Controlling Antibiotic Release from Polymethylmethacrylate Bone Cement



Abstract
:1. Prosthetic Joint Infections and Local Antimicrobial Delivery Strategy
2. Antibiotic Therapeutic Efficacy and Tissue Toxicity Consideration
2.1. Therapeutic Level, Duration and Effectiveness
2.2. Local Tissue Toxicity
3. Current State of Antibiotic Loaded PMMA Bone Cement
3.1. Loading Dose
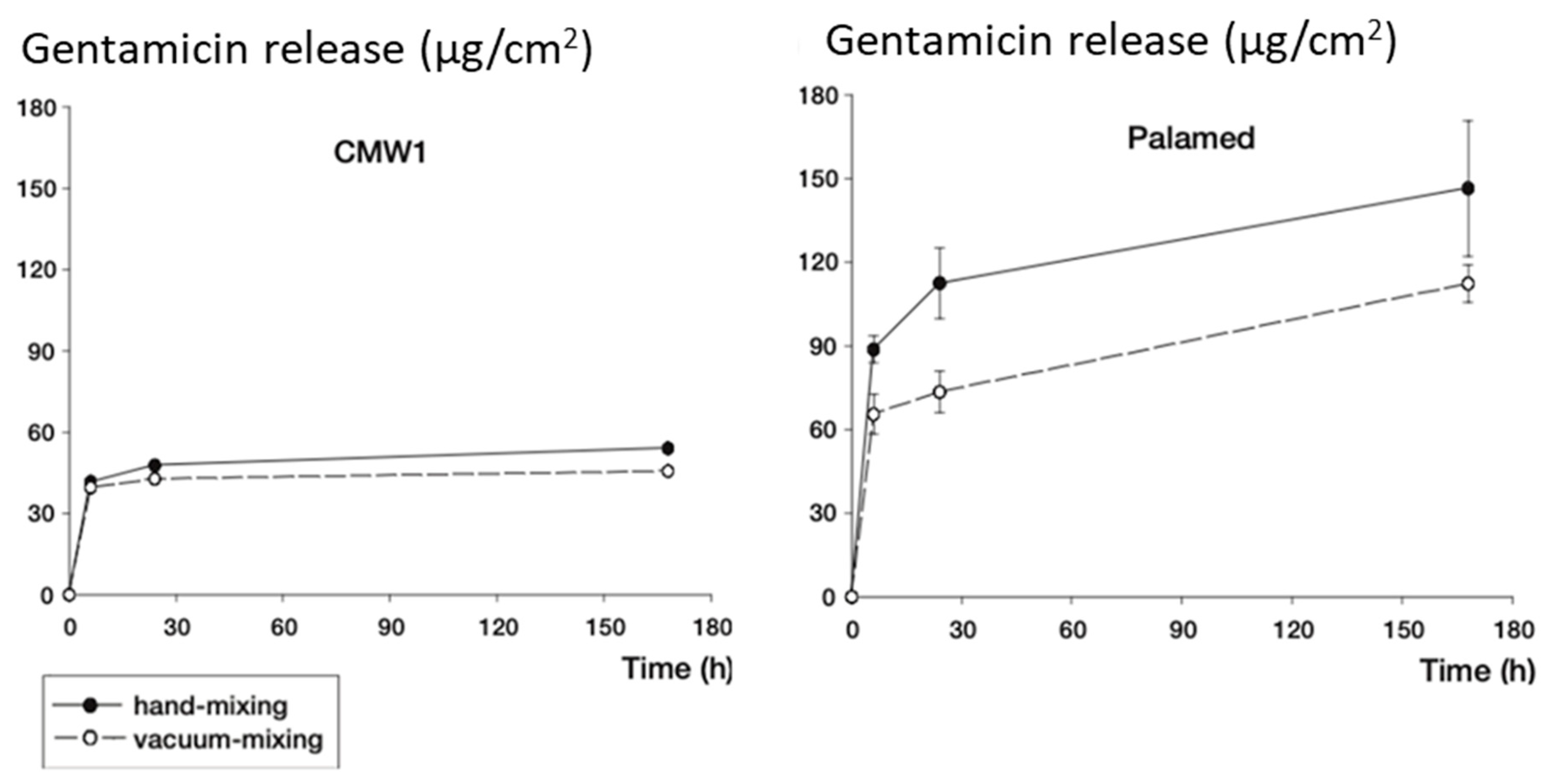
3.2. Mixing Methods and Release Characteristics
4. Controlling Antibiotic Release from PMMA Cement
4.1. Antibiotic Combinations and Antibiotic Heat Stability
4.2. Controlling Antibiotic Release and Osteo-Conductivity/Inductivity
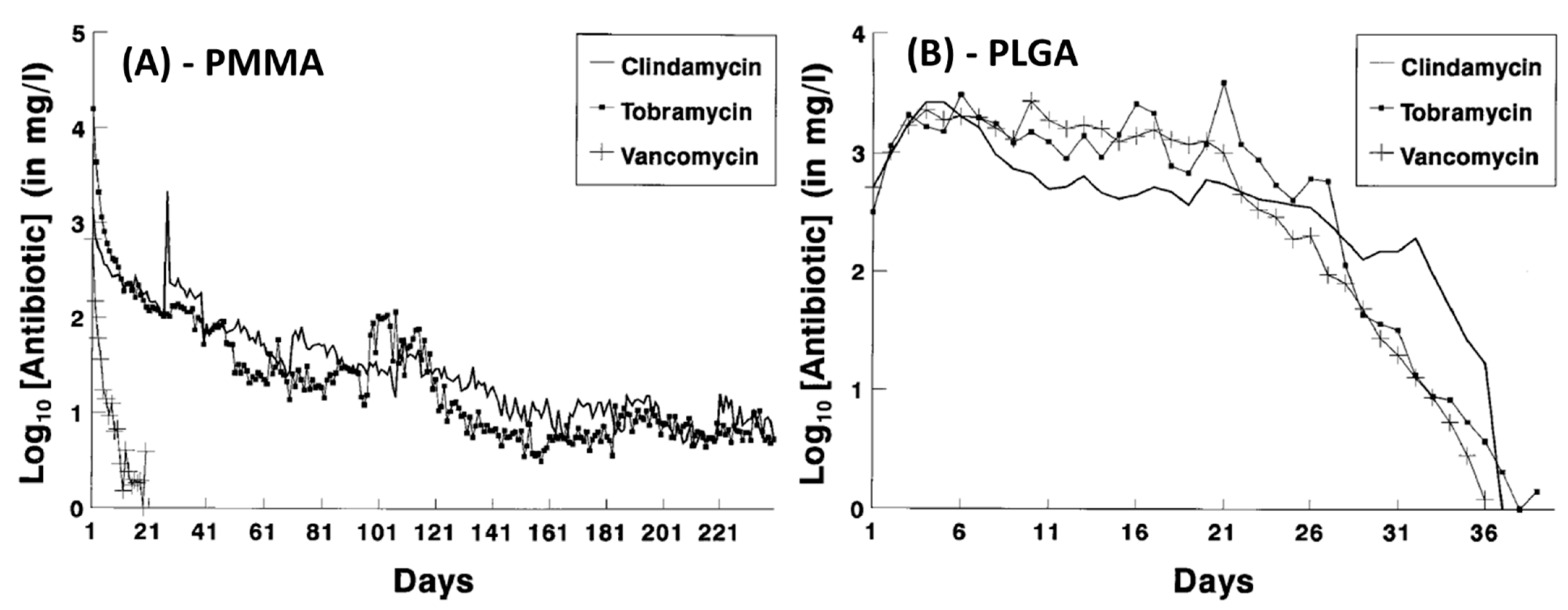
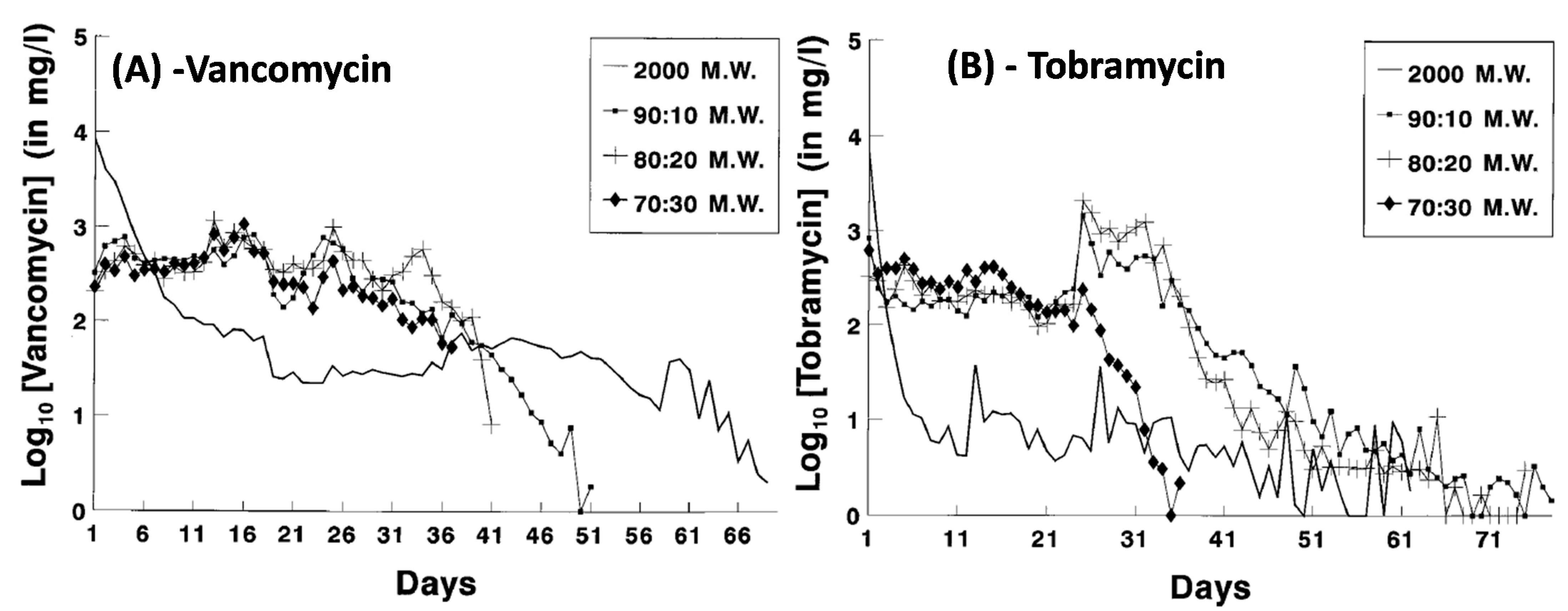
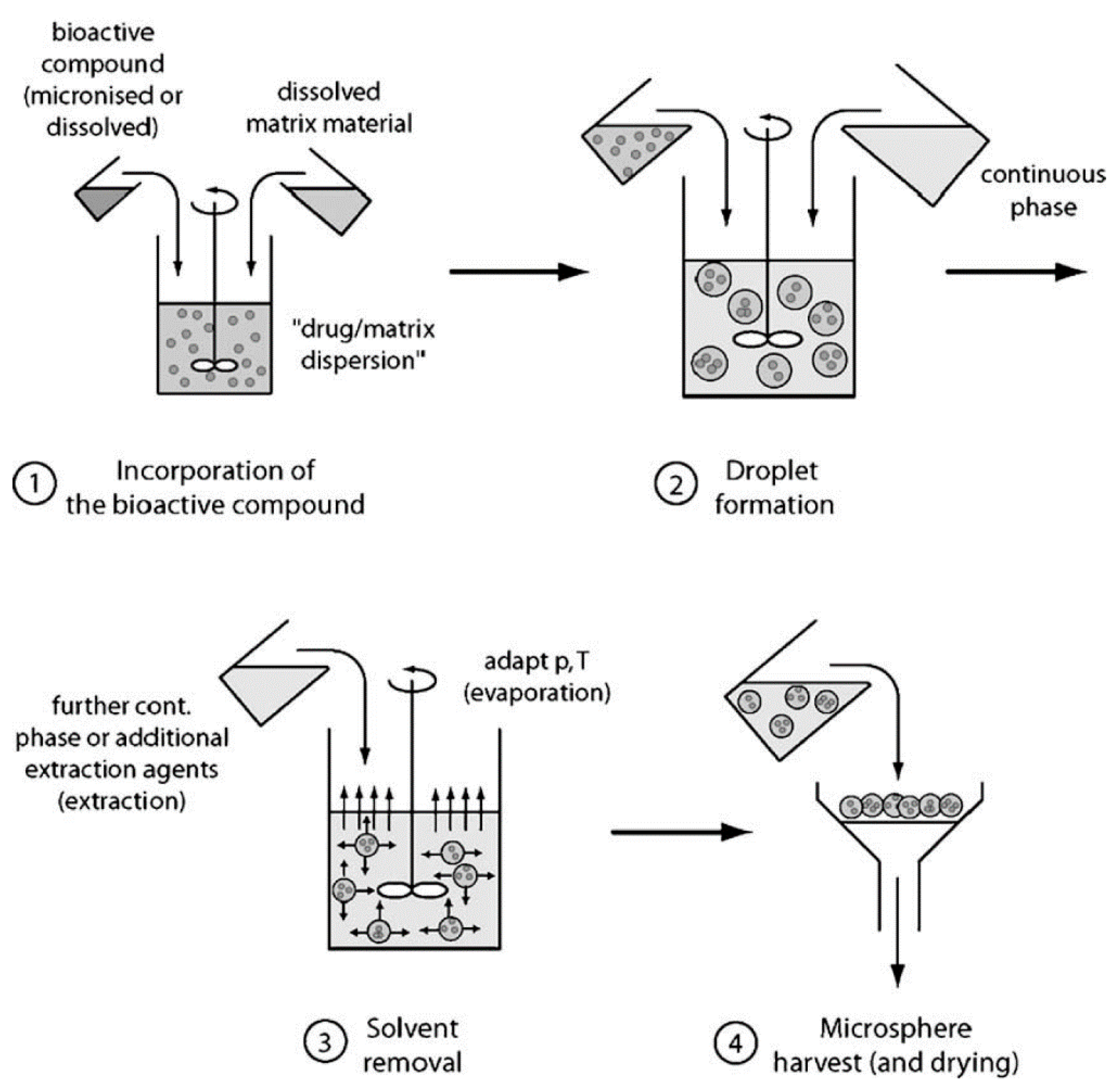
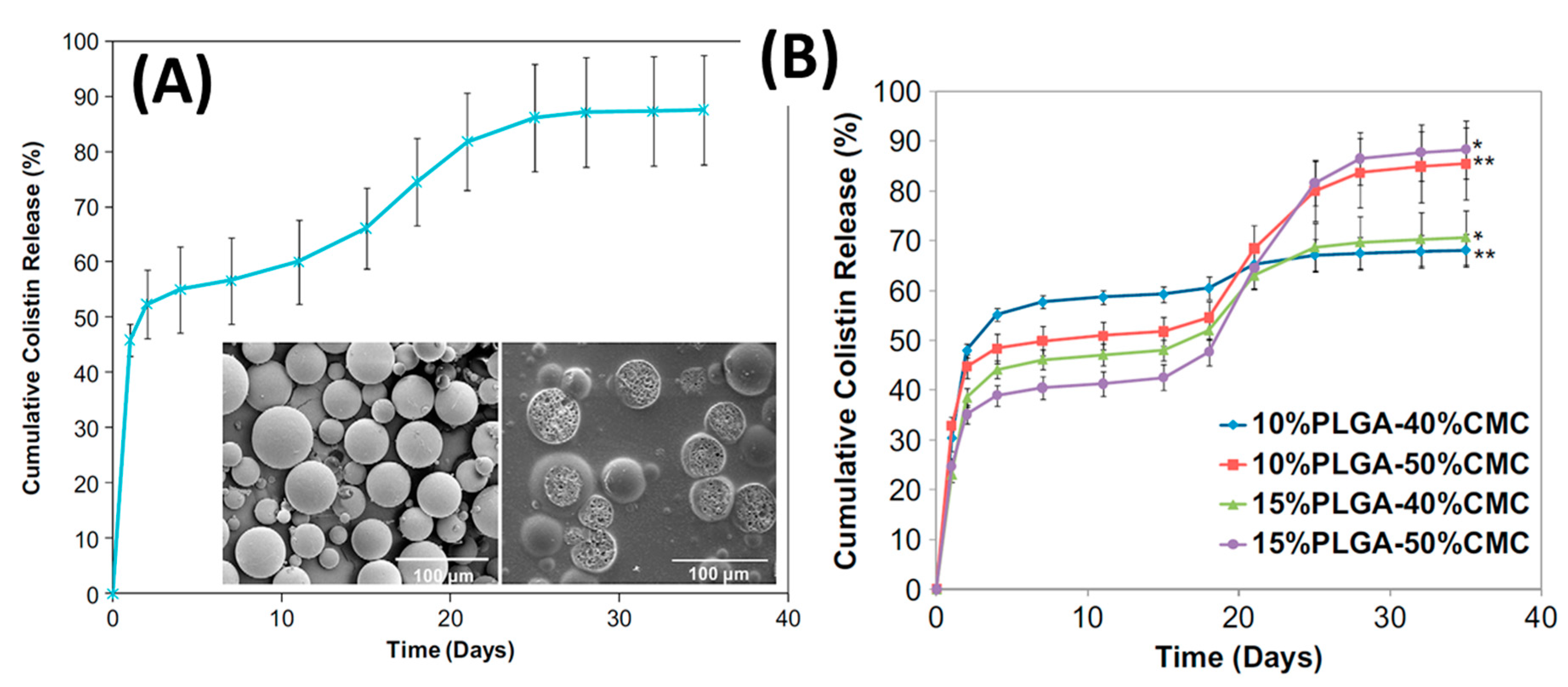
4.3. Controlling Antibiotic Release and Improving Bone in-Growth by Biodegradable Polymers—The Case of Poly(lactic-co-glycolic) Acid (PLGA)
4.4. Loading Methods
4.5. Controlling Antibiotic Release and Improving Bone in-Growth by Inorganic Biomaterials—The Case of Calcium Phosphate
4.6. CaP Materials as Additives to PMMA Bone Cement to Control Antibiotic Release
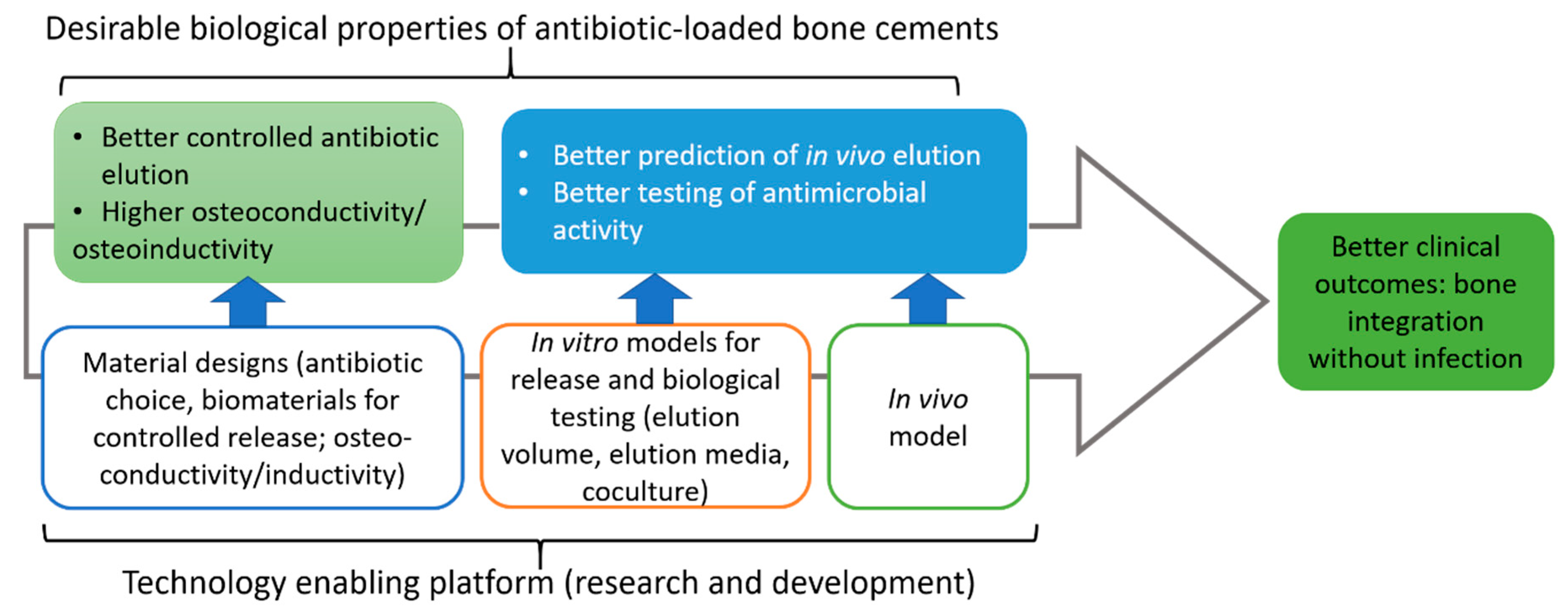
5. Concluding Remarks with an Emphasis on the Current Knowledge Gap
Funding
Acknowledgments
Conflicts of Interest
References
