
Serum Leptin and Resistin Levels in Knee Osteoarthritis—Clinical and Radiologic Links: Towards Precise Definition of Metabolic Type Knee Osteoarthritis


 ,
,  ,
, 
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Assessment of Adipokines
2.3. Statistical Analysis
3. Results
3.1. Leptin and Resistin Levels in Knee OA Patients with Different BMI
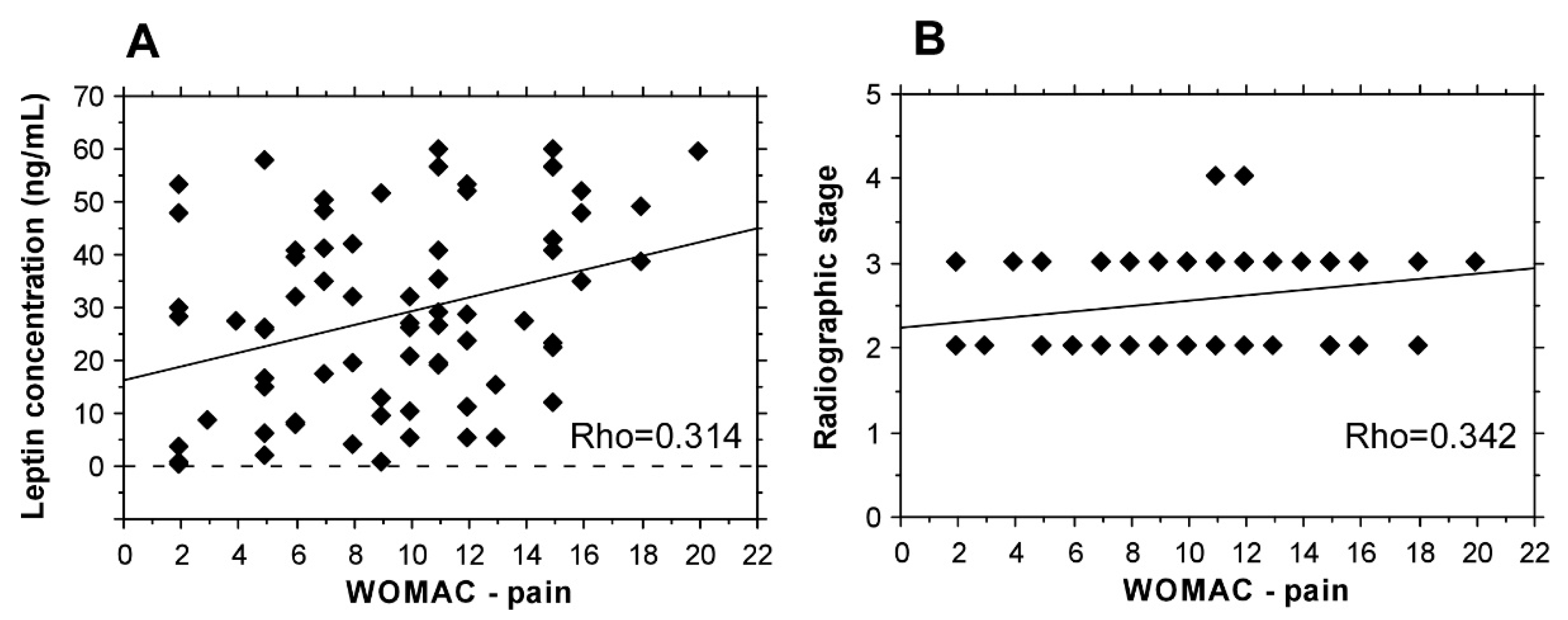
3.2. Leptin and Resistin Levels and WOMAC-Pain Score in Knee OA
3.3. Association of Leptin and Resistin Levels with Radiographic Stage of Knee OA
3.4. Clinical Associations in Knee OA with Different BMI
4. Discussion
4.1. Leptin and Resistin Levels in Knee OA with Different BMI
4.2. Leptin and Resistin Levels in Different Clinical Forms of OA
4.3. Leptin and Resistin Levels and WOMAC-Pain Score in Knee OA
4.4. Leptin and Resistin Levels and Radiographic Stage of Knee OA
4.5. Clinical Associations in Knee OA with Different BMI
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cicuttini, F.M.; Baker, J.R.; Spector, T.D. The association of obesity with osteoarthritis of the hand and knee in women: A twin study. J. Rheumatol. 1996, 23, 1221–1226. [Google Scholar]
- Dell’Isola, A.; Allan, R.; Smith, S.L.; Marreiros, S.S.; Steultjens, M. Identification of clinical phenotypes in knee osteoarthritis: A systematic review of the literature. BMC Musculoskelet. Disord. 2016, 17, 425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azamar-Llamas, D.; Hernandez-Molina, G.; Ramos-Avalos, B.; Furuzawa-Carballeda, J. Adipokine Contribution to the Pathogenesis of Osteoarthritis. Mediat. Inflamm. 2017, 2017, 5468023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, Y.H.; Zhao, C.W.; Liu, B.; Dong, N.; Ding, L.; Li, Y.R.; Liu, J.G.; Feng, W.; Qi, X.; Jin, X.H. An update on the association between metabolic syndrome and osteoarthritis and on the potential role of leptin in osteoarthritis. Cytokine 2020, 129, 155043. [Google Scholar] [CrossRef]
- Sokolove, J.; Lepus, C.M. Role of inflammation in the pathogenesis of osteoarthritis: Latest findings and interpretations. Ther. Adv. Musculoskelet. Dis. 2013, 5, 77–94. [Google Scholar] [CrossRef]
- Conde, J.; Scotece, M.; Gomez, R.; Lopez, V.; Gomez-Reino, J.J.; Gualillo, O. Adipokines and osteoarthritis: Novel molecules involved in the pathogenesis and progression of disease. Arthritis 2011, 2011, 203901. [Google Scholar] [CrossRef] [Green Version]
- Yan, M.; Zhang, J.; Yang, H.; Sun, Y. The role of leptin in osteoarthritis. Medicine 2018, 97, e0257. [Google Scholar] [CrossRef]
- Izquierdo, A.G.; Crujeiras, A.B.; Casanueva, F.F.; Carreira, M.C. Leptin, Obesity, and Leptin Resistance: Where Are We 25 Years Later? Nutrients 2019, 11, 2704. [Google Scholar] [CrossRef] [Green Version]
