
Efficacy and Safety of 10 kHz Spinal Cord Stimulation for the Treatment of Chronic Pain: A Systematic Review and Narrative Synthesis of Real-World Retrospective Studies

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Study Eligibility
2.3. Reviewers
2.4. Data Extraction
3. Results
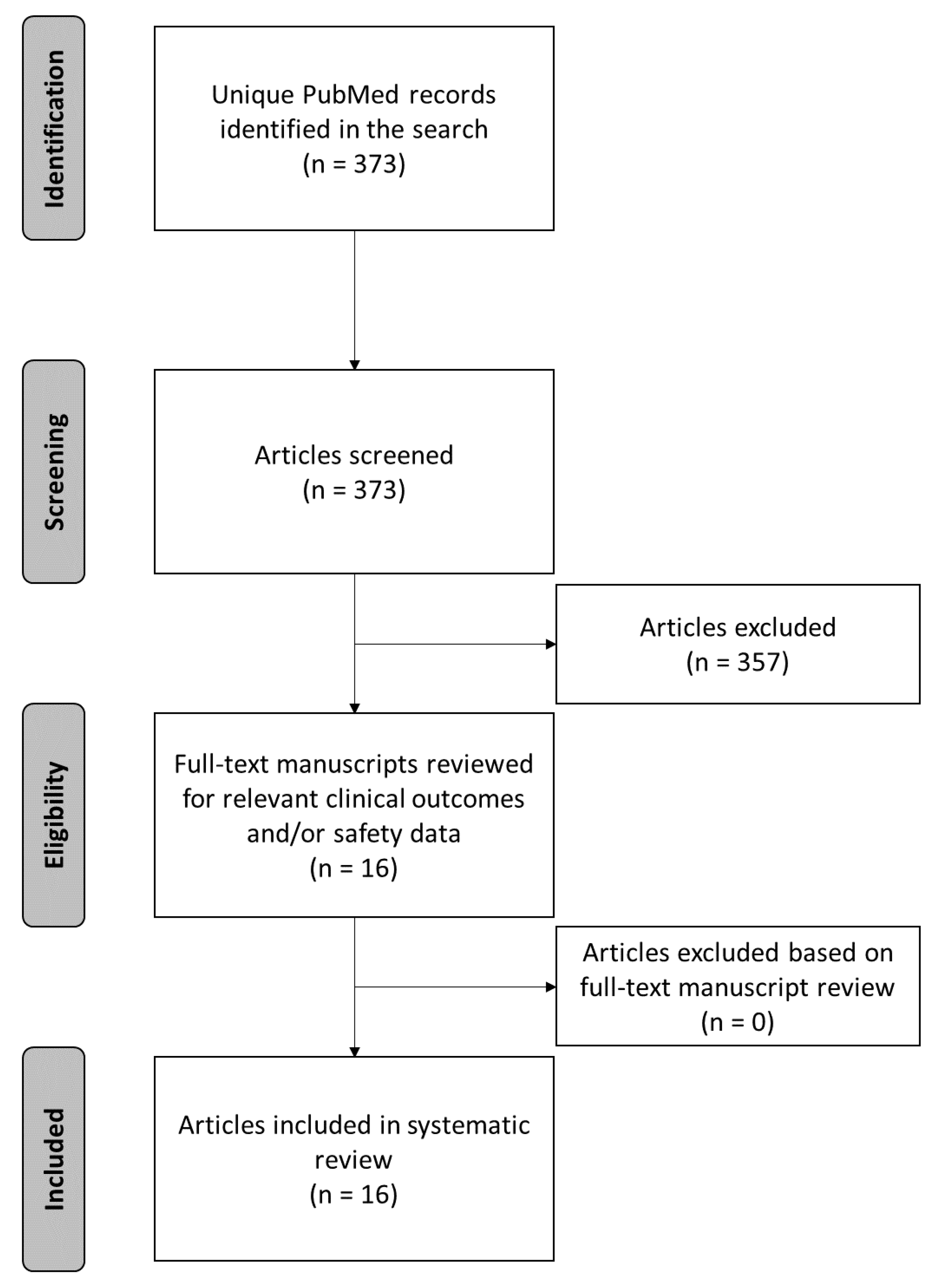
3.1. Study Selection
3.2. Study Characteristics
3.3. Effectiveness Outcomes with Predominant Thoracic Lead Placement
3.3.1. Studies with ≤12 Months of Follow-Up
3.3.2. Studies with >12 Months of Follow-Up
3.4. Effectiveness Outcomes in Studies with Predominant Cervical Lead Placement
3.4.1. Studies with ≤12 Months of Follow-Up
3.4.2. Studies with >12 Months of Follow-Up
3.5. Effectiveness Outcomes in Studies with Combined Thoracic and Cervical Lead Placement
3.6. Safety Outcomes
3.6.1. Lead Migration
3.6.2. Infection
3.6.3. Pain over the Site of the Implantable Pulse Generator
3.6.4. Insufficient Pain Relief/Nonresponders/Treatment Failure
3.6.5. Lead Fracture
3.6.6. Neurological Injury
3.6.7. System Explantation
4. Discussion
4.1. Effectiveness Outcomes
4.2. Safety Summary
4.3. Strengths and Limitations
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Dahlhamer, J.; Lucas, J.; Zelaya, C.; Nahin, R.; Mackey, S.; DeBar, L.; Kerns, R.; Von Korff, M.; Porter, L.; Helmick, C. Prevalence of chronic pain and high-impact chronic pain among adults-United States, 2016. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1001–1006. [Google Scholar] [CrossRef]
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef]
- Goldberg, D.S.; McGee, S.J. Pain as a global public health priority. BMC Public Health 2011, 11, 770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaskin, D.J.; Richard, P. The economic costs of pain in the United States. J. Pain 2012, 13, 715–724. [Google Scholar] [CrossRef] [PubMed]
- Raftery, M.N.; Ryan, P.; Normand, C.; Murphy, A.W.; de la Harpe, D.; McGuire, B.E. The economic cost of chronic noncancer pain in Ireland: Results from the PRIME study, part 2. J. Pain 2012, 13, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Gustavsson, A.; Bjorkman, J.; Ljungcrantz, C.; Rhodin, A.; Rivano-Fischer, M.; Sjolund, K.-F.; Mannheimer, C. Socio-economic burden of patients with a diagnosis related to chronic pain--register data of 840,000 Swedish patients. Eur. J. Pain 2012, 16, 289–299. [Google Scholar] [CrossRef]
- Allegri, M.; Lucioni, C.; Mazzi, S.; Serra, G. Social cost of chronic pain in Italy. Glob. Reg. Health Technol. Assess. 2015, 2, 33–42. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.S.; Farquharson, R.; Carroll, D.; Moore, A.; Phillips, C.J.; Taylor, R.S.; Barden, J. The impact and burden of chronic pain in the workplace: A qualitative systematic review. Pain Pract. 2012, 12, 578–589. [Google Scholar] [CrossRef]
- Duenas, M.; Ojeda, B.; Salazar, A.; Mico, J.A.; Failde, I. A review of chronic pain impact on patients, their social environment and the health care system. J. Pain Res. 2016, 9, 457–467. [Google Scholar] [CrossRef] [Green Version]
- Reid, K.J.; Harker, J.; Bala, M.M.; Truyers, C.; Kellen, E.; Bekkering, G.E.; Kleijnen, J. Epidemiology of chronic non-cancer pain in Europe: Narrative review of prevalence, pain treatments and pain impact. Curr. Med. Res. Opin. 2011, 27, 449–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pain-Assessment, Non-Opioid Treatment Approaches and Opioid Management (Health Care Guideline); Institute for Clinical Systems Improvement: Bloomington, MN, USA, 2017.
- Majedi, H.; Dehghani, S.S.; Soleyman-Jahi, S.; Tafakhori, A.; Emami, S.A.; Mireskandari, M.; Hosseini, S.M. Assessment of factors predicting inadequate pain management in chronic pain patients. Anesth. Pain Med. 2019, 9, e97229. [Google Scholar] [CrossRef] [Green Version]
- Glare, P.; Aubrey, K.R.; Myles, P.S. Transition from acute to chronic pain after surgery. Lancet 2019, 393, 1537–1546. [Google Scholar] [CrossRef]
- Tompkins, D.A.; Hobelmann, J.G.; Compton, P. Providing chronic pain management in the ‘’Fifth Vital Sign” Era: Historical and treatment perspectives on a modern-day medical dilemma. Drug Alcohol Depend. 2017, 173 (Suppl. 1), S11–S21. [Google Scholar] [CrossRef]
