
Netrin-1 in Atherosclerosis: Relationship between Human Macrophage Intracellular Levels and In Vivo Plaque Morphology

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Netrin Plasma Level Evaluation
2.3. Monocyte-Derived Macrophages (MDMs) Culture
2.4. Immunofluorescence Staining and Quantitative Analysis
2.5. OCT Image Acquisition and Analysis
2.6. Statistical Analysis
3. Results
3.1. Study Population
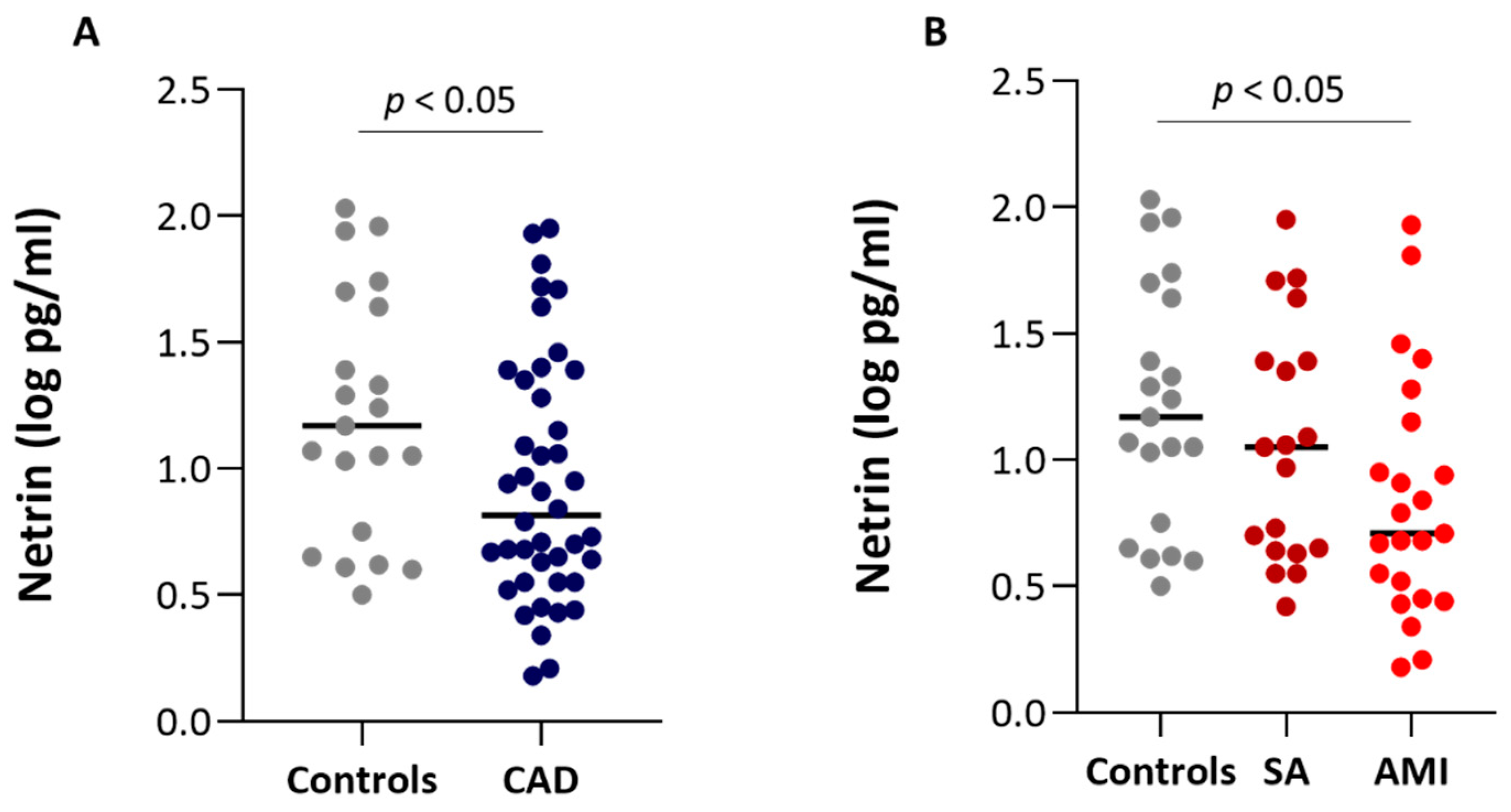
3.2. Netrin Plasma Levels
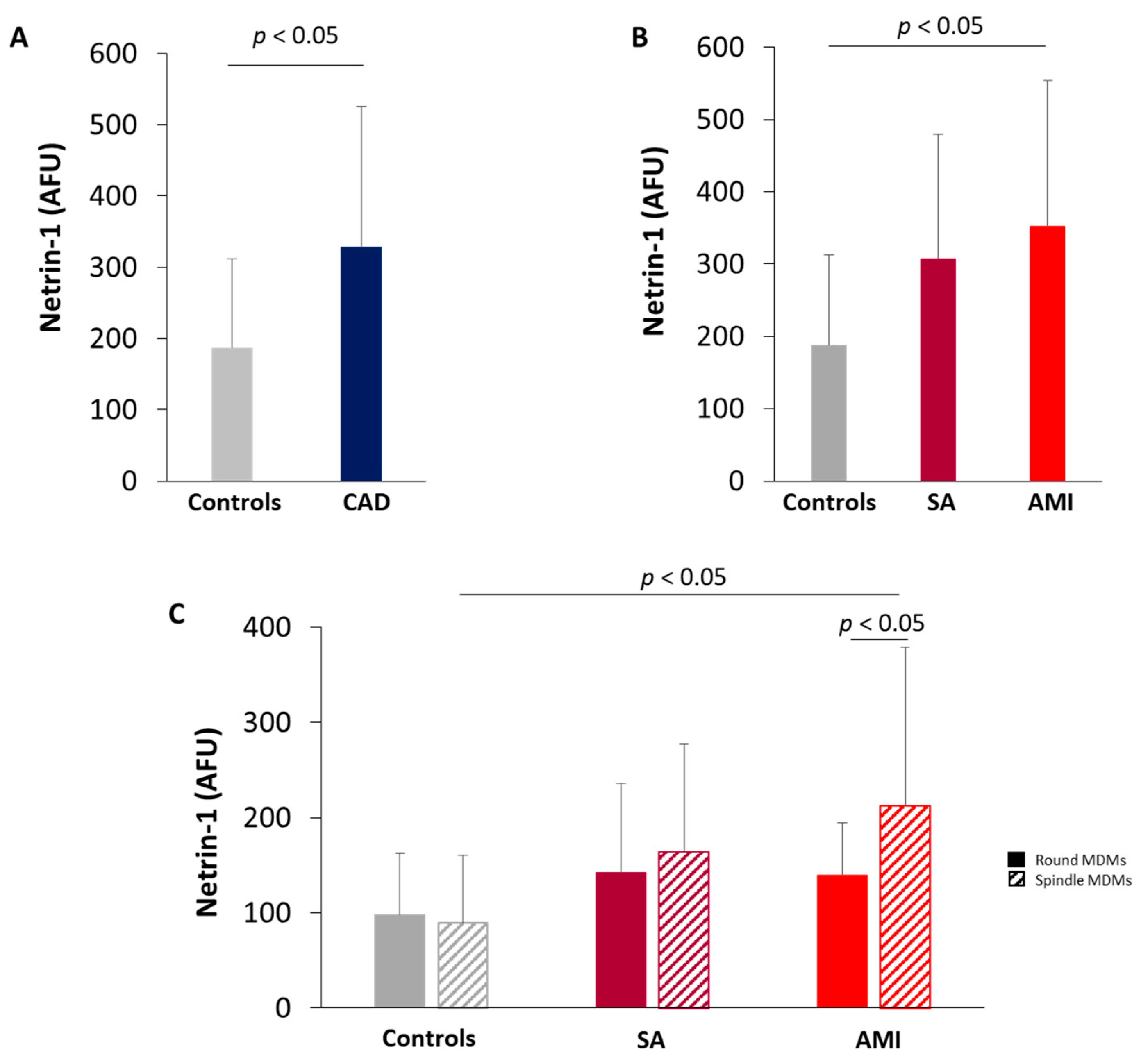
3.3. Netrin-1 Expression in MDMs
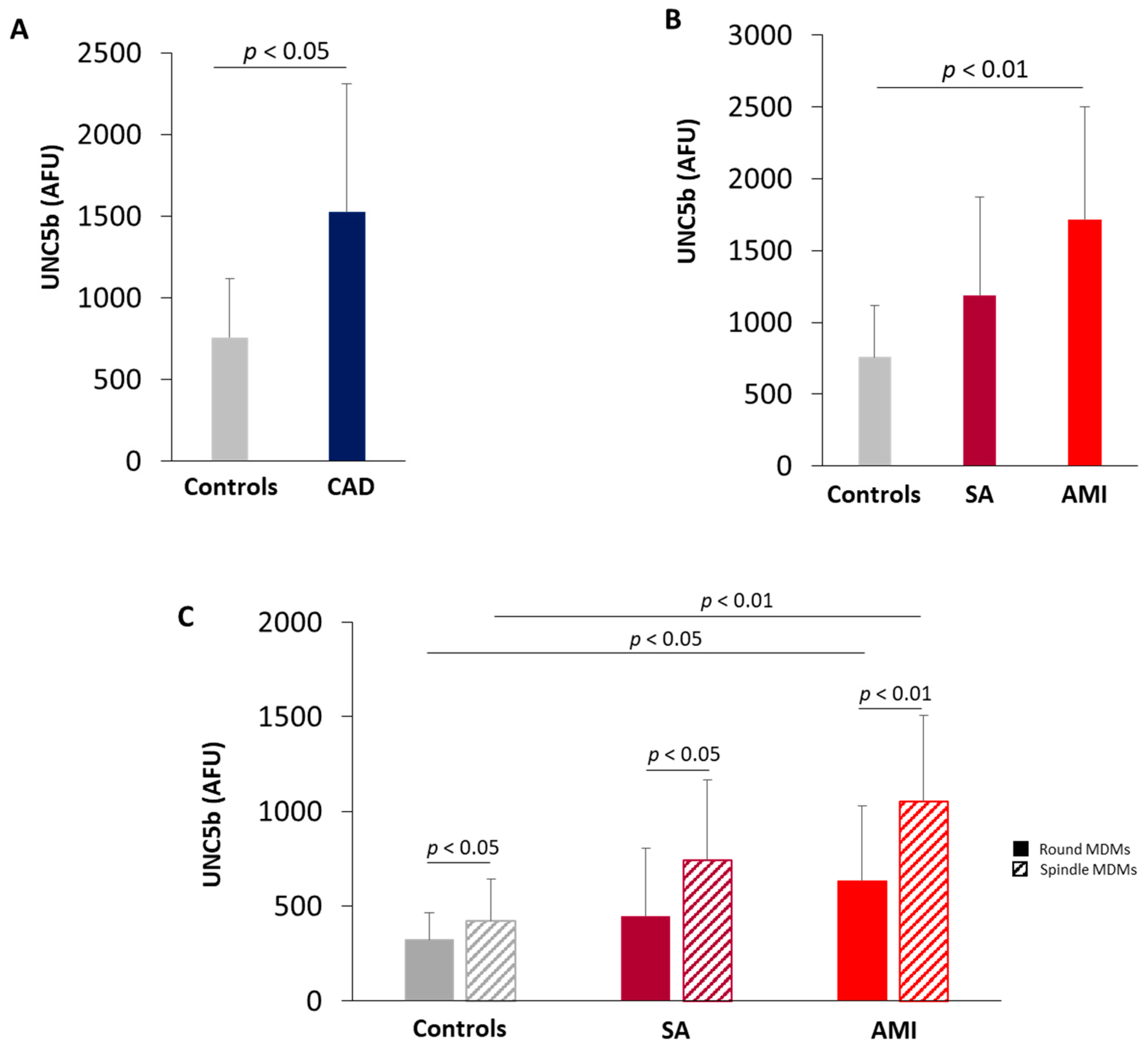
3.4. UNC5b Expression in MDMs
3.5. Correlation between the Intracellular Levels of Netrin-1 and Plaque Features Assessed by OCT
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Randolph, G.J. Emigration of monocyte-derived cells to lymph nodes during resolution of inflammation and its failure in atherosclerosis. Curr. Opin. Lipidol. 2008, 19, 462–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ly, N.P.; Komatsuzaki, K.; Fraser, I.P.; Tseng, A.A.; Prodhan, P.; Moore, K.J.; Kinane, T.B. Netrin-1 inhibits leukocyte migration in vitro and in vivo. Proc. Natl. Acad. Sci. USA 2005, 102, 14729–14734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, T.E.; Serafini, T.; de la Torre, J.R.; Tessier-Lavigne, M. Netrins are diffusible chemotropic factors for commissural axons in the embryonic spinal cord. Cell 1994, 78, 425–435. [Google Scholar] [CrossRef]
- Van Gils, J.M.; Ramkhelawon, B.; Fernandes, L.; Stewart, M.C.; Guo, L.; Seibert, T.; Menezes, G.B.; Cara, D.C.; Chow, C.; Kinane, T.B.; et al. Endothelial expression of guidance cues in vessel wall homeostasis dysregulation under proatherosclerotic conditions. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 911–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Z.; Jin, J.; Bai, W.; Li, J.; Shan, X. Netrin-1 prevents the attachment of monocytes to endothelial cells via an anti-inflammatory effect. Mol. Immunol. 2018, 103, 166–172. [Google Scholar] [CrossRef]
