Shockwave Therapy Modulates the Expression of BMP2 for Prevention of Bone and Cartilage Loss in the Lower Limbs of Postmenopausal Osteoporosis Rat Model

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Laparotomy and Bilateral Ovariectomy
2.3. Focused SW Application
2.4. Bone Strength Analysis
2.5. Micro-CT Scanning
2.6. Histopathology of the Articular Cartilage of the Knees
2.7. Enzyme-Linked Immunosorbent Assay
2.8. Immunohistochemistry
2.9. Statistical Analysis
3. Results
3.1. Improvement in Bone Strength of the Right Femur after SW on the Left Femur or Left Tibia in OVX Rats
3.2. SW to the Left Tibia or Left Femur Reduced Bone Loss in OVX Rats
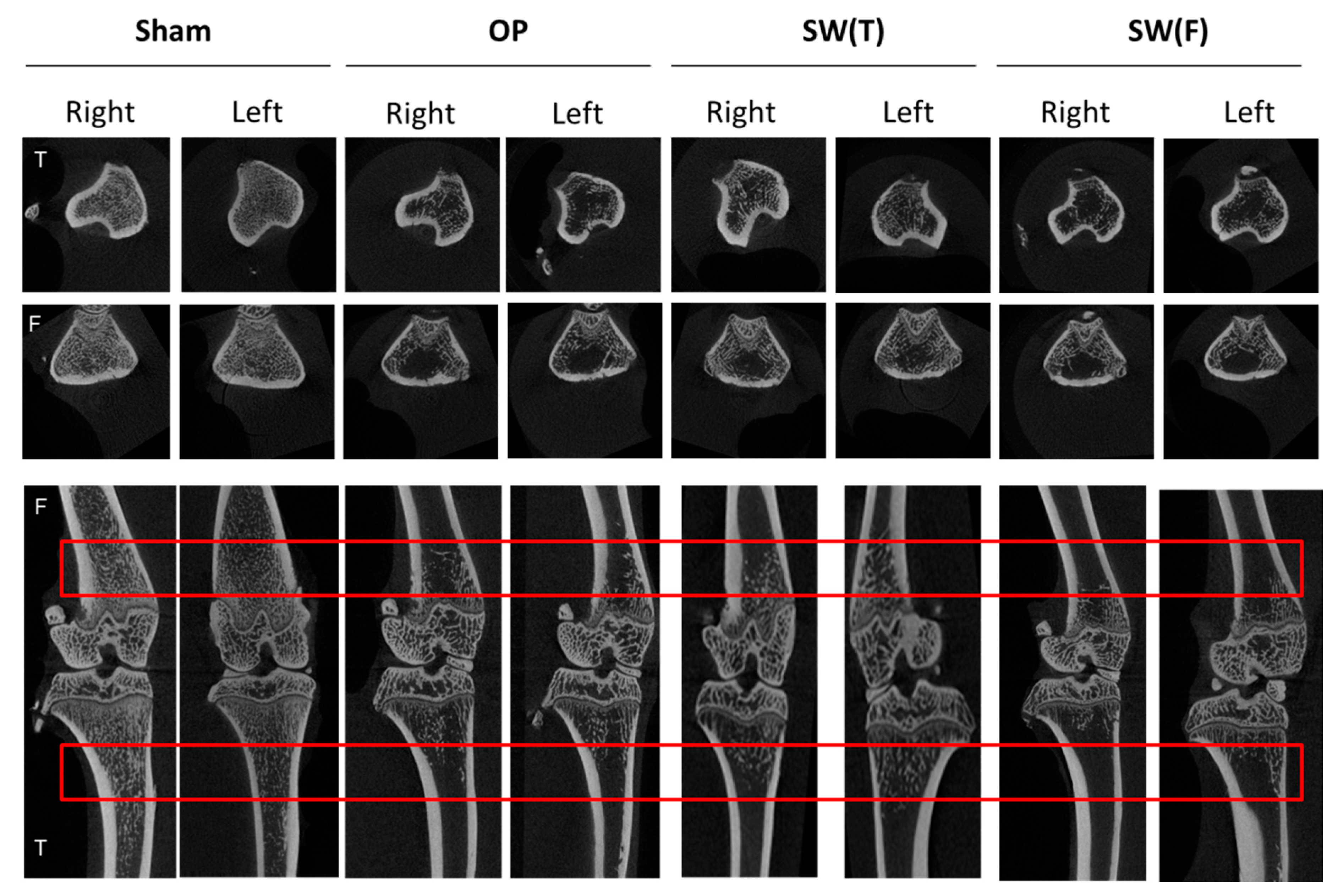
3.3. Micro-CT Analysis of Bone Quality after SW Therapy in OVX Rats
3.4. SW on Bone Stabilized BMP2 Expression in the Serum and May Have Induced Long-Range Effects to Protect the Extracellular Matrix of the Articular Cartilage in Both Lower Limbs of OVX Rat
3.5. SW Enhanced the Expressions of BMP2, BMP4, and Wnt3a Signaling in the Articular Cartilage of Osteoporotic Knees
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bernabei, R.; Martone, A.M.; Ortolani, E.; Landi, F.; Marzetti, E. Screening, diagnosis and treatment of osteoporosis: A brief review. Clin Cases Miner. Bone Metab. 2014, 11, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Lane, N.E. Epidemiology, etiology, and diagnosis of osteoporosis. Am. J. Obstet. Gynecol. 2006, 194, S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Larriera, A.I.; Palacio-Mancheno, P.E.; Gatti, V.; Fritton, J.C.; Bromage, T.G.; Cardoso, L.; Doty, S.B.; Fritton, S.P. The effects of estrogen deficiency on cortical bone microporosity and mineralization. Bone 2018, 110, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mauck, K.F.; Clarke, B.L. Diagnosis, screening, prevention, and treatment of osteoporosis. Mayo. Clin. Proc. 2006, 81, 662–672. [Google Scholar] [CrossRef] [Green Version]
- Leung, P.C.; Siu, W.S. Herbal treatment for osteoporosis: A current review. J. Tradit. Complement. Med. 2013, 3, 82–87. [Google Scholar] [CrossRef] [Green Version]
- Lirani-Galvao, A.P.; Lazaretti-Castro, M. Physical approach for prevention and treatment of osteoporosis. Arq. Bras. Endocrinol. Metabol. 2010, 54, 171–178. [Google Scholar] [CrossRef] [Green Version]
- Cosman, F.; de Beur, S.J.; LeBoff, M.S.; Lewiecki, E.M.; Tanner, B.; Randall, S.; Lindsay, R. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Osteoporos. Int. 2014, 25, 2359–2381. [Google Scholar] [CrossRef] [Green Version]
