
Stereotactic Arrhythmia Radioablation as a Novel Treatment Approach for Cardiac Arrhythmias: Facts and Limitations

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Stereotactic Arrhythmia Radioablation: Basic Principles
2.2.1. Patient Characteristics
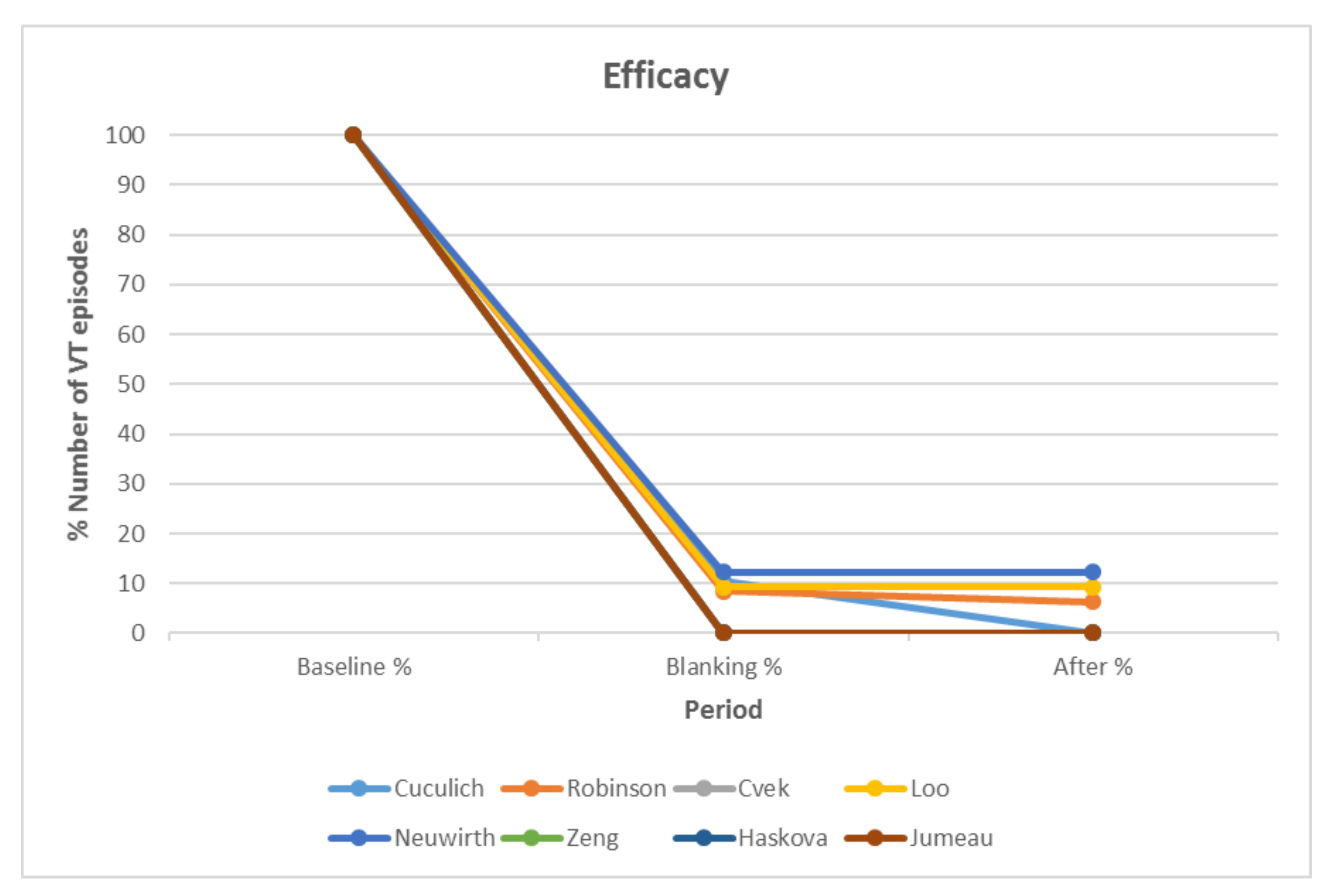
2.2.2. Assessment of Treatment Efficacy and Safety
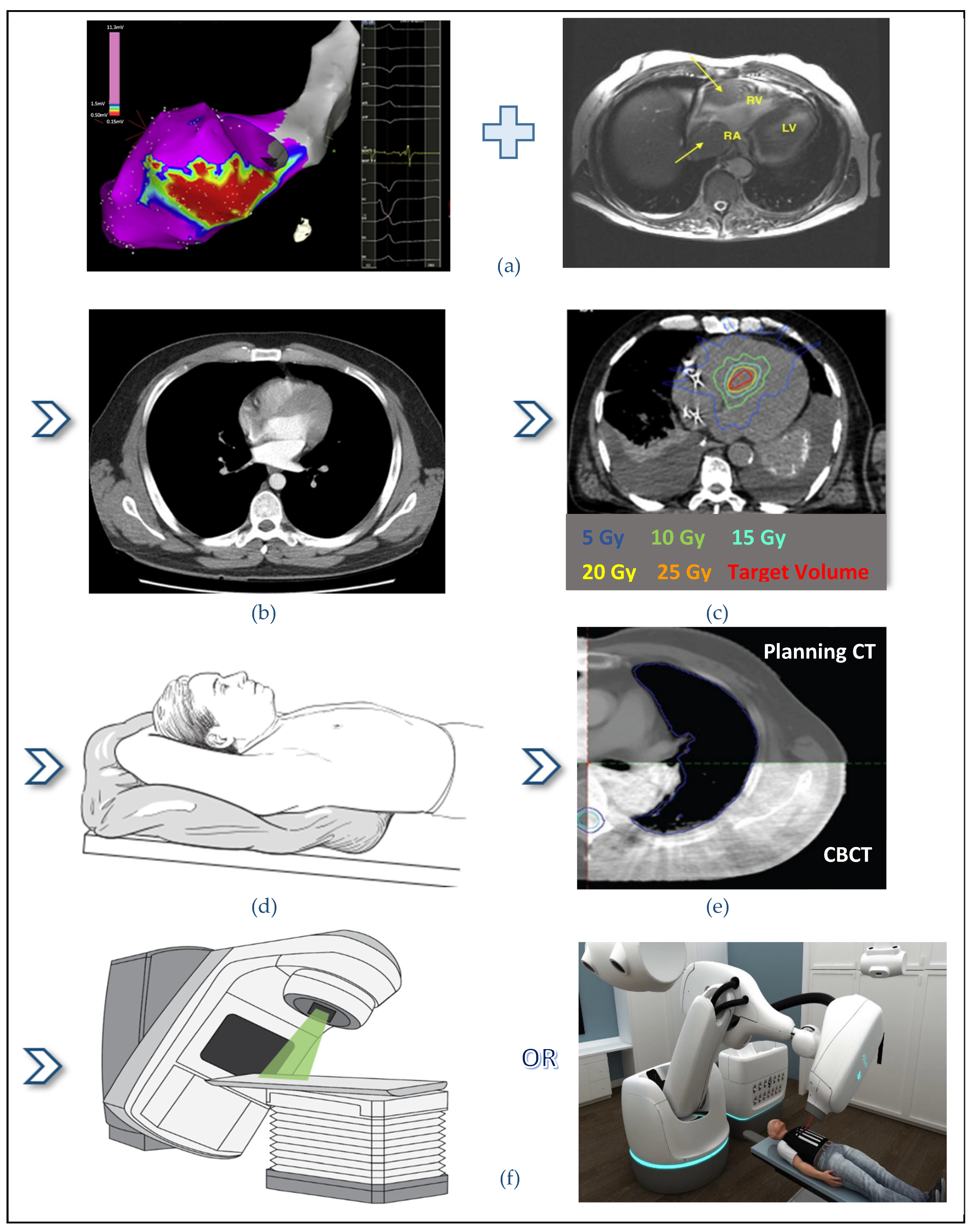
2.3. STAR Workflow and Treatment Delivery
2.3.1. Quality Assurance Processes
Treatment Delivery Machine Evaluation
- Small-field measurements, performed with appropriate stereotactic detectors (spatial resolution of approximately 1 mm, or better). International Atomic Energy Agency has published a code of practice for small field dosimetry, which is a useful guideline [38];
- Laser localization test;
- Radiation isocentricity test (STAR pattern), covering complete range of gantry, couch, collimator positions used clinically;
- IGRT positioning/repositioning;
- Accelerator output constancy;
- Coincidence of radiation and mechanical isocenter. The Winston-Lutz test is commonly used to establish coincidence of planning and delivery isocenters [39];
- End-to-end assessment of geometric accuracy of the entire imaging, planning, and delivery process using dosimetry phantoms and IGRT systems. The basic phantom is a simple block of plastic with small, embedded ball bearings positioned as fiducial markers. A more elaborate procedure could be with an anthropomorphic phantom with fiducial markers placed at selected locations to simulate registration landmarks and target locations [40];
- End-to-end dosimetric evaluation using dosimetry phantoms and IGRT systems.
