
Differential Capability of Clinically Employed Dermal Regeneration Scaffolds to Support Vascularization for Tissue Bioengineering

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents and Antibodies
2.2. Cell Isolation and Culture
2.3. Immunofluorescence
2.4. RNA Isolation, cDNA Synthesis and Real-Time Quantitative PCR
2.5. MTT Assay
2.6. Time Course Adhesion Assay
2.7. Proliferation Assay
2.8. Staining for Ki-67 and Vimentin
2.9. Growth Factors and Chemokines Detection
2.10. Subcutaneously Application of ADMECs and In Vivo Experiments
3. Results
3.1. Phenotypic Characterization of ADMECs and Evaluation of their Responsiveness to Pro-Inflammatory Cytokines
3.2. Evaluation of ADMEC Adhesive Properties and Colonization Capability of Different Dermal Substitutes
3.3. Assessment of the Proliferative Drive Induced by the Different Dermal Substitutes
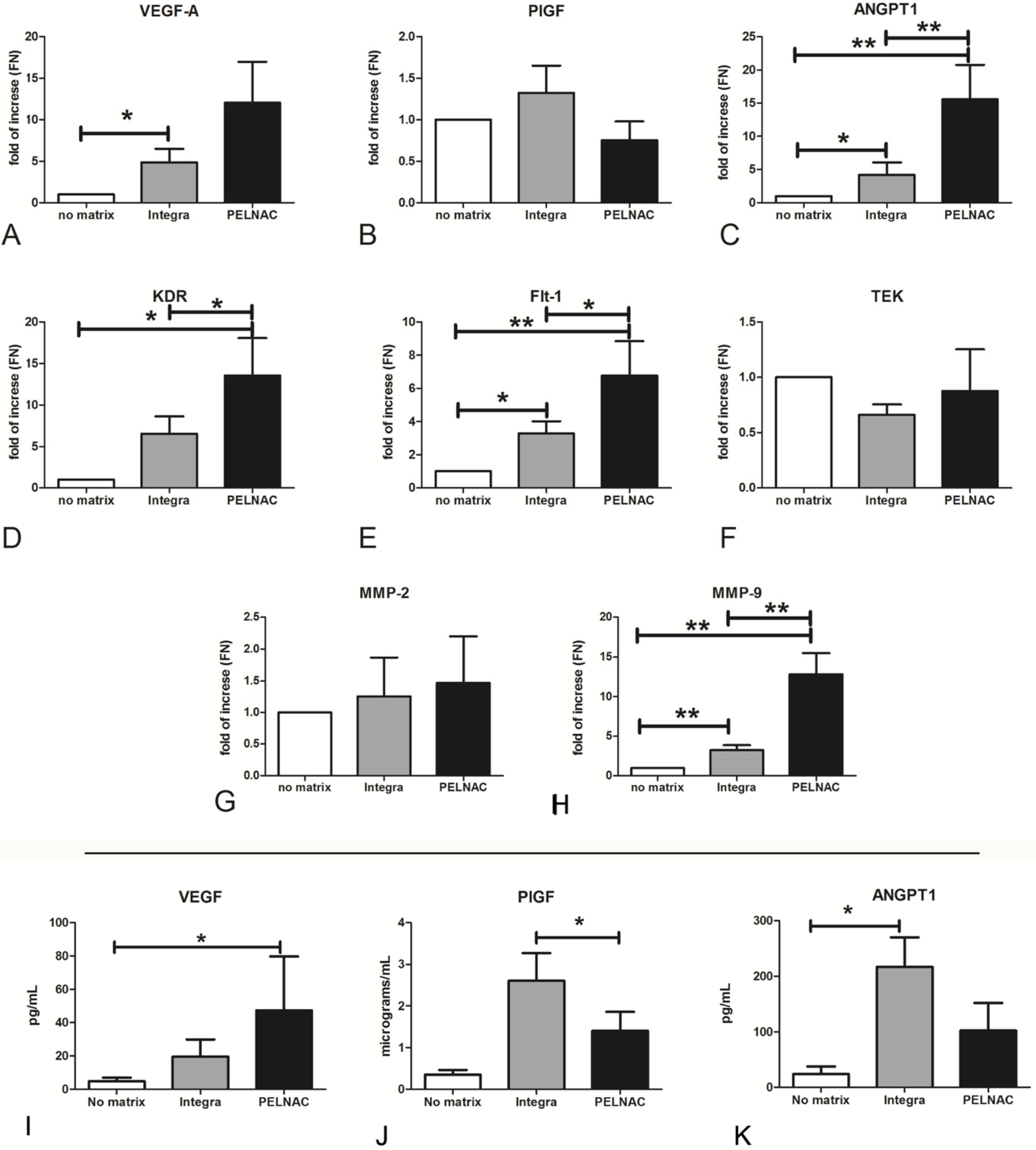
3.4. Proangiogenic and Remodeling Factors Produced by ADMECs on Different Dermal Substitutes
3.5. Dermal Substitutes Modulate the Pro-Inflammatory Behavior of ADMEC
3.6. In Vivo Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Whitney, J.A.D. Overview: Acute and chronic wounds. Nurs. Clin. N. Am. 2005, 40, 191–205. [Google Scholar] [CrossRef]
- Nwomeh, B.C.; Yager, D.R.; Cohen, I.K. Physiology of the Chronic Wound. Clin. Plast. Surg. 1998, 25, 341–356. [Google Scholar] [CrossRef]
- Höckel, M.; Dornhöfer, N. Vulvovaginal reconstruction for neoplastic disease. Lancet Oncol. 2008, 9, 559–568. [Google Scholar] [CrossRef]
- Cohen, I.K.; Diegelmann, R.F.; Lindblad, W.J. Wound Healing: Biochemical and Clinical Aspects. Plast. Reconstr. Surg. 1992, 90, 926. [Google Scholar] [CrossRef]
- Krause, P.J.; Ingardia, C.J.; Pontius, L.T.; Malech, H.L.; LoBello, T.M.; Maderazo, E.G. Host defense during pregnancy: Neutrophil chemotaxis and adherence. Am. J. Obstet. Gynecol. 1987, 157, 274–280. [Google Scholar] [CrossRef]
- Nikolaou, M.; Zampakis, P.; Vervita, V.; Almaloglou, K.; Adonakis, G.; Marangos, M.; Decavalas, G. Necrotizing Fasciitis Complicating Pregnancy: A Case Report and Literature Review. Case Rep. Obstet. Gynecol. 2014, 2014, 1–4. [Google Scholar] [CrossRef]
- Mekkes, J.R.; Westerhof, W. Image processing in the study of wound healing. Clin. Dermatol. 1995, 13, 401–407. [Google Scholar] [CrossRef]
- Levin, M. Diabetic Foot Wounds: Pathogenesis and Management. Adv. Ski. Wound Care 1993, 10, 24–30. [Google Scholar]
- Gallup, D.G.; Freedman, M.A.; Meguiar, R.V.; Freedman, S.N.; Nolan, T.E. Necrotizing fasciitis in gynecologic and obstetric patients: A surgical emergency. Am. J. Obstet. Gynecol. 2002, 187, 305–311. [Google Scholar] [CrossRef]
- Kerstein, M.D. The scientific basis of healing. Adv. Wound Care 1997, 10, 30–36. [Google Scholar]