- Watts, N.B.; Lewiecki, E.M.; Miller, P.D.; Baim, S. National Osteoporosis Foundation 2008 Clinician’s Guide to Prevention and Treatment of Osteoporosis and the World Health Organization Fracture Risk Assessment Tool (FRAX): What they mean to the bone densitometrist and bone technologist. J. Clin. Densitom. 2008, 11, 473–477. [Google Scholar] [CrossRef]
- Wang, C.J.; Chen, H.S.; Chen, W.S.; Chen, L.M. Treatment of painful heels using extracorporeal shock wave. J. Formos. Med. Assoc. 2000, 99, 580–583. [Google Scholar]
- Rompe, J.D.; Hope, C.; Kullmer, K.; Heine, J.; Burger, R. Analgesic effect of extracorporeal shock-wave therapy on chronic tennis elbow. J. Bone Joint Surg. Br. 1996, 78, 233–237. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.S.; Yang, K.D.; Kuo, Y.R.; Wang, C.J.; Sheen-Chen, S.M.; Huang, H.C.; Chen, Y.J. Temporal and spatial expression of bone morphogenetic proteins in extracorporeal shock wave-promoted healing of segmental defect. Bone 2003, 32, 387–396. [Google Scholar] [CrossRef]
- Wang, C.J.; Huang, H.Y.; Yang, K.; Wang, F.S.; Wong, M. Pathomechanism of shock wave injuries on femoral artery, vein and nerve. An experimental study in dogs. Injury 2002, 33, 439–446. [Google Scholar] [CrossRef]
- Wang, C.J. Extracorporeal shockwave therapy in musculoskeletal disorders. J. Orthop. Surg. Res. 2012, 7, 11. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, K.; Tomita, K.; Takayama, K. Application of extracorporeal shock wave on bone: Preliminary report. J. Trauma 1999, 47, 946–950. [Google Scholar] [CrossRef]
- Chen, Y.J.; Wurtz, T.; Wang, C.J.; Kuo, Y.R.; Yang, K.D.; Huang, H.C.; Wang, F.S. Recruitment of mesenchymal stem cells and expression of TGF-beta 1 and VEGF in the early stage of shock wave-promoted bone regeneration of segmental defect in rats. J. Orthop. Res. 2004, 22, 526–534. [Google Scholar] [CrossRef]
- Romeo, P.; Lavanga, V.; Pagani, D.; Sansone, V. Extracorporeal shock wave therapy in musculoskeletal disorders: A review. Med. Princ. Pract. 2014, 23, 7–13. [Google Scholar] [CrossRef]
- Wang, C.J.; Wang, F.S.; Yang, K.D.; Weng, L.H.; Hsu, C.C.; Huang, C.S.; Yang, L.C. Shock wave therapy induces neovascularization at the tendon-bone junction. A study in rabbits. J. Orthop. Res. 2003, 21, 984–989. [Google Scholar] [CrossRef]
