Clinical Significance of Preoperative Inflammatory Markers in Prediction of Prognosis in Node-Negative Colon Cancer: Correlation between Neutrophil-to-Lymphocyte Ratio and Poorly Differentiated Clusters

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
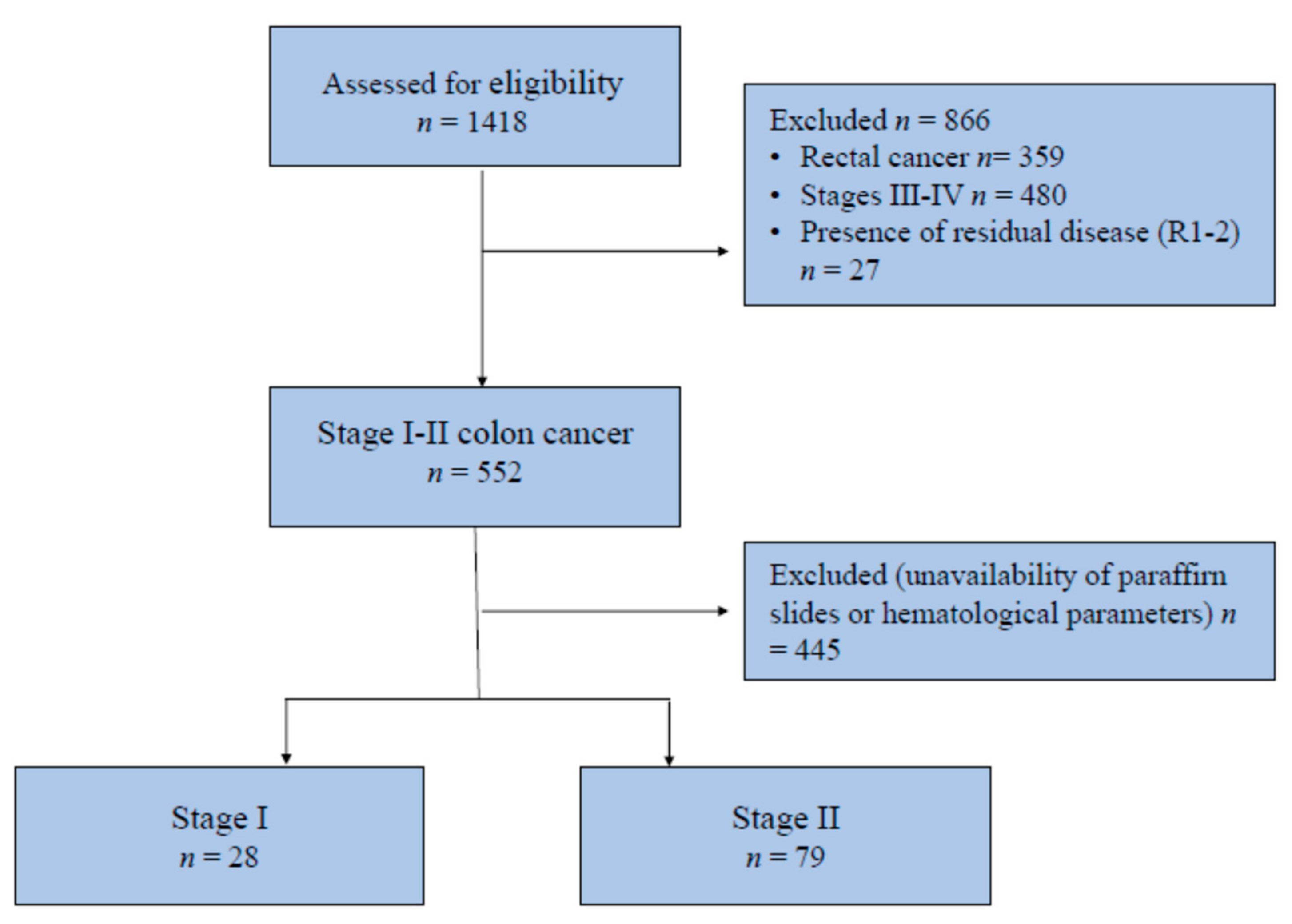
2.1. Inclusion Criteria and Population under Study
2.2. Assessment of Inflammatory Markers
2.3. Histological Evaluation
2.4. Preoperative Work-Up and Surgical Technique
2.5. Data Collection and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mattiuzzi, C.; Sanchis-Gomar, F.; Lippi, G. Concise update on colorectal cancer epidemiology. Ann. Transl. Med. 2019, 7, 609. [Google Scholar] [CrossRef]
- Poornakala, S.; Prema, N. A study of morphological prognostic factors in colorectal cancer and survival analysis. Indian J. Pathol. Microbiol. 2019, 62, 36–42. [Google Scholar] [CrossRef]
- Chi, Z.; Li, Z.; Cheng, L.; Wang, C. Comparison of long-term outcomes after laparoscopic-assisted and open colectomy for splenic flexure cancer. J. BUON 2018, 23, 322–328. [Google Scholar]
- Micu, B.V.; Vesa, Ş.C.; Pop, T.R.; Micu, C.M. Evaluation of prognostic factors for 5 year-survival after surgery for colorectal cancer. Ann. Ital. Chir. 2020, 91, 41–48. [Google Scholar]
- Guo, T.A.; Wu, Y.C.; Tan, C.; Jin, Y.T.; Sheng, W.Q.; Cai, S.J.; Liu, F.Q.; Xu, Y. Clinicopathologic features and prognostic value of KRAS, NRAS and BRAF mutations and DNA mismatch repair status: A single-center retrospective study of 1834 Chinese patients with Stage I–IV colorectal cancer. Int. J. Cancer 2019, 145, 1625–1634. [Google Scholar] [CrossRef] [Green Version]
- Osterman, E.; Glimelius, B. Recurrence risk after up-to-date colon cancer staging, surgery, and pathology: Analysis of the entire Swedish population. Dis. Colon Rectum 2018, 61, 1016–1025. [Google Scholar] [CrossRef]
- Mazaki, J.; Katsumata, K.; Kasahara, K.; Tago, T.; Wada, T.; Kuwabara, H.; Enomoto, M.; Ishizaki, T.; Nagakawa, Y.; Tsuchida, A. Neutrophil-to-lymphocyte ratio is a prognostic factor for colon cancer: A propensity score analysis. BMC Cancer 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Chen, J.H.; Zhai, E.T.; Yuan, Y.J.; Wu, K.M.; Xu, J.B.; Peng, J.J.; Chen, C.Q.; He, Y.L.; Cai, S.R. Systemic immune-inflammation index for predicting prognosis of colorectal cancer. World J. Gastroenterol. 2017, 23, 6261–6272. [Google Scholar] [CrossRef]