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg. Am. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Koh, C.K.; Zeng, I.; Ravi, S.; Zhu, M.; Vince, K.G.; Young, S.W. Periprosthetic Joint Infection Is the Main Cause of Failure for Modern Knee Arthroplasty: An Analysis of 11,134 Knees. Clin. Orthop. Relat. Res. 2017, 475, 2194–2201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tande, A.J.; Patel, R. Prosthetic joint infection. Clin. Microbiol. Rev. 2014, 27, 302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic-Joint Infections. N. Engl. J. Med. 2004, 351, 1645–1654. [Google Scholar] [CrossRef] [Green Version]
- Brandt, C.M.; Sistrunk, W.W.; Duffy, M.C.; Hanssen, A.D.; Steckelberg, J.M.; Ilstrup, D.M.; Osmon, D.R. Staphylococcus aureus Prosthetic Joint Infection Treated with Debridement and Prosthesis Retention. Clin. Infect. Dis. 1997, 24, 914–919. [Google Scholar] [CrossRef] [Green Version]
- Gbejuade, H.O.; Lovering, A.M.; Webb, J.C. The role of microbial biofilms in prosthetic joint infections: A review. Acta Orthop. 2015, 86, 147–158. [Google Scholar] [CrossRef]
- Sloan, M.; Premkumar, A.; Sheth, N.P. Projected Volume of Primary Total Joint Arthroplasty in the U.S., 2014 to 2030. J. Bone Jt. Surg. Am. 2018, 100, 1455–1460. [Google Scholar] [CrossRef]
- Wu, P.; Grainger, D.W. Drug/device combinations for local drug therapies and infection prophylaxis. Biomaterials 2006, 27, 2450–2467. [Google Scholar] [CrossRef]
- Campoccia, D.; Montanaro, L.; Speziale, P.; Arciola, C.R. Antibiotic-loaded biomaterials and the risks for the spread of antibiotic resistance following their prophylactic and therapeutic clinical use. Biomaterials 2010, 31, 6363–6377. [Google Scholar] [CrossRef]