- van Gils, J.M.; Derby, M.C.; Fernandes, L.R.; Ramkhelawon, B.; Ray, T.D.; Rayner, K.J.; Parathath, S.; Distel, E.; Feig, J.L.; Alvarez-Leite, J.I.; et al. The neuroimmune guidance cue netrin-1 promotes atherosclerosis by inhibiting the emigration of macrophages from plaques. Nat. Immunol. 2012, 13, 136–143. [Google Scholar] [CrossRef] [Green Version]
- Rubina, K.A.; Tkachuk, V.A. Guidance Receptors in the Nervous and Cardiovascular Systems. Biochemistry. Biokhimiia 2015, 80, 1235–1253. [Google Scholar] [CrossRef]
- Ramkhelawon, B.; Yang, Y.; van Gils, J.M.; Hewing, B.; Rayner, K.J.; Parathath, S.; Guo, L.; Oldebeken, S.; Feig, J.L.; Fisher, E.A.; et al. Hypoxia induces netrin-1 and Unc5b in atherosclerotic plaques: Mechanism for macrophage retention and survival. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1180–1188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Zhang, J.; Chen, L.; Yuan, Z.; Qin, X.; Wu, Q.; Shen, D.; He, H.; Yu, C. The role of UNC5b in ox-LDL inhibiting migration of RAW264.7 macrophages and the involvement of CCR7. Biochem. Biophys. Res. Commun. 2018, 505, 637–643. [Google Scholar] [CrossRef]
- Eligini, S.; Cosentino, N.; Fiorelli, S.; Fabbiocchi, F.; Niccoli, G.; Refaat, H.; Camera, M.; Calligaris, G.; De Martini, S.; Bonomi, A.; et al. Biological profile of monocyte-derived macrophages in coronary heart disease patients: Implications for plaque morphology. Sci. Rep. 2019, 9, 8680. [Google Scholar] [CrossRef] [PubMed]
- Eligini, S.; Crisci, M.; Bono, E.; Songia, P.; Tremoli, E.; Colombo, G.I.; Colli, S. Human monocyte-derived macrophages spontaneously differentiated in vitro show distinct phenotypes. J. Cell. Physiol. 2013, 228, 1464–1472. [Google Scholar] [CrossRef] [PubMed]