- Shibutani, M.; Maeda, K.; Nagahara, H.; Ohtani, H.; Sakurai, K.; Yamazoe, S.; Kimura, K.; Toyokawa, T.; Amano, R.; Kubo, N.; et al. Significance of markers of systemic inflammation for predicting survival and chemotherapeutic outcomes and monitoring tumor progression in patients with unresectable metastatic colorectal cancer. Anticancer Res. 2015, 35, 5037–5046. [Google Scholar]
- Pedrazzani, C.; Mantovani, G.; Fernandes, E.; Bagante, F.; Luca Salvagno, G.; Surci, N.; Campagnaro, T.; Ruzzenente, A.; Danese, E.; Lippi, G.; et al. Assessment of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio and platelet count as predictors of long-term outcome after R0 resection for colorectal cancer. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Pedrazzani, C.; Turri, G.; Mantovani, G.; Conti, C.; Ziello, R.; Conci, S.; Campagnaro, T.; Ruzzenente, A.; Guglielmi, A. Prognostic value of thrombocytosis in patients undergoing surgery for colorectal cancer with synchronous liver metastases. Clin. Transl. Oncol. 2019, 21, 1644–1653. [Google Scholar] [CrossRef]
- Kosuga, T.; Konishi, T.; Kubota, T.; Shoda, K.; Konishi, H.; Shiozaki, A.; Okamoto, K.; Fujiwara, H.; Kudou, M.; Arita, T.; et al. Clinical significance of neutrophil-to-lymphocyte ratio as a predictor of lymph node metastasis in gastric cancer. BMC Cancer 2019, 19, 1187. [Google Scholar] [CrossRef] [Green Version]
- Yin, X.; Wu, L.; Yang, H.; Yang, H.B. Prognostic significance of neutrophil-lymphocyte ratio (NLR) in patients with ovarian cancer: A systematic review and meta-analysis. Medicine (Baltimore) 2019, 98, e17475. [Google Scholar] [CrossRef]
- Hasegawa, T.; Iga, T.; Takeda, D.; Amano, R.; Saito, I.; Kakei, Y.; Kusumoto, J.; Kimoto, A.; Sakakibara, A.; Akashi, M. Neutrophil-lymphocyte ratio associated with poor prognosis in oral cancer: A retrospective study. BMC Cancer 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Inamoto, S.; Kawada, K.; Okamura, R.; Hida, K.; Sakai, Y. Prognostic impact of the combination of neutrophil-to-lymphocyte ratio and Glasgow prognostic score in colorectal cancer: A retrospective cohort study. Int. J. Colorectal Dis. 2019, 34, 1303–1315. [Google Scholar] [CrossRef]
- Silva, T.H.; Schilithz, A.O.C.; Peres, W.A.F.; Murad, L.B. Neutrophil-lymphocyte ratio and nutritional status are clinically useful in predicting prognosis in colorectal cancer patients. Nutr. Cancer 2020, 72, 1345–1354. [Google Scholar] [CrossRef]
