
Impact of Vitamin D Supplementation on Bone Mineral Density and All-Cause Mortality in Heart Transplant Patients

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
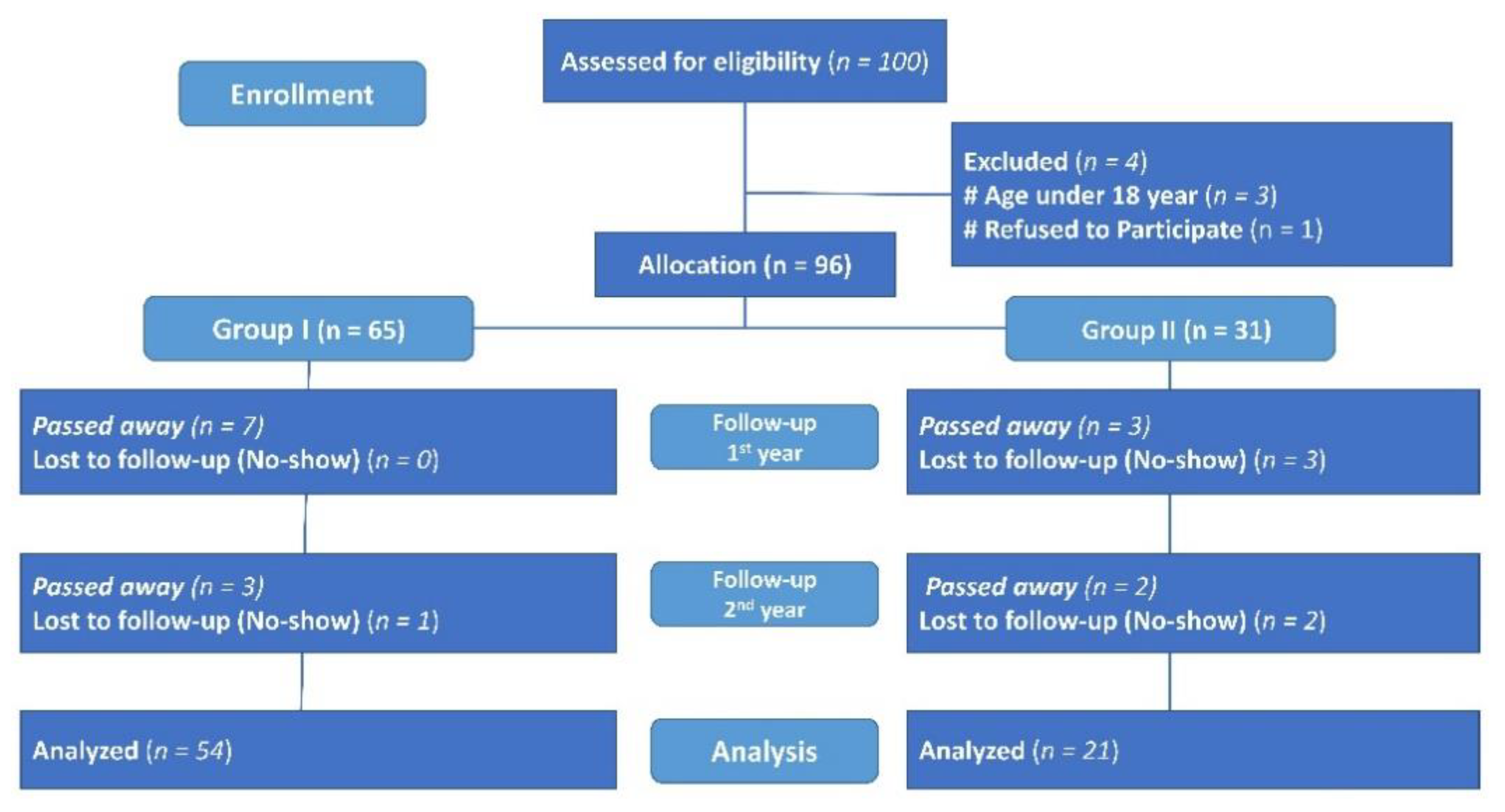
2.1. Study Design and Setting
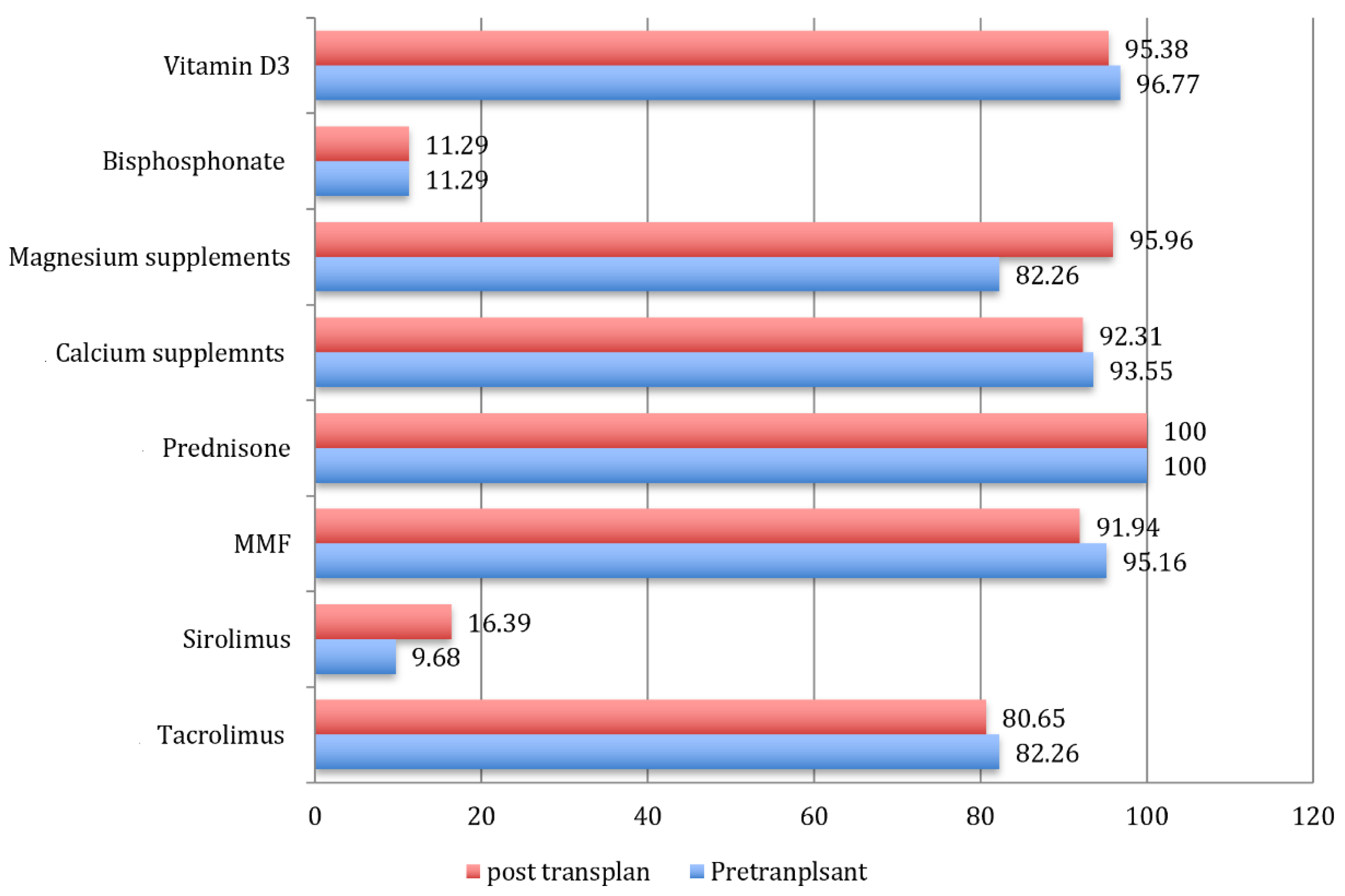
2.2. Given Supplementations and Medications
2.3. Anthropometric Parameters
2.4. Measurement of VD and Biochemical Parameters
2.5. Measurement of BMD
2.6. Sample Size and Satistical Power
2.7. Statistical Analysis
3. Results
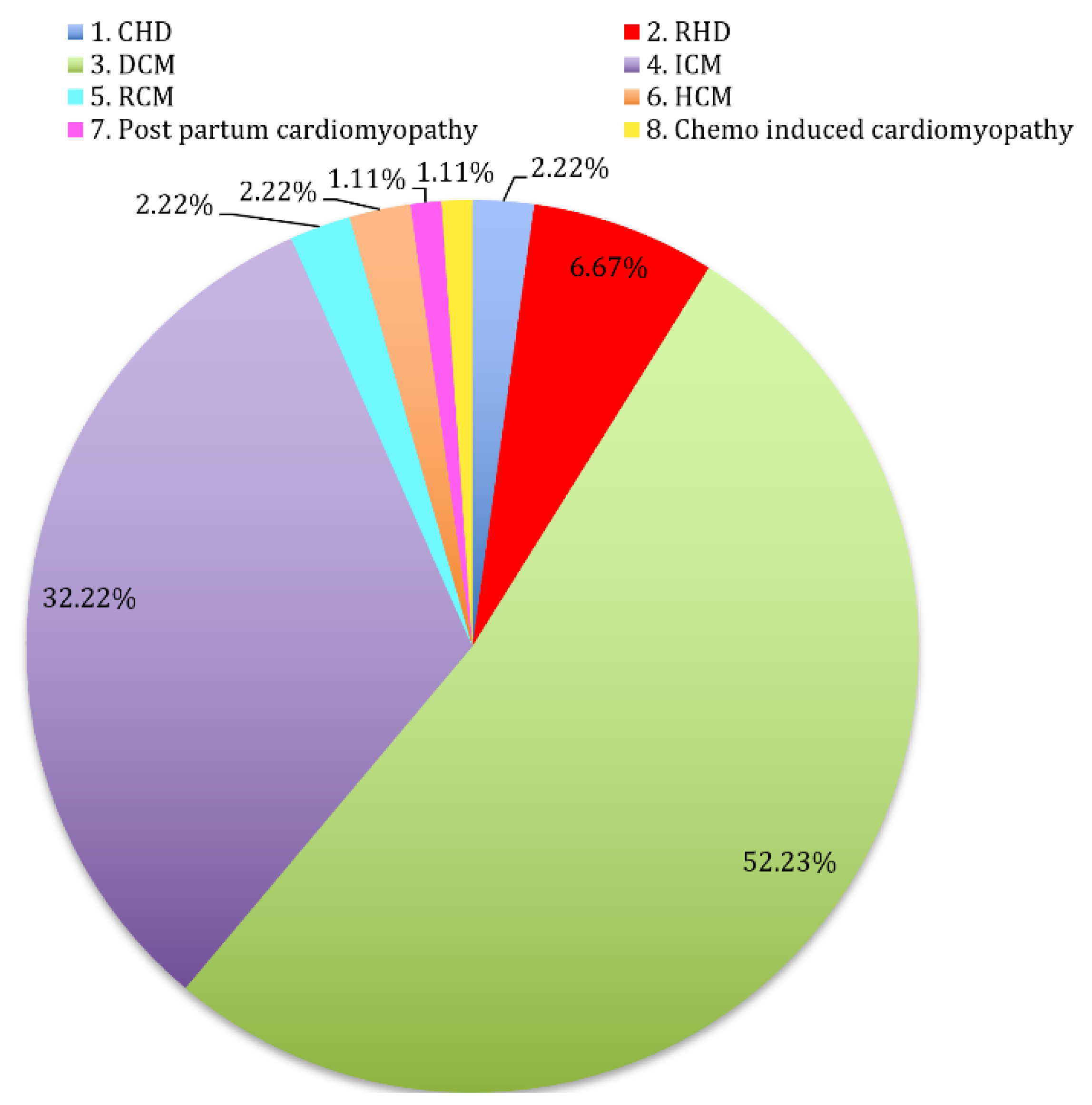
3.1. Basal Characteristics of Study Participants
3.2. Changes in VD and BMD throughout the Study Period
3.3. Survival Analysis Based on VD and BMD
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shane, E.; Mancini, D.; Aaronson, K.; Silverberg, S.J.; Seibel, M.J.; Addesso, V.; McMahon, D.J. Bone mass, vitamin D deficiency and hyperparathyroidism in congestive heart failure. Am. J. Med. 1997, 103, 197–207. [Google Scholar] [CrossRef]
- Stein, E.M.; Shane, E. Vitamin D in organ transplantation. Osteoporos. Int. 2011, 22, 2107–2118. [Google Scholar] [CrossRef] [PubMed]
- Dawson-Hughes, B.; Mithal, A.; Bonjour, J.P.; Boonen, S.; Burckhardt, P.; Fuleihan, G.E.; Josse, R.G.; Lips, P.; Morales-Torres, J.; Yoshimura, N. IOF position statement: Vitamin D recommendation for older adults. Osteoporos. Int. 2010, 21, 1151–1154. [Google Scholar] [CrossRef] [PubMed]
- Veugelers, P.J.; Pham, T.; Ekwaru, J.P. Optimal vitamin D supplementation doses that minimize the risk for both low and high serum 25-hydroxyvitamin D concentrations in the general population. Nutrients 2015, 7, 10189–10208. [Google Scholar] [CrossRef] [Green Version]
- Pludowski, P.; Karczmarewicz, E.; Bayer, M.; Carter, G.; Chlebna-Sokol, D.; Czech-Kowalska, J.; Dębski, R.; Decsi, T.; Dobrzańska, A.; Franek, E.; et al. Practical guidelines for the supplementation of vitamin D and the treatment of deficits in central Europe—recommended vitamin D intakes in the general population and groups at risk for vitamin D deficiency. Endokrynol. Pol. 2013, 64, 319–327. [Google Scholar] [CrossRef]
- Rosen, C.J.; Adams, J.S.; Bikle, D.D.; Black, D.M.; Demay, M.B.; Manson, J.E.; Murad, M.H.; Kovacs, C.S. The nonskeletal effects of vitamin D: An Endocrine Society scientific statement. Endocr. Rev. 2012, 33, 456–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cianferotti, L.; Bertoldo, F.; Bischoff-Ferrari, H.A.; Bruyere, O.; Cooper, C.; Cutolo, M.; Kanis, J.A.; Kaufman, J.M.; Reginster, J.Y.; Rizzoli, R.; et al. Vitamin D supplementation in the prevention and management of major chronic diseases not related to mineral homeostasis in adults: Research for evidence and a scientific statement from the European society for clinical and economic aspects of osteoporosis and osteoarthritis (ESCEO). Endocrine 2017, 56, 245–261. [Google Scholar] [CrossRef] [Green Version]
- Kaddam, I.M.; Al-Shaikh, A.M.; Abaalkhail, B.A.; Asseri, K.S.; Al-Saleh, Y.M.; Al-Qarni, A.A.; Al-Shuaibi, A.M.; Tamimi, W.G.; Mukhtar, A.M. Prevalence of vitamin D deficiency and its associated factors in three regions of Saudi Arabia. Saudi Med. J. 2017, 38, 381–390. [Google Scholar] [CrossRef]
