
Vasomotor Dysfunction in Patients with Ischemia and Non-Obstructive Coronary Artery Disease: Current Diagnostic and Therapeutic Strategies


Abstract
:1. Introduction
Search Methodology
- For the general description of microvascular disease, the following search syntax was used—coronary AND (“Microvascular angina” OR “syndrome X” OR “microvascular disease” OR “microvascular dysfunction”), and this yielded 3571 results;
- For different therapeutic/pharmacological approaches, the following search syntax was used—coronary AND (“Microvascular angina” OR “syndrome X” OR “microvascular disease” OR “microvascular dysfunction” OR “coronary flow reserve” OR “index of microvascular resistance *”) AND (therapy OR pharm *) AND prospective, and this yielded 353 results;
- For the prognosis/outcome, the following search syntax was used—(“Microvascular angina” OR “syndrome X” OR “microvascular disease” or “microvascular dysfunction”) AND (coronary) AND (“follow-up” OR hospitalization OR MACE OR death OR intervention OR “major adverse events” OR Follow * OR Predictor * OR Outcome * OR “myocardial infarction *” OR stroke * OR “heart attack *” OR hospitalization* OR “heart failure”), and this yielded 2866 results, which were already included in the results yielded by the first syntax.
2. Pathophysiology and Endotypes
2.1. Coronary Microvascular Dysfunction (CMD)/Microvascular Angina (MVA)
2.2. Epicardial Vasospastic Angina (VSA)
3. Risk Factors
3.1. CMD
3.2. Vasospastic Angina
4. Symptoms
5. Diagnostic Approaches
5.1. Non-Invasive Diagnosis
5.1.1. Transthoracic Echocardiography (TTE)
5.1.2. Positron Emission Tomography (PET)
5.1.3. Cardiac Magnetic Resonance (CMR)
5.2. Invasive Diagnosis
5.2.1. Patient Preparation
5.2.2. Assessment of Endothelial-Independent Microvascular Function
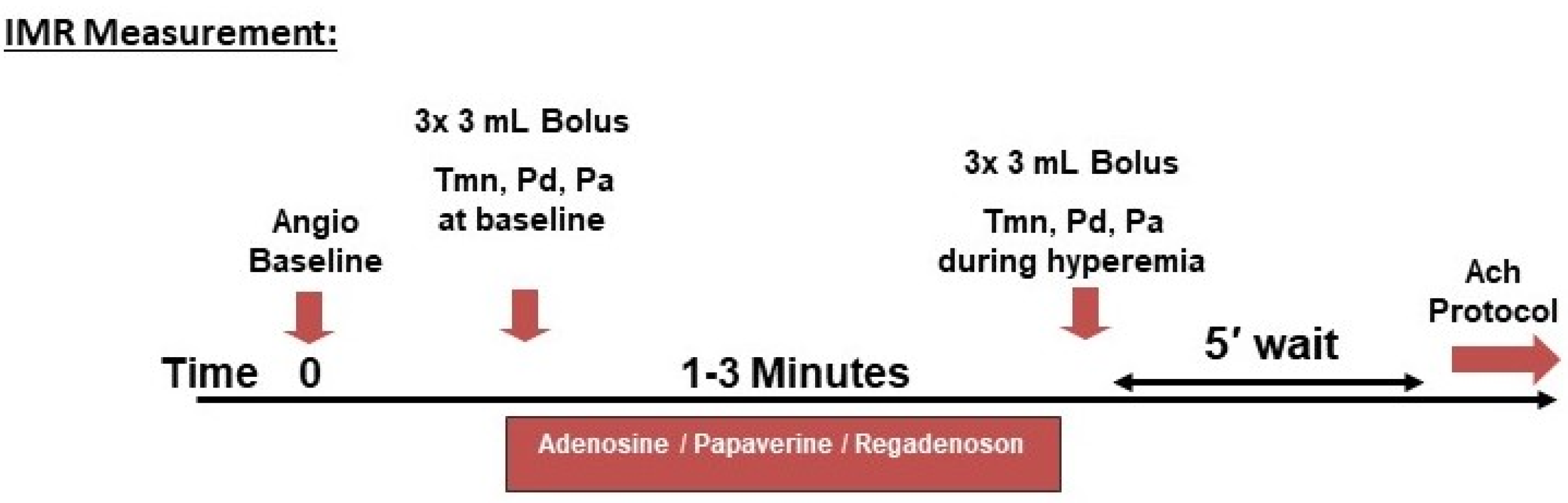
Thermodilution Technique
Doppler-Based Technique
Continuous Thermodilution Method
Cut-Off Values
5.2.3. Assessment of Endothelium-Dependent Microvascular and Macrovascular Function (Provocation Testing for Coronary Vasospasm)
5.2.4. Safety
5.2.5. Interpretation
6. Therapeutic Approaches and Strategies
6.1. Pharmacotherapy
6.1.1. First Line (Conventional) Drugs
Microvascular Angina
Vasospastic Angina
6.1.2. Second-Line Drugs
Nicorandil
Ranolazine
Ivabradine
Trimetazidine
Xanthines
6.1.3. Novel and Experimental Pharmacotherapies
6.2. Non-Pharmacologic/Interventional Therapies for Refractory Cases
7. Prognosis
8. Knowledge Gaps and Limitations
9. Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patel, M.R.; Peterson, E.D.; Dai, D.; Brennan, J.M.; Redberg, R.F.; Anderson, H.V.; Brindis, R.G.; Douglas, P.S. Low Diagnostic Yield of Elective Coronary Angiography. N. Engl. J. Med. 2010, 362, 886–895. [Google Scholar] [CrossRef] [Green Version]
- Jespersen, L.; Hvelplund, A.; Abildstrøm, S.Z.; Pedersen, F.; Galatius, S.; Madsen, J.K.; Jørgensen, E.; Kelbaek, H.; Prescott, E. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur. Heart J. 2012, 33, 734–744. [Google Scholar] [CrossRef] [PubMed]
- Asbury, E.A.; Collins, P. Cardiac syndrome X. Int. J. Clin. Pract. 2005, 59, 1063–1069. [Google Scholar] [CrossRef] [PubMed]
- Rahman, H.; Corcoran, D.; Aetesam-Ur-Rahman, M.; Hoole, S.P.; Berry, C.; Perera, D. Diagnosis of patients with angina and non-obstructive coronary disease in the catheter laboratory. Heart 2019, 105, 1536–1542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, B.-K.; Lim, H.-S.; Fearon, W.F.; Yong, A.; Yamada, R.; Tanaka, S.; Lee, D.P.; Yeung, A.C.; Tremmel, J.A. Invasive Evaluation of Patients with Angina in the Absence of Obstructive Coronary Artery Disease. Circulation 2015, 131, 1054–1060. [Google Scholar] [CrossRef] [Green Version]
- Bairey Merz, C.N.; Pepine, C.J.; Walsh, M.N.; Fleg, J.L. Ischemia and No Obstructive Coronary Artery Disease (INOCA): Developing Evidence-Based Therapies and Research Agenda for the Next Decade. Circulation 2017, 135, 1075–1092. [Google Scholar] [CrossRef]
- Britten, M.B.; Zeiher, A.M.; Schächinger, V. Microvascular dysfunction in angiographically normal or mildly diseased coronary arteries predicts adverse cardiovascular long-term outcome. Coron. Artery Dis. 2004, 15, 259–264. [Google Scholar] [CrossRef]
- Jespersen, L.; Abildstrøm, S.Z.; Hvelplund, A.; Prescott, E. Persistent angina: Highly prevalent and associated with long-term anxiety, depression, low physical functioning, and quality of life in stable angina pectoris. Clin. Res. Cardiol. 2013, 102, 571–581. [Google Scholar] [CrossRef]
- Piegza, M.; Wierzba, D.; Piegza, J. Cardiac syndrome X—the present knowledge. Psychiatr. Polska 2021, 55, 363–375. [Google Scholar] [CrossRef]
- Pepine, C.J.; Anderson, R.D.; Sharaf, B.L.; Reis, S.E.; Smith, K.M.; Handberg, E.M.; Johnson, B.D.; Sopko, G.; Bairey Merz, C.N. Coronary microvascular reactivity to adenosine predicts adverse outcome in women evaluated for suspected ischemia results from the National Heart, Lung and Blood Institute WISE (Women’s Ischemia Syndrome Evaluation) study. J. Am. Coll. Cardiol. 2010, 55, 2825–2832. [Google Scholar] [CrossRef] [Green Version]