- Cruz-Ramos, M.; del Puerto-Nevado, L.; Zheng, B.; López-Bajo, R.; Cebrian, A.; Rodríguez-Remirez, M.; García-García, L.; Solanes-Casado, S.; García-Foncillas, J. Prognostic significance of neutrophil-to lymphocyte ratio and platelet-to lymphocyte ratio in older patients with metastatic colorectal cancer. J. Geriatr. Oncol. 2019, 10, 742–748. [Google Scholar] [CrossRef]
- Xia, L.J.; Li, W.; Zhai, J.C.; Yan, C.W.; Chen, J.B.; Yang, H. Significance of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, lymphocyte-to-monocyte ratio and prognostic nutritional index for predicting clinical outcomes in T1-2 rectal cancer. BMC Cancer 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Dell’Aquila, E.; Cremolini, C.; Zeppola, T.; Lonardi, S.; Bergamo, F.; Masi, G.; Stellato, M.; Marmorino, F.; Schirripa, M.; Urbano, F.; et al. Prognostic and predictive role of neutrophil/lymphocytes ratio in metastatic colorectal cancer: A retrospective analysis of the TRIBE study by GONO. Ann. Oncol. 2018, 29, 924–930. [Google Scholar] [CrossRef]
- Malietzis, G.; Giacometti, M.; Askari, A.; Nachiappan, S.; Kennedy, R.H.; Faiz, O.D.; Aziz, O.; Jenkins, J.T. A preoperative neutrophil to lymphocyte ratio of 3 predicts disease-free survival after curative elective colorectal cancer surgery. Ann. Surg. 2014, 260, 287–292. [Google Scholar] [CrossRef]
- Li, Y.; Jia, H.; Yu, W.; Xu, Y.; Li, X.; Li, Q.; Cai, S. Nomograms for predicting prognostic value of inflammatory biomarkers in colorectal cancer patients after radical resection. Int. J. Cancer 2016, 139, 220–231. [Google Scholar] [CrossRef] [Green Version]
- Haram, A.; Boland, M.R.; Kelly, M.E.; Bolger, J.C.; Waldron, R.M.; Kerin, M.J. The prognostic value of neutrophil-to-lymphocyte ratio in colorectal cancer: A systematic review. J. Surg. Oncol. 2017, 115, 470–479. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, H.-Y.; Li, J.; Shao, X.-Y.; Zhang, C.-X. The elevated NLR, PLR and PLT may predict the prognosis of patients with colorectal cancer: A systematic review and meta-analysis. Oncotarget 2017, 8, 68837–68846. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.Z.; Chen, W.J.; Zhang, X.; Wu, C.C.; Zhang, C.Y.; Sun, S.S.; Wu, J. An Elevated Platelet-to-Lymphocyte Ratio Predicts Poor Prognosis and Clinicopathological Characteristics in Patients with Colorectal Cancer: A Meta-Analysis. Dis. Markers 2017, 2017, 1053125. [Google Scholar] [CrossRef]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; Fletcher, C.D.; O’reilly, D.S.J.; Foulis, A.K.; Horgan, P.G.; Mcmillan, D.C. A comparison of inflammation-based prognostic scores in patients with cancer. A Glasgow Inflammation Outcome Study. Eur. J. Cancer 2011, 47, 2633–2641. [Google Scholar] [CrossRef]