- AlHabeeb, W.; AlAyoubi, F.; Tash, A.; AlAhmari, L.; AlHabib, K.F. Attitude of the Saudi community towards heart donation, transplantation, and artificial hearts. Saudi Med. J. 2017, 38, 742–747. [Google Scholar] [CrossRef]
- Przybyłowski, P.; Wasilewski, G.; Koc-Żórawska, E.; Małyszko, J. Vitamin D Concentration in Patients after Heart and Kidney Transplantation. Transplant. Proc. 2018, 50, 2100–2104. [Google Scholar] [CrossRef]
- Löfdahl, E.; Söderlund, S.; Rådegran, G. Bone mineral density and osteoporosis in heart transplanted patients: A single-center retrospective study at Skåne University Hospital in Lund 1988–2016. Clin. Transplant. 2019, 33, 13477. [Google Scholar] [CrossRef]
- Anastasilakis, A.; Tsourdi, E.; Makras, P.; Polyzos, S.; Meier, C.; McCloskey, E.; Pepe, J.Z. Bone disease following solid organ transplantation: A narrative review and recommendations for management from the European Calcified Tissue Society. Bone 2019, 127, 401–418. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; O’Sullivan, S.; Gamble, G.; Ruygrok, P. Bone density in heart or lung transplant recipients—A longitudinal study. Transplant. Proc. 2013, 45, 2357–2365. [Google Scholar] [CrossRef]
- Selimovic, N.; Nisar, A.; Alburaiki, J.; Khaliel, F. Bone density in heart transplanted patients in Kingdom of Saudi Arabia. J. Saudi Heart Assoc. 2015, 27, 327–328. [Google Scholar] [CrossRef] [Green Version]
- Kunutsor, S.K.; Whitehouse, M.R.; Blom, A.W.; Laukkanen, J.A. Low serum magnesium levels are associated with increased risk of fractures: A long-term prospective cohort study. Eur. J. Epidemiol. 2017, 32, 593–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, J. Vitamin therapy after heart transplantation. Expert. Rev. Cardiovasc. Ther. 2015, 13, 1071–1074. [Google Scholar] [CrossRef]
- Zittermann, A.; Schleithoff, S.S.; Gotting, C.; Fuchs, U.; Kuhn, J.; Kleesiek, K.; Tenderich, G.; Koerfer, R. Calcitriol deficiency and 1-yearmortality in cardiac transplant recipients. Transplantation 2009, 87, 118–124. [Google Scholar] [CrossRef]
- Zittermann, A.; Ernst, J.B.; Prokop, S.; Fuchs, U.; Dreier, J.; Kuhn, J.; Knabbe, C.; Birschmann, I.; Schulz, U.; Berthold, H.K.; et al. Effect of vitamin D on all-cause mortality in heart failure (EVITA): A 3-year randomized clinical trial with 4000 IU vitamin D daily. Eur. Heart J. 2017, 38, 2279–2286. [Google Scholar] [CrossRef] [Green Version]
- Vos, R.; Ruttens, D.; Verleden, S.E.; Vandermeulen, E.; Bellon, H.; Van Herck, A.; Sacreas, A.; Heigl, T.; Schaevers, V.; Van Raemdonck, D.E.; et al. High-dose vitamin D after lung transplantation: A randomized trial. J. Heart Lung Transplant. 2017, 36, 897–905. [Google Scholar] [CrossRef]
- Sempos, C.T.; Heijboer, A.C.; Bikle, D.D.; Bollerslev, J.; Bouillon, R.; Brannon, P.M.; DeLuca, H.F.; Jones, G.; Munns, C.F.; Bilezikian, J.P.; et al. Vitamin D assays and the definition of hypovitaminosis D: Results from the First International Conference on Controversies in Vitamin D. Br. J. Clin. Pharmacol. 2018, 84, 2194–2207. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef]