- IrisTM field-size spot check, for CyberKnife systems;
- Path verification;
- Beam laser and radiation beam alignment for cone, IrisTM, and multi-leaf collimator (MLC).
Immobilization Devices and Simulation Procedure
Motion Management
Treatment Planning System
2.3.2. Imaging the Arrhythmia Substrate
2.3.3. CT-Simulation
2.3.4. Interfraction Motion Management
- Inhibition, which aims to limit respiratory motion using abdominal compression or breath-hold technique;
- Gating, which follows the full respiratory cycle to deliver radiation only when the target is within a defined region of the cycle. Varian Medical Systems implement the RPM and the RGSC respiratory gating systems. TG-147 provides detailed information for the test of integration of the respiratory gating device with peripheral equipment, spatial reproducibility and drift, static and dynamic localization accuracy [48];
- Tracking methods, which redirect the radiation beam to follow the moving target. Fiducial markers serve as surrogates for the target position. Fiducial markers may be an existing device component, an implanted gold seed or intracardiac and extracardiac structures. CyberKnife synchronizes the moving robotic arm with the target in real-time using an internal respiratory tracking system (Synchrony Respiratory Tracking System). The respiratory tracking system uses continual imaging of fiducials to align the radiation beam with the motion of the target.
2.3.5. Contouring
2.3.6. Treatment Planning Parameters
2.3.7. Patient-Specific QA
- Dose delivery measurements when appropriate;
- Independent check of the approved treatment plan and associated treatment delivery parameters. Verification plans should be created for each treatment plan at the treatment delivery machine, prior to treatment and then perform:
- Dose measurements with an appropriate phantom;
- and/or point dose measurements with an ionization chamber in a plastic water phantom, or water-equivalent phantom;
- and/or planar measurements with electronic portal imaging device-based dosimetry, calibrated for dose response;
- and/or film dosimetry, with films calibrated for the selected treatment beam.
- Dry run of the approved treatment plan to check for potential collision;
- Verification of patient setup/immobilization.
2.3.8. Treatment Delivery
2.3.9. Follow-Up
3. Discussion and Future Directions
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Available online: https://www.who.int/health-topics/cardiovascular-diseases/#tab=tab_1 (accessed on 5 October 2020).
- Wang, L.; Fahimian, B. Stereotactic Arrhythmia Radioablation (STAR) of Ventricular Tachycardia: A Treatment Planning Study. Cureus 2016, 8, e694. [Google Scholar] [CrossRef] [Green Version]
- Zei, P.; Soltys, S. Ablative Radiotherapy as a Noninvasive Alternative to Catheter Ablation for Cardiac Arrhythmias. Curr. Cardiol. Rep. 2017, 19, 79. [Google Scholar] [CrossRef] [Green Version]
- Robinson, C.; Samson, P. Phase I/II Trial of Electrophysiology-Guided Noninvasive Cardiac Radioablation for Ventricular Tachycardia. Circulation 2019, 139, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Xia, P.; Kotecha, R. A Treatment Planning Study of Stereotactic Body Radiotherapy for Atrial Fibrillation. Cureus 2016, 8, e678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sapp, J.L.; Wells, G.A. Ventricular tachycardia ablation versus escalation of antiarrhythmic drugs. N. Engl. J. Med. 2016, 375, 111–121. [Google Scholar] [CrossRef]