- Radico, F.; Zimarino, M.; Fulgenzi, F.; Ricci, F.; Di Nicola, M.; Jespersen, L.; Chang, S.M.; Humphries, K.H.; Marzilli, M.; De Caterina, R. Determinants of long-term clinical outcomes in patients with angina but without obstructive coronary artery disease: A systematic review and meta-analysis. Eur. Heart J. 2018, 39, 2135–2146. [Google Scholar] [CrossRef] [PubMed]
- Kunadian, V.; Chieffo, A.; Camici, P.G.; Berry, C.; Escaned, J.; Maas, A.; Prescott, E.; Karam, N.; Appelman, Y.; Fraccaro, C.; et al. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation Endorsed by Coronary Vasomotor Disorders International Study Group. EuroIntervention 2021, 16, 1049–1069. [Google Scholar] [PubMed]
- Pries, A.R.; Badimon, L.; Bugiardini, R.; Camici, P.G.; Dorobantu, M.; Duncker, D.J.; Escaned, J.; Koller, A.; Piek, J.J.; de Wit, C. Coronary vascular regulation, remodelling, and collateralization: Mechanisms and clinical implications on behalf of the working group on coronary pathophysiology and microcirculation. Eur. Heart J. 2015, 36, 3134–3146. [Google Scholar] [CrossRef] [Green Version]
- Fineschi, M.; Gori, T. Coronary slow flow: Description of a new “cardiac Y” syndrome. Int. J. Cardiol. 2009, 137, 308–310. [Google Scholar] [CrossRef] [PubMed]
- Mejía-Rentería, H.; Van Der Hoeven, N.; Van De Hoef, T.P.; Heemelaar, J.; Ryan, N.; Lerman, A.; Van Royen, N.; Escaned, J. Targeting the dominant mechanism of coronary microvascular dysfunction with intracoronary physiology tests. Int. J. Cardiovasc. Imaging 2017, 33, 1041–1059. [Google Scholar] [CrossRef] [PubMed]
- Sambuceti, G.; Marzilli, M.; Marraccini, P.; Schneider-Eicke, J.; Gliozheni, E.; Parodi, O.; L’Abbate, A. Coronary vasoconstriction during myocardial ischemia induced by rises in metabolic demand in patients with coronary artery disease. Circulation 1997, 95, 2652–2659. [Google Scholar] [CrossRef]
- Prinzmetal, M.; Kennamer, R.; Merliss, R.; Wada, T.; Bor, N. Angina pectoris. I. A variant form of angina pectoris; preliminary report. Am. J. Med. 1959, 27, 375–388. [Google Scholar] [CrossRef]
- Lanza, G.A.; Careri, G.; Crea, F. Mechanisms of Coronary Artery Spasm. Circulation 2011, 124, 1774–1782. [Google Scholar] [CrossRef] [Green Version]
- Jansen, T.P.J.; Elias-Smale, S.E.; Oord, S.V.D.; Gehlmann, H.; Dimitiriu-Leen, A.; Maas, A.H.E.M.; Konst, R.E.; van Royen, N.; Damman, P. Sex Differences in Coronary Function Test Results in Patient with Angina and Nonobstructive Disease. Front. Cardiovasc. Med. 2021, 8, 1379. [Google Scholar] [CrossRef]
- Wessel, T.R.; Arant, C.B.; McGorray, S.P.; Sharaf, B.L.; Reis, S.E.; Kerensky, R.A.; von Mering, G.O.; Smith, K.M.; Pauly, D.F.; Handberg, E.M.; et al. Coronary microvascular reactivity is only partially predicted by atherosclerosis risk factors or coronary artery disease in women evaluated for suspected ischemia: Results from the NHLBI Women’s Ischemia Syndrome Evaluation (WISE). Clin. Cardiol. 2007, 30, 69–74. [Google Scholar] [CrossRef]
- Sara, J.D.; Widmer, R.J.; Matsuzawa, Y.; Lennon, R.J.; Lerman, L.O.; Lerman, A. Prevalence of Coronary Microvascular Dysfunction Among Patients with Chest Pain and Nonobstructive Coronary Artery Disease. JACC Cardiovasc. Interv. 2015, 8, 1445–1453. [Google Scholar] [CrossRef] [PubMed]
- Mygind, N.D.; Michelsen, M.M.; Pena, A.; Frestad, D.; Dose, N.; Aziz, A.; Faber, R.; Høst, N.; Gustafsson, I.; Hansen, P.R.; et al. Coronary Microvascular Function and Cardiovascular Risk Factors in Women with Angina Pectoris and No Obstructive Coronary Artery Disease: The iPOWER Study. J. Am. Heart Assoc. 2016, 5, e003064. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.D.; Moccetti, F.; Brown, E.; Davidson, B.P.; Atkinson, T.; Belcik, J.T.; Giraud, G.; Duell, P.B.; Fazio, S.; Tavori, H.; et al. Lipoprotein Apheresis Acutely Reverses Coronary Microvascular Dysfunction in Patients with Severe Hypercholesterolemia. JACC Cardiovasc. Imaging 2019, 12, 1430–1440. [Google Scholar] [CrossRef]
- Wang, R.; Li, X.; Huangfu, S.; Yao, Q.; Wu, P.; Wu, Z.; Li, L.; Wang, Y.; Yang, M.; Hacker, M.; et al. Combining body mass index with waist circumference to assess coronary microvascular function in patients with non-obstructive coronary artery disease. J. Nucl. Cardiol. 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Rosas, E.A.; González, A.M.; Castillo, L.G.-R.; Valero, M.R.; Molina, P.A.L.; Petra, J.A.T.; Fernández, C.S.; García-Villa, P.C.; Zanella, H.G.R.; Pérez, M.B.; et al. [Endothelial function assessment by positron emission tomography in patients with hypercholesterolemia]. Arch. Cardiol. Mex. 2008, 78, 139–147. [Google Scholar]
- Zeiher, A.M.; Schächinger, V.; Minners, J. Long-term Cigarette Smoking Impairs Endothelium-Dependent Coronary Arterial Vasodilator Function. Circulation 1995, 92, 1094–1100. [Google Scholar] [CrossRef]
- Ishimori, M.L.; Martin, R.; Berman, D.S.; Goykhman, P.; Shaw, L.J.; Shufelt, C.; Slomka, P.J.; Thomson, L.E.; Schapira, J.; Yang, Y.; et al. Myocardial Ischemia in the Absence of Obstructive Coronary Artery Disease in Systemic Lupus Erythematosus. JACC Cardiovasc. Imaging 2011, 4, 27–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Recio-Mayoral, A.; Mason, J.; Kaski, J.C.; Rubens, M.B.; Harari, O.A.; Camici, P.G. Chronic inflammation and coronary microvascular dysfunction in patients without risk factors for coronary artery disease. Eur. Heart J. 2009, 30, 1837–1843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piaserico, S.; Osto, E.; Famoso, G.; Montisci, R.; De Michieli, L.; Zanetti, I.; Iliceto, S.; Tona, F. Long-term prognostic value of coronary flow reserve in psoriasis patients. Atherosclerosis 2019, 289, 57–63. [Google Scholar] [CrossRef]