- Zilberman, M.; Elsner, J. Antibiotic-eluting medical devices for various applications. J. Control. Release 2008, 130, 202–215. [Google Scholar] [CrossRef]
- Senneville, E.; Joulie, D.; Legout, L.; Valette, M.; Dezeque, H.; Beltrand, E.; Roselé, B.; d’Escrivan, T.; Loïez, C.; Caillaux, M.; et al. Outcome and Predictors of Treatment Failure in Total Hip/Knee Prosthetic Joint Infections Due to Staphylococcus aureus. Clin. Infect. Dis. 2011, 53, 334–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanellakopoulou, K.; Giamarellos-Bourboulis, E. Carrier Systems for the Local Delivery of Antibiotics in Bone Infections. Drugs 2000, 59, 1223–1232. [Google Scholar] [CrossRef] [PubMed]
- Charette, R.; Melnic, C. Two-Stage Revision Arthroplasty for the Treatment of Prosthetic Joint Infection. Curr. Rev. Musculoskelet. Med. 2018, 11, 332–340. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, M.W.; Ghoneim, M.M.; Hinrichs, J.V.; Mehta, M.P.; Wright, E.J. Psychological consequences of surgery. Psychosom. Med. 1989, 51, 356–370. [Google Scholar] [CrossRef]
- Prokuski, L. Prophylactic antibiotics in orthopaedic surgery. JAAOS-J. Am. Acad. Orthop. Surg. 2008, 16, 283–293. [Google Scholar] [CrossRef]
- Technical Guideline, Therapeutic Guidelines, Ltd. eTherapeutic Guidelines 2017. Available online: https://www.tg.org.au/ (accessed on 31 December 2020).