- Otero, M.; Lago, R.; Gomez, R.; Lago, F.; Dieguez, C.; Gomez-Reino, J.J.; Gualillo, O. Changes in plasma levels of fat-derived hormones adiponectin, leptin, resistin and visfatin in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2006, 65, 1198–1201. [Google Scholar] [CrossRef] [Green Version]
- Vuolteenaho, K.; Koskinen, A.; Moilanen, E. Leptin–A Link between Obesity and Osteoarthritis. Applications for Prevention and Treatment. Basic Clin. Pharmacol. Toxicol. 2014, 114, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Bao, J.-p.; Chen, W.-p.; Feng, J.; Hu, P.-f.; Shi, Z.-l.; Wu, L.-D. Leptin plays a catabolic role on articular cartilage. Mol. Biol. Rep. 2009, 37, 3265–3272. [Google Scholar] [CrossRef]
- Karvonen-Gutierrez, C.A.; Harlow, S. Leptin levels are associated with knee osteoarthritis among mid-aged women. Osteoarthr. Cartil. 2012, 20, S189–S190. [Google Scholar] [CrossRef] [Green Version]
- Zhao, C.-W.; Gao, Y.-H.; Song, W.-X.; Liu, B.; Ding, L.; Dong, N.; Qi, X. An Update on the Emerging Role of Resistin on the Pathogenesis of Osteoarthritis. Mediat. Inflamm. 2019, 2019, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steppan, C.M.; Bailey, S.T.; Bhat, S.; Brown, E.J.; Banerjee, R.R.; Wright, C.M.; Patel, H.R.; Ahima, R.S.; Lazar, M.A. The hormone resistin links obesity to diabetes. Nature 2001, 409, 307–312. [Google Scholar] [CrossRef]
- Acquarone, E.; Monacelli, F.; Borghi, R.; Nencioni, A.; Odetti, P. Resistin: A reappraisal. Mech. Ageing Dev. 2019, 178, 46–63. [Google Scholar] [CrossRef] [PubMed]
- Patel, L.; Buckels, A.C.; Kinghorn, I.J.; Murdock, P.R.; Holbrook, J.D.; Plumpton, C.; Macphee, C.H.; Smith, S.A. Resistin is expressed in human macrophages and directly regulated by PPARγ activators. Biochem. Biophys. Res. Commun. 2003, 300, 472–476. [Google Scholar] [CrossRef]
- Senolt, L.; Housa, D.; Vernerova, Z.; Jirasek, T.; Svobodova, R.; Veigl, D.; Anderlova, K.; Muller-Ladner, U.; Pavelka, K.; Haluzik, M. Resistin in rheumatoid arthritis synovial tissue, synovial fluid and serum. Ann. Rheum. Dis. 2006, 66, 458–463. [Google Scholar] [CrossRef] [Green Version]
- Migita, K.; Maeda, Y.; Miyashita, T.; Kimura, H.; Nakamura, M.; Ishibashi, H.; Eguchi, K. The serum levels of resistin in rheumatoid arthritis patients. Clin. Exp. Rheumatol. 2006, 24, 698–701. [Google Scholar]
- Alissa, E.M.; Alzughaibi, L.S.; Marzouki, Z.M. Relationship between serum resistin, body fat and inflammatory markers in females with clinical knee osteoarthritis. Knee 2020, 27, 45–50. [Google Scholar] [CrossRef]
- Koskinen, A.; Vuolteenaho, K.; Moilanen, T.; Moilanen, E. Resistin as a factor in osteoarthritis: Synovial fluid resistin concentrations correlate positively with interleukin 6 and matrix metalloproteinases MMP-1 and MMP-3. Scand. J. Rheumatol. 2014, 43, 249–253. [Google Scholar] [CrossRef]
- Wang, K.; Xu, J.; Cai, J.; Zheng, S.; Yang, X.; Ding, C. Serum levels of resistin and interleukin-17 are associated with increased cartilage defects and bone marrow lesions in patients with knee osteoarthritis. Mod. Rheumatol. 2016, 27, 339–344. [Google Scholar] [CrossRef]