- Lee, Y.S.; Suh, K.W.; Oh, S.Y. Preoperative thrombocytosis predicts prognosis in stage II colorectal cancer patients. Ann. Surg. Treat. Res. 2016, 90, 322–327. [Google Scholar] [CrossRef] [Green Version]
- Rao, X.-D.; Zhang, H.; Xu, Z.-S.; Cheng, H.; Shen, W.; Wang, X.-P. Poor prognostic role of the pretreatment platelet counts in colorectal cancer. Medicine (Baltimore) 2018, 97, e10831. [Google Scholar] [CrossRef]
- Schmoll, H.J.; Van Cutsem, E.; Stein, A.; Valentini, V.; Glimelius, B.; Haustermans, K.; Nordlinger, B.; Van De Velde, C.J.; Cervantes, A. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann. Oncol. 2012, 23, 2479–2516. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. NCCN Guidelines® Insights Colon Cancer, Version 2.2018 Featured Updates to the NCCN Guidelines. J. Natl. Compr. Cancer Netw. 2018, 16, 359–369. [Google Scholar] [CrossRef] [Green Version]
- Japanese Society for Cancer of the Colon and Rectum. Japanese Classification of Colorectal, Appendiceal, and Anal Carcinoma: The 3d English Edition [Secondary Publication]. J. Anus Rectum Colon 2019, 3, 175–195. [Google Scholar] [CrossRef] [Green Version]
- Ryan, É.; Khaw, Y.L.; Creavin, B.; Geraghty, R.; Ryan, E.J.; Gibbons, D.; Hanly, A.; Martin, S.T.; O’Connell, P.R.; Winter, D.C.; et al. Tumor Budding and PDC Grade Are Stage Independent Predictors of Clinical Outcome in Mismatch Repair Deficient Colorectal Cancer. Am. J. Surg. Pathol. 2018, 42, 60–68. [Google Scholar] [CrossRef]
- Ammendola, S.; Turri, G.; Marconi, I.; Burato, G.; Pecori, S.; Tomezzoli, A.; Conti, C.; Pedrazzani, C.; Barresi, V. The presence of poorly differentiated clusters predicts survival in stage II colorectal cancer. Virchows Arch. 2020, 1–8. [Google Scholar] [CrossRef]
- Shivji, S.; Conner, J.R.; Barresi, V.; Kirsch, R. Poorly differentiated clusters in colorectal cancer: A current review and implications for future practice. Histopathology 2020, 77, 351–368. [Google Scholar] [CrossRef]
- Konishi, T.; Shimada, Y.; Lee, L.H.; Cavalcanti, M.S.; Hsu, M.; Smith, J.J.; Nash, G.M.; Temple, L.K.; Guillem, J.G.; Paty, P.B.; et al. Poorly Differentiated Clusters Predict Colon Cancer Recurrence. Am. J. Surg. Pathol. 2018, 42, 705–714. [Google Scholar] [CrossRef]