- Kakuta, K.; Dohi, K.; Yamamoto, T.; Fujimoto, N.; Shimoyama, T.; Umegae, S.; Ito, M. Coronary Microvascular Dysfunction Restored After Surgery in Inflammatory Bowel Disease: A Prospective Observational Study. J. Am. Heart Assoc. 2021, 10, e019125. [Google Scholar] [CrossRef]
- Beltrame, J.F.; Sasayama, S.; Maseri, A. Racial heterogeneity in coronary artery vasomotor reactivity: Differences between Japanese and caucasian patients. J. Am. Coll. Cardiol. 1999, 33, 1442–1452. [Google Scholar] [CrossRef]
- Hung, M.-J.; Hsu, K.-H.; Cheng, C.-W.; Cherng, W.-J. Interactions among gender, age, hypertension and C-reactive protein in coronary vasospasm. Eur. J. Clin. Investig. 2010, 40, 1094–1103. [Google Scholar] [CrossRef] [PubMed]
- Nobuyoshi, M.; Abe, M.; Nosaka, H.; Kimura, T.; Yokoi, H.; Hamasaki, N.; Shindo, T.; Kimura, K.; Nakamura, T.; Nakagawa, Y.; et al. Statistical analysis of clinical risk factors for coronary artery spasm: Identification of the most important determinant. Am. Heart J. 1992, 124, 32–38. [Google Scholar] [CrossRef]
- Konst, R.E.; Meeder, J.G.; Wittekoek, M.E.; Maas, A.H.E.M.; Appelman, Y.; Piek, J.J.; Van De Hoef, T.P.; Damman, P.; Elias-Smale, S.E. Ischaemia with no obstructive coronary arteries. Neth. Heart J. 2020, 28, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Figueras, J.; Domingo, E.; Ferreira, I.; Lidon, R.M.; Bellera, N.; Garcia-Dorado, D. Typical angina without significant coronary stenosis: Comparison of clinical profile, circadian presentation, and long-term follow-up between patients with and patients without vasospastic angina. Coron. Artery Dis. 2013, 24, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Ong, P.; Camici, P.G.; Beltrame, J.F.; Crea, F.; Shimokawa, H.; Sechtem, U.; Kaski, J.C.; Merz, C.N.B. International standardization of diagnostic criteria for microvascular angina. Int. J. Cardiol. 2018, 250, 16–20. [Google Scholar] [CrossRef]
- Beltrame, J.F.; Crea, F.; Kaski, J.C.; Ogawa, H.; Ong, P.; Sechtem, U.; Shimokawa, H.; Merz, C.N.B. International standardization of diagnostic criteria for vasospastic angina. Eur. Heart J. 2017, 38, 2565–2568. [Google Scholar] [CrossRef] [Green Version]
- Albadri, A.; Wei, J.; Mehta, P.K.; Landes, S.; Petersen, J.; Anderson, R.D.; Samuels, B.; Azarbal, B.; Handberg, E.M.; Li, Q.; et al. Acetylcholine versus cold pressor testing for evaluation of coronary endothelial function. PLoS ONE 2017, 12, e0172538. [Google Scholar] [CrossRef]
- Cassar, A.; Chareonthaitawee, P.; Rihal, C.S.; Prasad, A.; Lennon, R.J.; Lerman, L.O.; Lerman, A. Lack of Correlation Between Noninvasive Stress Tests and Invasive Coronary Vasomotor Dysfunction in Patients with Nonobstructive Coronary Artery Disease. Circ. Cardiovasc. Interv. 2009, 2, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Vegsundvåg, J.; Holte, E.; Wiseth, R.; Hegbom, K.; Hole, T. Coronary Flow Velocity Reserve in the Three Main Coronary Arteries Assessed with Transthoracic Doppler: A Comparative Study with Quantitative Coronary Angiography. J. Am. Soc. Echocardiogr. 2011, 24, 758–767. [Google Scholar] [CrossRef]
- Zeiher, A.M.; Drexler, H.; Wollschlaeger, H.; Saurbier, B.; Just, H. Coronary vasomotion in response to sympathetic stimulation in humans: Importance of the functional integrity of the endothelium. J. Am. Coll. Cardiol. 1989, 14, 1181–1190. [Google Scholar] [CrossRef] [Green Version]
- Cortigiani, L.; Rigo, F.; Gherardi, S.; Sicari, R.; Galderisi, M.; Bovenzi, F.; Picano, E. Additional Prognostic Value of Coronary Flow Reserve in Diabetic and Nondiabetic Patients with Negative Dipyridamole Stress Echocardiography by Wall Motion Criteria. J. Am. Coll. Cardiol. 2007, 50, 1354–1361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortigiani, L.; Rigo, F.; Gherardi, S.; Bovenzi, F.; Molinaro, S.; Picano, E.; Sicari, R. Coronary Flow Reserve During Dipyridamole Stress Echocardiography Predicts Mortality. JACC Cardiovasc. Imaging 2012, 5, 1079–1085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortigiani, L.; Rigo, F.; Bovenzi, F.; Sicari, R.; Picano, E. The Prognostic Value of Coronary Flow Velocity Reserve in Two Coronary Arteries During Vasodilator Stress Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 81–91. [Google Scholar] [CrossRef]
- Sicari, R.; Rigo, F.; Gherardi, S.; Galderisi, M.; Cortigiani, L.; Picano, E. The prognostic value of Doppler echocardiographic-derived coronary flow reserve is not affected by concomitant antiischemic therapy at the time of testing. Am. Heart J. 2008, 156, 573–579. [Google Scholar] [CrossRef] [Green Version]
- Pelletier-Galarneau, M.; Dilsizian, V. Microvascular Angina Diagnosed by Absolute PET Myocardial Blood Flow Quantification. Curr. Cardiol. Rep. 2020, 22, 9. [Google Scholar] [CrossRef]