- Van Spil, W.E.; Welsing, P.M.J.; Kloppenburg, M.; Bierma-Zeinstra, S.M.; Bijlsma, J.W.J.; Mastbergen, S.C.; Lafeber, F.P.J.G. Cross-sectional and predictive associations between plasma adipokines and radiographic signs of early-stage knee osteoarthritis: Data from CHECK. Osteoarthr. Cartil. 2012, 20, 1278–1285. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.-C.; Lin, C.-Y.; Kuo, S.-J.; Liu, S.-C.; Lu, Y.-C.; Chen, Y.-L.; Wang, S.-W.; Tang, C.-H. Resistin Enhances VCAM-1 Expression and Monocyte Adhesion in Human Osteoarthritis Synovial Fibroblasts by Inhibiting MiR-381 Expression through the PKC, p38, and JNK Signaling Pathways. Cells 2020, 9, 1369. [Google Scholar] [CrossRef]
- Philp, A.M.; Collier, R.L.; Grover, L.M.; Davis, E.T.; Jones, S.W. Resistin promotes the abnormal Type I collagen phenotype of subchondral bone in obese patients with end stage hip osteoarthritis. Sci. Rep. 2017, 7, 4042. [Google Scholar] [CrossRef] [Green Version]
- Kellgren, J.H.; Lawrence, J.S. Radiological Assessment of Osteo-Arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khanna, V.; Sharma, R. Incidence of primary osteoarthritis knee below 40 years of age and its etiological factors: OPD survey of 200 knee pain patients. Indian J. Orthop. Surg. 2019, 5, 88–94. [Google Scholar] [CrossRef]
- Altman, R.; Asch, E.; Bloch, D.; Bole, G.; Borenstein, D.; Brandt, K.; Christy, W.; Cooke, T.D.; Greenwald, R.; Hochberg, M.; et al. Development of criteria for the classification and reporting of osteoarthritis: Classification of osteoarthritis of the knee. Arthritis Rheum. 1986, 29, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Nelson, A.E.; Smith, M.W.; Golightly, Y.M.; Jordan, J.M. “Generalized osteoarthritis”: A systematic review. Semin. Arthritis Rheum. 2014, 43, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Stratford, P.W.; Kennedy, D.M.; Woodhouse, L.J.; Spadoni, G.F. Measurement properties of the WOMAC LK 3.1 pain scale. Osteoarthr. Cartil. 2007, 15, 266–272. [Google Scholar] [CrossRef] [Green Version]
- Kroon, F.P.B.; Veenbrink, A.I.; de Mutsert, R.; Visser, A.W.; van Dijk, K.W.; le Cessie, S.; Rosendaal, F.R.; Kloppenburg, M. The role of leptin and adiponectin as mediators in the relationship between adiposity and hand and knee osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1761–1767. [Google Scholar] [CrossRef]
- Francisco, V.; Pérez, T.; Pino, J.; López, V.; Franco, E.; Alonso, A.; Gonzalez-Gay, M.A.; Mera, A.; Lago, F.; Gómez, R.; et al. Biomechanics, obesity, and osteoarthritis. The role of adipokines: When the levee breaks. J. Orthop. Res. 2018, 36, 594–604. [Google Scholar] [CrossRef] [Green Version]