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R. Diagnosis and Management of Prosthetic Joint Infection: Clinical Practice Guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, e1–e25. [Google Scholar] [CrossRef] [Green Version]
- Fish, D.N.; Hoffman, H.M.; Danziger, L.H. Antibiotic-impregnated cement use in U.S. hospitals. Am. J. Heal. Pharm. 1992, 49, 2469–2474. [Google Scholar] [CrossRef]
- Bourne, R.B. Prophylactic use of antibiotic bone cement: An emerging standard--in the affirmative. J. Arthroplast. 2004, 19, 69–72. [Google Scholar] [CrossRef]
- Savvidou, O.D.; Kaspiris, A.; Trikoupis, I.; Kakouratos, G.; Goumenos, S.; Melissaridou, D.; Papagelopoulos, P.J. Efficacy of antimicrobial coated orthopaedic implants on the prevention of periprosthetic infections: A systematic review and meta-analysis. J. Bone Jt. Infect. 2020, 5, 212–222. [Google Scholar] [CrossRef]
- Blondeau, J.M. New concepts in antimicrobial susceptibility testing: The mutant prevention concentration and mutant selection window approach. Veter Dermatol. 2009, 20, 383–396. [Google Scholar] [CrossRef]
- Li, S.; Starkey, E.S. What do I need to know about glycopeptide antibiotics? Arch. Dis. Child. Educ. Pract. Ed. 2016, 101, 323. [Google Scholar] [CrossRef] [PubMed]
- Duewelhenke, N.; Krut, O.; Eysel, P. Influence on Mitochondria and Cytotoxicity of Different Antibiotics Administered in High Concentrations on Primary Human Osteoblasts and Cell Lines. Antimicrob. Agents Chemother. 2007, 51, 54–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathbone, C.R.; Cross, J.D.; Brown, K.V.; Murray, C.K.; Wenke, J.C. Effect of various concentrations of antibiotics on osteogenic cell viability and activity. J. Orthop. Res. 2011, 29, 1070–1074. [Google Scholar] [CrossRef]
- James, A.; Larson, T. Acute renal failure after high-dose antibiotic bone cement: Case report and review of the literature. Ren. Fail. 2015, 37, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Charnley, J. Acrylic Cement in Orthopedic Surgery Baltimore; The Williams and Wilkins Co.: Philadelphia, PA, USA, 1970; p. 36. [Google Scholar]
- Webb, J.; Spencer, R. The role of polymethylmethacrylate bone cement in modern orthopaedic surgery. J. Bone Jt. Surg. 2007, 89, 851–857. [Google Scholar] [CrossRef]
- Galibert, P.; Deramond, H.; Rosat, P.; Le Gars, D. Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty. Neuro-Chirurgie 1987, 33, 166. [Google Scholar]
- Lacy, M.K.; Nicolau, D.P.; Quintiliani, R. The Pharmacodynamics of Aminoglycosides. Clin. Infect. Dis. 1998, 27, 23–27. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, T.S.; Sørensen, A.I. Bactericidal activity of gentamicin against S. aureus. In vitro study questions value of prolonged high concentrations. Acta Orthop. Scand. 1993, 64, 3. [Google Scholar] [CrossRef]
- Krause, K.M.; Serio, A.W.; Kane, T.R.; Connolly, L.E. Aminoglycosides: An Overview. Cold Spring Harb. Perspect. Med. 2016, 6, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Gálvez-López, R.; Peña-Monje, A.; Antelo-Lorenzo, R.; Guardia-Olmedo, J.; Moliz, J.; Hernández-Quero, J.; Parra-Ruiz, J. Elution kinetics, antimicrobial activity, and mechanical properties of 11 different antibiotic loaded acrylic bone cement. Diagn. Microbiol. Infect. Dis. 2014, 78, 70–74. [Google Scholar] [CrossRef]
- Belt, H.V.; Neut, D.; Schenk, W.; Horn, J.R.; Mei, H.C.; Busscher, H.J. Infection of orthopedic implants and the use of antibiotic-loaded bone cements. A review. Acta Orthop. Scand. 2001, 72, 15. [Google Scholar] [CrossRef] [PubMed]
- Buchholz, H.W.; Engelbrecht, H. Depot effects of various antibiotics mixed with Palacos resins. Der Chir. 1970, 41, 511–515. [Google Scholar]
- Wahlig, H.; Buchholz, H.W. Experimental and clinical studies on the release of gentamicin from bone cement. Der Chir. 1972, 43, 441–445. [Google Scholar]
- Chapman, M.W.; Hadley, W.K. The effect of polymethylmethacrylate and antibiotic combinations on bacterial viability: An in vitro and preliminary in vivo study. J. Bone Jt. Surg. Am. 1976, 58, 76–81. [Google Scholar] [CrossRef]
- Holm, N.J.; Vejlsgaard, R. The in vitro elution of gentamicin sulphate from methylmethacrylate bone cement: A comparative study. Acta Orthop. Scand. 1976, 47, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Marks, K.E.; Nelson, C.L.; Lautenschlager, E.P. Antibiotic-impregnated acrylic bone cement. J. Bone Jt. Surg. Am. 1976, 58, 358–364. [Google Scholar] [CrossRef]
- Elson, R.A.; Jephcott, A.; McGechie, D.B.; Verettas, D. Antibiotic-loaded acrylic cement. J. Bone Jt. Surg. Br. 1977, 59, 200–205. [Google Scholar] [CrossRef] [Green Version]
- Hill, J.; Klenerman, L.; Trustey, S.; Blowers, R. Diffusion of antibiotics from acrylic bone-cement in vitro. J. Bone Jt. Surg. Br. 1977, 59, 197–199. [Google Scholar] [CrossRef]
- Hoff, S.F.; Fitzgerald, R.H., Jr.; Kelly, P.J. The depot administration of penicillin G and gentamicin in acrylic bone cement. J. Bone Jt. Surg. Am. 1981, 63, 798–804. [Google Scholar] [CrossRef]
- Bayston, R.; Milner, R.D. The sustained release of antimicrobial drugs from bone cement: An appraisal of laboratory investigations and their significance. J. Bone Jt. Surg. Am. 1982, 64, 460–464. [Google Scholar] [CrossRef] [Green Version]
- Beeching, N.J.; Thomas, M.G.; Roberts, S.; Lang, S.D.R. Comparative in-vitro activity of antibiotics incorporated in acrylic bone cement. J. Antimicrob. Chemother. 1986, 17, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Kuechle, D.K.; Landon, G.C.; Musher, D.M.; Noble, P.C. Elution of vancomycin, daptomycin, and amikacin from acrylic bone cement. Clin. Orthop. Relat. Res. 1991, 1991, 302–308. [Google Scholar] [CrossRef]