- Jung, W.; Winter, H. Considerations for the use of clostridial collagenase in pratice from clinical drug investigation. Clin. Drug Investig. 1998, 15, 245–252. [Google Scholar] [CrossRef]
- Sibbald, R.G.; Williamson, D.; Orsted, H.L.; Campbell, K.; Keast, D.; Krasner, D.; Sibbald, D. Preparing the wound bed—Debridement, bacterial balance, and moisture balance. Ostomy Wound Manag. 2000, 46, 14–22, 24. [Google Scholar]
- Eming, S.A.; Martin, P.; Tomic-Canic, M. Wound repair and regeneration: Mechanisms, signaling, and translation. Sci. Transl. Med. 2014, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groppa, E.; Colliva, A.; Vuerich, R.; Kocijan, T.; Zacchigna, S. Immune cell therapies to improve regeneration and revascularization of non-healing wounds. Int. J. Mol. Sci. 2020, 21, 5235. [Google Scholar] [CrossRef]
- Patel, N.P.; Labropoulos, N.; Pappas, P.J. Current management of venous ulceration. Plast. Reconstr. Surg. 2006, 117, 254–260. [Google Scholar] [CrossRef]
- Frykberg, R.G.; Banks, J. Challenges in the Treatment of Chronic Wounds. Adv. Wound Care 2015, 4, 560–582. [Google Scholar] [CrossRef] [Green Version]
- Shevchenko, R.V.; James, S.L.; James, S.E. A review of tissue-engineered skin bioconstructs available for skin reconstruction. J. R. Soc. Interface 2010, 7, 229–258. [Google Scholar] [CrossRef] [Green Version]
- Kamel, R.A.; Ong, J.F.; Eriksson, E.; Junker, J.P.E.; Caterson, E.J. Tissue engineering of skin. J. Am. Coll. Surg. 2013, 217, 533–555. [Google Scholar] [CrossRef]
- Demidova-Rice, T.N.; Durham, J.T.; Herman, I.M. Wound Healing Angiogenesis: Innovations and Challenges in Acute and Chronic Wound Healing. Adv. Wound Care 2012, 1, 17–22. [Google Scholar] [CrossRef]
- Laschke, M.W.; Menger, M.D. Vascularization in tissue engineering: Angiogenesis versus inosculation. Eur. Surg. Res. 2012, 48, 85–92. [Google Scholar] [CrossRef]
- Laschke, M.W.; Menger, M.D. Prevascularization in tissue engineering: Current concepts and future directions. Biotechnol. Adv. 2016, 34, 112–121. [Google Scholar] [CrossRef]
- Félétou, M. The Endothelium, Part I: Multiple Functions of the Endothelial Cells—Focus on Endothelium-Derived Vasoactive Mediators. Colloq. Ser. Integr. Syst. Physiol. Mol. Funct. 2011. [Google Scholar] [CrossRef]
- Aird, W.C. Mechanisms of endothelial cell heterogeneity in health and disease. Circ. Res. 2006, 98, 159–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michiels, C. Endothelial cell functions. J. Cell. Physiol. 2003, 196, 430–443. [Google Scholar] [CrossRef] [PubMed]
- Augustin, H.G.; Young Koh, G.; Thurston, G.; Alitalo, K. Control of vascular morphogenesis and homeostasis through the angiopoietin—Tie system. Nat. Rev. Mol. Cell Biol. 2009, 10, 165–177. [Google Scholar] [CrossRef]