- Amin, M.; Edge, S.B.; Greene, F. AJCC Cancer Staging Manual, 8th ed.; Springer: Berlin/Heidelberg, Germany, 2017; Volume 14. [Google Scholar]
- Pedrazzani, C.; Tripepi, M.; Turri, G.; Fernandes, E.; Scotton, G.; Conci, S.; Campagnaro, T.; Ruzzenente, A.; Guglielmi, A. Prognostic value of red cell distribution width (RDW) in colorectal cancer. Results from a single-center cohort on 591 patients. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Pedrazzani, C.; Lauka, L.; Sforza, S.; Ruzzenente, A.; Nifosì, F.; Delaini, G.G.; Guglielmi, A. Management of nodal disease from colon cancer in the laparoscopic era. Int. J. Colorectal Dis. 2015, 30, 303–314. [Google Scholar] [CrossRef]
- Kim, C.G.; Ahn, J.B.; Jung, M.; Beom, S.H.; Kim, C.; Kim, J.H.; Heo, S.J.; Park, H.S.; Kim, J.H.; Kim, N.K.; et al. Effects of microsatellite instability on recurrence patterns and outcomes in colorectal cancers. Br. J. Cancer 2016, 115, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Domingo, E.; Camps, C.; Kaisaki, P.J.; Parsons, M.J.; Mouradov, D.; Pentony, M.M.; Makino, S.; Palmieri, M.; Ward, R.L.; Hawkins, N.J.; et al. Mutation burden and other molecular markers of prognosis in colorectal cancer treated with curative intent: Results from the QUASAR 2 clinical trial and an Australian community-based series. Lancet Gastroenterol. Hepatol. 2018, 3, 635–643. [Google Scholar] [CrossRef] [Green Version]
- Rashtak, S.; Ruan, X.; Druliner, B.R.; Liu, H.; Therneau, T.; Mouchli, M.; Boardman, L.A. Peripheral Neutrophil to Lymphocyte Ratio Improves Prognostication in Colon Cancer. Clin. Colorectal Cancer 2017, 16, 115–123. [Google Scholar] [CrossRef]
- Li, M.-X.; Liu, X.-M.; Zhang, X.-F.; Zhang, J.-F.; Wang, W.-L.; Zhu, Y.; Dong, J.; Cheng, J.-W.; Liu, Z.-W.; Ma, L.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in colorectal cancer: A systematic review and meta-analysis. Int. J. Cancer 2014, 134, 2403–2413. [Google Scholar] [CrossRef]
- Wu, Y.; Li, C.; Zhao, J.; Yang, L.; Liu, F.; Zheng, H.; Wang, Z.; Xu, Y. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios predict chemotherapy outcomes and prognosis in patients with colorectal cancer and synchronous liver metastasis. World J. Surg. Oncol. 2016, 14, 289. [Google Scholar] [CrossRef] [Green Version]
