
Expression of miR-1-3p, miR-16-5p and miR-122-5p as Possible Risk Factors of Secondary Cardiovascular Events

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
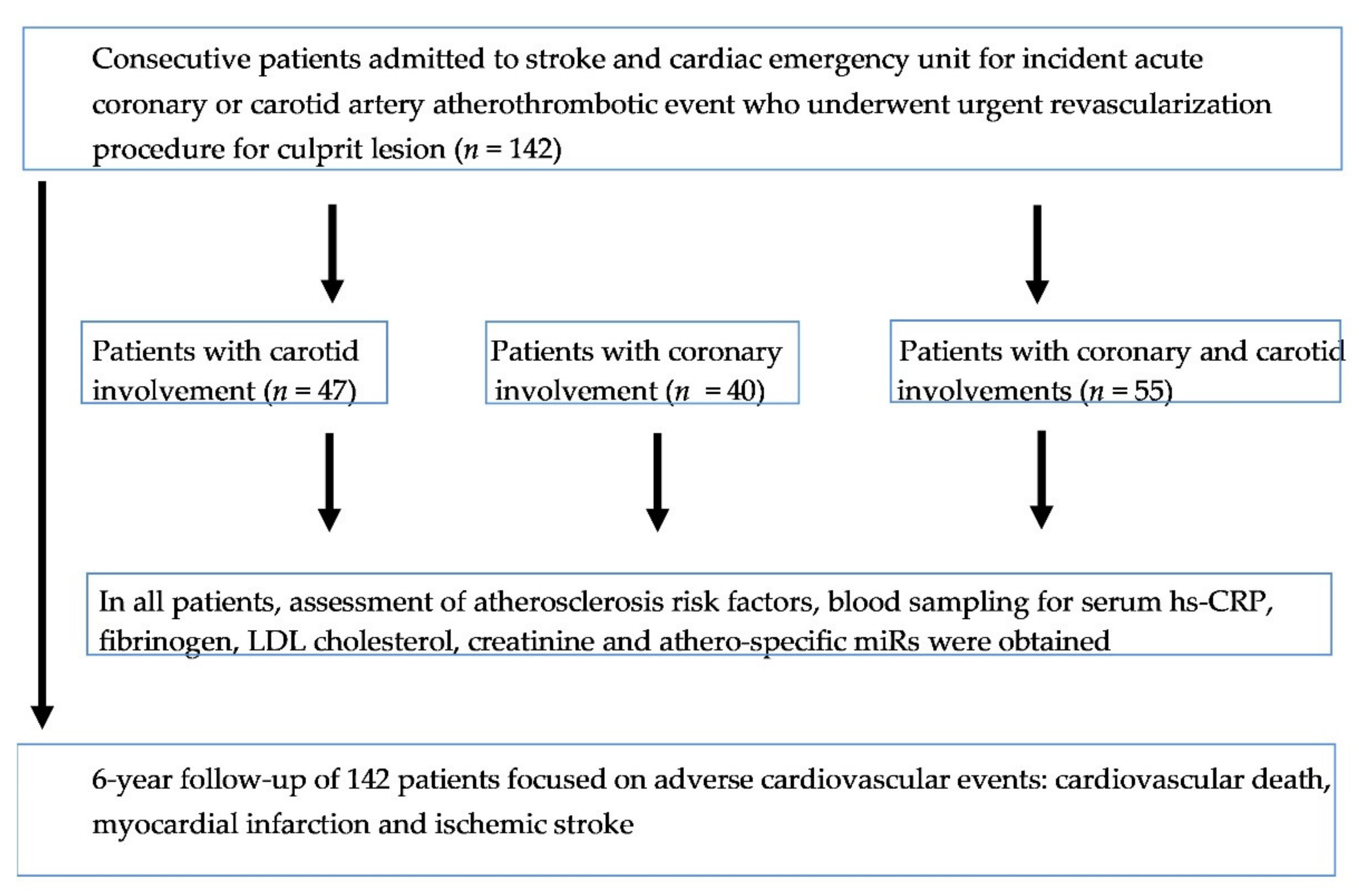
2.1. Study Population
2.2. Biochemical Tests and miRs Extraction
2.3. Profiling of miRs
2.4. Outcome Data, Follow-Up and Adverse Cardiovascular Events
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Clinical, Biochemical and miRs Parameters and the Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herrington, W.; Lacey, B.; Sherliker, P.; Armitage, J.; Lewington, S. Epidemiology of Atherosclerosis and the Potential to Reduce the Global Burden of Atherothrombotic Disease. Circ. Res. 2016, 118, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Gerber, Y.; Weston, S.A.; Jiang, R.; Roger, V.L. The changing epidemiology of myocardial infarction in Olmsted County, Minnesota, 1995–2012. Am. J. Med. 2015, 128, 144–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohan, K.M.; Wolfe, C.D.; Rudd, A.G.; Heuschmann, P.U.; Kolominsky-Rabas, P.L.; Grieve, A.P. Risk and cumulative risk of stroke recurrence: A systematic review and meta-analysis. Stroke 2011, 42, 1489–1494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diener, H.C.; Hankey, G.J. Primary and Secondary Prevention of Ischemic Stroke and Cerebral Hemorrhage: JACC Focus Seminar. J. Am. Coll. Cardiol. 2020, 75, 1804–1818. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Leifheit, E.; Normand, S.-L.T.; Krumholz, H.M. Association Between Subsequent Hospitalizations and Recurrent Acute Myocardial Infarction Within 1 Year After Acute Myocardial Infarction. J. Am. Heart Assoc. 2020, 9, e014907. [Google Scholar] [CrossRef] [PubMed]
- Bogacki, P.; Kabłak-Ziembicka, A.; Bryniarski, K.; Wrotniak, L.; Ostrowska-Kaim, E.; Żmudka, K.; Przewłocki, T. Triple anticoagulation therapy in patients with atrial fibrillation undergoing percutaneous coronary intervention—Real life assessment. Adv. Interv. Cardiol. 2016, 12, 303–313. [Google Scholar] [CrossRef] [Green Version]
- Voudris, K.V.; Feldman, D.N. Complete Revascularization in Patients With STEMI and Multivessel Coronary Artery Disease: Is It Beneficial? Curr. Treat. Options Cardio Med. 2021, 23, 15. [Google Scholar] [CrossRef]