- Meske, D.S.; Lawal, O.; Elder, H.; Langberg, V.; Paillard, F.; Katz, N. Efficacy of opioids versus placebo in chronic pain: A systematic review and meta-analysis of enriched enrollment randomized withdrawal trials. J. Pain Res. 2018, 11, 923–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, R.; Turner, J.A.; Devine, E.B.; Hansen, R.N.; Sullivan, S.D.; Blazina, I.; Dana, T.; Bougatsos, C.; Deyo, R.A. The effectiveness and risks of long-term opioid therapy for chronic pain: A systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann. Intern. Med. 2015, 162, 276–286. [Google Scholar] [CrossRef] [Green Version]
- Stannard, C.D. Where now for opioids in chronic pain? Drug Ther. Bull. 2018, 56, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Cooper, T.E.; Chen, J.; Wiffen, P.J.; Derry, S.; Carr, D.B.; Aldington, D.; Cole, P.; Moore, R.A. Morphine for chronic neuropathic pain in adults. Cochr. Database Syst. Rev. 2017, 5, CD011669. [Google Scholar] [CrossRef] [PubMed]
- Gaskell, H.; Derry, S.; Stannard, C.; Moore, R.A. Oxycodone for neuropathic pain in adults. Cochr. Database Syst Rev. 2016, 7, CD010692. [Google Scholar] [CrossRef]
- Baldini, A.; Von Korff, M.; Lin, E.H. A review of potential adverse effects of long-term opioid therapy: A practitioner’s guide. Prim. Care Compan. CNS Disord 2012, 14, 36. [Google Scholar] [CrossRef] [Green Version]
- Kalso, E.; Edwards, J.E.; Moore, R.A.; McQuay, H.J. Opioids in chronic non-cancer pain: Systematic review of efficacy and safety. Pain 2004, 112, 372–380. [Google Scholar] [CrossRef]
- Benyamin, R.; Trescot, A.; Datta, S.; Buenaventura, R.; Adlaka, R.; Sehgal, N.; Glaser, S.E.; Vallejo, R. Opioid complications and side effects. Pain Physician 2008, 11, S105–S120. [Google Scholar]
- Vowles, K.E.; McEntee, M.L.; Julnes, P.S.; Frohe, T.; Ney, J.P.; van der Goes, D.N. Rates of opioid misuse, abuse, and addiction in chronic pain: A systematic review and data synthesis. Pain 2015, 156, 569–576. [Google Scholar] [CrossRef] [Green Version]
- Ives, T.J.; Chelminski, P.R.; Hammett-Stabler, C.A.; Malone, R.M.; Perhac, J.S.; Potisek, N.M.; Shilliday, B.B.; DeWalt, D.A.; Pignone, M.P. Predictors of opioid misuse in patients with chronic pain: A prospective cohort study. BMC Health Serv. Res. 2006, 6, 46. [Google Scholar] [CrossRef] [Green Version]
- Kapural, L.; Yu, C.; Doust, M.W.; Gliner, B.E.; Vallejo, R.; Sitzman, B.T.; Amirdelfan, K.; Morgan, D.M.; Brown, L.L.; Yearwood, T.L.; et al. Novel 10-kHz High-frequency therapy (HF10 Therapy) is superior to traditional low-frequency spinal cord stimulation for the treatment of chronic back and leg pain: The SENZA-RCT randomized controlled trial. Anesthesiology 2015, 123, 851–860. [Google Scholar] [CrossRef]
- Kapural, L.; Yu, C.; Doust, M.; Kapural, L.; Yu, C.; Doust, M.W.; Gliner, B.E.; Vallejo, R.; Sitzman, B.T.; Amirdelfan, K.; et al. Multicenter randomized controlled pivotal trial comparing 10 khz and traditional spinal cord stimulation: 24-month results. Pain Pract. 2016, 16, 22. [Google Scholar]
- Van Buyten, J.P.; Al-Kaisy, A.; Smet, I.; Palmisani, S.; Smith, T. High-frequency spinal cord stimulation for the treatment of chronic back pain patients: Results of a prospective multicenter European clinical study. Neuromodulation 2013, 16, 59–65, discussion-6. [Google Scholar] [CrossRef]
- Al-Kaisy, A.; Van Buyten, J.P.; Smet, I.; Palmisani, S.; Pang, D.; Smith, T. Sustained effectiveness of 10 kHz high-frequency spinal cord stimulation for patients with chronic, low back pain: 24-month results of a prospective multicenter study. Pain Med. 2014, 15, 347–354. [Google Scholar] [CrossRef]