- Bol, A.; Melin, J.; Vanoverschelde, J.L.; Baudhuin, T.; Vogelaers, D.; De Pauw, M.; Michel, C.; Luxen, A.; Labar, D.; Cogneau, M. Direct comparison of [13N]ammonia and [15O]water estimates of perfusion with quantification of regional myocardial blood flow by microspheres. Circulation 1993, 87, 512–525. [Google Scholar] [CrossRef] [Green Version]
- Feher, A.; Sinusas, A.J. Quantitative Assessment of Coronary Microvascular Function: Dynamic Single-Photon Emission Computed Tomography, Positron Emission Tomography, Ultrasound, Computed Tomography, and Magnetic Resonance Imaging. Circ. Cardiovasc. Imaging 2017, 10, e006427. [Google Scholar] [CrossRef] [Green Version]
- Gould, K.L.; Johnson, N.P.; Bateman, T.M.; Beanlands, R.S.; Bengel, F.M.; Bober, R.; Camici, P.G.; Cerqueira, M.D.; Chow, B.J.W.; Di Carli, M.F.; et al. Anatomic versus physiologic assessment of coronary artery disease. Role of coronary flow reserve, fractional flow reserve, and positron emission tomography imaging in revascularization decision-making. J. Am. Coll. Cardiol. 2013, 62, 1639–1653. [Google Scholar] [CrossRef] [Green Version]
- Dilsizian, V.; Bacharach, S.L.; Beanlands, R.S.; Bergmann, S.R.; Delbeke, D.; Dorbala, S.; Gropler, R.J.; Knuuti, J.; Schelbert, H.R.; Travin, M.I. ASNC imaging guidelines/SNMMI procedure standard for positron emission tomography (PET) nuclear cardiology procedures. J. Nucl. Cardiol. 2016, 23, 1187–1226. [Google Scholar] [CrossRef] [Green Version]
- Vancheri, F.; Longo, G.; Vancheri, S.; Henein, M. Coronary Microvascular Dysfunction. J. Clin. Med. 2020, 9, 2880. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.A.E.; Onciul, S.C.; Broadbent, D.A.; Johnson, K.; Fent, G.J.; Foley, J.R.J.; Garg, P.; Chew, P.G.; Knott, K.; Dall’Armellina, E.; et al. Fully automated, inline quantification of myocardial blood flow with cardiovascular magnetic resonance: Repeatability of measurements in healthy subjects. J. Cardiovasc. Magn. Reson. 2018, 20, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biglands, J.D.; Magee, D.R.; Sourbron, S.P.; Plein, S.; Greenwood, J.P.; Radjenovic, A. Comparison of the Diagnostic Performance of Four Quantitative Myocardial Perfusion Estimation Methods Used in Cardiac MR Imaging: CE-MARC Substudy. Radiology 2015, 275, 393–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Indorkar, R.; Kwong, R.Y.; Romano, S.; White, B.E.; Chia, R.C.; Trybula, M.; Evans, K.; Shenoy, C.; Farzaneh-Far, A. Global Coronary Flow Reserve Measured During Stress Cardiac Magnetic Resonance Imaging Is an Independent Predictor of Adverse Cardiovascular Events. JACC Cardiovasc. Imaging 2019, 12, 1686–1695. [Google Scholar] [CrossRef]
- Kellman, P.; Hansen, M.S.; Nielles-Vallespin, S.; Nickander, J.; Themudo, R.; Ugander, M.; Xue, H. Myocardial perfusion cardiovascular magnetic resonance: Optimized dual sequence and reconstruction for quantification. J. Cardiovasc. Magn. Reson. 2017, 19, 42. [Google Scholar] [CrossRef] [Green Version]
- Engblom, H.; Xue, H.; Akil, S.; Carlsson, M.; Hindorf, C.; Oddstig, J.; Hedeer, F.; Hansen, M.S.; Aletras, A.H.; Kellman, P.; et al. Fully quantitative cardiovascular magnetic resonance myocardial perfusion ready for clinical use: A comparison between cardiovascular magnetic resonance imaging and positron emission tomography. J. Cardiovasc. Magn. Reson. 2017, 19, 78. [Google Scholar] [CrossRef] [Green Version]
- Kotecha, T.; Martinez-Naharro, A.; Boldrini, M.; Knight, D.; Hawkins, P.; Kalra, S.; Patel, D.; Coghlan, G.; Moon, J.; Plein, S.; et al. Automated Pixel-Wise Quantitative Myocardial Perfusion Mapping by CMR to Detect Obstructive Coronary Artery Disease and Coronary Microvascular Dysfunction: Validation Against Invasive Coronary Physiology. JACC Cardiovasc. Imaging 2019, 12, 1958–1969. [Google Scholar] [CrossRef]
- Fuetterer, M.; Busch, J.; Traechtler, J.; Wespi, P.; Peereboom, S.M.; Sauer, M.; Lipiski, M.; Fleischmann, T.; Cesarovic, N.; Stoeck, C.T.; et al. Quantitative myocardial first-pass cardiovascular magnetic resonance perfusion imaging using hyperpolarized [1-13C] pyruvate. J. Cardiovasc. Magn. Reson. 2018, 20, 73. [Google Scholar] [CrossRef]
- Groepenhoff, F.; Klaassen, R.G.M.; Valstar, G.B.; Bots, S.H.; Onland-Moret, N.C.; Ruijter, H.M.D.; Leiner, T.; Eikendal, A.L.M. Evaluation of non-invasive imaging parameters in coronary microvascular disease: A systematic review. BMC Med. Imaging 2021, 21, 5. [Google Scholar] [CrossRef]
- Xaplanteris, P.; Fournier, S.; Keulards, D.C.; Adjedj, J.; Ciccarelli, G.; Milkas, A.; Pellicano, M.; Veer, M.v.; Barbato, E.; Pijls, N.H.J.; et al. Catheter-Based Measurements of Absolute Coronary Blood Flow and Microvascular Resistance: Feasibility, Safety, and Reproducibility in Humans. Circ. Cardiovasc. Interv. 2018, 11, e006194. [Google Scholar] [CrossRef]
- Kodeboina, M.; Nagumo, S.; Munhoz, D.; Sonck, J.; Mileva, N.; Gallinoro, E.; Candreva, A.; Mizukami, T.; Van Durme, F.; Heyse, A.; et al. Simplified Assessment of the Index of Microvascular Resistance. J. Interv. Cardiol. 2021, 2021, 9971874. [Google Scholar] [CrossRef]