- Ji, R.; Cheng, Y.; Yue, J.; Yang, J.; Liu, X.; Chen, H.; Dean, D.B.; Zhang, C. MicroRNA expression signature and antisensemediated depletion reveal an essential role of microRNA in vascular neointimal lesion formation. Circ. Res. 2007, 100, 1579–1588. [Google Scholar] [CrossRef] [PubMed]
- Jickling, G.C.; Ander, B.P.; Zhan, X.; Noblett, D.; Stamova, B.; Liu, D. microRNA expression in peripheral blood cells following acute ischemic stroke and their predicted gene targets. PLoS ONE 2014, 9, e99283. [Google Scholar] [CrossRef]
- Kabłak-Ziembicka, A.; Przewłocki, T.; Stępień, E.; Pieniążek, P.; Rzeźnik, D.; Sliwiak, D.; Komar, M.; Tracz, W.; Podolec, P. Carotid intima-media thickness, cytokines: Atherosclerosis extend and two-year cardiovascular risk in patients with arteriosclerosis. Kardiol. Pol. 2011, 69, 1024–1031. [Google Scholar]
- Luengo-Fernandez, R.; Paul, N.L.; Gray, A.M.; Pendlebury, S.T.; Bull, L.M.; Welch, S.J.; Cuthbertson, F.C.; Rothwell, P.M. A population-based study of disability and institutionalisation after TIA and stroke: 10-year results of the Oxford Vascular Study. Stroke 2013, 44, 2854–2861. [Google Scholar] [CrossRef] [Green Version]
- Ghafouri-Fard, S.; Abak, A.; Shoorei, H.; Mohaqiq, M.; Majidpoor, J.; Sayad, A.; Taheri, M. Regulatory role of microRNAs on PTEN signaling. Biomed. Pharm. 2021, 133, 110986. [Google Scholar] [CrossRef] [PubMed]
- Sardu, C.; Modugno, P.; Castellano, G.; Scisciola, L.; Barbieri, M.; Petrella, L.; Fanelli, M.; Macchia, G.; Caradonna, E.; Massetti, M.; et al. Atherosclerotic Plaque Fissuration and Clinical Outcomes in Pre-Diabetics vs. Normoglycemics Patients Affected by Asymptomatic Significant Carotid Artery Stenosis at 2 Years of Follow-Up: Role of MIcRoRNAs Modulation: The ATIMIR Study. Biomedicines 2021, 9, 401. [Google Scholar] [CrossRef] [PubMed]
- Santovito, D.; Mezzetti, A.; Cipollone, F. MicroRNAs and atherosclerosis: New actors for an old movie. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 937–943. [Google Scholar] [CrossRef] [PubMed]
- Urbich, C.; Kuehbacher, A.; Dimmeler, S. Role of microRNAs in vascular diseases, inflammation, and angiogenesis. Cardiovasc. Res. 2008, 79, 581–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [PubMed] [Green Version]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T. ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef] [Green Version]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Gacoń, J.; Kabłak-Ziembicka, A.; Stępień, E.; Enguita, F.J.; Karch, I.; Derlaga, B.; Żmudka, K.; Przewłocki, T. Decision-making microRNAs (miR-124, -133a/b, -34a and -134) in patients with occluded target vessel in acute coronary syndrome. Kardiol. Pol. 2016, 74, 280–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elfaki, I.; Mir, R.; Mir, M.M.; AbuDuhier, F.M.; Babakr, A.T.; Barnawi, J. Potential Impact of MicroRNA Gene Polymorphisms in the Pathogenesis of Diabetes and Atherosclerotic Cardiovascular Disease. J. Pers. Med. 2019, 9, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cipollone, F.; Felicioni, L.; Sarzani, R.; Ucchino, S.; Spigonardo, F.; Mandolini, C.; Malatesta, S.; Bucci, M.; Mammarella, C.; Santovito, D.; et al. A unique microRNA signature associated with plaque instability in humans. Stroke 2011, 42, 2556–2563. [Google Scholar] [CrossRef] [Green Version]
- Badacz, R.; Przewłocki, T.; Gacoń, J.; Stępień, E.; Enguita, F.J.; Karch, I.; Żmudka, K.; Kabłak-Ziembicka, A. Circulating miRNA levels differ with respect to carotid plaque characteristics and symptom occurrence in patients with carotid artery stenosis and provide information on future cardiovascular events. Postepy Kardiol Interwencyjnej 2018, 14, 75–84. [Google Scholar] [CrossRef]
- Riera, A.R.P.; Uchida, A.H.; Schapachnik, E.; Dubner, S.; Filho, C.F.; Ferreira, C. Propofol infusion syndrome and Brugada syndrome electrocardiographic phenocopy. Cardiol. J. 2010, 17, 130–135. [Google Scholar]
- Giorgino, F.; D’Oria, R.; Schipani, R.; Leonardini, A.; Natalicchio, A.; Perrini, S.; Cignarelli, A.; Laviola, L. The Role of Oxidative Stress in Cardiac Disease: From Physiological Response to Injury Factor. Oxid. Med. Cell. Longev. 2020, 2020, 5732956. [Google Scholar] [CrossRef]
- Duisters, R.F.; Tijsen, A.J.; Schroen, B.; Leenders, J.J.; Lentink, V.; van der Made, I.; Herias, V.; van Leeuwen, R.E.; Schellings, M.W.; Barenbrug, P.; et al. miR-133 and miR-30 regulate connective tissue growth factor: Implications for a role of microRNAs in myocardial matrix remodeling. Circ. Res. 2009, 104, 170–178. [Google Scholar]
