha, L.M.C. Avaliação da Dor: Manual de estudo—Versão 1. Trat Dor Clínica 2016, 1, 81–92. [Google Scholar]
- Guinsburg, R. Avaliação e tratamento da dor no recém-nascido Assessing and treating pain in the newborn. J. Pediatr. 1999, 75, 149–160. [Google Scholar] [CrossRef] [Green Version]
- Bueno, M.; Costa, P.; de Oliveira, A.A.S.; Cardoso, R.; Kimura, A.F. Tradução e adaptação do premature infant pain profile para a língua Portuguesa. Texto Context Enferm. 2013, 22, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Bueno, M.; Moreno-Ramos, M.C.; Forni, E.; Kimura, A.F. Adaptation and Initial Validation of the Premature Infant Pain Profile–Revised (PIPP-R) in Brazil. Pain Manag Nurs. 2019, 20, 512–515. [Google Scholar] [CrossRef]
- Formiga, C.K.M.R. Desenvolvimento de bebês nascidos pré-termo no primeiro ano de vida. Paid 2009, 13, 59–72. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Küçük Alemdar, D.; Güdücü Tüfekcİ, F. Effects of maternal heart sounds on pain and comfort during aspiration in preterm infants. Jpn. J. Nurs. Sci. 2018, 15, 330–339. [Google Scholar] [CrossRef]
- Lopez, O.; Subramanian, P.; Rahmat, N.; Theam, L.C.; Chinna, K.; Rosli, R. The effect of facilitated tucking on procedural pain control among premature babies. J. Clin. Nurs. 2015, 24, 183–191. [Google Scholar] [CrossRef]
- Pillai Riddell, R.R.; Racine, N.M.; Gennis, H.G.; Turcotte, K.; Uman, L.S.; Horton, R.T.; Kohut, S.A.; Stuart, J.H.; Stevens, B.; Lisi, D.M. Non-pharmacological management of infant and young child procedural pain. Cochrane Database Syst Rev. 2015, 2015, CD006275. [Google Scholar] [CrossRef]
- Perroteau, A.; Nanquette, M.C.; Rousseau, A.; Renolleau, S.; Bérard, L.; Mitanchez, D.; Leblanc, J. Efficacy of facilitated tucking combined with non- nutritive sucking on very preterm infants’ pain during the heel-stick procedure: A randomized controlled trial. Int. J. Nurs. Stud. 2018, 86, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Stevens, B.; Yamada, J.; Campbell-Yeo, M.; Gibbins, S.; Harrison, D.; Dionne, K.; Taddio, A.; McNair, C.; Willan, A.; Ballantyne, M.; et al. The Minimally Effective Dose of Sucrose for Procedural Pain Relief in Neonates: A Randomized Controlled Trial. MCN Am. J. Matern. Nurs. 