- Kim, E.J.; Davogustto, G. Non-invasive Cardiac Radiation for Ablation of Ventricular Tachycardia: A New Therapeutic Paradigm in Electrophysiology. Arrhythmia Electrophysiol. Rev. 2018, 7, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Tokuda, M.; Kojodjojo, P. Acute failure of catheter ablation for ventricular tachycardia due to structural heart disease: Causes and significance. J. Am. Heart Assoc. 2013, 2, e000072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qian, P.C.; Azpiri, J.R. Noninvasive stereotactic radioablation for the treatment of atrial fibrillation: First-in-man experience. J. Arrhythmia 2020, 36, 67–74. [Google Scholar] [CrossRef]
- Kirchhof, P.; Benussi, S. ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace 2016, 18, 1609–1678. [Google Scholar] [CrossRef]
- Gianni, C.; Mohanty, S. Alternative approaches for ablation of resistant ventricular tachycardia. Cardiol. Electrophysiol. Clin. 2017, 9, 93–98. [Google Scholar] [CrossRef]
- Page, M.; McKenzie, J. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 372, 178–189. [Google Scholar] [CrossRef]
- Leksell, L. The stereotaxic method and radiosurgery of the brain. Acta Chir. Scand. 1951, 102, 316–319. [Google Scholar]
- Wei, C.; Qian, P. Non-invasive Stereotactic Radioablation: A New Option for the Treatment of Ventricular Arrhythmias. Arrhythmia Electrophysiol. Rev. 2019, 8, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Cuculich, P.; Schill, M. Noninvasive Cardiac Radiation for Ablation of Ventricular Tachycardia. N. Engl. J. Med. 2017, 14, 2325–2336. [Google Scholar] [CrossRef] [PubMed]
- Neuwirth, R.; Cvek, J. Stereotactic radiosurgery for ablation of ventricular tachycardia. Europace 2019, 21, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, M.S.; Wight, J. Clinical experience of stereotactic body radiation for refractory ventricular tachycardia in advanced heart failure patients. Heart Rhythm 2019, 17, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Chin, R.; Hayase, J. Non-invasive stereotactic body radiation therapy for refractory ventricular arrhythmias: An institutional experience. J. Interv. Card. Electrophysiol. 2020, 107, 2411–2502. [Google Scholar] [CrossRef]
- Gianni, C.; Rivera, D. Stereotactic arrhythmia radioablation for refractory scar related ventricular tachycardia. Heart Rhythm 2020, 17, 1241–1248. [Google Scholar] [CrossRef]
- Knutson, N.C.; Samson, P.P. Noninvasive Cardiac Radioablation for Ventricular Tachycardia. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 1114–1123. [Google Scholar] [CrossRef] [Green Version]
- Cvek, J.; Neuwirth, R. Cardiac Radiosurgery for Malignant Ventricular Tachycardia. Cureus 2014, 6, e190. [Google Scholar] [CrossRef] [Green Version]
- Loo, B.W.; Soltys, S.G. Stereotactic ablative radiotherapy for the treatment of refractory cardiac ventricular arrhythmia. Circ. Arrhythmia Electrophysiol. 2015, 8, 748–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, L.J.; Huang, L.H. Stereotactic body radiation therapy for refractory ventricular tachycardia secondary to cardiac lipoma: A case report. Pacing Clin. Electrophysiol. 2019, 42, 1276–1279. [Google Scholar] [CrossRef] [PubMed]
- Haskova, J.; Peichl, P. Stereotactic radiosurgery as a treatment for recurrent ventricular tachycardia associated with cardiac fibroma. Heart Rhythm Case Rep. 2019, 5, 44–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jumeau, R.; Ozsahin, M. Rescue procedure for an electrical storm using robotic non-invasive cardiac radio-ablation. Radiother. Oncol. 2018, 128, 189–191. [Google Scholar] [CrossRef] [PubMed]
- Bhaskaran, A.; Downar, E. Electroanatomical mapping—Guided stereotactic radiotherapy for right ventricular tachycardia storm. Heart Rhythm Case Rep. 2019, 30, 590–592. [Google Scholar] [CrossRef] [Green Version]
- Krug, D.; Blanck, O. Stereotactic body radiotherapy for ventricular tachycardia (cardiac radiosurgery): First-in-patient treatment in Germany. Strahlenther. Onkol. 2019, 196, 23–30. [Google Scholar] [CrossRef]