- Barresi, V.; Bonetti, L.R.; Branca, G.; Di Gregorio, C.; De Leon, M.P.; Tuccari, G. Colorectal carcinoma grading by quantifying poorly differentiated cell clusters is more reproducible and provides more robust prognostic information than conventional grading. Virchows Arch. 2012, 461, 621–628. [Google Scholar] [CrossRef]
- Jakubowska, K.; Koda, M.; Kisielewski, W.; Kańczuga-Koda, L.; Grudzińska, M.; Famulski, W. Pre- and postoperative neutrophil and lymphocyte count and neutrophil-to-lymphocyte ratio in patients with colorectal cancer. Mol. Clin. Oncol. 2020, 13, 1–10. [Google Scholar] [CrossRef]
- Barresi, V.; Branca, G.; Vitarelli, E.; Tuccari, G. Micropapillary Pattern and Poorly Differentiated Clusters Represent the Same Biological Phenomenon in Colorectal Cancer. Am. J. Clin. Pathol. 2014, 142, 375–383. [Google Scholar] [CrossRef] [Green Version]
- Barresi, V.; Bonetti, L.R.; Leni, A.; Caruso, R.A.; Tuccari, G. Histological grading in colorectal cancer: New insights and perspectives. Histol. Histopathol. 2015, 30, 1059–1067. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Data | H-NLR (n = 45) | p Value | H-PLR (n = 64) | p Value | H-PC (n = 30) | p Value | |
|---|---|---|---|---|---|---|---|
| Age, mean (SD) | 70.5 (14.9) | 0.238 | 70.8 (14.1) | 0.294 | 68.5 (17.5) | 0.846 | |
| Gender, male (%) | 26 (57.7) | 0.844 | 33 (51.6) | 0.321 | 12 (40) | 0.051 | |
| Tumor location (%) | 0.331 | 0.238 | 0.001 | ||||
| Right colon | 25 (55.6) | 35 (54.7) | 23 (76.7) | ||||
| Left colon | 20 (44.4) | 29 (45.3) | 7 (23.3) | ||||
| Elective surgery (%) | 42 (93.3) | 0.307 | 61 (95.3) | 0.647 | 29 (96.7) | 1 | |
| CACI, mean (SD) | 2.9 (1.5) | 0.845 | 3.1 (1.6) | 0.264 | 3.2 (2.0) | 0.389 | |
| Mucinous carcinoma, n (%) | 5 (11.1) | 0.774 | 12 (18.8) | 0.042 | 9 (30) | 0.003 | |
| Depth of tumor invasion, n (%) | 0.036 | 0.055 | 0.081 | ||||
| pT1–2 | 11 (24.4) | 12 (18.7) | 6 (20) | ||||
| pT3 | 20 (44.4) | 36 (56.2) | 14 (46.7) | ||||
| pT4 | 14 (31.2) | 16 (25.1) | 10 (33.3) | ||||
| AJCC TNM Stage II, n (%) | 34 (75.6) | 0.825 | 51 (79.7) | 0.118 | 23 (26.7) | 0.808 | |
| Harvested lymph-nodes ≥ 12, n (%) | 42 (93.3) | 0.731 | 58 (90.6) | 0.738 | 26 (86.7) | 0.264 | |
| Tumor grading, high grade, n (%) | 6 (13.3) | 0.162 | 6 (9.4) | 0.738 | 7 (23.3) | 0.002 | |
| Inflammatory reaction, present, n (%) | 36 (80) | 0.602 | 52 (81.2) | 0.604 | 25 (83.3) | 1 | |
| Budding, high grade, n (%) | 4 (8.9) | 0.446 | 3 (4.7) | 0.636 | 1 (3.3) | 0.063 | |