2018, 43, 297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, H.; Li, M.; Gao, H.; Xu, G.; Li, F.; Zhou, J.; Zou, Y.; Jiang, H. Effect of non-nutritive sucking and sucrose alone and in combination for repeated procedural pain in preterm infants: A randomized controlled trial. Int. J. Nurs. Stud. 2018, 83, 25–33. [Google Scholar] [CrossRef]
- Sen, E.; Manav, G. Effect of Kangaroo Care and Oral Sucrose on Pain in Premature Infants: A Randomized Controlled Trial. Pain Manag. Nurs. 2020, 21, P556–P564. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics of Preterm Newborns | Values |
|---|---|
| Type of Birth f (%) | |
| Vaginal | 29 (58) |
| Cesarean | 21 (42) |
| Sex f (%) | |
| Female | 26 (52) |
| Male | 24 (48) |
| Birth weight (g)—Med (min–max) | 1050 (886.3–1227.3) |
| Gestational age (weeks)—Med (min–max) | 28 (26.7–30.3) |
| Clinical risk—Med (min–max) | |
| Apgar in the first minute (score) | 6 (4–8) |
| Apgar in the fifth minute (score) | 8 (7–9) |
| Cried at birth f (%) | 36 (72) |
| Birth complications f (%) | 12 (24) |
| Fetal distress f (%) | 9 (18) |
| Neonatal health complications f (%) | |
| Infection f (%) | 25 (50) |
| Apnea f (%) | 8 (16) |
| Hyaline membrane disease f (%) | 50 (100) |
| Bronchopulmonary dysplasia f (%) | 1 (2) |
| Surfactant use f (%) | 39 (78) |
| Antibiotic use f (%) | 39 (78) |
| Phototherapy f (%) | 25 (50) |
| Transfusion f (%) | 10 (20) |
| Mechanical ventilation f (%) | 41 (82) |
| Nasal CPAP f (%) | 37 (74) |
| Oxygen support (%) | 21 (42) |
| Hood f (%) | 1 (2) |
| Transfontanellar ultrasound f (%) | |
| Altered | 27 (54) |
| Normal | 18 (36) |
| No information | 5 (10) |
| Indicator | Median (25–75% Interquartile Range) | Post Hoc | |||||
|---|---|---|---|---|---|---|---|
| Baseline Suctioning | Suctioning with Gentle Touch | Suctioning with Sucrose | p-Value * | Baseline x Gentle Touch | Baseline x Sucrose | Gentle Touch x Sucrose | |
| NIPS | |||||||
| Facial expression | 1.0 (0.5–1.0) | 1.0 (0.5–1.0) | 1.0 (0.5–1.0) | 0.220 | |||
| Cry | 0.5 (0.0–1.5) | 0.5 (0.0–1.5) | 0.0 (0.0–1.0) | <0.001 * | 0.137 | 0.010 * | 1 |
| Breathing pattern | 0.5 (0.5–1.0) | 0.5 (0.0–1.0) | 0.5 (0.0–1.0) | <0.001 * | 0.581 | 0.007 * | 0.24 |