- Al-Kaisy, A.; Palmisani, S.; Smith, T.E.; Pang, D.; Lam, K.; Burgoyne, W.; Houghton, R.; Hudson, E.; Lucas, J. 10 kHz High-frequency spinal cord stimulation for chronic axial low back pain in patients with no history of spinal surgery: A preliminary, prospective, open label and proof-of-concept study. Neuromodulation 2017, 20, 63–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Kaisy, A.; Palmisani, S.; Smith, T.E.; Carganillo, R.; Houghton, R.; Pang, D.; Burgoyne, W.; Lam, K.; Lucas, J. Long-Term Improvements in chronic axial low back pain patients without previous spinal surgery: A cohort analysis of 10-kHz high-frequency spinal cord stimulation over 36 months. Pain Med. 2018, 19, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Scowcroft, J.; Kloster, D.; Guirguis, M.; Carlson, J.; McJunkin, T.; Chaiban, G.; Israel, A.; Subbaroyan, J. 10-kHz spinal cord stimulation for chronic postsurgical pain: Results from a 12-month prospective, multicenter study. Pain Pract. 2020, 20, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Tate, J.L.; Stauss, T.; Li, S.; Rotte, A.; Subbaroyan, J. A prospective, multi-center, clinical trial of a 10-kHz spinal cord stimulation system in the treatment of chronic pelvic pain. Pain Pract. 2020, 21, 12932. [Google Scholar]
- Mekhail, N.A.; Argoff, C.E.; Taylor, R.S.; Nasr, C.; Caraway, D.L.; Gliner, B.E.; Subbaroyan, J.; Brooks, E.S. High-frequency spinal cord stimulation at 10 kHz for the treatment of painful diabetic neuropathy: Design of a multicenter, randomized controlled trial (SENZA-PDN). Trials 2020, 21, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapural, L.; Gupta, M.; Paicius, R.; Strodtbeck, W.; Vorenkamp, K.E.; Gilmore, C.; Gliner, B.; Rotte, A.; Subbaroyan, J.; Province-Azalde, R. Treatment of chronic abdominal pain with 10-kHz spinal cord stimulation: Safety and efficacy results from a 12-month prospective, multicenter, feasibility study. Clin. Transl. Gastroenterol. 2020, 11, e00133. [Google Scholar] [CrossRef] [PubMed]
- Arcioni, R.; Palmisani, S.; Mercieri, M.; Vano, V.; Tigano, S.; Smith, T.; Fiore, M.; Martelletti, P.; Al-Kaisy, A. Cervical 10 kHz spinal cord stimulation in the management of chronic, medically refractory migraine: A prospective, open-label, exploratory study. Eur. J. Pain 2016, 20, 70–78. [Google Scholar] [CrossRef]
- Amirdelfan, K.; Vallejo, R.; Benyamin, R.; Yu, C.; Yang, T.; Bundschu, R.; Yearwood, T.L.; Sitzman, B.T.; Gliner, B.; Subbaroyan, J.; et al. High-frequency spinal cord stimulation at 10 kHz for the treatment of combined neck and arm pain: Results from a prospective multicenter study. Neurosurgery 2020, 87, 176–185. [Google Scholar] [CrossRef] [Green Version]
- Spieth, P.M.; Kubasch, A.S.; Penzlin, A.I.; Illigens, B.M.; Barlinn, K.; Siepmann, T. Randomized controlled trials-a matter of design. Neuropsychiatr. Dis. Treat. 2016, 12, 1341–1349. [Google Scholar]
- Frieden, T.R. Evidence for health decision making-beyond randomized, controlled trials. N. Engl. J. Med. 2017, 377, 465–475. [Google Scholar] [CrossRef]
- Price, D.; Bateman, E.D.; Chisholm, A.; Papadopoulos, N.G.; Bosnic-Anticevich, S.; Pizzichini, E.; Hillyer, E.V.; Buist, A.S. Complementing the randomized controlled trial evidence base. Evolution not revolution. Ann. Am. Thorac. Soc. 2014, 11 (Suppl. 2), S92–S98. [Google Scholar] [CrossRef] [PubMed]
- Faraoni, D.; Schaefer, S.T. Randomized controlled trials vs. observational studies: Why not just live together? BMC Anesthesiol. 2016, 16, 102. [Google Scholar] [CrossRef] [Green Version]
- Sayed, D.; Kallewaard, J.W.; Rotte, A.; Jameson, J.; Caraway, D. Pain relief and improvement in quality of life with 10 kHz SCS therapy: Summary of clinical evidence. CNS Neurosci. Ther. 2020, 26, 403–415. [Google Scholar] [CrossRef]
- Russo, M.; Van Buyten, J.P. 10-kHz high-frequency SCS therapy: A clinical summary. Pain Med. 2015, 16, 934–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Kaisy, A.; Van Buyten, J.P.; Amirdelfan, K.; Gliner, B.; Caraway, D.; Subbaroyan, J.; Rotte, A.; Kapural, L. Opioid-sparing effects of 10 kHz spinal cord stimulation: A review of clinical evidence. Ann. NY Acad. Sci. 2020, 1462, 53–64. [Google Scholar] [CrossRef] [Green Version]
- Luecke, T.; Edgar, D.; Huse, D. 10 kHz spinal cord stimulation for the treatment of chronic back and/or leg pain: Summary of clinical studies. SAGE Open Med. 2020, 8, 2050312120951369. [Google Scholar] [CrossRef] [PubMed]