- Mayinger, M.; Kovacs, B. First magnetic resonance imaging-guided cardiac radioablation of sustained ventricular tachycardia. Radiother. Oncol. 2020, 152, 203–207. [Google Scholar] [CrossRef]
- Marti-Almor, J.; Jimenez-Lopez, J. Noninvasive ablation of ventricular tachycardia with stereotactic radiotherapy in a patient with arrhythmogenic right ventricular cardiomyopathy. Rev. Esp. Cardiol. 2019, 73, 97–99. [Google Scholar] [CrossRef]
- Scholz, E.P.; Seidensaal, K. Risen from the dead: Cardiac stereotactic ablative radiotherapy as last rescue in a patient with refractory ventricular fibrillation storm. Heart Rhythm Case Rep. 2019, 5, 329–332. [Google Scholar] [CrossRef] [Green Version]
- Monroy, E.; Azpiri, J. Late Gadolinium Enhancement Cardiac Magnetic Resonance Imaging Post-robotic Radiosurgical Pulmonary Vein Isolation (RRPVI): First Case in the World. Cureus 2016, 8, e738. [Google Scholar] [CrossRef] [Green Version]
- Shoji, M.; Inaba, K. Advantages and challenges for noninvasive atrial fibrillation ablation. J. Interv. Card. Electrophysiol. 2020. [Google Scholar] [CrossRef]
- Gossman, M.S.; Graham, J.D. Evaluation of a ventricular assist device: Stability under X-rays and therapeutic beam attenuation. ASAIO J. 2012, 58, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Blanck, O.; Ipsen, S. Treatment Planning Considerations for Robotic Guided Cardiac Radiosurgery for Atrial Fibrillation. Cureus 2016, 8, e705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benedict, S.; Yenice, K. Stereotactic body radiation therapy: The report of AAPM Task Group 101. Stereotactic body radiation therapy: The report of AAPM Task Group 101. Med. Phys. 2010, 37, 4078–4101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halvorsen, P.H.; Cirino, E. AAPM-RSS Medical Physics Practice Guideline 9.a. for SRS-SBRT. J. Appl. Clin. Med. Phys. 2017, 18, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Dieterich, S.; Cavedon, C. Report 135—Report of AAPM TG 135, quality assurance for robotic radiosurgery. Med. Phys. 2011, 38, 2914–2936. [Google Scholar] [CrossRef] [Green Version]
- International Atomic Energy Agency. Dosimetry of Small Static Fields Used in External Beam Radiotherapy: An IAEA-AAPM International Code of Practice for Reference and Relative Dose Determination; Technical Report Series 483; IAEA: Vienna, Austria, 2017. [Google Scholar]
- Lutz, W.; Winston, K.R. A system for stereotactic radiosurgery with a linear accelerator. Int. J. Radiat. Oncol. Biol. Phys. 1988, 14, 373–381. [Google Scholar] [CrossRef]
- Galvin, J.; Bednarz, G. Quality assurance procedures for stereotactic body radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2007, 71, S122–S125. [Google Scholar] [CrossRef]
- Weidlich, G.A.; Hacker, F. Ventricular Tachycardia: A Treatment Comparison Study of the CyberKnife with Conventional Linear Accelerators. Cureus 2018, 10, e3445. [Google Scholar] [CrossRef] [Green Version]
- Shi, C.; Tang, X. Evaluation of the new respiratory gating system. Prec. Radiat. Oncol. 2017, 1, 127–133. [Google Scholar] [CrossRef]
- Keall, P.J.; Mageras, G.S. The management of respiratory motion in radiation oncology report of AAPM Task Group 76. Med. Phys. 2006, 33, 3874–3900. [Google Scholar] [CrossRef]
- Lydiard, S.; Caillet, V. Investigating multi-leaf collimator tracking in stereotactic arrhythmic radioablation (STAR) treatments for atrial fibrillation. Phys. Med. Biol. 2018, 63, 195008. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.M.; Jain, R. Electrocardiographic localization of ventricular tachycardia in patients with structural heart disease. Cardiol. Electrophysiol. Clin. 2017, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Cuculich, P.S. Noninvasive electroanatomic mapping of human ventricular arrhythmias with electrocardiographic imaging. Sci. Transl. Med. 2011, 3, 98ra84. [Google Scholar] [CrossRef] [Green Version]