- Chou, N.K.; Su, I.C.; Kuo, H.L.; Chen, Y.H.; Yang, R.S.; Wang, S.S. Bone mineral density in long-term Chinese heart transplant recipients: A cross-sectional study. Transplant. Proc. 2006, 38, 2141–2144. [Google Scholar] [CrossRef]
- Stein, E.M.; Cohen, A.; Freeby, M.; Rogers, H.; Kokolus, S.; Scott, V.; Mancini, D.; Restaino, S.; Brown, R.; McMahon, D.J.; et al. Severe vitamin D deficiency among heart and liver transplant recipients. Clin. Transplant. 2009, 23, 861–865. [Google Scholar] [CrossRef] [Green Version]
- Rakusa, M.; Vrtovec, B.; Poglajen, G.; Janez, A.; Jensterle, M. Endocrine disorders after heart transplantation: National cohort study. BMC Endocr. Disord. 2020, 20, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briffa, N.K.; Keogh, A.M.; Sambrook, P.N.; Eisman, J.A. Reduction of immunosuppressant therapy requirement in heart transplantation by calcitriol. Transplantation 2003, 75, 2133–2134. [Google Scholar] [CrossRef] [PubMed]
- Schulze-Späte, U.; Mizani, I.; Salaverry, K.R.; Chang, J.; Wu, C.; Jones, M.; Kennel, P.J.; Brunjes, D.L.; Choo, T.H.; Kato, T.S.; et al. Periodontitis and bone metabolism in patients with advanced heart failure and after heart transplantation. ESC Heart Fail. 2017, 4, 169–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilfraguas, L.; Guadalix, S.; Martinez, G.; Jodar, E.; Vara, J.; Gomez-Sanchez, M.A.; Delgado, J.; De La Cruz, J.; Lora, D.; Hawkins, F. Bone loss after heart transplant: Effect of alendronate, etidronate, calcitonin, and calcium plus vitamin D3. Prog. Transplant. 2012, 22, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Kerschan-Schindl, K.; Ruzicka, M.; Mahr, S.; Paireder, M.; Krestan, C.; Gleiss, A.; Bieglmayer, C.; Fialka-Moser, V.; Pacher, R.; Grimm, M.; et al. Unexpected low incidence of vertebral fractures in heart transplant recipients: Analysis of bone turnover. Transpl. Int. 2008, 21, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Shane, E.; Rivas, M.; McMahon, D.J.; Staron, R.B.; Silverberg, S.J.; Seibel, M.J.; Mancini, D.; Michler, R.E.; Aaronson, K.; Addesso, V.; et al. Bone loss and turnover after cardiac transplantation. J. Clin. Endocrinol. Metabol. 1997, 82, 1497. [Google Scholar] [CrossRef]
- Kerschan-Schindl, K.; Strametz-Juranek, J.; Heinze, G.; Grampp, S.; Bieglmayer, C.; Pacher, R.; Maurer, G.; Fialka-Moser, V.; Pietschmann, P. Pathogenesis of bone loss in heart transplant candidates and recipients. J. Heart Lung Transplant. 2003, 22, 843. [Google Scholar] [CrossRef]
- Torregrosa, J.V.; Fuster, D.; Pedroso, S.; Diekmann, F.; Campistol, J.M.; Rubí, S.; Oppenheimer, F. Weekly risedronate in kidney transplant patients with osteopenia. Transpl. Int. 2007, 20, 708. [Google Scholar] [CrossRef] [PubMed]
- Vanderstraeten, K.; De Pauw, R.; Knops, N.; Bouts, A.; Cransberg, K.; El Amouri, A.; Raes, A.; Prytuła, A. Body mass index is associated with hyperparathyroidism in pediatric kidney transplant recipients. Pediatric Nephrol. J. Int. Pediatric Nephrol. Assoc. 2021, 36, 977. [Google Scholar] [CrossRef]
- Moreira, C.A.; Cochenski Borba, V.Z.; Kulak, J., Jr.; Custódio, M.R. Osteoporosis after Transplantation. Curr. Osteoporos. Rep. 2012, 10, 48–55. [Google Scholar] [CrossRef]