- Gualillo, O.; Sun, A.R.; Panchal, S.K.; Friis, T.; Sekar, S.; Crawford, R.; Brown, L.; Xiao, Y.; Prasadam, I. Obesity-associated metabolic syndrome spontaneously induces infiltration of pro-inflammatory macrophage in synovium and promotes osteoarthritis. PLoS ONE 2017, 12, e0183693. [Google Scholar] [CrossRef] [Green Version]
- Kluzek, S.; Newton, J.L.; Arden, N.K. Is osteoarthritis a metabolic disorder? Br. Med Bull. 2015, 115, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Berenbaum, F.; Walker, C. Osteoarthritis and inflammation: A serious disease with overlapping phenotypic patterns. Postgrad. Med. 2020, 132, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Berenbaum, F. Deep phenotyping of osteoarthritis: A step forward. Ann. Rheum. Dis. 2019, 78, 3–5. [Google Scholar] [CrossRef] [Green Version]
- Askari, A.; Arasteh, P.; Homayounfar, R.; Naghizadeh, M.M.; Ehrampoush, E.; Mousavi, S.M.; Alipoor, R. The role of adipose tissue secretion in the creation and pain level in osteoarthritis. Endocr. Regul. 2020, 54, 6–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvet, J.; Orellana, C.; Albinana Gimenez, N.; Berenguer-Llergo, A.; Caixas, A.; Garcia-Manrique, M.; Galisteo Lencastre, C.; Navarro, N.; Larrosa, M.; Gratacos, J. Differential involvement of synovial adipokines in pain and physical function in female patients with knee osteoarthritis. A cross-sectional study. Osteoarthr. Cartil. 2018, 26, 276–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.Z.; Guan, J.; Wang, H.J.; Ma, W.; Li, F.; Xu, F.; Ding, L.B.; Xie, L.; Liu, B.; Liu, K.; et al. Possible Involvement of Serum and Synovial Fluid Resistin in Knee Osteoarthritis: Cartilage Damage, Clinical, and Radiological Links. J. Clin. Lab. Anal. 2016, 30, 437–443. [Google Scholar] [CrossRef]
- Choe, J.-Y.; Bae, J.; Jung, H.-Y.; Park, S.-H.; Lee, H.-J.; Kim, S.-K. Serum resistin level is associated with radiographic changes in hand osteoarthritis: Cross-sectional study. Jt. Bone Spine 2012, 79, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Martel-Pelletier, J.; Raynauld, J.P.; Dorais, M.; Abram, F.; Pelletier, J.P. The levels of the adipokines adipsin and leptin are associated with knee osteoarthritis progression as assessed by MRI and incidence of total knee replacement in symptomatic osteoarthritis patients: A post hoc analysis. Rheumatology 2016, 55, 680–688. [Google Scholar] [CrossRef] [Green Version]
- Isidori, A.M.; Strollo, F.; Morè, M.; Caprio, M.; Aversa, A.; Moretti, C.; Frajese, G.; Riondino, G.; Fabbri, A. Leptin and Aging: Correlation with Endocrine Changes in Male and Female Healthy Adult Populations of Different Body Weights. J. Clin. Endocrinol. Metab. 2000, 85, 1954–1962. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Knee OA BMI ≥ 30 kg/m2 (Total n = 43) | Knee OA BMI ≤ 30 kg/m2 (Total n = 30) | Controls (n = 11) | ||
|---|---|---|---|---|