- Brett, C.L.; Cook, J.A. Novel Workflow for Conversion of Catheter-Based Electroanatomic Mapping to DICOM Imaging for Non-Invasive Radioablation of Ventricular Tachycardia. Pract. Radiat. Oncol. 2020, 11, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Willoughby, T.; Lehmann, J. Quality assurance for nonradiographic radiotherapy localization and positioning systems: Report of task group 147. Med. Phys. 2012, 39, 1728–1747. [Google Scholar] [CrossRef]
- Blanck, O.; Buergy, D. Radiosurgery for ventricular tachycardia: Preclinical and clinical evidence and study design for a German multi-center multi-platform feasibility trial (RAVENTA). Clin. Res. Cardiol. 2020, 109, 1319–1332. [Google Scholar] [CrossRef]
- Sharma, A.; Wong, D. Noninvasive stereotactic radiosurgery (CyberHeart) for creation of ablation lesions in the atrium. Heart Rhythm 2010, 7, 802–810. [Google Scholar] [CrossRef]
- Zei, P.C.; Wong, D. Safety and efficacy of stereotactic radioablation targeting pulmonary vein tissues in an experimental model. Heart Rhythm 2018, 15, 1420–1427. [Google Scholar] [CrossRef] [PubMed]
- Marino, C.; Garibaldi, C. A national survey on technology and quality assurance for stereotactic body radiation therapy. Phys. Med. 2019, 65, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Guckenberger, M.; Meyer, J. Precision of image-guided radiotherapy (IGRT) in six degrees of freedom and limitations in clinical practice. Strahlenther. Onkol. 2007, 183, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT04575662 (accessed on 25 September 2021).
- Yusuf, S.W.; Sami, S. Radiation-induced heart disease: A clinical update. Cardiol. Res. Pract 2011, 2011, 317659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, M.; Kaplan, H.S. The remarkable yin and yang of tumour hypoxia. Int. J. Radiat. Biol. 2010, 86, 907–917. [Google Scholar] [CrossRef]
- Maguire, P.J.; Gardner, E. Cardiac radiosurgery (CyberHeart™) for treatment of arrhythmia: Physiologic and histopathologic correlation in the porcine model. Cureus 2016, 3, e32. [Google Scholar] [CrossRef] [Green Version]
- Zei, P.C.; Soltys, S.G. First-in-man treatment of arrhythmia (ventricular tachycardia) using stereotactic radiosurgery. Heart Rhythm 2013, 10, 1–554. [Google Scholar]
- Blanck, O.; Bode, F. Dose-escalation study for cardiac radiosurgery in a porcine model. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 590–598. [Google Scholar] [CrossRef]
- Dusi, V.; Russo, G. Non-invasive ablation of cardiac arrhythmia. Is proton radiation therapy a step forward? Int. J. Cardiol. 2020, 313, 64–66. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | No. of Patients | Patient Characteristics | Cardiomyopathy Type | Inclusion Criteria | Exclusion Criteria | |||
|---|---|---|---|---|---|---|---|---|
| Episodes of VT | Antiarrhythmics * | History of Catheter Ablation | Additional | |||||
| Cuculich, P. 2017 [15] | 5 |
|
| ≥3 | ≥2 | ≥1 or contraindication | - | LVAD |
| Robinson, C. 2019 [4] | 19 |
|
| ≥3 | ≥1 | ≥1 or contraindication | ≥18 years old |
|
| Cvek, J. 2014 [21] | 1 |
| NICM (case report) | – | – | Ineffective due to excessive myocardium thickness | All standard treatment options exhausted | N/A |
| Loo, B.W. 2015 [22] | 11 |
| N/A | – | – | Contraindicated | – | N/A |
| Neuwirth, R. 2019 [16] | 10 |
|
| – | – | Failed due to Inaccess-ibility of the critical substrate part | – | Subjects with mechanical assist devices |