- Al-Kaisy, A.; Royds, J.; Al-Kaisy, O.; Palmisani, S.; Pang, D.; Smith, T.; Padfield, N.; Harris, S.; Markham, K.; Wesley, S.; et al. Cascade programming for 10 kHz spinal cord stimulation: A single center case series of 114 patients with neuropathic back and leg pain. Neuromodulation 2020. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, P.E.; Gill, J.S.; Simopoulos, T. The evolving role of high-frequency spinal cord stimulation as salvage therapy in neurostimulation. Pain Pract. 2020, 20, 706–713. [Google Scholar] [CrossRef]
- Sayed, D.; Foster, J.; Nairizi, A.; Sills, S.; Miller, A. 10 kHz high-frequency spinal cord stimulation for chronic thoracic pain: A multicenter case series and a guide for optimal anatomic lead placement. Pain Phys. 2020, 23, E369–E376. [Google Scholar]
- Sayed, D.; Salmon, J.; Khan, T.W.; Sack, A.M.; Braun, T.; Barnard, A.; Rotte, A. Retrospective analysis of real-world outcomes of 10 kHz SCS in patients with upper limb and neck pain. J. Pain Res. 2020, 13, 1441–1448. [Google Scholar] [CrossRef]
- Sills, S. Treatment of painful polyneuropathies of diabetic and other origins with 10 kHz SCS: A case series. Postgrad. Med. 2020, 132, 352–357. [Google Scholar] [CrossRef]
- El Majdoub, F.; Neudorfer, C.; Richter, R.; Schieferdecker, S.; Maarouf, M. 10 kHz cervical SCS for chronic neck and upper limb pain: 12 months’ results. Ann. Clin. Transl. Neurol. 2019, 6, 2223–2229. [Google Scholar] [CrossRef]
- Finch, P.; Price, L.; Drummond, P. High-frequency (10 kHz) electrical stimulation of peripheral nerves for treating chronic pain: A double-blind trial of presence vs absence of stimulation. Neuromodulation 2019, 22, 529–536. [Google Scholar] [CrossRef]
- Gill, J.S.; Asgerally, A.; Simopoulos, T.T. High-frequency spinal cord stimulation at 10 kHz for the treatment of complex regional pain syndrome: A case series of patients with or without previous spinal cord stimulator implantation. Pain Pract. 2019, 19, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Salmon, J. High-frequency spinal cord stimulation at 10 kHz for widespread pain: A retrospective survey of outcomes from combined cervical and thoracic electrode placements. Postgrad. Med. 2019, 131, 230–238. [Google Scholar] [CrossRef]
- Schieferdecker, S.; Neudorfer, C.; El Majdoub, F.; Maarouf, M. A retrospective case series of high-frequency spinal cord stimulation (HF10-SCS) in neurogenic bladder incontinence. Oper Neurosurg. 2019, 17, 14–20. [Google Scholar] [CrossRef]
- Stauss, T.; El Majdoub, F.; Sayed, D.; Surges, G.; Rosenberg, W.S.; Kapural, L.; Bundschu, R.; Lalkhen, A.; Patel, N.; Gliner, B.; et al. A multicenter real-world review of 10 kHz SCS outcomes for treatment of chronic trunk and/or limb pain. Ann. Clin. Transl. Neurol. 2019, 6, 496–507. [Google Scholar] [CrossRef]
- DiBenedetto, D.J.; Wawrzyniak, K.M.; Schatman, M.E.; Kulich, R.J.; Finkelman, M. 10 kHz spinal cord stimulation: A retrospective analysis of real-world data from a community-based, interdisciplinary pain facility. J. Pain Res. 2018, 11, 2929–2941. [Google Scholar] [CrossRef] [Green Version]
- Simopoulos, T.; Yong, R.J.; Gill, J.S. Treatment of chronic refractory neuropathic pelvic pain with high-frequency 10-kilohertz spinal cord stimulation. Pain Pract. 2018, 18, 805–809. [Google Scholar] [CrossRef]
- Van Buyten, J.P.; Wille, F.; Smet, I.; Wensing, C.; Breel, J.; Karst, E.; Devos, M.; Pöggel-Krämer, K.; Vesper, J. Therapy-related explants after spinal cord stimulation: Results of an international retrospective chart review study. Neuromodulation 2017, 20, 642–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russo, M.; Verrills, P.; Mitchell, B.; Salmon, J.; Barnard, A.; Santarelli, D. High frequency spinal cord stimulation at 10 kHz for the treatment of chronic pain: 6-month australian clinical experience. Pain Phys. 2016, 19, 267–280. [Google Scholar]