| LVI present, n (%) | 15 (33.3) | 1 | 19 (29.7) | 0.529 | 12 (40) | 0.362 | |
| PNI present, n (%) | 9 (20) | 0.815 | 14 (21.9) | 1 | 8 (26.7) | 0.439 | |
| PDC present, n (%) | 23 (51.1) | 0.007 | 28 (43.7) | 0.039 | 15 (50) | 0.071 | |
| Data | Pts | OS | p | CSS | p | |
|---|---|---|---|---|---|---|
| Age | ||||||
| ≤median | 45 (42.1%) | 95.6% | 0.009 | 97.7% | 0.521 | |
| >median | 62 (57.9%) | 75.8% | 87.7% | |||
| Gender | ||||||
| Male | 60 (56.1%) | 91.7% | 0.562 | 93% | 0.862 | |
| Female | 47 (43.9%) | 78.7% | 90.9% | |||
| Tumor location | ||||||
| Right colon | 53 (49.5%) | 88.7% | 0.866 | 94% | 0.533 | |
| Left colon | 54 (50.5%) | 79.6% | 90.1% | |||
| TNM Stage | ||||||
| I | 28 (26.2%) | 82.1% | 0.015 | 100% | 0.868 | |
| II | 79 (73.8%) | 84.8% | 89.5% | |||
| Harvested lymph-nodes | ||||||
| <12 | 9 (8.4%) | 66.7% | 0.269 | 87.5% | 0.359 | |
| ≥12 | 98 (91.6%) | 85.7% | 92.5% | |||
| Lympho-vascular invasion | ||||||
| LVI - | 72 (67.3%) | 88.9% | 0.135 | 95.6% | 0.109 | |
| LVI + | 35 (32.7%) | 74.3% | 83.9% | |||
| Perineural invasion | ||||||
| PNI - | 84 (78.5%) | 84.5% | 0.548 | 93.6% | 0.576 | |
| PNI + | 23 (21.5%) | 82.6% | 86.4% | |||
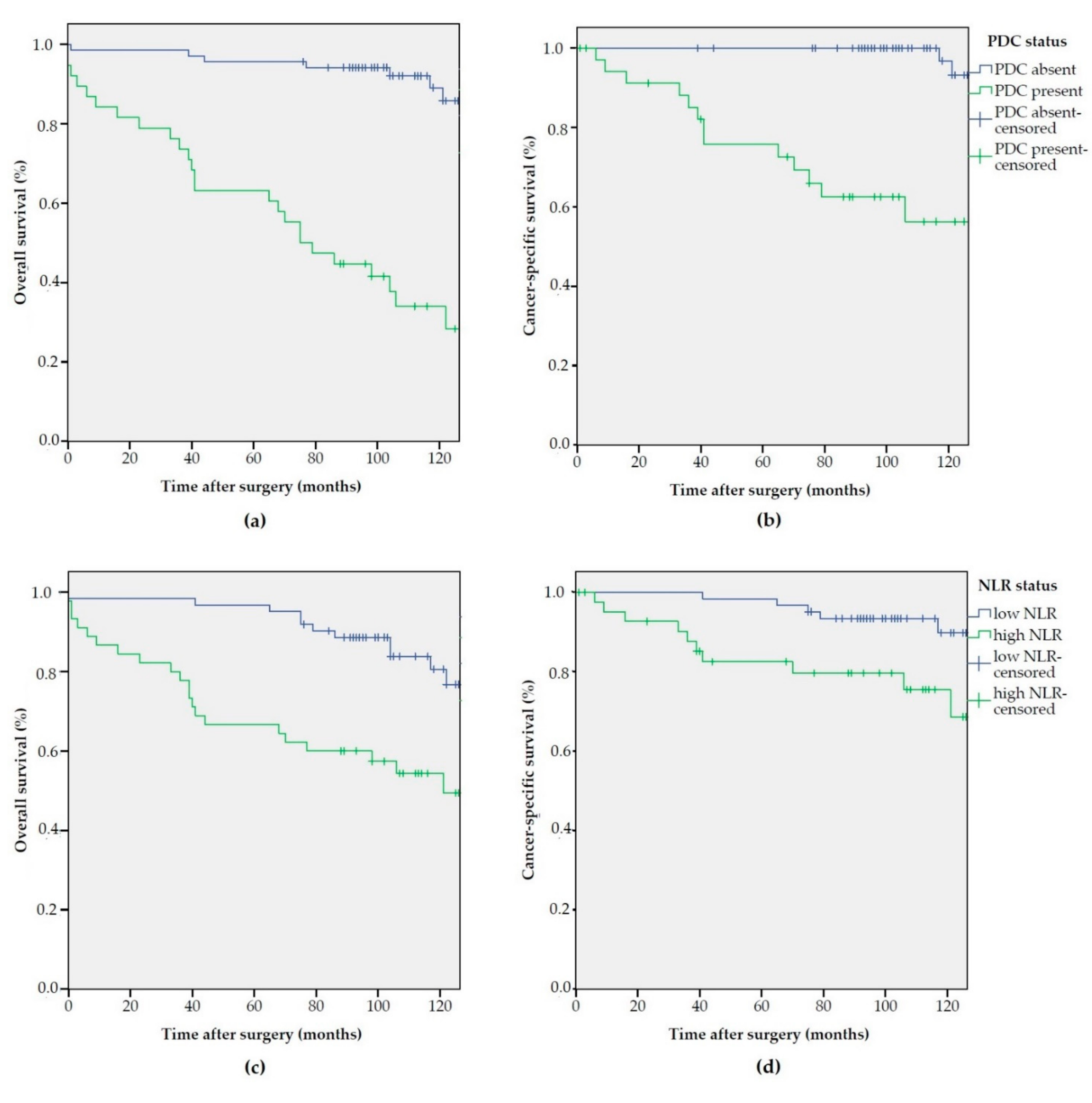
| PDC | ||||||
| Absent | 69 (64.5%) | 95.7% | <0.001 | 100% | <0.001 | |
| Present | 38 (35.5%) | 63.2% | 75.7% | |||
| NLR | ||||||
| L-NLR | 62 (57.9%) | 96.8% | <0.001 | 98.4% | 0.011 | |
| H-NLR | 45 (42.1%) | 66.7% | 82.5% | |||
| PLR | 0.563 | 0.825 | ||||
| L-PLR | 43 (40.2%) | 90.7% | 95.2% | |||
| H-PLR | 64 (59.8%) | 79.7% | 89.8% | |||
| PC | 0.457 | 0.894 | ||||
| L-PC | 77 (72%) | 88.3% | 93.3% | |||
| H-PC | 30 (38%) | 73.3% | 88.6% | |||
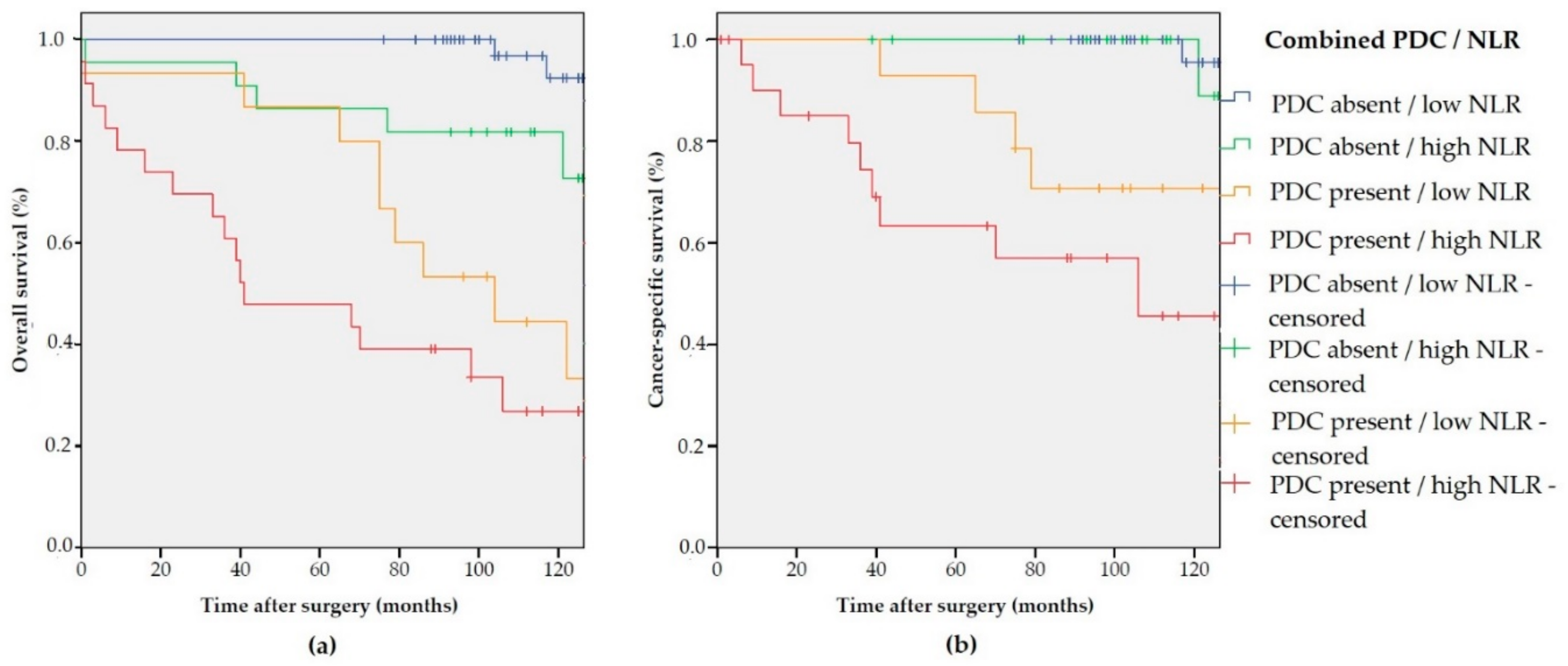
| Combined | ||||||
| PDC absent/L-NLR | 47 (43.9%) | 100% | <0.001 | 100% | <0.001 | |
| PDC absent/H-NLR | 22 (20.6%) | 86.4% | 100% | |||
| PDC present/L-NLR | 15 (14%) | 86.7% | 92.9% | |||
| PDC present/H-NLR | 23 (21.5%) | 47.8% | 63.3% | |||
| Data | OS: HR (95% CI) | p Value | CSS: HR (95% CI) | p Value | |
|---|---|---|---|---|---|
| Age | <0.001 | 0.169 | |||
| ≤median | - | - | |||
| >median | 5.0 (2.07–12.29) | 2.27 (0.71–7.33) | |||
| Gender | 0.303 | 0.920 | |||
| Male | - | - | |||
| Female | 0.67 (0.31–1.44) | 0.94 (0.61–2.06) | |||
| Tumor location | 0.107 | 0.263 | |||
| Right colon | - | - | |||
| Left colon | 2.05 (0.94–4.51) | 1.95 (0.61–6.30) | |||
