
Drug Prescriptions Requiring Compounding at a Canadian University Affiliated Pediatric Hospital: A Cross-Sectional Study
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
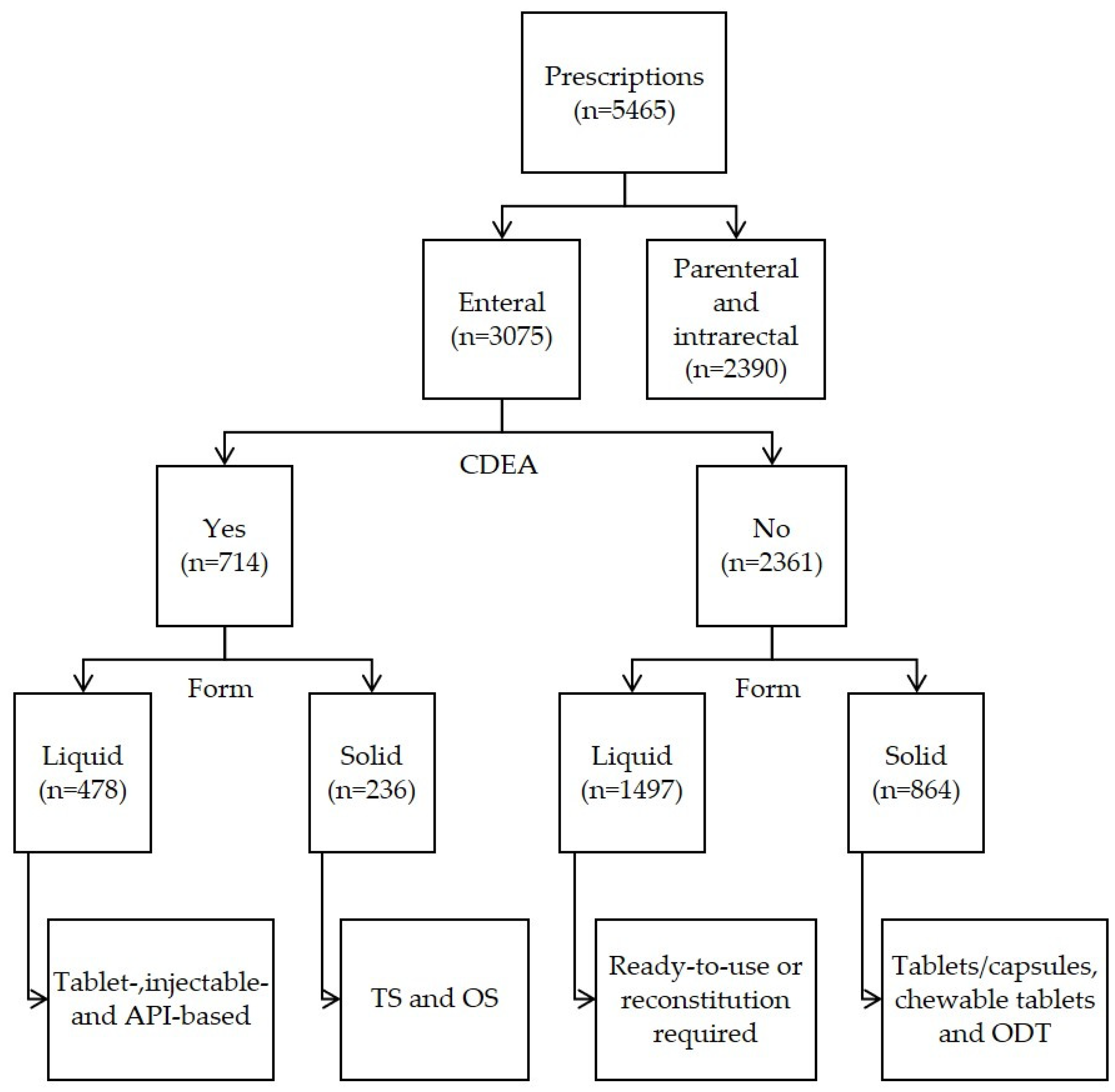
2.3. Prescriptions of Interest
2.4. Data Extraction
2.5. Quality Control
2.6. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Richey, R.; Shah, U.; Peak, M.; Craig, J.; Ford, J.; Barker, C.; Nunn, A.; Turner, M. Manipulation of drugs to achieve the required dose is intrinsic to paediatric practice but is not supported by guidelines or evidence. BMC Pediatr. 2013, 13, 81. [Google Scholar] [CrossRef] [Green Version]
- Minghetti, P.; Pantano, D.; Gennari, C.; Casiraghi, A. Regulatory framework of pharmaceutical compounding and actual developments of legislation in Europe. Health Policy 2014, 117, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Watson, C.; Whitledge, J.; Siani, A.; Burns, M. Pharmaceutical Compounding: A History, Regulatory Overview, and Systematic Review of Compounding Errors. J. Med. Toxicol. 2021, 17, 197–217. [Google Scholar] [CrossRef] [PubMed]
- Ernest, T.; Craig, J.; Nunn, A.; Salunke, S.; Tuleu, C.; Breitkreutz, J.; Alex, R.; Hempenstall, J. Preparation of medicines for children—A hierarchy of classification. Int. J. Pharm. 2012, 435, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Bhatt-Mehta, V.; MacArthur, R.; Lobenberg, R.; Cies, J.; Cernak, I.; Ibolja, C.; Parrish II, R. An Algorithm to Identify Compounded Non-Sterile Products that Can Be Formulated on a Commercial Scale or Imported to Promote Safer Medication Use in