- Scalone, G.; Niccoli, G.; Refaat, H.; Vergallo, R.; Porto, I.; Leone, A.M.; Burzotta, F.; D’Amario, D.; Liuzzo, G.; Fracassi, F.; et al. Not all plaque ruptures are born equal: An optical coherence tomography study. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1271–1277. [Google Scholar] [CrossRef] [Green Version]
- Prati, F.; Regar, E.; Mintz, G.S.; Arbustini, E.; Di Mario, C.; Jang, I.K.; Akasaka, T.; Costa, M.; Guagliumi, G.; Grube, E.; et al. Expert review document on methodology, terminology, and clinical applications of optical coherence tomography: Physical principles, methodology of image acquisition, and clinical application for assessment of coronary arteries and atherosclerosis. Eur. Heart J. 2010, 31, 401–415. [Google Scholar] [CrossRef]
- Tearney, G.J.; Yabushita, H.; Houser, S.L.; Aretz, H.T.; Jang, I.K.; Schlendorf, K.H.; Kauffman, C.R.; Shishkov, M.; Halpern, E.F.; Bouma, B.E. Quantification of macrophage content in atherosclerotic plaques by optical coherence tomography. Circulation 2003, 107, 113–119. [Google Scholar] [CrossRef]
- Tearney, G.J.; Regar, E.; Akasaka, T.; Adriaenssens, T.; Barlis, P.; Bezerra, H.G.; Bouma, B.; Bruining, N.; Cho, J.M.; Chowdhary, S.; et al. Consensus standards for acquisition, measurement, and reporting of intravascular optical coherence tomography studies: A report from the International Working Group for Intravascular Optical Coherence Tomography Standardization and Validation. J. Am. Coll. Cardiol. 2012, 59, 1058–1072. [Google Scholar] [CrossRef] [Green Version]
- Di Vito, L.; Agozzino, M.; Marco, V.; Ricciardi, A.; Concardi, M.; Romagnoli, E.; Gatto, L.; Calogero, G.; Tavazzi, L.; Arbustini, E.; et al. Identification and quantification of macrophage presence in coronary atherosclerotic plaques by optical coherence tomography. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Ramkhelawon, B.; Hennessy, E.J.; Menager, M.; Ray, T.D.; Sheedy, F.J.; Hutchison, S.; Wanschel, A.; Oldebeken, S.; Geoffrion, M.; Spiro, W.; et al. Netrin-1 promotes adipose tissue macrophage retention and insulin resistance in obesity. Nat. Med. 2014, 20, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yim, J.; Kim, G.; Lee, B.W.; Kang, E.S.; Cha, B.S.; Kim, J.H.; Cho, J.W.; Lee, S.G.; Lee, Y.H. Relationship Between Circulating Netrin-1 Concentration, Impaired Fasting Glucose, and Newly Diagnosed Type 2 Diabetes. Front. Endocrinol. 2018, 9, 691. [Google Scholar] [CrossRef]
- Liu, C.; Ke, X.; Wang, Y.; Feng, X.; Li, Q.; Zhang, Y.; Zhu, J. The level of netrin-1 is decreased in newly diagnosed type 2 diabetes mellitus patients. BMC Endocr. Disord. 2016, 16, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruikman, C.S.; Vreeken, D.; Hoogeveen, R.M.; Bom, M.J.; Danad, I.; Pinto-Sietsma, S.J.; van Zonneveld, A.J.; Knaapen, P.; Hovingh, G.K.; Stroes, E.S.G.; et al. Netrin-1 and the Grade of Atherosclerosis Are Inversely Correlated in Humans. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 462–472. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Cai, H. Netrin-1 prevents ischemia/reperfusion-induced myocardial infarction via a DCC/ERK1/2/eNOS s1177/NO/DCC feed-forward mechanism. J. Mol. Cell. Cardiol. 2010, 48, 1060–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, N.M.; Siu, K.L.; Youn, J.Y.; Cai, H. Attenuation of neointimal formation with netrin-1 and netrin-1 preconditioned endothelial progenitor cells. J. Mol. Med. (Berl.) 2017, 95, 335–348. [Google Scholar] [CrossRef]
- Khan, J.A.; Cao, M.; Kang, B.Y.; Liu, Y.; Mehta, J.L.; Hermonat, P.L. Systemic human Netrin-1 gene delivery by adeno-associated virus type 8 alters leukocyte accumulation and atherogenesis in vivo. Gene Ther. 2011, 18, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Bruikman, C.S.; Vreeken, D.; Zhang, H.; van Gils, M.J.; Peter, J.; van Zonneveld, A.J.; Hovingh, G.K.; van Gils, J.M. The identification and function of a Netrin-1 mutation in a pedigree with premature atherosclerosis. Atherosclerosis 2020, 301, 84–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadagavadi, R.K.; Wang, W.; Ramesh, G. Netrin-1 regulates Th1/Th2/Th17 cytokine production and inflammation through UNC5B receptor and protects kidney against ischemia-reperfusion injury. J. Immunol. 