- Al-Kaisy, A.; Palmisani, S.; Smith, T.; Harris, S.; Pang, D. The use of 10-kilohertz spinal cord stimulation in a cohort of patients with chronic neuropathic limb pain refractory to medical management. Neuromodulation 2015, 18, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Cameron, T. Safety and efficacy of spinal cord stimulation for the treatment of chronic pain: A 20-year literature review. J. Neurosurg. 2004, 100, 254–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, J.A.; Loeser, J.D.; Deyo, R.A.; Sanders, S.B. Spinal cord stimulation for patients with failed back surgery syndrome or complex regional pain syndrome: A systematic review of effectiveness and complications. Pain 2004, 108, 137–147. [Google Scholar] [CrossRef]
- Kumar, K.; Hunter, G.; Demeria, D. Spinal cord stimulation in treatment of chronic benign pain: Challenges in treatment planning and present status, a 22-year experience. Neurosurgery 2006, 58, 481–496. [Google Scholar] [CrossRef]
- Mekhail, N.A.; Mathews, M.; Nageeb, F.; Guirguis, M.; Mekhail, M.N.; Cheng, J. Retrospective review of 707 cases of spinal cord stimulation: Indications and complications. Pain Pract. 2011, 11, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Eldabe, S.; Buchser, E.; Duarte, R.V. Complications of spinal cord stimulation and peripheral nerve stimulation techniques: A review of the literature. Pain Med. 2015, 17, 325–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleiber, J.C.; Marlier, B.; Bannwarth, M.; Theret, E.; Peruzzi, P.; Litre, F. Is spinal cord stimulation safe? A review of 13 years of implantations and complications. Rev. Neurol. 2016, 172, 689–695. [Google Scholar] [CrossRef]
- Hoelzer, B.C.; Bendel, M.A.; Deer, T.R.; Eldrige, J.S.; Walega, D.R.; Wang, Z.; Costandi, S.; Azer, G.; Qu, W.; Falowski, S.M.; et al. Spinal cord stimulator implant infection rates and risk factors: A multicenter retrospective study. Neuromodul. Technol. Neural Interface 2017, 20, 558–562. [Google Scholar] [CrossRef] [PubMed]
- Hayek, S.M.; Veizi, E.; Hanes, M. Treatment-limiting complications of percutaneous spinal cord stimulator implants: A review of eight years of experience from an academic center database. Neuromodulation 2015, 18, 603–608. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Year Published | Single/ Multicenter | Consecutive Patients | Follow-Up Duration | Key Inclusion | Outcomes Reported | Geographical Location |
|---|---|---|---|---|---|---|---|
| Al-Kaisy et al. [45] | 2020 | Single center | Yes | 15.1 ± 4.2 mo | Back pain with or without leg pain and programmed using Cascade protocol | NRS, responder rate, trial-to-perm ratio, and PGIC. | UK |
| Ghosh et al. [46] | 2020 | Single center | Yes | 21.2 ± 8.4 mo | Failed traditional SCS trial or permanent implant | NRS, responder rate, trial-to-perm ratio, ODI, and SFMPQ. | USA |
| Sayed et al. [47] | 2020 | Multicenter | Yes | 12 mo | Thoracic back pain and lead(s) placed between T1–T6 | NRS, responder rate, general change in function and sleep, and change in medication. | USA |
| Sayed et al. [48] | 2020 | Multicenter | Yes | 19.4 ± 12.4 mo | Neck and/or upper limb pain | VRS, patient-reported percentage pain relief, responder rate, general change in function and sleep, and change in medication. | USA |
| Sills [49] | 2020 | Single center | Yes | 29.8 mo | Peripheral neuropathy | VNRS, responder rate, trial-to-perm ratio, change in sensation, change in medication, and general improvement. | USA |
| El Majdoub et al. [50] | 2019 | Single center | Yes | 12 mo | Neck and/or upper limb pain | VAS, trial-to-perm ratio, ODI, and GAF, change in medication, and satisfaction. | Germany |
| Finch et al. [51] | 2019 | Single center | Yes | 12 mo | Chronic pain and implanted with a 10 kHz SCS system | VAS, ODI, and change in medication. | Australia |
| Gill et al. [52] | 2019 | Single center | Yes | 12.1 ± 4.6 mo | Uni- or bilateral CRPS | NRS, patient-reported percentage pain relief, responder rate, trial-to-perm ratio, and SF-MPQ-2. | USA |
| Salmon [53] | 2019 | Single center | Yes | 2.3 ± 1.7 y | Combined upper and lower body neuropathic/nociplastic pain syndromes | NRS, trial-to-perm ratio, RMDQ, PGIC, PSEQ, DASS, satisfaction, opioid use, and employment capacity. | USA |