Children. Pharmacy 2015, 3, 284–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawlence, E.; Lowey, A.; Tomlin, S.; Auyeung, V. Is the provision of paediatric oral liquid unlicensed medicines safe? Arch. Dis. Child. Educ. Pract. Ed. 2018, 103, 310–313. [Google Scholar] [CrossRef] [PubMed]
- Rood, J.; Engels, M.; Ciarkowski, S.; Wagenknecht, L.; Dickinson, C.; Stevenson, J. Variability in compounding of oral liquids for pediatric patients: A patient safety concern. J. Am. Pharm. Assoc. 2014, 54, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Institute for Safe Medication Practices Canada. Pediatric Medication Errors in the Community: A Multi-Incident Analysis. ISMP Can. Saf. Bull. 2022, 22, 7. [Google Scholar]
- Litalien, C.; Autmizguine, J.; Carli, A.; Giroux, D.; Lebel, D.; Leclerc, J.-M.; Théorêt, Y.; Gilpin, A.; Bérubé, S. Providing Suitable Pediatric Formulations for Canadian Children: A Call for Action. Can. J. Hosp. Pharm. 2020, 73, 10. [Google Scholar] [CrossRef]
- Raja, P.; Duffett, M.; Mazer-Amirshahi, M.; Patel, A.; Gilpin, A.; Litalien, C.; Chan, A.; van den Anker, J.; Lacaze-Masmonteil, T.; Samiee-Zafarghandy, S. Pediatric drug data in Canadian drug monographs: A descriptive analysis. CMAJ Open 2020, 8, E522–E529. [Google Scholar] [CrossRef] [PubMed]
- International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. ICH Harmonised Guideline: Addendum to ICH E11: Clinical Investigation of Medicinal Products in the Pediatric Population. Available online: https://database.ich.org/sites/default/files/E11_R1_Addendum.pdf (accessed on 1 May 2020).