- Evenepoel, P.; Claes, K.; Kuypers, D.; Maes, B.; Bammens, B.; Vanrenterghem, Y. Natural history of parathyroid function and calcium metabolism after kidney transplantation: A single-centre study. Nephrol. Dial. Transplant. 2004, 19, 1281–1287. [Google Scholar] [CrossRef] [Green Version]
- Palermo, A.; Sanesi, L.; Colaianni, G.; Tabacco, G.; Naciu, A.M.; Cesareo, R.; Pedone, C.; Lelli, D.; Brunetti, G.; Mori, G.; et al. A Novel Interplay between Irisin and PTH: From Basic Studies to Clinical Evidence in Hyperparathyroidism. J. Clin. Endocrinol. Metab. 2019, 104, 3088–3096. [Google Scholar] [CrossRef]
- Zini, M.; Attanasio, R.; Cesareo, R.; Emmolo, I.; Frasoldati, A.; Gianotti, L.; Guglielmi, R.; Piovesan, A.; Procopio, M.; Scillitani, A.; et al. AME position statement: Primary hyperparathyroidism in clinical practice. J. Endocrinol. Investig. 2012, 35 (Suppl. S7), 2–21. [Google Scholar]
- Walker, M.D.; Cong, E.; Lee, J.A.; Kepley, A.; Zhang, C.; McMahon, D.J.; Silverberg, S.J. Vitamin D in Primary Hyperparathyroidism: Effects on Clinical, Biochemical, and Densitometric Presentation. J. Clin. Endocrinol. Metab. 2015, 100, 3443–3451. [Google Scholar] [CrossRef]
- Silverberg, S.J.; Clarke, B.L.; Peacock, M.; Bandeira, F.; Boutroy, S.; Cusano, N.E.; Dempster, D.; Lewiecki, E.M.; Liu, J.M.; Minisola, S.; et al. Current issues in the presentation of asymptomatic primary hyperparathyroidism: Proceedings of the Fourth International Workshop. J. Clin. Endocrinol. Metab. 2014, 99, 3580–3594. [Google Scholar] [CrossRef]
- Delos Santos, R.; Rossi, A.; Coyne, D.; Maw, T.T. Management of Post-transplant Hyperparathyroidism and Bone Disease. Drugs 2019, 79, 501–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sushilkumar, S.; Guleria, S.; Crowe, D.R.; Steenwyk, B.; Singh, S. Progressive Lung Calcification after Orthotopic Heart Transplant. Pediatric Radiol. 2015, 45, 124–128. [Google Scholar] [CrossRef]
- Caffarelli, C.; Tomai Pitinca, M.D.; Alessandri, M.; Cameli, P.; Bargagli, E.; Bennett, D.; Fossi, A.; Bernazzali, S.; Gonnelli, S. Timing of Osteoporotic Vertebral Fractures in Lung and Heart Transplantation: A Longitudinal Study. J. Clin. Med. 2020, 9, 2941. [Google Scholar] [CrossRef] [PubMed]
- Kulak, C.A.M.; Borba, V.Z.C.; Junior, J.K.; Custodio, M.R. Bone disease after transplantation: Osteoporosis and fractures risk. Arq. Bras. Endocrinol. Metabol. 2014, 58, 484–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sambrook, P.; Henderson, N.K.; Keogh, A.; MacDonald, P.; Glanville, A.; Spratt, P.; Bergin, P.; Ebeling, P.; Eisman, J. Effect of calcitriol on bone loss after cardiac or lung transplantation. J. Bone Miner Res. 2000, 15, 1818–1824. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Delgado, I.; Prieto, S.; Gil-Fraguas, L.; Robles, E.; Rufilanchas, J.J.; Hawkins, F. Calcitonin, etidronate, and calcidiol treatment in bone loss after cardiac transplantation. Calcif. Tissue Int. 1997, 60, 155–159. [Google Scholar] [CrossRef]
- Chokshi, A.; Cheema, F.H.; Schaefle, K.J.; Jiang, J.; Collado, E.; Shahzad, K.; Khawaja, T.; Farr, M.; Takayama, H.; Naka, Y.; et al. Hepatic dysfunction and survival after orthotopic heart transplantation: Application of the MELD scoring system for outcome prediction. J. Heart Lung Transplant. 2012, 31, 591–600. [Google Scholar] [CrossRef] [Green Version]