- Konst, R.E.; Damman, P.; Pellegrini, D.; van Royen, N.; Maas, A.H.E.M.; Elias-Smale, S.E. Diagnostic approach in patients with angina and no obstructive coronary artery disease: Emphasising the role of the coronary function test. Neth. Heart J. 2021, 29, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Fearon, W.F.; Honda, Y.; Tanaka, S.; Pargaonkar, V.; Fitzgerald, P.J.; Lee, D.P.; Stefanick, M.; Yeung, A.C.; Tremmel, J.A. Effect of Sex Differences on Invasive Measures of Coronary Microvascular Dysfunction in Patients with Angina in the Absence of Obstructive Coronary Artery Disease. JACC Cardiovasc. Interv. 2015, 8, 1433–1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez-Barrios, A.; Izaga-Torralba, E.; Crespo, F.R.; Gheorghe, L.; Cañadas-Pruaño, D.; Gómez-Lara, J.; Silva, E.; Noval-Morillas, I.; Rueda, R.Z.; Calle-Pérez, G.; et al. Continuous Thermodilution Method to Assess Coronary Flow Reserve. Am. J. Cardiol. 2021, 141, 31–37. [Google Scholar] [CrossRef]
- Lee, J.M.; Jung, J.-H.; Hwang, D.; Park, J.; Fan, Y.; Na, S.-H.; Doh, J.-H.; Nam, C.-W.; Shin, E.-S.; Koo, B.-K. Coronary Flow Reserve and Microcirculatory Resistance in Patients with Intermediate Coronary Stenosis. J. Am. Coll. Cardiol. 2016, 67, 1158–1169. [Google Scholar] [CrossRef]
- Usui, E.; Murai, T.; Kanaji, Y.; Hoshino, M.; Yamaguchi, M.; Hada, M.; Hamaya, R.; Kanno, Y.; Lee, T.; Yonetsu, T.; et al. Clinical significance of concordance or discordance between fractional flow reserve and coronary flow reserve for coronary physiological indices, microvascular resistance, and prognosis after elective percutaneous coronary intervention. EuroIntervention 2018, 14, 798–805. [Google Scholar] [CrossRef] [PubMed]
- Albadri, A.; Merz, C.N.B.; Johnson, B.D.; Wei, J.; Mehta, P.K.; Cook-Wiens, G.; Reis, S.E.; Kelsey, S.F.; Bittner, V.; Sopko, G.; et al. Impact of Abnormal Coronary Reactivity on Long-Term Clinical Outcomes in Women. J. Am. Coll. Cardiol. 2019, 73, 684–693. [Google Scholar] [CrossRef]
- van de Hoef, T.P.; van Lavieren, M.A.; Damman, P.; Delewi, R.; Piek, M.A.; Chamuleau, S.A.; Voskuil, M.; Henriques, J.P.S.; Koch, K.T.; de Winter, R.J.; et al. Physiological basis and long-term clinical outcome of discordance between fractional flow reserve and coronary flow velocity reserve in coronary stenoses of intermediate severity. Circ. Cardiovasc. Interv. 2014, 7, 301–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serruys, P.W.; Di Mario, C.; Piek, J.; Schroeder, E.; Vrints, C.; Probst, P.; de Bruyne, B.; Hanet, C.; Fleck, E.; Haude, M.; et al. Prognostic value of intracoronary flow velocity and diameter stenosis in assessing the short- and long-term outcomes of coronary balloon angioplasty: The DEBATE Study (Doppler Endpoints Balloon Angioplasty Trial Europe). Circulation 1997, 96, 3369–3377. [Google Scholar] [CrossRef]
- Fearon, W.F.; Kobayashi, Y. Invasive Assessment of the Coronary Microvasculature: The Index of Microcirculatory Resistance. Circ. Cardiovasc. Interv. 2017, 10, e005361. [Google Scholar] [CrossRef]
- Sheikh, A.R.; Zeitz, C.J.; Rajendran, S.; Di Fiore, D.P.; Tavella, R.; Beltrame, J.F. Clinical and coronary haemodynamic determinants of recurrent chest pain in patients without obstructive coronary artery disease—A pilot study. Int. J. Cardiol. 2018, 267, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Nolte, F.; Van De Hoef, T.P.; Meuwissen, M.; Voskuil, M.; Chamuleau, S.A.; Henriques, J.P.; Verberne, H.J.; Van Eck-Smit, B.L.; Koch, K.T.; De Winter, R.J.; et al. Increased hyperaemic coronary microvascular resistance adds to the presence of myocardial ischaemia. EuroIntervention 2014, 9, 1423–1431. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.P.; de Waard, G.A.; De Silva, K.; Lumley, M.; Asrress, K.; Arri, S.; Ellis, H.; Mir, A.; Clapp, B.; Chiribiri, A.; et al. Doppler Versus Thermodilution-Derived Coronary Microvascular Resistance to Predict Coronary Microvascular Dysfunction in Patients with Acute Myocardial Infarction or Stable Angina Pectoris. Am. J. Cardiol. 2018, 121, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picchi, A.; Limbruno, U.; Focardi, M.; Cortese, B.; Micheli, A.; Boschi, L.; Severi, S.; De Caterina, R. Increased basal coronary blood flow as a cause of reduced coronary flow reserve in diabetic patients. Am. J. Physiol. Circ. Physiol. 2011, 301, H2279–H2284. [Google Scholar] [CrossRef] [Green Version]
- Widmer, R.J.; Samuels, B.; Samady, H.; Price, M.J.; Jeremias, A.; Anderson, R.D.; Jaffer, F.A.; Escaned, J.; Davies, J.; Prasad, M.; et al. The functional assessment of patients with non-obstructive coronary artery disease: Expert review from an international microcirculation working group. EuroIntervention 2019, 14, 1694–1702. [Google Scholar] [CrossRef]
- Wei, J.; Mehta, P.K.; Johnson, B.D.; Samuels, B.; Kar, S.; Anderson, R.D.; Azarbal, B.; Petersen, J.; Sharaf, B.; Handberg, E.; et al. Safety of coronary reactivity testing in women with no obstructive coronary artery disease: Results from the NHLBI-sponsored WISE (Women’s Ischemia Syndrome Evaluation) study. JACC Cardiovasc. Interv. 2012, 5, 646–653. [Google Scholar] [CrossRef] [Green Version]