- Jones, D.; McRea, A.; Jairath, M.; Jones, M.; Bradfort, K.; Jhaveri, R. Prospective Assessment of Pill-Swallowing Ability in Pediatric Patients. Clin. Pediatr. 2018, 57, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Polaha, J.; Dalton III, W.; Lancaster, B. Parental Report of Medication Acceptance Among Youth- Implications for Everyday Practice. South. Med. Assoc. 2008, 101, 1106–1112. [Google Scholar] [CrossRef] [PubMed]
- Brion, F.; Nunn, A.; Rieutord, A. Extemporaneous (magistral) preparation of oral medicines for children in European hospitals. Acta Paediatr. 2003, 92, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Giam, J.; McLachlan, A. Extemporaneous product use in paediatric patients: A systematic review. Int. J. Pharm. Pract. 2008, 16, 3–10. [Google Scholar] [CrossRef]
- McPherson, T.; Fontane, P.; Iyengar, R.; Henderson, R. Utilization and Costs of Compounded Medications for Comercially Insured Patients, 2012–2013. J. Manag. Care Spec. Pharm. 2016, 22, 172–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magalhaes, J.; Rodrigues, A.; Roque, F.; Figueiras, A.; Falcao, A.; Herdeiro, M. Use of off-label and unlicenced drugs in hospitalised paediatric patients: A systematic review. Eur. J. Clin. Pharmacol. 2015, 71, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Saito, J.; Akabane, M.; Ishikawa, Y.; Iwahashi, K.; Nakamura, H.; Yamatani, A. Retrospective survey of compounded medications for children in Japan. Eur. J. Pharm. Biopharm. 2020, 155, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Gilpin, A.; Berube, S.; Moore-Hepburn, C.; Lacaze-Masmonteil, T.; Samiee-Zafarghandy, S.; Rieder, M.; Gruenwoldt, E.; MacLeod, S.; Litalien, C. Time for a regulatory framework for pediatric medications in Canada. CMAJ 2022, 194, E678–E680. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Prescription Type | Description | CDEA |
|---|---|---|
| Tablet-or capsule based liquid | Tablet typically crushed into a fine powder or content of capsule dispersed before diluting or mixing into syrup or other liquid | Yes |
| Injectable-based liquid | Injectable drug diluted for oral administration or without dilution | Yes |
| API-based liquid | API directly diluted or mixed into syrup or other liquid | Yes |
| Tablet Splitting | Tablet scored and unscored tablets administered in fractions of dosage | Yes |
| Other solid | May include API encapsulated for appropriate pediatric dosing or a marketed capsule opened to weigh and split API (powder or granules) | Yes |
| Ready-to-use | Marketed as is | No |
| Reconstitution required | Water dilution of bottled API required as indicated by the manufacturer | No |
| Other liquid | Injectable liquid drug administered orally (no dilution required) | No |
| Tablets/capsules | Marketed as is | No |
| Chewable tablets | Chewing required before swallowing | No |
| ODT | No chewing or drinking liquids needed to swallow and ingest, as API disintegrates rapidly in saliva | No |
| Other solid | Marketed as gums, throat lozenges, or dispersible tablets | No |
| Age Group | ||||||
|---|---|---|---|---|---|---|
| Parameter | Total (N = 606) | <28 Days (N = 213) | 28 Days to <2 Years (N = 108) | 2 to <8 Years (N = 85) | 8 to <12 Years (N = 71) | 12 to <18 Years (N = 129) |
| Sex, N (%) | ||||||
| Male | 318 (52) | 119 (56) | 65 (60) | 47 (55) | 38 (54) | 49 (38) |
| Hospital unit, N (%) | ||||||
| Pediatrics | 124 (20) | 11 (5) | 40 (37) | 22 (26) | 15 (21) | 36 (28) |
| NICU 1 | 121 (20) | 119 (56) | 2 (2) | |||
| Multispecialty | 78 (13) | 8 (4) | 16 (15) | 11 (13) | 9 (13) | 34 (26) |
| Surgery | 74 (12) | 5 (2) | 18 (17) | 16 (19) | 12 (17) | 23 (18) |
| Nursery 2 | 56 (9) | 56 (26) | ||||