- Jaffe, E.A.; Nachman, R.L.; Becker, C.G.; Minick, C.R. Culture of human endothelial cells derived from umbilical veins. Identification by morphologic and immunologic criteria. J. Clin. Investig. 1973, 52, 2745–2756. [Google Scholar] [CrossRef] [PubMed]
- Krǎling, B.M.; Bischoff, J. A simplified method for growth of human microvascular endothelial cells results in decreased senescence and continued responsiveness to cytokines and growth factors. In Vitro Cell. Dev. Biol. Anim. 1998, 34, 308–315. [Google Scholar] [CrossRef]
- Agostinis, C.; Masat, E.; Bossi, F.; Ricci, G.; Menegazzi, R.; Lombardelli, L.; Zito, G.; Mangogna, A.; Degan, M.; Gattei, V.; et al. Transcriptomics and immunological analyses reveal a pro-angiogenic and anti-inflammatory phenotype for decidual endothelial cells. Int. J. Mol. Sci. 2019, 20, 1604. [Google Scholar] [CrossRef] [Green Version]
- McCurdy, R.D.; McGrath, J.J.; Mackay-Sim, A. Validation of the comparative quantification method of real-time PCR analysis and a cautionary tale of housekeeping gene selection. Gene Ther. Mol. Biol. 2008, 12, 15–24. [Google Scholar]
- Sánchez-Elsner, T.; Botella, L.M.; Velasco, B.; Corbí, A.; Attisano, L.; Bernabéu, C. Synergistic Cooperation between Hypoxia and Transforming Growth Factor-β Pathways on Human Vascular Endothelial Growth Factor Gene Expression. J. Biol. Chem. 2001, 276, 38527–38535. [Google Scholar] [CrossRef] [Green Version]
- Gallo, D.; Cocchietto, M.; Masat, E.; Agostinis, C.; Harei, E.; Veronesi, P.; Sava, G. Human recombinant lysozyme downregulates advanced glycation endproduct-induced interleukin-6 production and release in an in-vitro model of human proximal tubular epithelial cells. Exp. Biol. Med. 2014, 239, 337–346. [Google Scholar] [CrossRef]
- Lédée, N.; Munaut, C.; Sérazin, V.; d’Hauterive, S.P.; Lombardelli, L.; Logiodice, F.; Wainer, R.; Gridelet, V.; Chaouat, G.; Frankenne, F.; et al. Performance evaluation of microbead and ELISA assays for follicular G-CSF: A non-invasive biomarker of oocyte developmental competence for embryo implantation. J. Reprod. Immunol. 2010, 86, 126–132. [Google Scholar] [CrossRef]
- Vig, K.; Chaudhari, A.; Tripathi, S.; Dixit, S.; Sahu, R.; Pillai, S.; Dennis, V.A.; Singh, S.R. Advances in skin regeneration using tissue engineering. Int. J. Mol. Sci. 2017, 18, 789. [Google Scholar] [CrossRef] [PubMed]
- MacNeil, S. Progress and opportunities for tissue-engineered skin. Nature 2007, 445, 874–880. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.A.F.; Ghosh, K.; Tonnesen, M.G. Tissue engineering for cutaneous wounds. J. Investig. Dermatol. 2007, 127, 1018–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greaves, N.S.; Iqbal, S.A.; Baguneid, M.; Bayat, A. The role of skin substitutes in the management of chronic cutaneous wounds. Wound Repair Regen. 2013, 21, 194–210. [Google Scholar] [CrossRef] [PubMed]