- Zittermann, A.; Ernst, J.B.; Prokop, S.; Fuchs, U.; Berthold, H.K.; Gouni-Berthold, I.; Gummert, J.F.; Pilz, S. A 3 year post-intervention follow-up on mortality in advanced heart failure (EVITA vitamin D supplementation trial). ESC Heart Fail. 2020, 7, 3754–3761. [Google Scholar] [CrossRef] [PubMed]
- Barbarawi, M.; Kheiri, B.; Zayed, Y.; Barbarawi, O.; Dhillon, H.; Swaid, B.; Yelangi, A.; Sundus, S.; Bachuwa, G.; Alkotob, M.L.; et al. Vitamin D Supplementation and Cardiovascular Disease Risks in More Than 83,000 Individuals in 21 Randomized Clinical Trials: A Meta-analysis. JAMA Cardiol. 2019, 4, 765–776. [Google Scholar] [CrossRef]
- Bhandari, R.; Malvar, J.; Sacapano, A.; Aguayo-Hiraldo, P.; Jodele, S.; Orgel, E. Association between Vitamin D and Risk for Early and Late Post-Transplant Complications. Biol. Blood Marrow Transplant. 2020, 26, 343–350. [Google Scholar] [CrossRef]
- Bienaimé, F.; Girard, D.; Anglicheau, D.; Canaud, G.; Claude Souberbielle, J.; Kreis, H.; Noël, L.; Friedlander, G.; Elie, C.; Legendre, C.; et al. Vitamin D Status and Outcomes After Renal Transplantation. JASN 2013, 24, 831–841. [Google Scholar] [CrossRef]
- Thorsen, I.S.; Bleskestad, I.H.; Åsberg, A.; Hartmann, A.; Skadberg, Ø.; Brede, C.; Ueland, T.; Pasch, A.; Reisaeter, A.V.; Gøransson, L.G. Vitamin D as a risk factor for patient survival after kidney transplantation: A prospective observational cohort study. Clin. Transplant. 2019, 33, e13517. [Google Scholar] [CrossRef] [Green Version]
- Cubbon, R.M.; Lowry, J.E.; Drozd, M.; Hall, M.; Gierula, J.; Paton, M.F.; Byrom, R.; Kearney, L.C.; Barth, J.H.; Kearney, M.T.; et al. Vitamin D deficiency is an independent predictor of mortality in patients with chronic heart failure. Eur. J. Nutr. 2019, 58, 2535–2543. [Google Scholar] [CrossRef] [Green Version]
- Wallace, G.; Jodele, S.; Howell, J.; Myers, K.C.; Teusink, A.; Zhao, X.; Setchell, K.; Holtzapfel, C.; Lane, A.; Taggart, C.; et al. Vitamin D Deficiency and Survival in Children after Hematopoietic Stem Cell Transplant. Biol. Blood Marrow Transplant. 2015, 21, 1627–1631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foroutan, F.; Doumouras, B.S.; Ross, H.; Alba, A.C. Impact of pretransplant recipient body mass index on post heart transplant mortality: A systematic review and meta-analysis. Clin. Transplant. 2018, 32, e13348. [Google Scholar] [CrossRef] [PubMed]
- Doumouras, B.S.; Fan, C.S.; Dipchand, A.I.; Manlhiot, C.; Stehlik, J.; Ross, H.J.; Alba, A.C. The effect of pre-heart transplant obesity on post-transplant mortality: Analysis of the ISHLT registry data. J. Heart Lung Transplant. 2017, 36, S190. [Google Scholar] [CrossRef]
- Nagendran, J.; Moore, M.; Norris, C.; Khani-Hanjani, A.; Graham, M.M.; Freed, D.H. The varying effects of obesity and morbid obesity on outcomes following cardiac transplantation. Int. J. Obes. 2016, 40, 721–724. [Google Scholar] [CrossRef]
- Paschou, S.A.; Kosmopoulos, M.; Nikas, I.P.; Spartalis, M.; Kassi, E.; Goulis, D.G.; Lambrinoudaki, I.; Siasos, G. The Impact of Obesity on the Association between Vitamin D Deficiency and Cardiovascular Disease. Nutrients 2019, 11, 2458. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 96) | Men (n = 71) | Women (n = 25) | p-Value |