- Ong, P.; Athanasiadis, A.; Borgulya, G.; Vokshi, I.; Bastiaenen, R.; Kubik, S.; Hill, S.; Schäufele, T.; Mahrholdt, H.; Kaski, J.C.; et al. Clinical Usefulness, Angiographic Characteristics, and Safety Evaluation of Intracoronary Acetylcholine Provocation Testing Among 921 Consecutive White Patients with Unobstructed Coronary Arteries. Circulation 2014, 129, 1723–1730. [Google Scholar] [CrossRef] [Green Version]
- Ford, T.J.; Stanley, B.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; Robertson, K.; et al. Stratified Medical Therapy Using Invasive Coronary Function Testing in Angina: The CorMicA Trial. J. Am. Coll. Cardiol. 2018, 72 Pt A, 2841–2855. [Google Scholar] [CrossRef]
- Ford, T.J.; Stanley, B.; Sidik, N.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; et al. 1-Year Outcomes of Angina Management Guided by Invasive Coronary Function Testing (CorMicA). JACC Cardiovasc. Interv. 2020, 13, 33–45. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- Ohba, K.; Sugiyama, S.; Sumida, H.; Nozaki, T.; Matsubara, J.; Matsuzawa, Y.; Konishi, M.; Akiyama, E.; Kurokawa, H.; Maeda, H.; et al. Microvascular Coronary Artery Spasm Presents Distinctive Clinical Features with Endothelial Dysfunction as Nonobstructive Coronary Artery Disease. J. Am. Heart Assoc. 2012, 1, e002485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- JCS Joint Working Group. Guidelines for diagnosis and treatment of patients with vasospastic angina (Coronary Spastic Angina) (JCS 2013). Circ. J. 2014, 78, 2779–2801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antzelevitch, C.; Belardinelli, L.; Zygmunt, A.C.; Burashnikov, A.; Di Diego, J.M.; Fish, J.M.; Cordeiro, J.; Thomas, G. Electrophysiological Effects of Ranolazine, a Novel Antianginal Agent with Antiarrhythmic Properties. Circulation 2004, 110, 904–910. [Google Scholar] [CrossRef] [PubMed]
- Fraser, H.; Belardinelli, L.; Wang, L.; Light, P.E.; McVeigh, J.J.; Clanachan, A.S. Ranolazine decreases diastolic calcium accumulation caused by ATX-II or ischemia in rat hearts. J. Mol. Cell. Cardiol. 2006, 41, 1031–1038. [Google Scholar] [CrossRef]
- Venkataraman, R.; Belardinelli, L.; Blackburn, B.; Heo, J.; Iskandrian, A.E. A Study of the Effects of Ranolazine Using Automated Quantitative Analysis of Serial Myocardial Perfusion Images. JACC Cardiovasc. Imaging 2009, 2, 1301–1309. [Google Scholar] [CrossRef] [Green Version]
- Aldakkak, M.; Camara, A.K.; Heisner, J.S.; Yang, M.; Stowe, D.F. Ranolazine reduces Ca2+ overload and oxidative stress and improves mitochondrial integrity to protect against ischemia reperfusion injury in isolated hearts. Pharmacol. Res. 2011, 64, 381–392. [Google Scholar] [CrossRef] [Green Version]
- Deshmukh, S.H.; Patel, S.R.; Pinassi, E.; Mindrescu, C.; Hermance, E.V.; Infantino, M.N.; Coppola, J.T.; Staniloae, C.S. Ranolazine improves endothelial function in patients with stable coronary artery disease. Coron. Artery Dis. 2009, 20, 343–347. [Google Scholar] [CrossRef]
- Borer, J.S.; Fox, K.; Jaillon, P.; Lerebours, G. Antianginal and antiischemic effects of ivabradine, an I(f) inhibitor, in stable angina: A randomized, double-blind, multicentered, placebo-controlled trial. Circulation 2003, 107, 817–823. [Google Scholar] [CrossRef] [Green Version]
- Villano, A.; Di Franco, A.; Nerla, R.; Sestito, A.; Tarzia, P.; Lamendola, P.; Di Monaco, A.; Sarullo, F.M.; Lanza, G.A.; Crea, F. Effects of Ivabradine and Ranolazine in Patients with Microvascular Angina Pectoris. Am. J. Cardiol. 2013, 112, 8–13. [Google Scholar] [CrossRef]
- Skalidis, E.I.; Hamilos, M.I.; Chlouverakis, G.; Zacharis, E.A.; Vardas, P.E. Ivabradine improves coronary flow reserve in patients with stable coronary artery disease. Atherosclerosis 2011, 215, 160–165. [Google Scholar] [CrossRef]
- Nalbantgil, S.; Altinti gbreve Yilmaz, H.; Nalbantgil, I.I.; Onder, R. The Effect of Trimetazidine in the Treatment of Microvascular Angina. Int. J. Angiol. 1999, 8, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Rogacka, D.; Guzik, P.; Wykrętowicz, A.; Rzeźniczak, J.; Dziarmaga, M.; Wysocki, H. Effects of trimetazidine on clinical symptoms and tolerance of exercise of patients with syndrome X: A preliminary study. Coron. Artery Dis. 2000, 11, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Leonardo, F.; Fragasso, G.; Rossetti, E.; Dabrowski, P.; Pagnotta, P.; Rosano, G.M.; Chierchia, S.L. Comparison of trimetazidine with atenolol in patients with syndrome X: Effects on diastolic function and exercise tolerance. Cardiologia 1999, 44, 1065–1069. [Google Scholar]
- Elliott, P.; Krzyzowska-Dickinson, K.; Calvino, R.; Hann, C.; Kaski, J.C. Effect of oral aminophylline in patients with angina and normal coronary arteriograms (cardiac syndrome X). Heart 1997, 77, 523–526. [Google Scholar] [CrossRef]
- Yeşildağ, O.; Yazici, M.; Yilmaz, O.; Uçar, R.; Sağkan, O. The effect of aminophylline infusion on the exercise capacity in patients with syndrome X. Acta Cardiol. 1999, 54, 335–337. [Google Scholar]
- Bøtker, H.E.; Sonne, H.S.; Schmitz, O.; Nielsen, T.T. Effects of doxazosin on exercise-induced angina pectoris, ST-segment depression, and insulin sensitivity in patients with syndrome X. Am. J. Cardiol. 1998, 82, 1352–1356. [Google Scholar] [CrossRef]