| Schieferdecker et al. [54] | 2019 | Single center | No | 10.0 mo | Trunk and/or limb pain + neurogenic bladder dysfunction | NRS, ICIQ-LUTSqol, micturition frequency, incontinence frequency, residual volume, and catheterization frequency. | Germany |
| Stauss et al. [55] | 2019 | Multicenter | Yes | 8.9 ± 6.7 mo | Trunk and/or limb pain | VNRS, patient-reported percentage pain relief, responder rate, trial-to-perm ratio, changes in medication use, general change in function and sleep, general QoL, and satisfaction. | Germany, UK, and USA. |
| DiBenedetto et al. [56] | 2018 | Single center | Yes | 12 mo | Back pain with or without leg pain | Daily MME, visit volume, functional pain scale, NRS, PCS, PHQ-9, PHQ-15, Generalized Anxiety Disorder-7, WHODAS 2.0, and RMDQ-m. | USA |
| Simopoulos et al. [57] | 2018 | Single center | No | 10.7 mo | Neuropathic pelvic pain | VAS | USA |
| Van Buyten et al. [58] | 2017 | Multicenter | Yes | 2.83 y | Implanted with SCS device for dorsal column stimulation | Explants | Belgium, Germany, and the Netherlands. |
| Russo et al. [59] | 2016 | Multicenter | Yes | 6 mo | Not candidates for SCS or nonresponders | NPRS, responder rate, trial-to-perm ratio, ODI, and activity tolerance. | Australia |
| Al-Kaisy et al. [60] | 2015 | Single center | Yes | 6 mo | Neuropathic pain in the upper or lower limbs | NRS, responder rate, trial-to-perm ratio, BPI, PCS, EQ-5D, painDETECT, and satisfaction. | UK |
| Reference | Year | N Implanted Subjects | Pain Location | Lead Location | Responder Rate % (n/N) | Average Pain Relief % (N) | Opioid/Medication Change from Baseline to Last Follow-Up | Patients that Reduced or Eliminated Opioids/Medication at Last Follow-Up (%, n/N) | Average Functional Change from Baseline to Last Follow-Up (N) | Patients that Improved Functional Outcomes at last Follow-Up (%, n/N) | Average QoL Change from Baseline to Last Follow-Up (N) | Patients that Improved QoL Outcomes at Last Follow-Up (%, n/N) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Stauss et al. [55] | 2019 | 1660 | Back and leg pain: 84% (1370/1640) Other: 16% (270/1640) | NR (Back and/or leg pain: Typically T8-T12) | All patients: 74% (838/1131) Previous LF-SCS subgroup: 74% (197/266) | All patients: 63% (NR) Previous LF-SCS subgroup: 63% (N = 266) | NR | All patients 32% (343/1070) Previous LF-SCS subgroup: 33% (13/40) | NR | General improvement in function: All patients: 72% (787/1088) Previous LF-SCS subgroup: 83% (33/40) | NR | General improvement in sleep: All patients: 68% (694/1020) Previous LF-SCS subgroup: 70% (21/30) |
| Russo et al. [59] | 2016 | 186 | Back and/or leg: 69% (177/256) Head ± neck: 8% (21/256) Neck ± arm/shoulder: 6% (15/256) Other/ unrecorded: 17% (43/256) | Low back and/or leg pain: T8-T11 Neck and arm pain: C2/3 disc, C3, C4 | All patients: NR Previous SCS/PNFS subgroup: 55% (21/38) | All patients: 51% (p < 0.001; N = 125) Previous SCS/PNFS subgroup: 49% (p < 0.001; N = 38) | NR | NR | ODI score: All patients: 41.4 to 32.8 points (21% reduction; p < 0.001; N = 68) Previous SCS/PNFS subgroup: NR | NR | NR | NR |
| Finch et al. [51] | 2019 | 58 | Spinal: 84% (49/58) Other: 16% (9/58) | T9-T10: 93% (54/58) T9-T10 + T1-T2: 3% (2/58) T9-T10 + C2: 3% (2/58) | NR | NR (p < 0.001; N = 58) | Change from baseline to 3–6 months clinical review: 72.7 to 62.8 mg/day MEDD (p < 0.05, N = 57) | NR | Change from baseline to 3–6 months clinical review in ODI score: 50.4 to 36.6 points (27% reduction; p < 0.001; N = 56) | NR | NR | NR |
| DiBenedetto et al. [56] | 2018 | 32 | Back ± leg | NR (Back and/or leg pain: Typically T8-T12) | Back pain: NR Leg pain: NR | Back: 46% (p < 0.001; N = 30) Leg: 51% (p = 0.01; N = 16) | 92.2 to 66.0 mg/day MEDD (28% reduction; p = 0.001; N = 21) | 71% (15/21) | RMDQ-m score: 13.9 to 10.8 points (22% reduction; p = 0.02; N = 21) WHO-DAS score: 1.97 to 1.92 points (p = 0.57; N = 19) | NR | NR | NR |
| Sayed et al. [47] | 2020 | 19 | Thoracic back | T1-T6 | 89% (17/19) (Last-follow-up) | 70% (p = 0.004; N = 9) | NR | 47% (9/19) | NR | General improvement in function: 84% (16/19) | NR | General improvement in sleep: 74% (14/19) |