|---|---|---|---|---|
| Age (Years) | 36.17 ± 13.53 | 39.84 ± 12.22 | 32.35 ± 9.31 | 0.031 |
| Height (cm) | 165.33 ± 9.02 | 168.56 ± 7.57 | 156.16 ± 6.02 | <0.001 |
| Weight (kg) | 65.05 ± 17.29 | 69.68 ± 15.87 | 51.90 ± 14.31 | <0.001 |
| BMI (kg/m2) | 23.62 ± 5.37 | 24.50 ± 5.21 | 21.12 ± 5.11 | 0.006 |
| BMD lumbar spine (gm/cm2) | 1.05 ± 0.16 | 1.07 ± 0.16 | 0.95 ± 0.11 | 0.041 |
| Lumbar spine Z-score | −0.31 ± 1.10 | −0.25 ± 1.15 | −0.48 ± 0.96 | 0.380 |
| BMD femoral neck (gm/ cm2) | 0.59 ± 0.49 | 0.67 ± 0.48 | 0.38 ± 0.45 | 0.012 |
| Femoral neck Z-score | −0.10 ± 0.91 | −0.04 ± 0.99 | −0.26 ± 0.60 | 0.293 |
| 25OHVD (nmol/L) | 27.80 ± 23.78 | 27.72 ± 24.63 | 28.04 ± 21.63 | 0.954 |
| Vitamin D3 (nmol/L) | 14.82 ± 14.73 | 15.23 ± 13.63 | 13.68 ± 17.76 | 0.654 |
| Intact parathyroid h. (mmol/L) | 78.15 ± 65.13 | 80.17 ± 61.88 | 72.40 ± 74.67 | 0.611 |
| ALP (U/L) | 96.07 ± 78.76 | 99.97 ± 80.56 | 84.98 ± 73 | 0.416 |
| Calcium (mmol/L) | 2.22 ± 0.18 | 2.20 ± 0.18 | 2.28 ± 0.19 | 0.054 |
| Phosphate (mmol/L) | 1.14 ± 0.34 | 1.15 ± 0.34 | 1.11 ± 0.35 | 0.600 |
| Mg (mmol/L) | 0.95 ± 0.55 | 0.86 ± 0.17 | 1.19 ± 1.02 | 0.011 |
| Creatinine (umol/L) | 91.14 ± 36.80 | 96.01 ± 36.14 | 77.32 ± 35.83 | 0.028 |
| Urea (mmol/L) | 10.14 ± 6.59 | 10.71 ± 5.75 | 8.50 ± 8.45 | 0.149 |
| Sodium (mmol/L) | 136.67 ± 6.43 | 136.04 ± 5.87 | 138.44 ± 7.63 | 0.110 |
| Potassium (mmol/L) | 4.05 ± 0.57 | 4.03 ± 0.56 | 4.10 ± 0.60 | 0.571 |
| Chloride (mmol/L) | 97.62 ± 6.89 | 96.52 ± 6.24 | 100.64 ± 7.80 | 0.010 |
| Variables | Male (n = 60) | p-Value † | Female (n = 15) | p-Value † | ||||
|---|---|---|---|---|---|---|---|---|
| Pre-Transplant Mean ± SD | 1-Y Post-Transplant Mean ± SD | 2-Y Post-Transplant Mean ± SD | Pre-Transplant Mean ± SD | 1-Y Post-Transplant Mean ± SD | 2-Y Post-Transplant Mean ± SD | |||
| Weight (kg) | 70.08 ± 13.24 a,* | 76.95 ± 14.95 b,* | 89.03 ± 12.40 b,* | <0.001 | 52.41 ± 12.56 a | 61.89 ± 17.61 b | 64.35 ± 18.97 b | 0.015 |
| BMI (kg/m2) | 24.75 ± 4.43 a | 26.85 ± 5.37 b,* | 27.21 ± 5.15 b | 0.011 | 21.46 ± 5.20 a | 24.86 ± 6.52 b | 26.27 ± 7.27 b | 0.021 |
| DEXA parameters | ||||||||
| BMD lumbar spine (gm/cm2) | 1.07 ± 0.16 a,* | 1.02 ± 0.17 a,* | 0.99 ± 0.27 a,* | 0.231 | 0.95 ± 0.11 a | 0.93 ± 0.09 a | 1.09 ± 0.17 a | 0.247 |
| Lumbar spine Z-score | −0.28 ± 1.49 a | −0.66 ± 1.39 b,* | −0.50 ± 1.47 a | 0.019 | −0.12 ± 0.99 a | −1.02 ± 0.59 b | −0.80 ± 1.10 a | 0.016 |
| BMD femoral neck (gm/cm2) | 0.88 ± 0.33 a | 0.75 ± 0.35 b,* | 0.87 ± 0.25 a | 0.012 | 0.91 ± 0.12 a | 0.66 ± 0.38 a | 0.90 ± 0.13 a | 0.268 |
| Femoral neck Z-score | −0.09 ± 1.33 a,* | −0.56 ± 1.22 b,* | −0.47 ± 1.18 a,* | 0.106 | −0.10 ± 0.61 a | −0.78 ± 0.75 b | −0.36 ± 0.62 a | 0.007 |
| Biochemical parameters | ||||||||
| 25OHVD (nmol/L) | 22.07 ± 22.02 a | 54.79 ± 31.13 b,* | 70.05 ± 27.58 b,* | <0.001 | 27.20 ± 20.13 a | 37.80 ± 24.36 a | 58.20 ± 27.69 a | 0.143 |
| Vitamin D3 (nmol/L) | 17.07 ± 14.36 a | 40.44 ± 25.43 b,* | 64.00 ± 25.06 c | <0.001 | 17.80 ± 18.83 a | 32.47 ± 19.65 a | 51.21 ± 25.19 a | 0.145 |