- Kendall, R.W.; Duncan, C.P.; Smith, J.A.; Ngui-Yen, J.H. Persistence of Bacteria on Antibiotic Loaded Acrylic Depots. Clin. Orthop. Relat. Res. 1996, 329, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Penner, M.J.; Masri, B.A.; Duncan, C.P. Elution characteristics of vancomycin and tobramycin combined in acrylic bone—cement. J. Arthroplast. 1996, 11, 939–944. [Google Scholar] [CrossRef]
- Greene, N.; Holtom, P.D.; Warren, C.A.; Ressler, R.L.; Shepherd, L.; McPherson, E.J.; Patzakis, M.J. In vitro elution of tobramycin and vancomycin polymethylmethacrylate beads and spacers from Simplex and Palacos. Am. J. Orthop. 1998, 27, 201–205. [Google Scholar]
- Chohfi, M.; Langlais, F.; Fourastier, J.; Minet, J.; Thomazeau, H.; Cormier, M. Pharmacokinetics, uses, and limitations of vancomycin-loaded bone cement. Int. Orthop. 1998, 22, 171–177. [Google Scholar] [CrossRef] [Green Version]
- Arora, M.; Chan, E.K.; Gupta, S.; Diwan, A.D. Polymethylmethacrylate bone cements and additives: A review of the literature. World J. Orthop. 2013, 4, 67–74. [Google Scholar] [CrossRef]
- Bertazzoni Minelli, E.; Benini, A.; Samaila, E.; Bondi, M.; Magnan, B. Antimicrobial activity of gentamicin and vancomycin combination in joint fluids after antibiotic-loaded cement spacer implantation in two-stage revision surgery. J. Chemother. 2015, 27, 17–24. [Google Scholar] [CrossRef]
- Jiranek, A.W.; Hanssen, D.A.; Greenwald, S.A. Antibiotic-Loaded Bone Cement for Infection Prophylaxis in Total Joint Replacement. J. Bone Jt. Surg. 2006, 88, 2487–2500. [Google Scholar] [CrossRef]
- Duey, R.E.; Chong, A.C.; McQueen, D.A.; Womack, J.L.; Song, Z.; Steinberger, T.A.; Wooley, P.H. Mechanical Properties and Elution Characteristics of Polymethylmethacrylate Bone Cement Impregnated with Antibiotics for Various Surface Area and Volume Constructs. Iowa Orthop. J. 2012, 32, 104–115. [Google Scholar]
- Technical Guidelines, American Society for Testing and Materials, ASTM F451-16 Standard Specification for Acrylic Bone Cement. 2016. Available online: https://www.astm.org/Standards/F451.htm (accessed on 31 December 2020).
- Funk, G.A.; Burkes, J.C.; Cole, K.A.; Rahaman, M.N.; McIff, T. Antibiotic Elution and Mechanical Strength of PMMA Bone Cement Loaded With Borate Bioactive Glass. J. Bone Jt. Infect. 2018, 3, 187–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, L.C.; Chang, S.J.; Kuo, S.M.; Chen, S.F.; Kuo, C.H. Evaluation of chitosan/[beta]-tricalcium phosphate microspheres as a constituent to PMMA cement. J. Mater. Sci. Mater. Med. 2005, 16, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Kendoff, D.O.; Gehrke, T.; Stangenberg, P.; Frommelt, L.; Bösebeck, H. Bioavailability of Gentamicin and Vancomycin Released from an Antibiotic Containing Bone Cement in Patients Undergoing a Septic One-Stage Total Hip Arthroplasty (THA) Revision: A Monocentric Open Clinical Trial. HIP Int. 2016, 26, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Frew, N.M.; Cannon, T.; Nichol, T.; Smith, T.J.; Stockley, I. Comparison of the elution properties of commercially available gentamicin and bone cement containing vancomycin with ‘home-made’ preparations. Bone Jt. J. 2017, 99, 73–77. [Google Scholar] [CrossRef]
- Macaulay, W.; DiGiovanni, C.W.; Restrepo, A.; Saleh, K.J.; Walsh, H.; Crossett, L.S.; Peterson, M.G.; Li, S.; Salvati, E.A. Differences in bone–cement porosity by vacuum mixing, centrifugation, and hand mixing. J. Arthroplast. 2002, 17, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Wixson Rl Fau-Lautenschlager, E.P.; Lautenschlager Ep Fau-Novak, M.A.; Novak, M.A. Vacuum mixing of acrylic bone cement. J. Arthroplast. 1987, 2, 10. [Google Scholar]
- Neut, D.; Van De Belt, H.; Van Horn, J.; Van Der Mei, H.; Busscher, H. The effect of mixing on gentamicin release from polymethylmethacrylate bone cements. Acta Orthop. Scand. 2003, 74, 670–676. [Google Scholar] [CrossRef]
- McLaren, A.C.; Nugent, M.; Economopoulos, K.; Kaul, H.; Vernon, B.L.; McLemore, R. Hand-mixed and Premixed Antibiotic-loaded Bone Cement Have Similar Homogeneity. Clin. Orthop. Relat. Res. 2009, 467, 1693–1698. [Google Scholar] [CrossRef] [Green Version]
- Gergely, R.C.R.; Toohey, K.S.; Jones, M.E.; Small, S.R.; Berend, M.E. Towards the optimization of the preparation procedures of PMMA bone cement. J. Orthop. Res. 2016, 34, 915–923. [Google Scholar] [CrossRef]
- Bertazzoni Minelli, E.; Della Bora, T.; Benini, A. Different microbial biofilm formation on polymethylmethacrylate (PMMA) bone cement loaded with gentamicin and vancomycin. Anaerobe 2011, 17, 380–383. [Google Scholar] [CrossRef]
- Bertazzoni Minelli, E.; Benini, A.; Magnan, B.; Bartolozzi, P. Release of gentamicin and vancomycin from temporary human hip spacers in two-stage revision of infected arthroplasty. J. Antimicrob. Chemother. 2004, 53, 329–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertazzoni Minelli, E.; Caveiari, C.; Benini, A. Release of Antibiotics from Polymethylmethacrylate Cement. J. Chemother. 2002, 14, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Boelch, S.; Jordan, M.C.; Arnholdt, J.; Rudert, M.; Luedemann, M.; Steinert, A.F. Loading with vancomycin does not decrease gentamicin elution in gentamicin premixed bone cement. J. Mater. Sci. Mater. Med. 2017, 28, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, P.H.; Tai, C.L.; Lee, P.C.; Chang, Y.H. Liquid Gentamicin and Vancomycin in Bone Cement: A Potentially More Cost-Effective Regimen. J. Arthroplast. 