- Liu, J.; Sun, F.; Wang, Y.; Yang, W.; Xiao, H.; Zhang, Y.; Lu, H.; Zhu, H.; Zhuang, Y.; Pan, Z.; et al. Suppression of microRNA-16 protects against acute myocardial infarction by reversing beta2-adrenergic receptor down-regulation in rats. Oncotarget 2017, 8, 20122–20132. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Li, J.; Cai, J.; Cheng, L.; Wang, X.; Xu, P.; Li, G.; Liang, X. Overexpression of MicroRNA-16 Alleviates Atherosclerosis by Inhibition of Inflammatory Pathways. Biomed Res. Int. 2020, 2020, 8504238. [Google Scholar] [CrossRef] [PubMed]
- Tian, C.; Li, Z.; Yang, Z.; Huang, Q.; Liu, J.; Hong, B. Plasma MicroRNA-16 Is a Biomarker for Diagnosis, Stratification, and Prognosis of Hyperacute Cerebral Infarction. PLoS ONE 2016, 11, e0166688. [Google Scholar] [CrossRef]
- D’Onofrio, N.; Sardu, C.; Paolisso, P.; Minicucci, F.; Gragnano, F.; Ferraraccio, F.; Panarese, I.; Scisciola, L.; Mauro, C.; Rizzo, M.R.; et al. MicroRNA-33 and SIRT1 influence the coronary thrombus burden in hyperglycemic STEMI patients. J. Cell. Physiol. 2020, 235, 1438–1452. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Morelli, M.B.; Matarese, A.; Sardu, C.; Santulli, G. Cardiomyocyte-derived exosomal microRNA-92a mediates post-ischemic myofibroblast activation both in vitro and ex vivo. ESC Heart Fail. 2020, 7, 284–288. [Google Scholar] [CrossRef] [Green Version]
- Sheikh, M.S.A.; Alduraywish, A.; Almaeen, A.; Alruwali, M.; Alruwaili, R.; Alomair, B.M.; Salma, U.; Hedeab, G.M.; Bugti, N.; Abdulhabeeb, I.A.M. Therapeutic Value of miRNAs in Coronary Artery Disease. Oxid. Med. Cell. Longev. 2021, 2021, 8853748. [Google Scholar] [CrossRef]
- Navickas, R.; Gal, D.; Laucevičius, A.; Taparauskaitė, A.; Zdanytė, M.; Holvoet, P. Identifying circulating microRNAs as biomarkers of cardiovascular disease: A systematic review. Cardiovasc. Res. 2016, 111, 322–337. [Google Scholar] [CrossRef] [PubMed]
- Jankauskas, S.S.; Gambardella, J.; Sardu, C.; Lombardi, A.; Santulli, G. Functional Role of miR-155 in the Pathogenesis of Diabetes Mellitus and Its Complications. Non Coding RNA 2021, 7, 39. [Google Scholar] [CrossRef] [PubMed]
- Sardu, C.; Trotta, M.C.; Pieretti, G.; Gatta, G.; Ferraro, G.; Nicoletti, G.F.; D’Onofrio, N.; Balestrieri, M.L.; D’Amico, M.; Abbatecola, A.; et al. MicroRNAs modulation and clinical outcomes at 1 year of follow-up in obese patients with pre-diabetes treated with metformin vs. placebo. Acta Diabetol. 2021. [Google Scholar] [CrossRef]