| Intact parathyroid h (pmol/L) | 77.40 ± 53.88 a,* | 30.85 ± 39.41 b,* | 86.09 ± 35.36 c | 0.013 | 98.67 ± 55.93 a | 102.80 ± 18.10 a | 126.25 ± 61.1 b | 0.015 |
| ALP (U/L) | 103.70 ± 42.42 a,* | 94.55 ± 42.85 a,* | 81.71 ± 29.10 b | 0.026 | 89.00 ± 40.14 a | 65.00 ± 12.63 a | 63.80 ± 4.55 a | 0.449 |
| Calcium (mmol/L) | 2.18 ± 0.14 a,* | 2.26 ± 0.11 b,* | 2.27 ± 0.9 b,* | 0.024 | 2.25 ± 0.12 a | 2.17 ± 0.04 a | 2.02 ± 0.50 a | 0.449 |
| Phosphate (mmol/L) | 1.10 ± 0.30 a,* | 1.12 ± 0.18 a,* | 1.07 ± 0.16 a | 0.314 | 1.00 ± 0.44 a | 1.09 ± 0.25 a | 1.01 ± 0.34 a | 0.531 |
| Mg (mmol/L) | 0.88 ± 0.12 a,* | 0.72 ± 0.10 b | 0.64 ± 0.18 b | <0.001 | 0.91 ± 0.11 a | 0.71 ± 0.16 a | 0.62 ± 0.05 a | 0.074 |
| Creatinine (umol/L) | 95.85 ± 35.06 a,* | 108.25 ± 52.63 a,* | 95.67 ± 23.88 b | 0.819 | 79.00 ± 23.36 a | 80.40 ± 31.30 a | 79.00 ± 24.22 a | 0.437 |
| Urea (mmol/L) | 10.00 ± 6.33 a,* | 7.30 ± 3.04 b,* | 9.01 ± 10.55 b | 0.030 | 7.60 ± 3.21 a | 7.28 ± 2.82 a | 6.38 ± 1.63 a | 0.819 |
| Sodium (mmol/L) | 135.10 ± 7.40 a,* | 141.3 ± 2.92 a | 140.02 ± 3.44 a | 0.051 | 139.86 ± 9.21 a | 140.43 ± 2.23 a | 145.05 ± 4.34 a | 0.869 |
| Potassium (mmol/L) | 4.07 ± 0.64 a,* | 4.11 ± 0.35 a,* | 4.10 ± 0.15 a | 0.600 | 4.21 ± 0.58 a | 4.31 ± 0.40 a | 4.19 ± 0.39 a | 0.725 |
| Chloride (mmol/L) | 95.45 ± 7.57 a,* | 104.45 ± 3.44 b | 99.33 ± 4.90 a | 0.031 | 104.14 ± 8.21 a | 105.57 ± 2.37 a | 102.90 ± 4.32 a | 0.625 |
| Variables | Group I; 25OHVD < 25 nmol/L (n = 54) | p-Value † | Group II; 25OHVD ≥ 25 nmol/L (n = 21) | p-Value † | ||||
|---|---|---|---|---|---|---|---|---|
| Pre-Transplant Mean ± SD | 1-y Post-Transplant Mean ± SD | 2-y Post-Transplant Mean ± SD | Pre-Transplant Mean ± SD | 1-y Post-Transplant Mean ± SD | 2-y Post-Transplant Mean ± SD | |||
| Weight (kg) | 64.55 ± 9.22 a | 68.67 ± 12.04 b,* | 70.89 ± 9.67 b,* | 0.035 | 74.57 ± 26.57 a | 83.39 ± 17.79 b | 86.99 ± 19.35 b | 0.057 |
| BMI (kg/m2) | 23.42 ± 3.63 a | 24.92 ± 4.58 b,* | 26.21 ± 5.02 b,* | 0.037 | 27.60 ± 7.51 a | 31.17 ± 4.56 a | 32.67 ± 3.47 a | 0.063 |
| DEXA parameters | ||||||||
| BMD lumbar spine (gm/cm2) | 1.04 ± 0.14 a | 1.01 ± 0.16 a | 0.98 ± 0.26 a | 0.179 | 1.09 ± 0.15 a | 0.83 ± 0.11 a | 1.01 ± 0.16 a | 0.207 |
| Lumbar spine Z-score | −0.19 ± 1.43 a | −0.69 ± 1.28 b | −0.45 ± 1.20 a | 0.002 | −0.40 ± 1.37 a | −0.84 ± 1.33 a | −0.86 ± 1.86 a | 0.368 |
| BMD femoral neck (gm/cm2) | 0.86 ± 0.33 a | 0.71 ± 0.34 b | 0.85 ± 0.25 b | 0.001 | 0.96 ± 0.17 a | 0.79 ± 0.38 a | 0.97 ± 0.13 a | 0.867 |
| Femoral neck Z-score | −0.06 ± 1.09 a | −0.73 ± 0.96 b | −0.49 ± 1.00 a | 0.001 | −0.17 ± 1.58 a | −0.27 ± 1.52 a | −0.34 ± 1.35 a | 0.867 |
| Biochemical parameters | ||||||||
| 25OHVD (nmol/L) | 11.52 ± 6.49 a,* | 48.49 ± 27.11 b | 64.00 ± 22.23 b | <0.001 | 52.86 ± 16.41 a | 58.86 ± 38.52 a | 77.14 ± 38.33 a | 0.368 |
| Vitamin D3 (nmol/L) | 10.97 ± 5.84 a,* | 41.43 ± 24.84 b | 57.67 ± 16.67 b | <0.001 | 33.29 ± 19.35 a | 32.19 ± 22.96 a | 76.14 ± 38.06 b | 0.032 |
| Intact parathyroid h (pmol/L) | 63.50 ± 51.29 a | 23.89 ± 39.54 a | 91.64 ± 43.51 b | 0.002 | 83.86 ± 58.24 a | 37.86 ± 35.92 a | 100.48 ± 45.78 a | 0.368 |