2009, 24, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Regis, D.; Sandri, A.; Samaila, E.; Benini, A.; Bondi, M.; Magnan, B. Release of Gentamicin and Vancomycin from Preformed Spacers in Infected Total Hip Arthroplasties: Measurement of Concentrations and Inhibitory Activity in Patients’ Drainage Fluids and Serum. Sci. World J. 2013, 2013, 752184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corona, P.S.; Barro, V.; Mendez, M.; Cáceres, E.; Flores, X. Industrially Prefabricated Cement Spacers: Do Vancomycin- and Gentamicin-impregnated Spacers Offer Any Advantage? Clin. Orthop. Relat. Res. 2014, 472, 923–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nau, C.; Seebach, C.; Trumm, A.; Schaible, A.; Kontradowitz, K.; Meier, S.; Buechner, H.; Marzi, I.; Henrich, D. Alteration of Masquelet’s induced membrane characteristics by different kinds of antibiotic enriched bone cement in a critical size defect model in the rat’s femur. Injury 2016, 47, 325–334. [Google Scholar] [CrossRef]
- Sarkar, P.; Yarlagadda, V.; Ghosh, C.; Haldar, J. A review on cell wall synthesis inhibitors with an emphasis on glycopeptide antibiotics. MedChemComm 2017, 8, 516–533. [Google Scholar] [CrossRef]
- Dunne, N.; Ormsby, R.W. MWCNT Used in Orthopaedic Bone Cements. In Carbon Nanotubes: Growth and Applications; Naraghi, M., Ed.; IntechOpen: London, UK, 2011. [Google Scholar]
- Samara, E.; Moriarty, T.F.; Decosterd, L.A.; Richards, R.G.; Gautier, E.; Wahl, P. Antibiotic stability over six weeks in aqueous solution at body temperature with and without heat treatment that mimics the curing of bone cement. Bone Jt. Res. 2017, 6, 296–306. [Google Scholar] [CrossRef]
- Fink, B.; Vogt, S.; Reinsch, M.; Büchner, H. Sufficient Release of Antibiotic by a Spacer 6 Weeks after Implantation in Two-Stage Revision of Infected Hip Prostheses. Clin. Orthop. Relat. Res. 2011, 469, 3141–3147. [Google Scholar] [CrossRef] [Green Version]
- Ensing, G.T.; van Horn, J.R.; van der Mei, H.C.; Busscher, H.J.; Neut, D. Copal Bone Cement Is More Effective in Preventing Biofilm Formation than Palacos R-G. Clin. Orthop. Relat. Res. 2014, 466, 1492–1498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anagnostakos, K.; Kelm, J. Enhancement of antibiotic elution from acrylic bone cement. J. Biomed. Mater. Res. B: Appl. Biomater. 2009, 90, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Dinu, V.; Lu, Y.; Weston, N.; Harrison, P.J.; Coupe, H.; Channell, G.; Adams, G.; Torcello-Gómez, A.; Sabater, C.; Mackie, A.; et al. The antibiotic vancomycin induces complexation and aggregation of gastrointestinal and submaxillary mucins. Sci. Rep. 2020, 10, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kadurugamuwa, J.L.; Clarke, A.J.; Beveridge, T.J. Surface action of gentamicin on Pseudomonas aeruginosa. J. Bacteriol. 1993, 175, 5798–5805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anagnostakos, K.; Meyer, C. Antibiotic Elution from Hip and Knee Acrylic Bone Cement Spacers: A Systematic Review. BioMed. Res. Int. 2017, 2017, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anagnostakos, K.; Wilmes, P.; Schmitt, E.; Kelm, J. Elution of gentamicin and vancomycin from polymethylmethacrylate beads and hip spacers in vivo. Acta Orthop. 2009, 80, 193–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balato, G.; Ascione, T.; Rosa, D.; Pagliano, P.; Solarino, G.; Moretti, B.; Mariconda, M. Release of Gentamicin from Cement Spacers in Two-Stage Procedures for Hip and Knee Prosthetic Infection: An. In Vivo Pharmacokinetic Study with Clinical Follow-Up. J. Boil. Regul. Homeost. Agents 2016, 29, 63–72. [Google Scholar]
- Hsieh, P.H.; Chang, Y.-H.; Chen, S.-H.; Ueng, S.W.N.; Shih, C.-H. High concentration and bioactivity of vancomycin and aztreonam eluted from Simplex cement spacers in two-stage revision of infected hip implants: A study of 46 patients at an average follow-up of 107 days. J. Orthop. Res. 2006, 24, 1615–1621. [Google Scholar] [CrossRef]
- Isiklar, Z.U.; Demirörs, H.; Akpinar, S.; Tandogan, R.N.; Alparslan, M. Two-stage treatment of chronic staphylococcal orthopaedic implant-related infections using vancomycin impregnated PMMA spacer and rifampin containing antibiotic protocol. Bull. Hosp. Jt. Dis. 1999, 58, 79–85. [Google Scholar]
- Kelm, J.; Regitz, T.; Schmitt, E.; Jung, W.; Anagnostakos, K. In Vivo and In Vitro Studies of Antibiotic Release from and Bacterial Growth Inhibition by Antibiotic-Impregnated Polymethylmethacrylate Hip Spacers. Antimicrob. Agents Chemother. 2006, 50, 332–335. [Google Scholar] [CrossRef] [Green Version]
- Gentile, P.; Chiono, V.; Carmagnola, I.; Hatton, P.V. An Overview of Poly(lactic-co-glycolic) Acid (PLGA)-Based Biomaterials for Bone Tissue Engineering. Int. J. Mol. Sci. 2014, 15, 3640–3659. [Google Scholar] [CrossRef] [PubMed]
- Mader, J.T.; Calhoun, J.; Cobos, J. In vitro evaluation of antibiotic diffusion from antibiotic-impregnated biodegradable beads and polymethylmethacrylate beads. Antimicrob. Agents Chemother. 1997, 41, 415–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freitas, S.; Merkle, H.P.; Gander, B. Microencapsulation by solvent extraction/evaporation: Reviewing the state of the art of microsphere preparation process technology. J. Control. Release 2005, 102, 313–332. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Rouaud, O.; Poncelet, D. Microencapsulation by solvent evaporation: State of the art for process engineering approaches. Int. J. Pharm. 2008, 363, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Spicer, P.P.; Shah, S.R.; Henslee, A.M.; Watson, B.M.; Kinard, L.A.; Kretlow, J.D.; Bevil, K.; Kattchee, L.; Bennett, G.N.; Demian, N.; et al. Evaluation of antibiotic releasing porous polymethylmethacrylate space maintainers in an infected composite tissue defect model. Acta Biomater. 2013, 9, 8832–8839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, M.; Kretlow, J.D.; Nguyen, A.; Young, S.; Baggett, L.S.; Wong, M.E.; Kasper, F.; Mikos, A.G. Antibiotic-releasing porous polymethylmethacrylate constructs for osseous space maintenance and infection control. Biomaterials 2010, 31, 4146–4156. [Google Scholar] [CrossRef] [Green Version]