- Murphy, S.A.; Pedersen, T.R.; Gaciong, Z.A.; Ceska, R.; Ezhov, M.V.; Connolly, D.L.; Jukema, J.W.; Toth, K.; Tikkanen, M.J.; Im, K.; et al. Effect of the PCSK9 Inhibitor Evolocumab on Total Cardiovascular Events in Patients with Cardiovascular Disease: A Prespecified Analysis from the FOURIER Trial. JAMA Cardiol. 2019, 4, 613–619. [Google Scholar] [CrossRef]
- Smolina, K.; Wright, F.L.; Rayner, M.; Goldacre, M.J. Long-term survival and recurrence after acute myocardial infarction in England, 2004 to 2010. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 532–540. [Google Scholar] [CrossRef] [Green Version]
- Feng, W.; Hendry, R.M.; Adams, R.J. Risk of recurrent stroke, myocardial infarction, or death in hospitalized stroke patients. Neurology 2010, 74, 588–593. [Google Scholar] [CrossRef]
- Allen, N.B.; Holford, T.R.; Bracken, M.B.; Goldstein, L.B.; Howard, G.; Wang, Y.; Lichtman, J.H. Trends in one-year recurrent ischemic stroke among the elderly in the USA: 1994–2002. Cerebrovasc. Dis. 2010, 30, 525–532. [Google Scholar] [CrossRef]
- Callaly, E.; Ni Chroinin, D.; Hannon, N.; Marnane, M.; Akijian, L.; Sheehan, O.; Merwick, A.; Hayden, D.; Horgan, G.; Duggan, J.; et al. Rates, Predictors, and Outcomes of Early and Late Recurrence After Stroke: The North Dublin Population Stroke Study. Stroke 2016, 47, 244–246. [Google Scholar] [CrossRef] [Green Version]
- Hillen, T.; Coshall, C.; Tilling, K.; Rudd, A.G.; McGovern, R.; Wolfe, C.D. South London Stroke Register. Cause of stroke recurrence is multifactorial: Patterns, risk factors, and outcomes of stroke recurrence in the South London Stroke Register. Stroke 2003, 34, 1457–1463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bye, A.; Røsjø, H.; Nauman, J.; Silva, G.J.; Follestad, T.; Omland, T.; Wisløff, U. Circulating microRNAs predict future fatal myocardial infarction in healthy individuals—The HUNT study. J. Mol. Cell. Cardiol. 2016, 97, 162–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayr, B.; Müller, E.E.; Schäfer, C.; Droese, S.; Schönfelder, M.; Niebauer, J. Exercise-induced changes in miRNA expression in coronary artery disease. Clin. Chem. Lab. Med. 2021. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group I Carotid Involvement N = 47 | Group II Coronary Involvement N = 40 | Group III Carotid and Coronary Involvements N = 55 | ANOVA p-Value | |
|---|---|---|---|---|