| Motor activity of arms | 0.5 (0.0–1.0) | 0.5 (0.5–1.0) | 0.5 (0.0–0.8) | 0.005 * | 1 | 0.83 | 0.26 |
| Motor activity of legs | 0.5 (0.0–1.0) | 0.5 (0.0–1.0) | 0.5 (0.0–0.5) | 0.002 * | 0.154 | 0.032 * | 1 |
| State of arousal | 0.5 (0.0–1.0) | 0.5 (0.0–1.0) | 0.0 (0.0–0.5) | <0.001 * | 0.363 | 0.002 * | 0.19 |
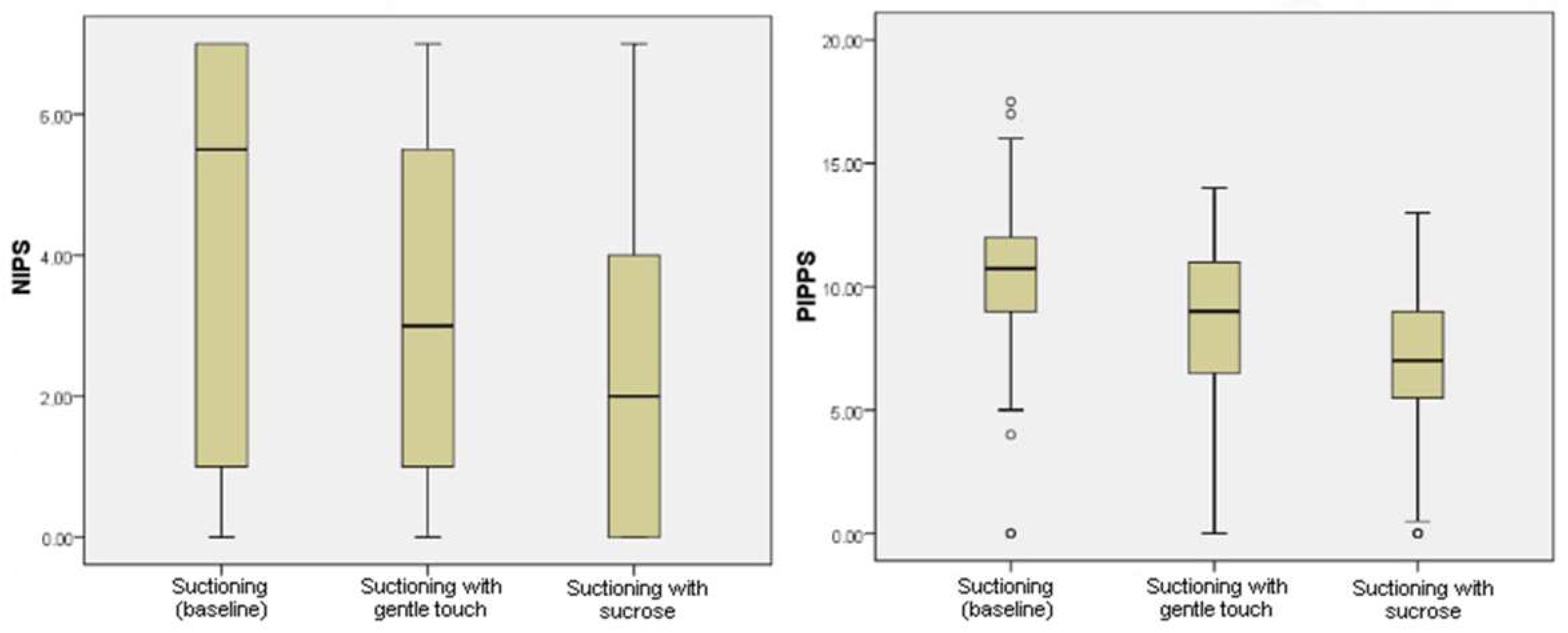
| Total | 5.0 (1.0–6.0) | 3.0 (1.5–5.5) | 2.5 (1.0–4.5) | <0.001 * | 0.010 * | <0.001 * | 0.24 |
| PIPP-R | |||||||
| Heart rate change | 1.0 (0.3–1.8) | 1.0 (1.0–2.5) | 1.0 (0.0–2.0) | 0.327 | |||
| Drop in oxygen saturation | 1.0 (0.0–2.0) | 1.0 (0.0–3.0) | 0.5 (0.0–1.5) | 0.157 | |||
| Brow bulge | 1.0 (0.5–2.0) | 1.0 (0.5–1.8) | 1.0 (0.3–1.5) | <0.001 * | 0.002 * | <0.001 * | 0.48 |
| Eye squeeze | 1.0 (0.5–2.0) | 1.0 (0.5–1.8) | 1.0 (0.5–1.5) | <0.001 * | 0.024 * | <0.001 * | 0.32 |
| Nasolabial furrow | 1.0 (0.3–2.0) | 0.5 (0.0–1.5) | 0.5 (0.0–1.0) | <0.001 * | 0.024 * | 0.001 * | 0.95 |
| Gestational age | 2.0 (2.0–3.0) | 2.0 (2.0–3.0) | 2.5 (2.0–3.0) | 0.459 | |||
| Behavioral state | 1.5 (1.0–2.5) | 1.5 (1.0–2.0) | 1.5 (1.0–2.5) | 0.704 | |||
| Total | 10.0 (7.5–12.0) | 10.0 (8.5–12.0) | 8.5 (7.0–10.5) | <0.001 * | 0.121 | <0.001 * | 0.56 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveira, N.R.G.d.; Formiga, C.K.M.R.; Ramos, B.A.; Santos, R.N.d.; Moreira, N.N.d.S.; Marçal, P.G.E.; Amaral, W.N.d. Gentle Touch and Sucrose for Pain Relief during Suctioning in Preterm Newborns—A Randomized Clinical Trial. Children 2023, 10, 158. https://doi.org/10.3390/children10010158
Oliveira NRGd, Formiga CKMR, Ramos BA, Santos RNd, Moreira NNdS, Marçal PGE, Amaral WNd. Gentle Touch and Sucrose for Pain Relief during Suctioning in Preterm Newborns—A Randomized Clinical Trial. Children. 2023; 10(1):158. https://doi.org/10.3390/children10010158
Chicago/Turabian StyleOliveira, Nayara Rodrigues Gomes de, Cibelle Kayenne Martins Roberto Formiga, Bruna Abreu Ramos, Rafaela Noleto dos Santos, Nayara Nubia de Sousa Moreira, Patricia Gonçalves Evangelista Marçal, and Waldemar Naves do Amaral. 2023. "Gentle Touch and Sucrose for Pain Relief during Suctioning in Preterm Newborns—A Randomized Clinical Trial" Children 10, no. 1: 158. https://doi.org/10.3390/children10010158