- Iacobini, C.; Vitale, M.; Pesce, C.; Pugliese, G.; Menini, S. Diabetic complications and oxidative stress: A 20-year voyage back in time and back to the future. Antioxidants 2021, 10, 727. [Google Scholar] [CrossRef]
- Wong, B.W.; Marsch, E.; Treps, L.; Baes, M.; Carmeliet, P. Endothelial cell metabolism in health and disease: Impact of hypoxia. EMBO J. 2017, 36, 2187–2203. [Google Scholar] [CrossRef]
- Semenza, G.L. Hypoxia-inducible factors in physiology and medicine. Cell 2012, 148, 399–408. [Google Scholar] [CrossRef] [Green Version]
- Tan, K.C.B.; Chow, W.S.; Ai, V.H.G.; Metz, C.; Bucala, R.; Lam, K.S.L. Advanced glycation end products and endothelial dysfunction in type 2 diabetes. Diabetes Care 2002, 25, 1055–1059. [Google Scholar] [CrossRef] [Green Version]
- Galiano, R.D.; Michaels, V.J.; Dobryansky, M.; Levine, J.P.; Gurtner, G.C. Quantitative and reproducible murine model of excisional wound healing. Wound Repair Regen. 2004, 12, 485–492. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Commercial Scaffolds | Components | |
|---|---|---|
 | Integra® Bilayer Matrix Wound Dressing | The dermal layer is composed of bovine type I tendon collagen and chondroitin-6-sulfate; the epidermal layer is made of silicon. |
 | PELNAC® | A bilayer scaffold made of porcine tendon atelocollagen and a silicon layer. |
 | PriMatrix® Dermal Repair Scaffold | Acellular dermal tissue matrix from fetal bovine dermis, particularly rich in type II collagen. |
 | Endoform® Natural Dermal Template | Derived from ovine forestomach tissue that is minimally processed to separate tissue layers and decellularize the tissue extracellular matrix (ECM). It maintains components essential to tissue repair (e.g., collagen I, III, IV, fibronectin, laminin, elastin, hyaluronic acid, heparin sulfate, GAGs, growth factors and chemokines). |
 | Myriad Matrix® | A collagen matrix with an intact ECM. Derived from ovine forestomach, it retains the innate biological structure and function of the native ECM associated macromolecules including elastin, fibronectin, glycosaminoglycans and laminin. |
| Gene | Tm | Sense | Sequence (5′ → 3′) | Accession Number | |
|---|---|---|---|---|---|
| Ribosomal protein S18 | RPS18 | 60 | Forward Reverse | ATC CCT GAA AAG TTC CAG CA CCC TGT TGG TGA GGT CAA TG | NM_022551.2 |
| Glyceraldehyde-3-phosphate dehydrogenase | GAPDH | 60 | Forward Reverse | GAT CAT CAG CAA TGC CTC CT GT GGT CAT GAG TCC TTC CA | NM_002046.5 |
| TATA-box binding protein | TBP | 60 | Forward Reverse | GAG CCA AGA GTG AAG AAC AGT C GCT CCC CAC CAT ATT CTG AAT CT | NM_003194.4 |