- Rosen, S.D.; Lorenzoni, R.; Kaski, J.-C.; Foale, R.A.; Camici, P.G. Effect of α1-Adrenoceptor Blockade on Coronary Vasodilator Reserve in Cardiac Syndrome X. J. Cardiovasc. Pharmacol. 1999, 34, 554–560. [Google Scholar] [CrossRef]
- Rakhimov, K.; Gori, T. Non-Pharmacological Treatment of Refractory Angina and Microvascular Angina. Biomedicines 2020, 8, 285. [Google Scholar] [CrossRef]
- Lamendola, P.; Lanza, G.A.; Spinelli, A.; Sgueglia, G.A.; Di Monaco, A.; Barone, L.; Sestito, A.; Crea, F. Long-term prognosis of patients with cardiac syndrome X. Int. J. Cardiol. 2010, 140, 197–199. [Google Scholar] [CrossRef]
- Al Suwaidi, J.; Hamasaki, S.; Higano, S.T.; Nishimura, R.A.; HolmesJr, D.R.; Lerman, A. Long-Term Follow-Up of Patients with Mild Coronary Artery Disease and Endothelial Dysfunction. Circulation 2000, 101, 948–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Mering, G.O.; Arant, C.B.; Wessel, T.R.; McGorray, S.P.; Bairey Merz, C.N.; Sharaf, B.L.; Smith, K.M.; Olson, M.B.; Johnson, B.D.; Sopko, G.; et al. Abnormal coronary vasomotion as a prognostic indicator of cardiovascular events in women: Results from the National Heart, Lung, and Blood Institute-Sponsored Women’s Ischemia Syndrome Evaluation (WISE). Circulation 2004, 109, 722–725. [Google Scholar] [CrossRef] [Green Version]
- Gdowski, M.A.; Murthy, V.L.; Doering, M.; Monroy-Gonzalez, A.G.; Slart, R.; Brown, D.L. Association of Isolated Coronary Microvascular Dysfunction with Mortality and Major Adverse Cardiac Events: A Systematic Review and Meta-Analysis of Aggregate Data. J. Am. Heart Assoc. 2020, 9, e014954. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, K.; Fukuda, S.; Shimada, K.; Miyazaki, C.; Otsuka, K.; Maeda, K.; Miyahana, R.; Kawarabayashi, T.; Watanabe, H.; Yoshikawa, J.; et al. Impaired Coronary Flow Reserve as a Marker of Microvascular Dysfunction to Predict Long-Term Cardiovascular Outcomes, Acute Coronary Syndrome and the Development of Heart Failure. Circ. J. 2012, 76, 1958–1964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masumoto, A.; Mohri, M.; Takeshita, A. Three-year follow-up of the Japanese patients with microvascular angina attributable to coronary microvascular spasm. Int. J. Cardiol. 2001, 81, 151–156. [Google Scholar] [CrossRef]
- Suda, A.; Takahashi, J.; Beltrame, J.F.; Berry, C.; Camici, P.G.; Crea, F.; Escaned, J.; Ford, T.; Kaski, J.C.; Kiyooka, T.; et al. International prospective cohort study of microvascular angina—Rationale and design. IJC Heart Vasc. 2020, 31, 100630. [Google Scholar] [CrossRef]
- Shimokawa, H.; Suda, A.; Takahashi, J.; Berry, C.; Camici, P.G.; Crea, F.; Escaned, J.; Ford, T.; Yii, E.; Kaski, J.C.; et al. Clinical characteristics and prognosis of patients with microvascular angina: An international and prospective cohort study by the Coronary Vasomotor Disorders International Study (COVADIS) Group. Eur. Heart J. 2021. Online ahead of print. [Google Scholar] [CrossRef]
- Lee, S.H.; Lee, J.M.; Park, J.; Choi, K.H.; Hwang, D.; Doh, J.; Nam, C.; Shin, E.; Hoshino, M.; Murai, T.; et al. Prognostic Implications of Resistive Reserve Ratio in Patients with Coronary Artery Disease. J. Am. Heart Assoc. 2020, 9, e015846. [Google Scholar] [CrossRef]
- Murthy, V.; Naya, M.; Taqueti, V.R.; Foster, C.R.; Gaber, M.; Hainer, J.; Dorbala, S.; Blankstein, R.; Rimoldi, O.; Camici, P.G.; et al. Effects of Sex on Coronary Microvascular Dysfunction and Cardiac Outcomes. Circulation 2014, 129, 2518–2527. [Google Scholar] [CrossRef] [Green Version]
- Zhou, W.; Lee, J.C.Y.; Leung, S.T.; Lai, A.; Lee, T.-F.; Chiang, J.B.; Cheng, Y.W.; Chan, H.-L.; Yiu, K.-H.; Goh, V.K.-M.; et al. Long-Term Prognosis of Patients with Coronary Microvascular Disease Using Stress Perfusion Cardiac Magnetic Resonance. JACC Cardiovasc. Imaging 2021, 14, 602–611. [Google Scholar] [CrossRef]
- Chung, J.-H.; Lee, K.E.; Lee, J.M.; Her, A.-Y.; Kim, C.H.; Choi, K.H.; Bin Song, Y.; Hahn, J.-Y.; Kim, H.Y.; Choi, J.-H.; et al. Effect of Sex Difference of Coronary Microvascular Dysfunction on Long-Term Outcomes in Deferred Lesions. JACC Cardiovasc. Interv. 2020, 13, 1669–1679. [Google Scholar] [CrossRef]
- Rush, C.J.; Berry, C.; Oldroyd, K.G.; Rocchiccioli, J.P.; Lindsay, M.M.; Touyz, R.M.; Murphy, C.L.; Ford, T.J.; Sidik, N.; McEntegart, M.B.; et al. Prevalence of Coronary Artery Disease and Coronary Microvascular Dysfunction in Patients with Heart Failure with Preserved Ejection Fraction. JAMA Cardiol. 2021, 6, 1130. [Google Scholar] [CrossRef] [PubMed]
- Elgendy, I.Y.; Pepine, C.J. Heart Failure with Preserved Ejection Fraction: Is Ischemia Due to Coronary Microvascular Dysfunction a Mechanistic Factor? Am. J. Med. 2019, 132, 692–697. [Google Scholar] [CrossRef] [PubMed]
- AbouEzzeddine, O.F.; Kemp, B.J.; Borlaug, B.A.; Mullan, B.P.; Behfar, A.; Pislaru, S.; Fudim, M.; Redfield, M.M.; Chareonthaitawee, P. Myocardial Energetics in Heart Failure with Preserved Ejection Fraction. Circ. Heart Fail. 2019, 12, e006240. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.H.; Obokata, M.; Reddy, Y.N.; Redfield, M.M.; Lerman, A.; Borlaug, B.A. Endothelium-dependent and independent coronary microvascular dysfunction in patients with heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2020, 22, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Mahfouz, R.A.; Gouda, M.; Abdelhamid, M. Relation of microvascular dysfunction and exercise tolerance in patients with heart failure with preserved ejection fraction. Echocardiography 2020, 37, 1192–1198. [Google Scholar] [CrossRef]