| Rehabilitation Centre | 56 (9) | 1 (0) | 4 (4) | 18 (21) | 18 (25) | 15 (12) |
| Hematology-Oncology | 50 (8) | 10 (9) | 12 (14) | 11 (15) | 17 (13) | |
| Pediatric ICU | 47 (8) | 13 (6) | 18 (17) | 6 (7) | 6 (8) | 4 (3) |
| ICD-11 class of diagnosis, N (%) | ||||||
| Infectious Diseases | 97 (16) | 12 (6) | 41 (38) | 28 (33) | 10 (14) | 6 (5) |
| Preterm Birth | 92 (15) | 91 (43) | 1 (1) | |||
| Term Birth | 62 (10) | 62 (29) | ||||
| Hematology-Oncology | 62 (10) | 10 (9) | 14 (16) | 18 (25) | 20 (16) | |
| Neurology | 55 (9) | 4 (2) | 3 (3) | 17 (20) | 18 (25) | 13 (10) |
| Digestive System | 52 (9) | 10 (5) | 15 (14) | 7 (8) | 6 (8) | 14 (11) |
| Psychiatry | 44 (7) | 1 (1) | 1 (1) | 42 (33) | ||
| Cardiovascular System | 30 (5) | 13 (6) | 10 (9) | 5 (6) | 2 (2) | |
| Trauma | 30 (5) | 5 (5) | 6 (7) | 8 (11) | 11 (9) | |
| Others 3 | 82 (13) | 21 (10) | 23 (21) | 7 (8) | 10 (14) | 21 (16) |
| Age Group | ||||||
|---|---|---|---|---|---|---|
| Prescription Type | Total (N = 5465) | <28 Days (N = 1225) | 28 Days to <2 Years (N = 893) | 2 to <8 Years (N = 1000) | 8 to <12 Years (N = 1054) | 12 to <18 Years (N = 1293) |
| Enteral administration, N(%) 1 | 3075 (56) | 712 (58) | 454 (51) | 550 (55) | 584 (55) | 775 (60) |
| Commercial form | 2361 (43) | 530 (43) | 327 (37) | 409 (41) | 428 (41) | 667 (52) |
| CDEA | 714 (13) | 182 (15) | 127 (14) | 141 (14) | 156 (15) | 108 (8) |
| 🢖Liquid | 478 (9) | 168 (14) | 96 (11) | 106 (11) | 85 (8) | 23 (2) |
| 🢒Tablet/capsule-based | 299 (5) | 74 (6) | 68 (8) | 91 (9) | 53 (5) | 13 (1) |
| 🢒Injectable-based | 92 (2) | 38 (3) | 13 (1) | 9 (1) | 25 (2) | 7 (1) |
| 🢒API-based | 87 (2) | 56 (5) | 15 (2) | 6 (1) | 7 (1) | 3 (0) |
| 🢖Solid | 236 (4) | 14 (1) | 31 (3) | 35 (3) | 71 (7) | 85 (7) |
| 🢒Tablet splitting | 231 (4) | 13 (1) | 28 (3) | 35 (3) | 70 (7) | 85 (7) |
| 🢒Others 2 | 5 (0) | 1 (0) | 3 (0) | 1 (0) | ||
| Parenteral administration. N(%) 1 | 2390 (44) | 513 (42) | 439 (49) | 450 (45) | 470 (45) | 518 (40) |
| Age Group | ||||||
|---|---|---|---|---|---|---|
| Parameter | Total (N = 298) | <28 Days (N = 75) | 28 Days to <2 Years (N = 55) | 2 to <8 Years (N = 51) | 8 to <12 Years (N = 51) | 12 to <18 Years (N = 66) |
| Sex, N (%) | ||||||
| Male | 160 (54) | 41 (55) | 35 (64) | 29 (57) | 27 (53) | 28 (42) |
| Hospital Unit, N (%) | ||||||
| Pediatric ICU | 37 (12) | 10 (13) | 13 (24) | 5 (9) | 6 (12) | 3 (5) |
| NICU | 58 (19) | 58 (77) | ||||
| Hematology–Oncology | 43 (14) | 8 (15) | 11 (22) | 10 (20) | 14 (21) | |
| Pediatrics | 40 (13) | 1 (1) | 13 (24) | 8 (16) | 6 (12) | 12 (18) |
| Surgery | 25 (8) | 6 (11) | 3 (6) | 7 (14) | 9 (14) | |
| Multispecialty | 50 (17) | 5 (7) | 11 (20) | 8 (16) | 7 (14) | 19 (29) |
| Rehabilitation Centre | 45 (15) | 1 (1) | 4 (7) | 16 (31) | 15 (29) | 9 (14) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Landry, É.K.; Autmizguine, J.; Bérubé, S.; Kraus, R.; Métras, M.-É.; Lebel, D.; Litalien, C. Drug Prescriptions Requiring Compounding at a Canadian University Affiliated Pediatric Hospital: A Cross-Sectional Study. Children 2023, 10, 147. https://doi.org/10.3390/children10010147
Landry ÉK, Autmizguine J, Bérubé S, Kraus R, Métras M-É, Lebel D, Litalien C. Drug Prescriptions Requiring Compounding at a Canadian University Affiliated Pediatric Hospital: A Cross-Sectional Study. Children. 2023; 10(1):147. https://doi.org/10.3390/children10010147
Chicago/Turabian StyleLandry, Émilie Kate, Julie Autmizguine, Sophie Bérubé, Raphael Kraus, Marie-Élaine Métras, Denis Lebel, and Catherine Litalien. 2023. "Drug Prescriptions Requiring Compounding at a Canadian University Affiliated Pediatric Hospital: A Cross-Sectional Study" Children 10, no. 1: 147. https://doi.org/10.3390/children10010147