| Demographic data | ||||
| Age, (years) | 68.8 ± 9.7 | 57.3 ± 10.1 | 68.7 ± 9.2 | <0.001 *; 0.996 **; <0.001 *** |
| Male, n (%) | 27 (57%) | 27 (68%) | 37 (67%) | 0.597 *; 0.561 **; 0.999 *** |
| Smoking habit, n (%) | 27 (57%) | 26 (65%) | 36 (65%) | 0.751 *; 0.686 **; 0.998 *** |
| Hypertension, n (%) | 44 (94%) | 31 (78%) | 53 (96%) | 0.026 *; 0.882 **; 0.005 *** |
| Diabetes, n (%) | 14 (30%) | 19 (48%) | 23 (42%) | 0.210 *; 0.429 **; 0.841 *** |
| Hypercholesterolemia, n (%) | 42 (89%) | 34 (85%) | 45 (82%) | 0.837 *; 0.537 **; ***0.903 |
| Renal artery stenosis, n (%) | 13 (28%) | 6 (15%) | 9 (16%) | 0.629 *; 0.496 **; ***0.105 |
| Peripheral artery disease, n (%) | 13 (28%) | 5 (13%) | 15 (27%) | 0.215 *; 0.998 **; ***0.210 |
| Laboratory data | ||||
| Serum creatinine, (µmol/L) | 86.3 ± 31.0 | 76.8 ± 15.5 | 91.4 ± 28.9 | 0.222 *; 0.599 **; 0.023 *** |
| C-reactive protein, (g/L) | 4.07 ± 8.02 | 10.32 ± 16.5 | 5.83 ± 6.38 | 0.017 *; 0.681 **; 0.104 *** |
| LDL cholesterol, (mmol/L) | 2.62 ± 1.04 | 3.83 ± 1.32 | 2.71 ± 0.93 | <0.001 *; 0.923 **; <0.001 *** |
| Fibrinogen, (g/L) | 3.88 ± 1.34 | 4.02 ± 1.71 | 3.78 ± 1.37 | 0.909 *; 0.937 **; 0.729 *** |
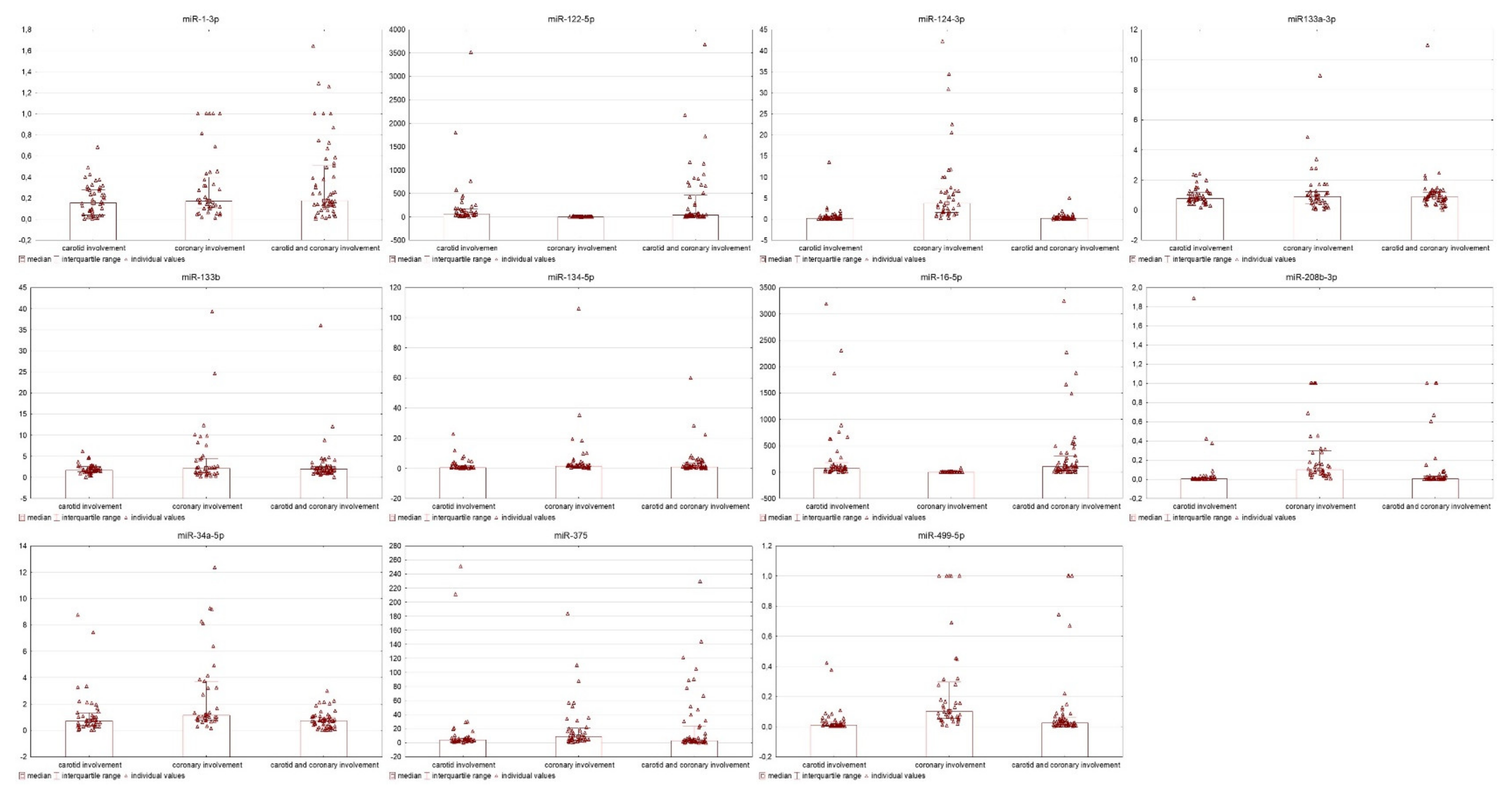
| miR expression | ||||
| miR-1-3p, A.U. | 0.18 ± 0.15 | 0.31 ± 0.31 | 0.35 ± 0.37 | 0.147 *; 0.016 **; 0.756 *** |
| miR-122-5p, A.U. | 244.1 ± 592 | 1.94 ± 3.01 | 338.7 ± 664.8 | 0.095 *; 0.664 **; 0.007 *** |
| miR-124-3p, A.U. | 0.77 ± 2.06 | 7.36 ± 9.64 | 0.44 ± 0.74 | <0.001 *; 0.950 **; <0.001 *** |
| miR-133a-3p, A.U. | 0.96 ± 0.55 | 1.23 ± 1.58 | 1.48 ± 3.10 | 0.832 *; 0.453 **; 0.839 *** |
| miR-133b, A.U. | 1.95 ± 1.15 | 4.45 ± 7.38 | 2.95 ± 4.97 | 0.065 *; 0.598 **; 0.342 *** |
| miR-134-5p, A.U. | 9.75 ± 50.9 | 6.37 ± 17.4 | 3.79 ± 9.20 | 0.869 *; 0.606 **; 0.914 *** |
| miR-16-5p, A.U. | 155 ± 225 | 3.25 ± 11.7 | 149 ± 175 | <0.001 *; 0.986 **; <0.001 *** |
| miR-208b-3p, A.U. | 0.07 ± 0.29 | 0.24 ± 0.32 | 0.64 ± 2.78 | 0.887 *; 0.251 **; 0.539 *** |
| miR-34a-5p, A.U. | 1.95 ± 5.16 | 4.85 ± 9.97 | 0.77 ± 0.65 | 0.076 *; 0.604 **; 0.004 *** |
| miR-375, A.U. | 38.6 ± 112.7 | 22.15 ± 35.5 | 24.6 ± 35.1 | 0.995 *; 0.593 **; 0.546 *** |
| miR-499-5p, A.U. | 0.38 ± 0.08 | 0.24 ± 0.32 | 0.11 ± 0.25 | <0.001 *; 0.253 **; 0.018 *** |
| CVD/MI/IS incidence, n (%) # | 18 (38.3%) | 19 (47.5%) | 25 (45.5%) | 0.719 *; 0.755 **; 0.992 *** |