2010, 185, 3750–3758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.; Shim, D.; Lee, J.S.; Zaitsev, K.; Williams, J.W.; Kim, K.W.; Jang, M.Y.; Seok Jang, H.; Yun, T.J.; Lee, S.H.; et al. Transcriptome Analysis Reveals Nonfoamy Rather Than Foamy Plaque Macrophages Are Proinflammatory in Atherosclerotic Murine Models. Circ. Res. 2018, 123, 1127–1142. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Controls (n = 21) | CAD (n = 42) | p Value Controls vs. CAD | CAD | ||
|---|---|---|---|---|---|---|
| SA (n = 19) | AMI (n = 23) | ANOVA p Value | ||||
| Demographics | ||||||
| Age (years) | 44.24 ± 9.73 | 62.76 ± 11.03 | 0.0001 | 64.84 ± 8.64 * | 61.04 ± 12.60 * | 0.0001 |
| Male sex, n (%) | 8 (38.0) | 35 (83.3) | 0.0003 | 14 (73.7) | 21 (91.3) * | 0.0003 |
| Body mass index (kg/m2) | 24.50 ± 3.61 | 29.95 ± 4.3 | 0.0001 | 29.11.0 ± 3.6 * | 30.65 ± 4.88 * | 0.0001 |
| Clinical characteristics | ||||||
| Current smoking, n (%) | 3 (14.3) | 23 (54.8) | 0.0026 | 10 (52.6) | 13 (56.5) * | 0.007 |
| Diabetes mellitus, n (%) | 0 | 18 (42.8) | 0.0002 | 7 (36.8) | 11 (47.8) | 0.003 |
| Dyslipidemia, n (%) | 2 (9.5) | 21 (50.0) | 0.0019 | 10 (52.6) * | 11 (47.8) * | 0.004 |
| Hypertension, n (%) | 1 (4.8) | 21 (50.0) | 0.0003 | 10 (52.6) * | 11 (47.8) * | 0.0006 |
| Family history of CAD, n (%) | 3 (14.3) | 21 (50.0) | 0.0066 | 7 (36.8) | 14 (60.9) * | 0.006 |
| LVEF (%) | - | 53.5 (45; 57) | - | 55 (45; 57) | 49 (45; 57) | 0.4611 |
| Laboratory data | ||||||
| WBC (×109/L) | 6.4 (5.4; 6.6) | 8.3 (7.5;10) | 0.0001 | 8.4 (7.6; 11) * | 7.6 (7.1; 9.6) * | 0.0001 |
| RBC (×1012/L) | 4.7 (4.3; 5.2) | 4.5 (4.0; 5.2) | 0.161 | 4.3 (3.9; 4.7) | 4.7 (4; 5.2) | 0.068 |
| Neutrophil count (×109/L) | 3.61 (3.1; 4.23) | 5.1 (4.1; 6.8) | 0.0001 | 5 (4.2; 7.8) * | 5.1 (4, 6.8) * | 0.0001 |