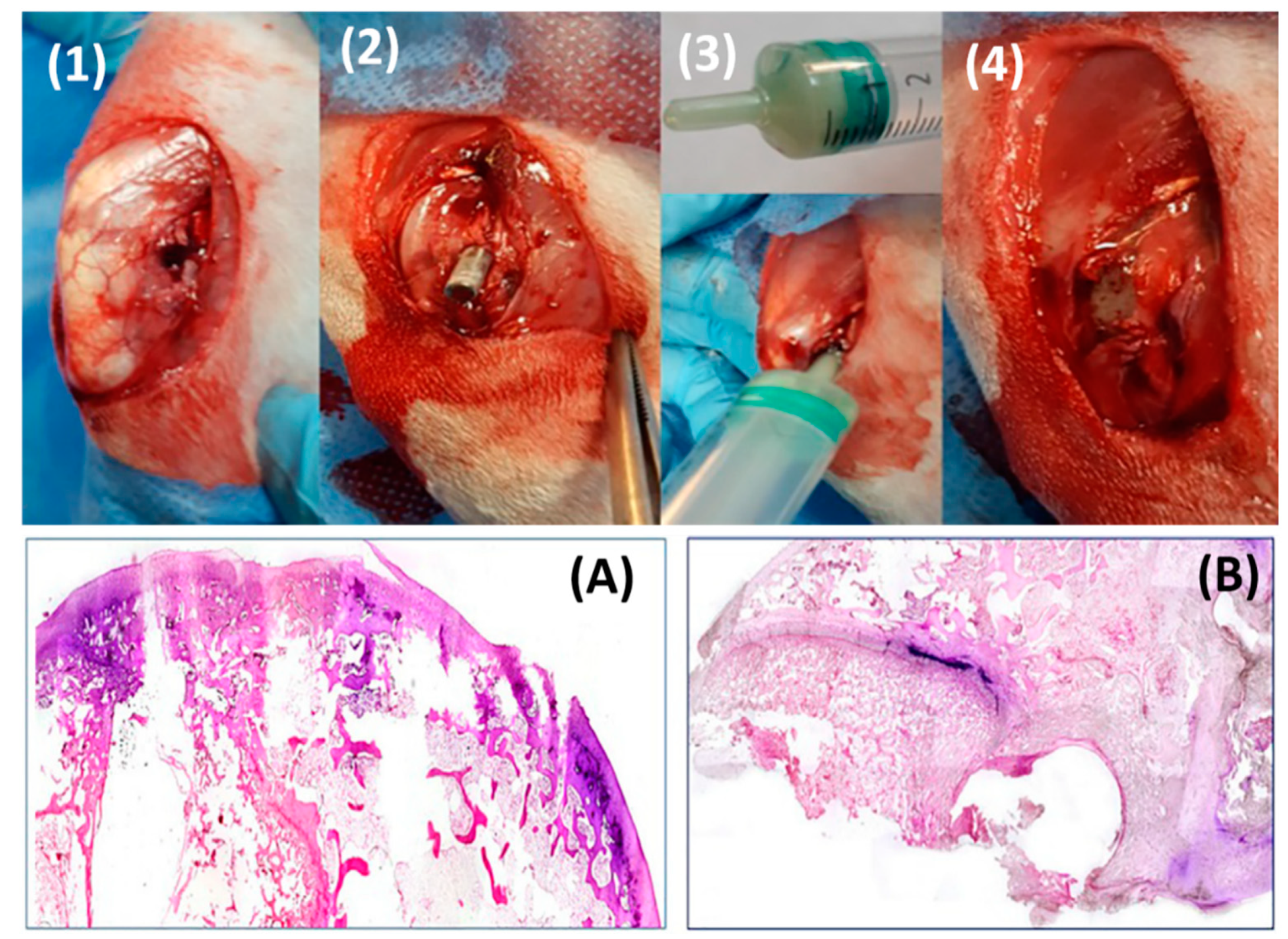
- Azuara, G.; García-García, J.; Ibarra, B.; Parra-Ruiz, F.J.; Asúnsolo, A.; Ortega, M.A.; Vázquez-Lasa, B.; Buján, J.; San Román, J.; de la Torre, B. Experimental study of the application of a new bone cement loaded with broad spectrum antibiotics for the treatment of bone infection. Rev. Esp. Cir. Ortop. Traumatol. (English Edition) 2019, 63, 95–103. [Google Scholar] [CrossRef]
- Dorati, R.; DeTrizio, A.; Modena, T.; Conti, B.; Benazzo, F.; Gastaldi, G.; Genta, I. Biodegradable Scaffolds for Bone Regeneration Combined with Drug-Delivery Systems in Osteomyelitis Therapy. Pharmaceuticals 2017, 10, 96. [Google Scholar] [CrossRef] [Green Version]
- Xie, L.; Yu, H.; Deng, Y.; Yang, W.; Liao, L.; Long, Q. Preparation, characterization and in vitro dissolution behavior of porous biphasic α/β-tricalcium phosphate bioceramics. Mater. Sci. Eng. C 2016, 59, 1007–1015. [Google Scholar] [CrossRef]
- Vázquez, B.; Ginebra, M.P.; Gil, X.; Planell, J.A.; San Román, J. Acrylic bone cements modified with beta-TCP particles encapsulated with poly(ethylene glycol). Biomaterials 2005, 26, 4309–4316. [Google Scholar] [CrossRef]
- Wu, C.C.; Yang, K.C.; Yang, S.H.; Lin, M.H.; Kuo, T.F.; Lin, F.H. In Vitro Studies of Composite Bone Filler Based on Poly(Propylene Fumarate) and Biphasic a-Tricalcium Phosphate/Hydroxyapatite Ceramic Powder. Artif. Organs 2012, 36, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Khandaker, M.; Meng, Z. The Effect of Nanoparticles and Alternative Monomer on the Exothermic Temperature of PMMA Bone Cement. Procedia Eng. 2015, 105, 946–952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fini, M.; Giavaresi, G.; Aldini, N.N.; Torricelli, P.; Botter, R.; Beruto, D.; Giardino, R. A bone substitute composed of polymethylmethacrylate and α-tricalcium phosphate: Results in terms of osteoblast function and bone tissue formation. Biomaterials 2002, 23, 4523–4531. [Google Scholar] [CrossRef]
- Dall’Oca, C.; Maluta, T.; Cavani, F.; Morbioli, G.; Bernardi, P.; Sbarbati, A.; Degl’Innocenti, D.; Magnan, B. The biocompatibility of porous vs non-porous bone cements: A new methodological approach. Eur. J. Histochem. 2014, 58, 2255. [Google Scholar] [CrossRef] [Green Version]
- Giavaresi, G.; Minelli, E.B.; Sartori, M.; Benini, A.; Parrilli, A.; Maltarello, M.C.; Salamanna, F.; Torricelli, P.; Giardino, R.; Fini, M. New PMMA-based composites for preparing spacer devices in prosthetic infections. J. Mater. Sci. Mater. Med. 2012, 23, 1247–1257. [Google Scholar] [CrossRef]
- Uchiyama, K.; Takahira, N.; Fukushima, K.; Moriya, M.; Yamamoto, T.; Minegishi, Y.; Sakai, R.; Itoman, M.; Takaso, M. Two-Stage Revision Total Hip Arthroplasty for Periprosthetic Infections Using Antibiotic-Impregnated Cement Spacers of Various Types and Materials. Sci. World J. 2013, 2013, 1–7. [Google Scholar] [CrossRef]
- Shirtliff, M.E.; Calhoun, J.H.; Mader, J.T. Experimental Osteomyelitis Treatment with Antibiotic-Impregnated Hydroxyapatite. Clin. Orthop. Relat. Res. 2002, 401, 239–247. [Google Scholar] [CrossRef]
- Jeffery, C.A. A Medical Implant and a Method of Coating a MEDICAL Implant. Patent WO2018107243A1, 15 December 2017. [Google Scholar]
- Levick, J.; McDonald, J. Fluid movement across synovium in healthy joints: Role of synovial fluid macromolecules. Ann. Rheum. Dis. 1995, 54, 417–423. [Google Scholar] [CrossRef] [Green Version]
- Dragoo, J.L.; Miller, M.D.; Vaughn, Z.D.; Schmidt, J.D.; Handley, E. Restoration of Knee Volume Using Selected Arthroscopic Releases. Am. J. Sports Med. 2010, 38, 2288–2293. [Google Scholar] [CrossRef]
- Alho, A.; Hoiseth, A.; Husby, T. Bone-mass distribution in the femur A cadaver study on the relations of structure and strength. Acta Orthop. Scand. 1989, 60, 101–104. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibiotic | Mean Inhibitory Concentration (μg/mL) for 20% Inhibition (IC20) and 50% Inhibition (IC50) of Proliferation and Metabolic Activity in Different Cell Types (Highest Concentration Tested Was 400 μg/mL) | |||||
|---|---|---|---|---|---|---|
| IC20PHO | IC50PHO | IC20MG63 | IC50 MG63 | IC20 HeLa | IC50 HeLa | |
| Penicillin G | No effect | No effect | No effect | No effect | No effect | No effect |
| Flucloxacillin | No effect | No effect | No effect | No effect | No effect | No effect |
| Amoxicillin | No effect | No effect | No effect | No effect | No effect | No effect |
| Cefazolin | 380, >400 | >400, >400 | 230, 400 | >400, >400 | 270, >400 | >400, >400 |
| Vancomycin | No effect | No effect | No effect | No effect | No effect | No effect |
| Fosfomycin | No effect | No effect | No effect | No effect | No effect | No effect |
| Gentamicin | No effect | No effect | No effect | No effect | No effect | No effect |
| Streptomycin | No effect | No effect | No effect | No effect | No effect | No effect |
| Tobramycin | No effect | No effect | No effect | No effect | No effect | No effect |
| Ciprofloxacin | 70, 260 | 170, >400 | 80, 60 | 160, 150 | 100, 70 | 290, 120 |