| Gill et al. [52] | 2019 | 12 | Lower extremities: 83% (10/12) Upper extremities: 17% (2/12) | T8–T12: 83% (10/12) C2–C7: 17% (2/12) | All patients: 67% (8/12) Previous LF-SCS subgroup: 71% (5/7) | All patients: NR Previous LF-SCS subgroup: 58% (N = 7) | NR | NR | NR | NR | NR | NR |
| Schieferdecker et al. [54] | 2019 | 5 | Back and/or legs: 80% (4/5) Other: 20% (1/5) | T9-T10 (4/5) T8-T9 (1/5) | 6 mo: 100% (4/4) 12 mo: 100% (2/2) | 6 mo: 56% (N = 4) 12 mo: 53% (N = 2) | NR | NR | NR | NR | Incontinence frequency: 80% reduction (N = 5) ICIQ-LUTSqol score: 38% reduction (N = 5) | Incontinence frequency: 100% (5/5) ICIQ-LUTSqol score: 100% (N = 5) |
| Simopoulos et al. [57] | 2018 | 3 | Pelvis | T8 superior endplate + mid-T9 | 67% (2/3) | 53% (N = 3) | n = 1 reported a 75% reduction in opioids | NR | NR | NR | NR | NR |
| Al-Kaisy et al. [45] | 2020 | 99 | Back ± leg | T8-T10 | Back pain: 56% (40/72) Leg pain: 59% (34/58) | Back: 52% (p < 0.0001; N = 72) Leg: 53% (p < 0.0001; N = 58) | NR | NR | NR | NR | NR | PGIC scale: 83% of patients moderately to a great deal better (60/72) |
| Ghosh et al. [46] | 2020 | 28 | FBSS: 61% (17/28) CRPS: 32% (9/28) Other (neck, groin, or rectal pain): 7% (2/28) | NR (Back and/or leg pain: Typically T8-T12) | All patients: 46% (13/28) FBSS subgroup: 35% (6/17) CRPS subgroup: 67% (6/9) | All responding patients *: 64% (p < 0.0001; N = 13) FBSS subgroup *: 60% (p < 0.0001; N = 6) CRPS subgroup *: 52% (p < 0.0001; N = 6) | NR | NR | ODI score: FBSS subgroup: 58.3 to 38.6 points (34% reduction; p < 0.0001; N = 17) | ODI category: FBSS subgroup: 44% reduced their disability category from severe and/or bedbound to minimal and/or moderate | NR | NR |
| Sills [49] | 2020 | 6 | Lower extremities ± feet: 67% (4/6) Legs + feet: 17% (1/6) Low back + legs: 17% (1/6) | Stimulation near T9-T10 | 50% (3/6) | 60% (N = 6) | NR | 67% (4/6) | NR | NR | NR | Sensation: 67% (4/6) reported improvements (3 PDPN; 1 iPN) |
| Al-Kaisy et al. [60] | 2015 | 11 | Upper limb: 73% (8/11) Lower limb: 27% (3/11) | C2–C7: 73% (8/11) T8–T12: 27% (3/11) | 73% (8/11) | 59% (p < 0.05; N = 11) | NR | NR | NR | NR | EQ5D time trade off score: 101% increase (N = 11) PCS score: 33 to 7 points (79% reduction; N = 11) BPI score: 57.6 to 29.4 points (49% reduction; N = 10) | NR |
| El Majdoub et al. [50] | 2019 | 23 | Neck and/or upper limb | C2 | NR | Neck pain: 74% (p < 0.01; N = 20) Upper limb: 77% (p < 0.05; N = 20) | Opioids: 1020 to 450 mg/day morphine equivalent total daily dosage (56% reduction; N = 23) NSAIDs: 6750 mg/day to 1425 mg/day total daily dosage (79% reduction; N = 10) | NR | ODI score: 31.0 to 19.8 points (36% reduction, N = 20) GAF median interval: 50–41% to 70–61% (N = 20) | NR | NR | NR |
| Sayed et al. [48] | 2020 | 47 | Neck and/or upper limb | C2-C6 | All patients: 76% (35/46) Surgery naïve: 71% (17/24) Previous spine surgery: 83% (15/18) | All patients: 58% (N = 46) Surgery naïve: 59% (NR) Previous spine surgery: 60% (NR) | NR | All patients: 36% (17/47) | NR | General improvement in function: All patients: 72% (34/47) | NR | General improvement in sleep: 53% (25/47) |
| Salmon [53] | 2019 | 38 | Truncal/spinal regions + distal extremities | C2 + T9: 37% (13/35) C2 + T2 + T9: 37% (13/35) C2 + T2: 26% (9/35) | NR | All patients: 48% (p = 0.00001; N = 35) Head and neck pain subgroup: 63% (NR) Upper back pain subgroup: 60% (NR) Lower back pain subgroup: 59% (NR) | Patients on opioids at last follow-up: 165.4 to 99.3 mg/day MEDD (40% reduction; N = 15) Patients on high-dose opioids: 210.5 to 111.8 mg/day MEDD (47% reduction; N = 11) | 38% (9/24) | RMDQ score: 12.3 to 7.8 points (37% reduction; p ≤ 0.05; N = 29) | NR | PSEQ score:21.0 to 34.0 points (62% increase; N = 29) DASS: 6.9% to 3.6% of patients classified as moderately severe (N = 29) 10.3% to 7.1% of patients classified as severe (N = 29) Work participation in work eligible patients: 8/31 to 20/31 patients | PGIC: 79% moderately to a great deal better (23/29) |
| Reference | Year Published | Safety Population N | Adverse Event | Affected Patients n (%) | Status at Time of Reporting |