- Wang, C.J. An overview of shock wave therapy in musculoskeletal disorders. Chang. Gung. Med. J. 2003, 26, 220–232. [Google Scholar]
- Wang, C.J.; Wang, F.S.; Yang, K.D. Biological effects of extracorporeal shockwave in bone healing: A study in rabbits. Arch. Orthop. Trauma Surg. 2008, 128, 879–884. [Google Scholar] [CrossRef]
- Wang, C.J.; Huang, H.Y.; Pai, C.H. Shock wave-enhanced neovascularization at the tendon-bone junction: An experiment in dogs. J. Foot Ankle Surg. 2002, 41, 16–22. [Google Scholar] [CrossRef]
- Wang, C.J.; Huang, C.Y.; Hsu, S.L.; Chen, J.H.; Cheng, J.H. Extracorporeal shockwave therapy in osteoporotic osteoarthritis of the knee in rats: An experiment in animals. Arthritis Res. Ther. 2014, 16, R139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- d’Agostino, M.C.; Craig, K.; Tibalt, E.; Respizzi, S. Shock wave as biological therapeutic tool: From mechanical stimulation to recovery and healing, through mechanotransduction. Int. J. Surg. 2015, 24, 147–153. [Google Scholar] [CrossRef]
- Russo, S.; Servodidio, V.; Mosillo, G.; Sadile, F. Local and Systemic Effects of Extracorporeal Shockwave Therapy on Bone. In Shockwave Medicine; Karger Publishers: Berlin, Germany, 2018. [Google Scholar] [CrossRef]
- Wang, C.J.; Yang, Y.J.; Huang, C.C. The effects of shockwave on systemic concentrations of nitric oxide level, angiogenesis and osteogenesis factors in hip necrosis. Rheumatol. Int. 2011, 31, 871–877. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.S.; Yang, K.D.; Chen, R.F.; Wang, C.J.; Sheen-Chen, S.M. Extracorporeal shock wave promotes growth and differentiation of bone-marrow stromal cells towards osteoprogenitors associated with induction of TGF-beta1. J. Bone Joint Surg. Br. 2002, 84, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Tam, K.F.; Cheung, W.H.; Lee, K.M.; Qin, L.; Leung, K.S. Shockwave exerts osteogenic effect on osteoporotic bone in an ovariectomized goat model. Ultrasound. Med. Biol. 2009, 35, 1109–1118. [Google Scholar] [CrossRef] [PubMed]
- Lama, A.; Santoro, A.; Corrado, B.; Pirozzi, C.; Paciello, O.; Pagano, T.B.; Russo, S.; Calignano, A.; Mattace Raso, G.; Meli, R. Extracorporeal shock waves alone or combined with raloxifene promote bone formation and suppress resorption in ovariectomized rats. PLoS ONE 2017, 12, e0171276. [Google Scholar] [CrossRef]
- Kearney, C.J.; Hsu, H.P.; Spector, M. The Use of Extracorporeal Shock Wave-Stimulated Periosteal Cells for Orthotopic Bone Generation. Tissue Eng. Part A 2012, 18, 1500–1508. [Google Scholar] [CrossRef]