| Zeng, L.J. 2019 [23] | 1 | Refractory VT secondary to unresectable cardiac lipoma | N/A | – | Failed | Failed | – | N/A |
| Haskova, J. 201 [24] | 1 |
| N/A | Occurr-ence of incessant VT | – | Failed | – | N/A |
| Jumeau, R. 2018 [25] | 3 (report-ed: 1) |
| NICM (1 reported pt) | – | Unrespon-sive | Unrespon-sive | – | N/A |
| Bhaskaran, A. 2019 [26] | 1 |
| N/A | – | Unresp- onsive | Unrespon- sive | – | N/A |
| Lloyd, M.S. 2019 [17] | 10 | Refractory VT |
| – | ≥2 | ≥1 | Failed 1 adjunctive therapy (mechanical support or sympathetic blockade) | N/A |
| Chin, R. 2020 [18] | 8 | Refractory, scar-related VT |
| – | – | Failed multiple RF ablations or contra-indicated | – | N/A |
| Gianni C. 2020 [19] | 5 |
|
| Recurrent sympto-matic VT that induced ICD shock(s) | – | – |
|
|
| Krug D. 2019 [27] | 1 |
| N/A | – | – | Contraindicated | – | N/A |
| Scholz, E.P. 2019 [30] | 1 | Ventricular fibrillation storm | – | – | – | – | All available cardiologic therapeutic strategies failed | – |
| Monroy, E. 2016 [31] | 1 | Paroxysmal AF | – | – | Adverse effects of the AAD and failure to alleviate the symptoms | Contraind-ication | – | – |
| Qian, P.C. 2020 [9] | 2 | Drug-refractory paroxysmal AF | – | – | ≥1 | Refused catheter ablation of AF | Symptom-atic AF |
|
| Shoji, M. 2020 [32] | 3 | Drug-refractory AF | – | – | ≥1 | Unsuitable candidates |
|
|
| Study | Safety Endpoints | Monitoring (Follow-Up) | Outcomes |
|---|---|---|---|
| Cuculich, P. 2017 [15] | Complications |
|
|
| Robinson, C. 2019 [4] | The rate of ≤90-day SAEs defined using CTCAEs |
|
|
| Cvek, J. 2014 [21] | Signs of toxicity |
|
|
| Loo, B.W. 2015 [22] | Complications |
| No definite acute or late complications |
| Neuwirth, R. 2019 [16] | Acute and late radiation-induced events according to the CTCAE 4.0 scale |
|
|
| Zeng, L.J. 2019 [23] | Complications | Not mentioned | No complications during 4 months of follow-up |
| Jumeau, R. 2018 [25] | Complications | Not mentioned | No complications |
| Bhaskaran, A. 2019 [26] | Complications |
| No complications during 2 months of follow-up |
| Lloyd, MS. 2019 [17] | Acute and late radiation-induced events | ICD monitoring 3 months post-STAR for:
|
|
| Chin, R. 2020 [18] | Complications |
|
|
| Gianni, C. 2020 [19] | Radiation-related adverse events |
|
|
| Krug, D. 201 [27] | Radiation-related adverse events |
|
|
| Scholz, E.P. 2019 [30] | Acute and late radiation-induced events |
| No complications during 2 months follow-up |
| Monroy, E. 2016 [31] | Acute and late radiation-induced events |
| No esophageal, respiratory, or pericardial symptoms |
| Qian, P.C. 2020 [9] | Acute and late radiation-induced events |
|
|
| Shoji, M. 2020 [32] | Complications |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chalkia, M.; Kouloulias, V.; Tousoulis, D.; Deftereos, S.; Tsiachris, D.; Vrachatis, D.; Platoni, K. Stereotactic Arrhythmia Radioablation as a Novel Treatment Approach for Cardiac Arrhythmias: Facts and Limitations. Biomedicines 2021, 9, 1461. https://doi.org/10.3390/biomedicines9101461
Chalkia M, Kouloulias V, Tousoulis D, Deftereos S, Tsiachris D, Vrachatis D, Platoni K. Stereotactic Arrhythmia Radioablation as a Novel Treatment Approach for Cardiac Arrhythmias: Facts and Limitations. Biomedicines. 2021; 9(10):1461. https://doi.org/10.3390/biomedicines9101461
Chicago/Turabian StyleChalkia, Marina, Vassilis Kouloulias, Dimitris Tousoulis, Spyridon Deftereos, Dimitris Tsiachris, Dimitrios Vrachatis, and Kalliopi Platoni. 2021. "Stereotactic Arrhythmia Radioablation as a Novel Treatment Approach for Cardiac Arrhythmias: Facts and Limitations" Biomedicines 9, no. 10: 1461. https://doi.org/10.3390/biomedicines9101461