| Lymphocyte count (×109/L) | 1.81 ± 0.54 | 2.22 ± 0.97 | 0.034 | 2.51 ± 0.95* | 1.98 ± 0.94 | 0.026 |
| Eosinophil count (×109/L) | 0.12 (0.09; 0.19) | 0.2 (0.1; 0.3) | 0.048 | 0.3 (0.1; 0.3) * | 0.2 (0.1; 0.3) | 0.051 |
| Monocyte count (×109/L) | 0.38 (0.31; 0.46) | 0.6 (0.5; 0.8) | 0.0001 | 0.6 (0.5; 0.7) * | 0.6 (0.5; 0.9) * | 0.0001 |
| Platelets (×109/L) | 236 (215; 271) | 212 (184;268) | 0.07 | 200 (154; 269) | 212 (192; 268) | 0.185 |
| hs-CRP (mg/L) | - | 2.65 (1.8; 16.9) | 2.1 (1; 2.2) | 13.6 (6; 21) ǂ | 0.0001 | |
| Creatinine (mg/dL) | 0.96 ± 0.48 | 0.98 ± 0.37 | 0.85 | 0.93 ± 0.29 | 1.02 ± 0.42 | 0.755 |
| Glycaemia (mg/dL) | 88.5 (84;98) | 134.5 (110; 171) | 0.0001 | 121 (104;140) * | 147 (121; 187) * ǂ | 0.0001 |
| Total cholesterol (mg/dL) | 200.71 ± 23.83 | 199.55 ± 46 | 0.89 | 186.0 ± 39.15 | 210.74 ± 48.98 | 0.132 |
| LDL (mg/dL) | 130.43 ± 23.35 | 119.05 ± 40.16 | 0.161 | 106.0 ± 29.75 | 129.83 ± 44.87 | 0.045 |
| HDL (mg/dL) | 54 (43; 59) | 45 (41; 58) | 0.24 | 48 (43; 61) | 43 (36; 48) | 0.054 |
| Triglycerides (mg/dL) | 87 (63; 129) | 169 (113; 190) | 0.0004 | 119 (82; 178) | 186 (147; 214) * | 0.0003 |
| Peak TnI (μg/dL) | - | 0.3 (0; 24.9) | 0 (0; 0) | 6 (1.3; 34.6) ǂ | 0.0001 | |
| Peak CK-MB (μg/dL) | - | 5 (1.9; 35.7) | 2 (1.5; 2.21) | 28 (12.3; 156.7) ǂ | 0.0001 | |
| Angiographic data | ||||||
| Culprit or treated vessel | ||||||
| LAD, n (%) | 0 | 32 (76.2) | 11 (57.9) | 21 (91.3) | ||
| LCX, n (%) | 0 | 2 (4.8) | 2 (10.5) | 0 (0) | ||
| RCA, n (%) | 0 | 8 (19.0) | 6 (31.6) | 2 (8.7) | ||
| Multivessel disease, n (%) | 0 | 27 (64.2) | 16 (84.2) | 11 (47.8) ǂ | 0.02 | |
| Admission therapy | ||||||
| ASA, n (%) | 0 | 15 (35.7) | 8 (42.1) | 7 (30.4) | 0.002 | |
| Beta-Blockers, n (%) | 0 | 14 (33.3) | 9 (47.3) | 5 (21.7) | 0.0006 | |
| ACE-inhibitors, n (%) | 0 | 15 (35.7) | 11 (57.9) | 4 (17.4) | 0.0001 | |