| Moxifloxacin | 80, 190 | 160, >400 | 110, 30 | 230, 170 | 90, 40 | 320, 110 |
| Tetracycline | 60, ÷ | 180, ÷ | 60, ÷ | 180, ÷ | 200, ÷ | >400, ÷ |
| Rifampin | 30, ÷ | 130, ÷ | 120, ÷ | 240, ÷ | 180, ÷ | 270, ÷ |
| Clindamycin | 40, 340 | 150, >400 | 160, 200 | 250, >400 | 230, 80 | >400, 200 |
| Lincomycin | No effect | No effect | No effect | No effect | No effect | No effect |
| Erythromycin | 30, 210 | 180, >400 | 130, 180 | 300, 310 | 210, 110 | >400, 170 |
| Roxithromycin | 20, 110 | 70, 210 | 50, 50 | 180, 110 | 100, 30 | 160, 90 |
| Azithromycin | 20, 80 | 25, 160 | 30, 70 | 190, 180 | 110, 50 | 240, 160 |
| Chloramphenicol | 60, 260 | 230, >400 | 200, 110 | >400, 400 | 340, 100 | >400, 340 |
| Linezolid | 240, >400 | >400, >400 | No effect, 250 | No effect, >400 | No effect, 300 | No effect, >400 |
| Antibiotics | Cement | Reference |
|---|---|---|
| Gentamicin/penicillin/erythromycin | Palacos | [34] |
| Gentamicin | Palacos | [35] |
| Penicillin/methicillin/erythromycin/lincomycin/nafcillin/polymyxin/colistimate | Simplex | [36] |
| Gentamicin | CMW/Simplex/Palacos | [37] |
| Gentamicin/oxacillin/cephazolin | Simplex/Palacos | [38] |
| Sodium fusidate/gentamicin | Palacos/Simplex/CMW | [39] |
| Fusidin/clindamycin/gentamicin | Simplex | [40] |
| Penicillin/gentamicin | Palacos/Simplex | [41] |
| Gentamicin sulfate/sodium fusidate/diethanolamine | Palacos/CMW | [42] |
| Ceftriaxone/coumermycin/sulfampicion-methoxozaole/trimethoprim/cephalothin/vacomycin/fusidic acid/ gentamicin/rifampicin/vancomycin | Palacos/CMW | [43] |
| Vancomycin/amikacin/daptomycin | Palacos/Simplex/Zimmer low viscosity and dough type | [44] |
| Tobramycin/vancomycin | Palacos/Simplex | [45] |
| Vancomycin/tobramycin | Palacos | [46] |
| Tobramycin/vancomycin | Simplex/Palacos | [47] |
| Vancomycin | Cerafix | [48] |
| Product Name | Manufacturers/U.S. Distributors | Cement Type | Dosage of Antibiotic Per 40 g of Bone Cement |
|---|---|---|---|
| Cobalt g-HV | Biomet (Warsaw, IN, USA) | Copolymer high viscosity | 0.5 g of gentamicin |
| Palacos G | Biomet (Warsaw, IN, USA) | Copolymer high viscosity | 0.5 g of gentamicin |
| DePuy 1 | DePuy Orthopaedics (Warsaw, IN, USA) | Homopolymer high viscosity | 1.0 g of gentamicin |
| Cemex Genta | Exactech (Gainesville, FL, USA) | Copolymer medium viscosity | 0.5 g of gentamicin |
| VersaBond AB | Smith and Nephew (Memphis, TN, USA) | Copolymer medium viscosity | 1.0 g of tobramycin |
| Simplex P | Stryker Orthopaedics (Mahwah, NJ, USA) | Copolymer medium viscosity | 1.0 g of tobramycin |
| Biomet Refobacin Cement R | Biomet (Warsaw, IN, USA) | High viscosity | 2% of gentamicin sulfate |
| Palacos R+G p (predecessor Refobacin Palacos) | Heraeus (Langhorne, PA, USA) | High viscosity | 1.96% of gentamicin |
| Cement Used and Reference | Antibiotic Amount per 40 g Cement Powder | Antibiotic Powder Combination | Hour 1 | Day 1 | Day 2 | Day 7 | Week 2 | Week 6 |
|---|---|---|---|---|---|---|---|---|
| (All Values Are in μg/mL) | ||||||||
| Palacos [80] | 2 g | Vancomycin | 72 | 6.6 | ||||
| 0.5 g | Gentamicin | 39 | 1.9 | |||||
| Palacos [81] | 1 g | Clindamycin | ||||||
| 1 g | Gentamicin | 30.61 | 53.9 | |||||
| Cemex [50] | 1 g | Vancomycin | 28.8 | |||||
| 0.76 g | Gentamicin | 88 | ||||||
| Simplex [82] | 4 g | Vancomycin | 1538 | 571.9 | >MIC | |||
| 4 g | Azertonam | 1003 | 313.6 | >MIC | ||||
| Simplex [67] | 3 g | Vancomycin | 485.5 | 76.1 | ||||
| 480 mg | Gentamicin (liquid) | 58.3 | 14.6 | |||||
| Prepare in house [83] | 2 g | Vancomycin | 57 | |||||
| - | Gentamicin | |||||||
| Palacos [84] | 2 g | Vancomycin | <MIC | |||||
| 0.5 g | Gentamicin | <MIC | ||||||
| Cemex [68] | 150–170 mg | Vancomycin | 13.8-40 | |||||
| 1 g | Gentamicin | 15–90 | ||||||
| Palacos [74] | 2 g | Vancomycin | 50 | |||||
| 1 g | Gentamicin | 177 | ||||||
| 1 g | Clindamycin | 322 | ||||||
| Polymer | Modulus (GPa) | Elongation (%) | Solvent | Crystallinity (%) | Degradation Time (Weeks) | Applications |
|---|---|---|---|---|---|---|
| Polyglycolide/Polyglactine | 7 | 15–20 | Hexafluoroispropanol | 45–55 | 6–12 | Suture anchors, meniscus repair, medical devices, drug delivery, orbital floor |
| Poly(l-lactide) | 2.7 | - | Benzene, THF, dioxane | 37 | 12–18 | Fracture fixation, interference screws, suture anchors, meniscus repair |
| Poly(d,l-lactide) | - | 3–10 | Methanol, DMF | Amorphous | 11–15 | Orthopaedic implants, drug delivery |
| Poly(d,l-lactide-co-glycolide) 85/15 | 2 | 3–10 | Ethyl acetate, chloroform, acetone, THF | Amorphous | 5–6 | Interference screws, suture anchors, ACL reconstruction |
| Poly(d,l-lactide-co-glycolide) 75/25 | 2 | 3–10 | Ethyl acetate, chloroform, acetone, DMF, THF | Amorphous | 4–5 | Plates, mesh, screws, tack, drug delivery |
| Poly(d,l-lactide-co-glycolide) 50/50 | 2 | 3–10 | Ethyl acetate, chloroform, acetone, DMF, THF | Amorphous | 1–2 | Orthopaedic implants, drug delivery |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wall, V.; Nguyen, T.-H.; Nguyen, N.; Tran, P.A. Controlling Antibiotic Release from Polymethylmethacrylate Bone Cement. Biomedicines 2021, 9, 26. https://doi.org/10.3390/biomedicines9010026
Wall V, Nguyen T-H, Nguyen N, Tran PA. Controlling Antibiotic Release from Polymethylmethacrylate Bone Cement. Biomedicines. 2021; 9(1):26. https://doi.org/10.3390/biomedicines9010026
Chicago/Turabian StyleWall, Victoria, Thi-Hiep Nguyen, Nghi Nguyen, and Phong A. Tran. 2021. "Controlling Antibiotic Release from Polymethylmethacrylate Bone Cement" Biomedicines 9, no. 1: 26. https://doi.org/10.3390/biomedicines9010026