- Wang, R.N.; Green, J.; Wang, Z.; Deng, Y.; Qiao, M.; Peabody, M.; Zhang, Q.; Ye, J.; Yan, Z.; Denduluri, S.; et al. Bone Morphogenetic Protein (BMP) signaling in development and human diseases. Genes Dis. 2014, 1, 87–105. [Google Scholar] [CrossRef] [Green Version]
- Deng, Z.H.; Li, Y.S.; Gao, X.; Lei, G.H.; Huard, J. Bone morphogenetic proteins for articular cartilage regeneration. Osteoarthr. Cartil. 2018, 26, 1153–1161. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.-B.; Sui, C.; Wu, T.-T.; Wu, L.-Z.; Zhu, Y.-Y.; Ren, Z.-H. Association of Bone Morphogenetic Protein (BMP)/Smad Signaling Pathway with Fracture Healing and Osteogenic Ability in Senile Osteoporotic Fracture in Humans and Rats. Med Sci. Monit. 2018, 24, 4363–4371. [Google Scholar] [CrossRef]
- Wang, C.-J.; Huang, C.-C.; Yip, H.-K.; Yang, Y.-J. Dosage effects of extracorporeal shockwave therapy in early hip necrosis. Int. J. Surg. 2016, 35, 179–186. [Google Scholar] [CrossRef]
- Ma, H.-Z.; Zeng, B.-F.; Li, X.-L.; Chai, Y.-M. Temporal and spatial expression of BMP-2 in sub-chondral bone of necrotic femoral heads in rabbits by use of extracorporeal shock waves. Acta Orthop. 2009, 79, 98–105. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.-M.; Li, X.-L.; Tu, S.-Q.; Chen, X.-F.; Lu, C.-C.; Jiang, L.-H. Effects of Roughly Focused Extracorporeal Shock Waves Therapy on the Expressions of Bone Morphogenetic Protein-2 and Osteoprotegerin in Osteoporotic Fracture in Rats. Chin. Med J. 2016, 129, 2567–2575. [Google Scholar] [CrossRef]
- van der Jagt, O.P.; van der Linden, J.C.; Schaden, W.; van Schie, H.T.; Piscaer, T.M.; Verhaar, J.A.; Weinans, H.; Waarsing, J.H. Unfocused extracorporeal shock wave therapy as potential treatment for osteoporosis. J. Orthop. Res. 2009, 27, 1528–1533. [Google Scholar] [CrossRef]
- Giustina, A.; Mazziotti, G.; Canalis, E. Growth Hormone, Insulin-Like Growth Factors, and the Skeleton. Endocr. Rev. 2008, 29, 535–559. [Google Scholar] [CrossRef] [Green Version]
- Kanazawa, I.; Yamaguchi, T.; Sugimoto, T. Serum insulin-like growth factor-I is a marker for assessing the severity of vertebral fractures in postmenopausal women with type 2 diabetes mellitus. Osteoporos. Int. 2010, 22, 1191–1198. [Google Scholar] [CrossRef]