| Age | 62 ± 11 years 40 females, 3 males | 72 ± 7 years 26 females, 4 males | 72 ± 7 years 26 females, 4 males | Controls vs. patients with knee OA BMI ≥ 30 kg/m2 (p < 0.0001; Controls vs. patients with knee OA BMI < 30 kg/m2 (p < 0.0001); Patients with knee OA and BMI ≥ 30 kg/m2 vs. patients with knee OA and BMI < 30 kg/m2 (p = 0.0002) |
| BMI mean ± SD | 38.68 ± 7.98 kg/m2 | 25.03 ± 2.91 kg/m2 | 27.87 ± 8.830 kg/m2 | Controls vs. patients with knee OA BMI ≥ 30 kg/m2 (p < 0.0001; Controls vs. patients with knee OA BMI < 30 kg/m2 (p = 0.23); Patients with knee OA and BMI ≥ 30 kg/m2 vs. patients with knee OA and BMI < 30 kg/m2 (p < 0.0001) |
| Clinical forms |
|
|
| Leptin | Resistin | |
|---|---|---|
| 35.06 ± 20.11 ng/mL 23.43 ± 17.63 ng/mL 28.67 ± 17.66 ng/mL 15.83 ± 16.53 ng/ml | 3.026 ± 0.776 ng/mL 1.908 ± 0.900 ng/mL 2.441 ± 1.250 ng/mL 1.610 ± 1.001 ng/ml |
| Controls vs. isolated knee OA p < 0.05; Controls vs. knee OA combined with spondyloarthritis ± hip OA p < 0.05; Generalized OA vs. isolated knee OA p > 0.05: Knee OA combined with spondyloarthritis ± hip OA vs. isolated knee OA p > 0.05; Knee OA combined with spondyloarthritis ± hip OA vs. generalized OA p > 0.05 | Controls vs. isolated knee OA p < 0.05; Controls vs. knee OA combined with spondyloarthritis ± hip OA p < 0.05; Generalized OA vs. isolated knee OA p > 0.05: Knee OA combined with spondyloarthritis ± OA vs. isolated knee OA p > 0.05; Knee OA combined with spondyloarthritis ± OA vs. generalized OA p > 0.05 |
| BMI | |
|---|---|
| 41.48 ± 13.68 kg/m2 29.19 ± 3.45 kg/m2 32.65 ± 8.83 kg/m2 |
| Generalized OA vs. isolated knee OA p < 0.05: Knee OA combined with spondyloarthritis ± hip OA vs. isolated knee OA p < 0.05; Knee OA combined with spondyloarthritis ± hip OA vs. generalized OA p = 0.28 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lambova, S.N.; Batsalova, T.; Moten, D.; Stoyanova, S.; Georgieva, E.; Belenska-Todorova, L.; Kolchakova, D.; Dzhambazov, B. Serum Leptin and Resistin Levels in Knee Osteoarthritis—Clinical and Radiologic Links: Towards Precise Definition of Metabolic Type Knee Osteoarthritis. Biomedicines 2021, 9, 1019. https://doi.org/10.3390/biomedicines9081019
Lambova SN, Batsalova T, Moten D, Stoyanova S, Georgieva E, Belenska-Todorova L, Kolchakova D, Dzhambazov B. Serum Leptin and Resistin Levels in Knee Osteoarthritis—Clinical and Radiologic Links: Towards Precise Definition of Metabolic Type Knee Osteoarthritis. Biomedicines. 2021; 9(8):1019. https://doi.org/10.3390/biomedicines9081019
Chicago/Turabian StyleLambova, Sevdalina Nikolova, Tsvetelina Batsalova, Dzhemal Moten, Stela Stoyanova, Elenka Georgieva, Lyudmila Belenska-Todorova, Desislava Kolchakova, and Balik Dzhambazov. 2021. "Serum Leptin and Resistin Levels in Knee Osteoarthritis—Clinical and Radiologic Links: Towards Precise Definition of Metabolic Type Knee Osteoarthritis" Biomedicines 9, no. 8: 1019. https://doi.org/10.3390/biomedicines9081019