|---|---|---|---|---|---|
| Stauss et al. [55] | 2019 | 1290 | Explant due to infection | 22 (1.7%) | - |
| Explant due to loss of efficacy | 15 (1.2%) | - | |||
| Explant for other reasons | 11 (0.9%) | - | |||
| Russo et al. [59] | 2016 | 186 | Lead migration | 3 (1.6%) | NR |
| IPG /anchor site pain | 2 (1.1%) | NR | |||
| Infection | 1 (0.5%) | NR | |||
| Loss of therapy efficacy | 1 (0.5%) | NR | |||
| Van Buyten et al. [58] | 2017 | 155 | Explant due to ineffective stimulation | 22 (14.2%) * | - |
| Al-Kaisy et al. [45] | 2020 | 114 | Infection during trial | 4 (3.5%) | 4/4 systems explanted with permanent implantations carried out later |
| 99 | IPG site pain | 16 (16.2%) | 9/16 had surgical intervention; 7/16 managed conservatively | ||
| Lead migration | 7 (7.1%) | 6/7 had leads revised; 1/7 elected not to have revision | |||
| Suspected hardware malfunction | 1 (1.0%) | 1/1 system replaced | |||
| Infection after permanent implantation | 0 (0.0%) | - | |||
| Finch et al. [51] | 2019 | 58 | All complications, including wound infection, hematoma, lead migration, and IPG repositioning | 21 (36.2%) | NR |
| Sayed et al. [48] | 2020 | 47 | Insufficient pain relief | 2 (4.3%) | 2/2 resolved with programming |
| Overstimulation | 2 (4.3%) | 2/2 resolved with programming | |||
| IPG site pain | 1 (2.1%) | 1/1 resolved with programming | |||
| Salmon [53] | 2020 | 38 | Revision due to lead migration | 0 (0.0%) | - |
| Insufficient pain relief | 6 (15.8%) | 6/6 had additional epidural leads placed | |||
| IPG site pain | 6 (15.8%) | 6/6 managed conservatively | |||
| Electrode high impedance | 1 (2.6%) | 1/1 lead replaced | |||
| Explant due to infection | 0 (0.0%) | - | |||
| Ghosh et al. [46] | 2020 | 28 | Bleeding | 0 (0.0%) | - |
| Infection | 0 (0.0%) | - | |||
| Neurological deficit | 0 (0.0%) | - | |||
| El Majdoub et al. [50] | 2019 | 23 | Infection | 3 (13.0%) | 3/3 systems explanted |
| Lead migration | 1 (4.3%) | 1/1 lead revised and pain decreased to previous level | |||
| Al-Kaisy et al. [60] | 2015 | 15 | Infection during trial | 1 (6.7%) | 1/1 lead(s) removed and permanent implantation planned 6 months later |
| 11 | IPG site pain | 3 (27.3%) | 3/3 transient only | ||
| Lead migration | 2 (18.2%) | 2/2 had lead revisions: 1/2 (post-fall) regained pain relief; 1/2 failed to respond after revision | |||
| Neurological deficit | 0 (0.0%) | - | |||
| Gill et al. [52] | 2019 | 12 | Any complications | 0 (0.0%) | - |
| Reference | Infection | IPG Site Pain | Migration | Lead Fracture |
|---|---|---|---|---|
| Cameron 2004 [61] | 3.4% | 0.9% | 13.2% | 9.1% |
| Turner et al. 2004 [62] | 4.6% | 5.8% | 23.1% | 10.2% |
| Kumar et al. 2006 [63] | 3.4% | 1.2% | 21.5% | 5.9% |
| Mekhail et al. 2011 [64] | 4.5% | 12.0% | 22.6% | 6.0% |
| Eldabe et al. 2015 [65] | 4.9% | 6.2% | 15.5% | 6.4% |
| Kleiber et al. 2016 [66] | 4.2% | 6.4% | 0.0% | 3.8% |
| Hoelzer et al. 2017 [67] | 2.5% | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baranidharan, G.; Edgar, D.; Bretherton, B.; Crowther, T.; Lalkhen, A.-G.; Fritz, A.-K.; Vajramani, G. Efficacy and Safety of 10 kHz Spinal Cord Stimulation for the Treatment of Chronic Pain: A Systematic Review and Narrative Synthesis of Real-World Retrospective Studies. Biomedicines 2021, 9, 180. https://doi.org/10.3390/biomedicines9020180
Baranidharan G, Edgar D, Bretherton B, Crowther T, Lalkhen A-G, Fritz A-K, Vajramani G. Efficacy and Safety of 10 kHz Spinal Cord Stimulation for the Treatment of Chronic Pain: A Systematic Review and Narrative Synthesis of Real-World Retrospective Studies. Biomedicines. 2021; 9(2):180. https://doi.org/10.3390/biomedicines9020180
Chicago/Turabian StyleBaranidharan, Ganesan, Deborah Edgar, Beatrice Bretherton, Tracey Crowther, Abdul-Ghaaliq Lalkhen, Ann-Katrin Fritz, and Girish Vajramani. 2021. "Efficacy and Safety of 10 kHz Spinal Cord Stimulation for the Treatment of Chronic Pain: A Systematic Review and Narrative Synthesis of Real-World Retrospective Studies" Biomedicines 9, no. 2: 180. https://doi.org/10.3390/biomedicines9020180