| Statins, n (%) | 0 | 15 (35.7) | 9 (47.4) | 6 (26.1) | 0.0009 | |
| Variables | SA (n = 19) | AMI (n = 23) | p Value |
|---|---|---|---|
| Lipid plaque, n (%) | 14 (73.6) | 18 (78.2) | 0. 73 |
| Fibrous plaque, n (%) | 3 (15.8) | 2 (8.7) | 0.64 |
| Calcific plaque, n (%) | 4 (21.1) | 4 (17.4) | 1.0 |
| Plaque rupture, n (%) | 7 (36.8%) | 18 (78.3) | 0.006 |
| Plaque erosion, n (%) | 8 (42.1) | 11 (47.8) | 0.71 |
| MLA, mm2 | 1.9 (1.7–3.6) | 1.7 (1.1–3.9) | 0.37 |
| TCFA, n (%) | 2 (10.5) | 12 (52.2) | 0.007 |
| Thrombus, n (%) | 1 (5.3) | 16 (69.6) | 0.0001 |
| Lipid quadrants, n | 2 (2–3) | 3 (2–3) | 0.06 |
| Lipid arc degree, ° | 1215 (87–265) | 260 (172–280) | 0.006 |
| Presence of microchannels, n (%) | 5 (26.3) | 13 (56.5) | 0.049 |
| Macrophage infiltration detection, n (%) | 10 (56.2) | 14 (60.9) | 0.59 |
| Macrophage NSD | 6.4 (5.29–6.49) | 6.5 (5.92–7.62) | 0.21 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiorelli, S.; Cosentino, N.; Porro, B.; Fabbiocchi, F.; Niccoli, G.; Fracassi, F.; Capra, N.; Barbieri, S.; Crea, F.; Marenzi, G.; et al. Netrin-1 in Atherosclerosis: Relationship between Human Macrophage Intracellular Levels and In Vivo Plaque Morphology. Biomedicines 2021, 9, 168. https://doi.org/10.3390/biomedicines9020168
Fiorelli S, Cosentino N, Porro B, Fabbiocchi F, Niccoli G, Fracassi F, Capra N, Barbieri S, Crea F, Marenzi G, et al. Netrin-1 in Atherosclerosis: Relationship between Human Macrophage Intracellular Levels and In Vivo Plaque Morphology. Biomedicines. 2021; 9(2):168. https://doi.org/10.3390/biomedicines9020168
Chicago/Turabian StyleFiorelli, Susanna, Nicola Cosentino, Benedetta Porro, Franco Fabbiocchi, Giampaolo Niccoli, Francesco Fracassi, Nicolò Capra, Simone Barbieri, Filippo Crea, Giancarlo Marenzi, and et al. 2021. "Netrin-1 in Atherosclerosis: Relationship between Human Macrophage Intracellular Levels and In Vivo Plaque Morphology" Biomedicines 9, no. 2: 168. https://doi.org/10.3390/biomedicines9020168