| CVD | 15 | 11 | 18 | 0.606 *; 0.938 **; 0.544 *** |
| MI | 3 | 11 | 10 | 0.008 *; 0.075 **; 0.301 *** |
| IS | 6 | 2 | 8 | 0.200 *; 0.799 **; 0.127 *** |
| Cardiovascular Adverse Events | Univariate Cox Analysis | Multivariate Cox Analysis | ||
|---|---|---|---|---|
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| CVD/MI/IS | ||||
| Peripheral artery disease | 2.07 (1.22–3.52) | 0.007 | 2.16 (1.26–3.70) | 0.004 |
| miR-122-5p | 1.0005 (1.0003–1.001) | 0.039 | 1.0006 (1.0001–1.0011) | 0.017 |
| miR-16-5p | 1.0003 (1.0001–1.0006) | 0.010 | NS | |
| CVD | ||||
| Age | 1.03 (1.01–1.06) | 0.026 | NS | |
| Peripheral artery disease | 3.19 (1.73–5.86) | <0.001 | 3.47 (1.88–6.41) | <0.001 |
| Carotid and coronary involvement | 1.96 (1.06–3.65) | 0.032 | NS | |
| miR-1-3p | 2.41 (1.05–5.52) | 0.036 | 2.73 (1.22–6.12) | 0.014 |
| miR-16-5p | 1.0003 (1.000–1.0007) | 0.012 | NS | |
| MI | ||||
| Diabetes | 2.11 (0.91–4.87) | 0.081 | NS | |
| miR-1-3p | 2.36 (0.78–717) | 0.100 | NS | |
| miR-16-5p | 1.0004 (1.0001–1.0008) | 0.011 | 1.0004 (1.0001–1.0008) | 0.011 |
| IS | ||||
| Age | 1.04 (0.99–1.09) | 0.085 | NS | |
| Renal artery stenosis | 3.48 (1.29–9.35) | 0.013 | NS | |
| Creatinine level | 1.02 (1.01–1.03) | 0.001 | 1.02 (1.01–1.03) | <0.001 |
| miR-122-5p | 1.000 (0.9999–1.0001) | 0.070 | 1.0001 (1.000–1.0002) | 0.024 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badacz, R.; Kleczyński, P.; Legutko, J.; Żmudka, K.; Gacoń, J.; Przewłocki, T.; Kabłak-Ziembicka, A. Expression of miR-1-3p, miR-16-5p and miR-122-5p as Possible Risk Factors of Secondary Cardiovascular Events. Biomedicines 2021, 9, 1055. https://doi.org/10.3390/biomedicines9081055
Badacz R, Kleczyński P, Legutko J, Żmudka K, Gacoń J, Przewłocki T, Kabłak-Ziembicka A. Expression of miR-1-3p, miR-16-5p and miR-122-5p as Possible Risk Factors of Secondary Cardiovascular Events. Biomedicines. 2021; 9(8):1055. https://doi.org/10.3390/biomedicines9081055
Chicago/Turabian StyleBadacz, Rafał, Paweł Kleczyński, Jacek Legutko, Krzysztof Żmudka, Jacek Gacoń, Tadeusz Przewłocki, and Anna Kabłak-Ziembicka. 2021. "Expression of miR-1-3p, miR-16-5p and miR-122-5p as Possible Risk Factors of Secondary Cardiovascular Events" Biomedicines 9, no. 8: 1055. https://doi.org/10.3390/biomedicines9081055