| Vascular endothelial growth factor A | VEGFA | 60 | Forward Reverse | CCT GGT GGA CAT CTT CCA GGA GT CTC ACC GCC TCG GCT TGT CAC A | NM_001025366.2 |
| Placental growth factor | PGF | 62 | Forward Reverse | GAA CGG CTC GTC AGA GGT G ACA GTG CAG ATT CTC ATC GCC | NM_001207012 |
| Angiopoietin 1 | ANGPT1 | 60 | Forward Reverse | AGC GCC GAA GTC CAG AAA AC TAC TCT CAC GAC AGT TGC CAT | NM_001146 |
| Kinase insert domain receptor | KDR | 60 | Forward Reverse | GGC CCA ATA ATC AGA GTG GCA CCA GTG TCA TTT CCG ATC ACT TT | NM_002253 |
| Fms related tyrosine kinase 1 | FLT1 | 62 | Forward Reverse | GAA AAC GCA TAA TCT GGG ACA GT GCG TGG TGT GCT TAT TTG GA | NM_001159920 |
| TEK receptor tyrosine kinase | TEK | 62 | Forward Reverse | CAG GAT ACG AAC CAT GAA GAT GC GGG GCA CTG AAT GGA TGA AG | NM_000459 |
| Interleukin 6 | IL6 | 60 | Forward Reverse | GTA CAT CCT CGA CGG CAT C CCA GGC AAG TCT CCT CAT TG | NM_000600.3 |
| C-X-C motif chemokine ligand 8 | IL8/CXCL8 | 60 | Forward Reverse | AGG TGC AGT AGT TTT GCC AAG GA TTT CTG TGT TGG CGC AGT GT | NM_000584 |
| Tumor necrosis factor | TNF | 65 | Forward Reverse | GGC CCA GGC AGT CAG ATC AT GGG GCT CTT GAT GGC AGA GA | NM_000594.3 |
| C-C motif chemokine ligand 2 | MCP1/CCL2 | 60 | Forward Reverse | ATC AAT GCC CCA GTC ACC AGT CTT CGG AGT TTG GG | NM_002982.3 |
| Matrix metallopeptidase 2 | MMP2 | 60 | Forward Reverse | TAC AGG ATC ATT GGC TAC ACA CC GGT CAC ATC GCT CCA GAC T | NM_004530 |
| Matrix metallopeptidase 9 | MMP9 | 60 | Forward Reverse | GGG ACG CAG ACA TCG TCA TC TCG TCA TCG TCG AAA TGG GC | NM_004994 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agostinis, C.; Spazzapan, M.; Vuerich, R.; Balduit, A.; Stocco, C.; Mangogna, A.; Ricci, G.; Papa, G.; Zacchigna, S.; Bulla, R. Differential Capability of Clinically Employed Dermal Regeneration Scaffolds to Support Vascularization for Tissue Bioengineering. Biomedicines 2021, 9, 1458. https://doi.org/10.3390/biomedicines9101458
Agostinis C, Spazzapan M, Vuerich R, Balduit A, Stocco C, Mangogna A, Ricci G, Papa G, Zacchigna S, Bulla R. Differential Capability of Clinically Employed Dermal Regeneration Scaffolds to Support Vascularization for Tissue Bioengineering. Biomedicines. 2021; 9(10):1458. https://doi.org/10.3390/biomedicines9101458
Chicago/Turabian StyleAgostinis, Chiara, Mariagiulia Spazzapan, Roman Vuerich, Andrea Balduit, Chiara Stocco, Alessandro Mangogna, Giuseppe Ricci, Giovanni Papa, Serena Zacchigna, and Roberta Bulla. 2021. "Differential Capability of Clinically Employed Dermal Regeneration Scaffolds to Support Vascularization for Tissue Bioengineering" Biomedicines 9, no. 10: 1458. https://doi.org/10.3390/biomedicines9101458