| Stage | 0.035 | 0.688 | |||
| I | - | - | |||
| II | 0.43 (0.21–0.94) | 1.30 (0.36–4.63) | |||
| NLR | 0.007 | 0.072 | |||
| L-NLR | - | - | |||
| H-NLR | 4.25 (1.77–10.26) | 4.38 (1.25–15.34) | |||
| PDC | <0.001 | <0.001 | |||
| Absent | - | - | |||
| Present | 11.96 (4.70–30.40) | 26.37 (5.30–131.28) | |||
| Data | OS: HR (95% CI) | p Value | CSS: HR (95% CI) | p Value | |
|---|---|---|---|---|---|
| Age | 0.001 | 0.196 | |||
| ≤ median | - | - | |||
| > median | 5.0 (2.07–12.29) | 2.27 (0.71–7.33) | |||
| Gender | 0.170 | 0.572 | |||
| Male | - | - | |||
| Female | 0.67 (0.31–1.44) | 0.74 (0.61–2.06) | |||
| Tumor location | 0.107 | 0.263 | |||
| Right colon | - | - | |||
| Left colon | 2.05 (0.94–4.51) | 1.95 (0.61–6.30) | |||
| Stage | 0.04 | 0.688 | |||
| I | - | - | |||
| II | 0.43 (0.21–0.94) | 1.30 (0.36–4.63) | |||
| Combined PDC/NLR | <0.001 | <0.001 | |||
| PDC absent/L-NLR | - | - | |||
| PDC absent/H-NLR | 5.78 (1.11–30.27) | 2.52 (0.16–40.74) | |||
| PDC present/L-NLR | 19.13 (3.96–92.36) | 19.91 (2.14–185.11) | |||
| PDC present/H-NLR | 43.58 (9.29–204.34) | 56.67 (6.63–483.94) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turri, G.; Barresi, V.; Valdegamberi, A.; Gecchele, G.; Conti, C.; Ammendola, S.; Guglielmi, A.; Scarpa, A.; Pedrazzani, C. Clinical Significance of Preoperative Inflammatory Markers in Prediction of Prognosis in Node-Negative Colon Cancer: Correlation between Neutrophil-to-Lymphocyte Ratio and Poorly Differentiated Clusters. Biomedicines 2021, 9, 94. https://doi.org/10.3390/biomedicines9010094
Turri G, Barresi V, Valdegamberi A, Gecchele G, Conti C, Ammendola S, Guglielmi A, Scarpa A, Pedrazzani C. Clinical Significance of Preoperative Inflammatory Markers in Prediction of Prognosis in Node-Negative Colon Cancer: Correlation between Neutrophil-to-Lymphocyte Ratio and Poorly Differentiated Clusters. Biomedicines. 2021; 9(1):94. https://doi.org/10.3390/biomedicines9010094
Chicago/Turabian StyleTurri, Giulia, Valeria Barresi, Alessandro Valdegamberi, Gabriele Gecchele, Cristian Conti, Serena Ammendola, Alfredo Guglielmi, Aldo Scarpa, and Corrado Pedrazzani. 2021. "Clinical Significance of Preoperative Inflammatory Markers in Prediction of Prognosis in Node-Negative Colon Cancer: Correlation between Neutrophil-to-Lymphocyte Ratio and Poorly Differentiated Clusters" Biomedicines 9, no. 1: 94. https://doi.org/10.3390/biomedicines9010094