| ALP (U/L) | 91.28 ± 35.60 a | 79.39 ± 26.70 a | 71.01 ± 13.56 a | 0.056 | 125.14 ± 48.61 a | 112.43 ± 59.71 a | 96.43 ± 42.96 a | 0.066 |
| Calcium (mmol/L) | 2.16 ± 0.11 a,* | 2.26 ± 0.99 b | 2.25 ± 0.93 b | 0.016 | 2.27 ± 0.17 a | 2.18 ± 0.12 a | 2.15 ± 0.45 a | 0.565 |
| Phosphate (mmol/L) | 1.14 ± 0.33 a | 1.11 ± 0.22 a | 1.05 ± 0.17 a | 0.454 | 1.10 ± 0.27 a | 1.14 ± 0.25 a | 1.11 ± 0.30 a | 0.867 |
| Mg (mmol/L) | 0.88 ± 0.10 a | 0.72 ± 0.12 b | 0.62 ± 0.17 b | <0.001 | 0.90 ± 0.14 a | 0.70 ± 0.10 a | 0.68 ± 0.11 a | 0.066 |
| Creatinine (umol/L) | 85.94 ± 28.05 a | 105.83 ± 55.69 a | 89.47 ± 25.01 a | 0.486 | 109.29 ± 41.92 a | 94.57 ± 32.35 a | 99.86 ± 22.70 a | 0.156 |
| Urea (mmol/L) | 8.06 ± 4.25 a | 7.31 ± 3.28 b | 5.93 ± 1.86 b | 0.076 | 13.29 ± 7.97 a | 7.26 ± 2.04 a | 15.06 ± 16.70 a | 0.102 |
| Sodium (mmol/L) | 134.50 ± 6.79 a | 141.44 ± 2.79 a | 143.12 ± 4.14 a | 0.251 | 139.71 ± 7.50 a | 140.43 ± 2.70 a | 143.15 ± 3.36 a | 0.867 |
| Potassium (mmol/L) | 4.04 ± 0.54 a | 4.18 ± 0.33 a | 4.07 ± 0.19 a | 0.600 | 4.29 ± 0.75 a | 4.01 ± 0.42 a | 4.09 ± 0.24 a | 0.867 |
| Chloride (mmol/L) | 95.72 ± 7.64 a | 104.83 ± 3.49 b | 98.29 ± 5.91 a | 0.131 | 98.29 ± 5.47 a | 104.14 ± 2.85 a | 102.97 ± 3.34 a | 0.867 |
| Variables | Group I (25OHVD < 25 nmol/L) | Group II (25OHVD ≥ 25 nmol/L) | ||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |||
| Lower | Upper | Lower | Upper | |||||
| Age | 0.962 | 0.888 | 1.042 | 0.345 | 0.869 | 0.696 | 1.086 | 0.218 |
| BMI | 1.327 | 1.015 | 1.733 | 0.038 | 1.145 | 1.756 | 1.734 | 0.524 |
| Normal BMD at LS | Reference | Reference | ||||||
| Osteopenia at LS | 0.342 | 0.000 | 77,594.19 | 0.865 | 0.008 | 0.000 | - | 0.995 |
| Osteoporosis at LS | 0.000 | 0.000 | - | 0.995 | 0.000 | 0.000 | - | 0.995 |
| Normal BMD at FN | Reference | Reference | ||||||
| Osteopenia at FN | 0.538 | 0.000 | 123,625.63 | 0.922 | 0.004 | 0.000 | - | 0.994 |
| Osteoporosis at FN | 0.000 | 0.000 | - | 0.996 | 0.382 | 0.000 | - | 0.999 |
| VD3 serum level | 0.916 | 0.712 | 1.179 | 0.497 | 0.958 | 0.868 | 1.058 | 0.394 |
| 25OHVD serum level | 0.930 | 0.681 | 1.270 | 0.648 | 0.345 | 0.650 | 1.163 | 0.345 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abulmeaty, M.M.A.; Almutawa, D.A.; Selimovic, N.; Almuammar, M.; Al-Khureif, A.A.; Hashem, M.I.; Hassan, H.M.; Moety, D.A.A. Impact of Vitamin D Supplementation on Bone Mineral Density and All-Cause Mortality in Heart Transplant Patients. Biomedicines 2021, 9, 1450. https://doi.org/10.3390/biomedicines9101450
Abulmeaty MMA, Almutawa DA, Selimovic N, Almuammar M, Al-Khureif AA, Hashem MI, Hassan HM, Moety DAA. Impact of Vitamin D Supplementation on Bone Mineral Density and All-Cause Mortality in Heart Transplant Patients. Biomedicines. 2021; 9(10):1450. https://doi.org/10.3390/biomedicines9101450
Chicago/Turabian StyleAbulmeaty, Mahmoud M. A., Deema A. Almutawa, Nedim Selimovic, May Almuammar, Abdulaziz A. Al-Khureif, Mohamed I. Hashem, Heba M. Hassan, and Doaa A. Abdel Moety. 2021. "Impact of Vitamin D Supplementation on Bone Mineral Density and All-Cause Mortality in Heart Transplant Patients" Biomedicines 9, no. 10: 1450. https://doi.org/10.3390/biomedicines9101450