- Hage, C.; Svedlund, S.; Saraste, A.; Faxén, U.L.; Benson, L.; Fermer, M.L.; Gan, L.M.; Shah, S.J.; Lam, C.S.P.; Lund, L.H. Association of Coronary Microvascular Dysfunction with Heart Failure Hospitalizations and Mortality in Heart Failure with Preserved Ejection Fraction: A Follow-up in the PROMIS-HFpEF Study. J. Card. Fail. 2020, 26, 1016–10121. [Google Scholar] [CrossRef]
- Konerman, M.C.; Greenberg, J.C.; Kolias, T.J.; Corbett, J.R.; Shah, R.V.; Murthy, V.L.; Hummel, S.L. Reduced Myocardial Flow Reserve Is Associated with Diastolic Dysfunction and Decreased Left Atrial Strain in Patients with Normal Ejection Fraction and Epicardial Perfusion. J. Card. Fail. 2018, 24, 90–100. [Google Scholar] [CrossRef]
- Taqueti, V.R.; Solomon, S.D.; Shah, A.M.; Desai, A.S.; Groarke, J.D.; Osborne, M.; Hainer, J.; Bibbo, C.F.; Dorbala, S.; Blankstein, R.; et al. Coronary microvascular dysfunction and future risk of heart failure with preserved ejection fraction. Eur. Heart J. 2018, 39, 840–849. [Google Scholar] [CrossRef]
- Sucato, V.; Galassi, A.R.; Novo, S.; Saladino, A.; Evola, S.; Novo, G. Correlation between longitudinal strain analysis and coronary microvascular dysfunction in patients with heart failure with preserved ejection fraction. Microcirculation 2020, 27, e12605. [Google Scholar] [CrossRef]
- Pena, A.; Michelsen, M.M.; Mygind, N.D.; Gustafsson, I.; Høst, N.; Bech, J.; Kastrup, J.; Hansen, H.S.; Hansen, P.R.; Prescott, E. Coronary microvascular dysfunction is associated with cardiac time intervals in women with angina and no obstructive coronary artery disease: An iPOWER substudy. Echocardiography 2019, 36, 1110–1117. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Diagnosis | Mechanism | Definition |
|---|---|---|
| Microvascular Disease | ||
| Abnormally high microvascular resistance at rest | Coronary slow flow/Syndrome Y | |
| Impaired microvascular relaxation | With microvascular disease: IMR > 25 AND/OR HMR > 2.4 No clear conclusion about microvascular disease: CFR < 2.0 with FFR > 0.80 and/or resting indexes > 0.89 | |
| Microvascular spasm | Angina during intracoronary infusion of acetylcholine with typical ischemic ST-segment changes, FFR/resting indexes normal AND IMR > 25 immediately after highest dose Ach | |
| Epicardial Disease | ||
| Epicardial spasm | (1) reproduction of the usual symptoms AND; (2) ischemic ECG changes (1 mm horizontal or downsloping ST depression OR ST elevation OR T Wave inversion) AND; (3) >75% vasoconstriction on angiography AND FFR < 0.80 OR resting indexes < 0.89 | |
| Obstructive epicardial disease | FFR < 0.80 Contrast FFR < 0.83 Resting indexes < 0.89 | |
| Endotype | Diagnosis: Coronary Vasomotion Disorder | Stratified Medical Therapy |
|---|---|---|
| Microvascular angina | IMR ≥ 25\(Microvascular resistance) | Baseline therapy: Consider aspirin, statin and ACE inhibitor therapy in all patients. PRN sublingual GTNAntianginal therapy 1st Line—Beta blocker (e.g., nebivolol 2.5 mg OD or carvedilol 6.25 mg BD uptitrated) 2nd Line—Calcium channel blockers (CCB) substituted (Non DHP e.g., verapamil 40 mg BD uptitrated)—where β-blockers are not tolerated or are ineffective 3rd Line—Add in therapy (avoid long acting nitrates) • CCB—DHP (e.g., amlodipine)—only for those on beta-blockers • Ranolazine (375 mg BD, uptitrated) Avoid long-acting nitrate unless previously established good response or co-existent epicardial spasm |
| CFR < 2.0 (Coronary vasorelaxation) | ||
| Microvascular spasm to Ach (Propensity to microvascular constriction) | ||
| Vasospastic angina | Epicardial spasm (>90%) | Baseline therapy: If atherosclerosis or endothelial impairment, aspirin, statin and ACE inhibitor should be considered. PRN sublingual GTN Antianginal Rx 1st Line—Calcium channel blocker (CCB)—e.g., verapamil 40 mg BD uptitrated 2nd Line—Add nitrate—e.g., PETN 50 mg BD-TID |
| Non-cardiac | Nil | Cessation of antianginal therapy. Stop antiplatelet and statin unless other indication. Consider non-cardiac investigation or referral where appropriate (e.g., psychological referral, gastroenterology) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abouelnour, A.; Gori, T. Vasomotor Dysfunction in Patients with Ischemia and Non-Obstructive Coronary Artery Disease: Current Diagnostic and Therapeutic Strategies. Biomedicines 2021, 9, 1774. https://doi.org/10.3390/biomedicines9121774
Abouelnour A, Gori T. Vasomotor Dysfunction in Patients with Ischemia and Non-Obstructive Coronary Artery Disease: Current Diagnostic and Therapeutic Strategies. Biomedicines. 2021; 9(12):1774. https://doi.org/10.3390/biomedicines9121774
Chicago/Turabian StyleAbouelnour, Amr, and Tommaso Gori. 2021. "Vasomotor Dysfunction in Patients with Ischemia and Non-Obstructive Coronary Artery Disease: Current Diagnostic and Therapeutic Strategies" Biomedicines 9, no. 12: 1774. https://doi.org/10.3390/biomedicines9121774