- Böttner, M.; Christoffel, J.; Wuttke, W. Effects of long-term treatment with 8-prenylnaringenin and oral estradiol on the GH–IGF-1 axis and lipid metabolism in rats. J. Endocrinol. 2008, 198, 395–401. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.-J.; Weng, L.-H.; Ko, J.-Y.; Sun, Y.-C.; Yang, Y.-J.; Wang, F.-S. Extracorporeal shockwave therapy shows chondroprotective effects in osteoarthritic rat knee. Arch. Orthop. Trauma Surg. 2011, 131, 1153–1158. [Google Scholar] [CrossRef]
- Shi, L.; Gao, F.; Sun, W.; Wang, B.; Guo, W.; Cheng, L.; Li, Z.; Wang, W. Short-term effects of extracorporeal shock wave therapy on bone mineral density in postmenopausal osteoporotic patients. Osteoporos. Int. 2017, 28, 2945–2953. [Google Scholar] [CrossRef]
- van der Jagt, O.P.; Piscaer, T.M.; Schaden, W.; Li, J.; Kops, N.; Jahr, H.; van der Linden, J.C.; Waarsing, J.H.; Verhaar, J.N.; de Jong, M.; et al. Unfocused Extracorporeal Shock Waves Induce Anabolic Effects in Rat Bone. J. Bone Joint Surg. Am. Vol. 2011, 93, 38–48. [Google Scholar] [CrossRef] [Green Version]
- Hayami, T.; Pickarski, M.; Zhuo, Y.; Wesolowski, G.A.; Rodan, G.A.; Duong, L.T. Characterization of articular cartilage and subchondral bone changes in the rat anterior cruciate ligament transection and meniscectomized models of osteoarthritis. Bone 2006, 38, 234–243. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Modulus | ||||
|---|---|---|---|---|
| Legs | Sham | OP | SW(F) 1 | SW(T) 1 |
| Right | 382.45 ± 73.33 * | 279.55 ± 37.91 | 412.81 ± 87.45 * | 314.15 ± 30.05 |
| Extension at peak load | ||||
| Legs | Sham | OP | SW(F) | SW(T) |
| Right | 0.82 ± 0.15 | 0.71 ± 0.10 | 0.88 ± 0.13 | 0.96 ± 0.14 * |
| Handleability | ||||
| Legs | Sham | OP | SW(F) | SW(T) |
| Right | 12.08 ± 3.56 | 11.85 ± 2.53 | 14.93 ± 1.59 | 16.99 ± 3.04 * |
| Strain at break | ||||
| Legs | Sham | OP | SW(F) | SW(T) |
| Right | 10.86 ± 2.03 | 9.45 ± 1.34 | 11.88 ± 1.33 | 12.79 ± 1.86 * |
| Bone Mineral Density (BMD; g/mm3) | ||||
| Legs | Sham | OP | SW(F) a | SW(T) a |
| Right | 0.46 ± 0.02 | 0.23 ± 0.01 | 0.27 ± 0.01 ** | 0.30 ± 0.01 ** |
| Left | 0.46 ± 0.03 | 0.23 ± 0.01 | 0.27 ± 0.01 ** | 0.31 ± 0.01 ** |
| Trabecular Thickness (TbTh; mm) | ||||
| Legs | Sham | OP | SW(F) | SW(T) |
| Right | 0.09 ± 0.01 | 0.09 ± 0.01 | 0.12 ± 0.01 *** | 0.12 ± 0.01 *** |
| Left | 0.09 ± 0.01 | 0.10 ± 0.01 | 0.11 ± 0.01 ** | 0.13 ± 0.01 ** |
| Bone Volume/Tissue Volume (BV/TV; %) | ||||
| Legs | Sham | OP | SW(F) | SW(T) |
| Right | 45.60 ± 0.04 | 27.84 ± 0.01 | 28.82 ± 0.05 | 31.61 ± 0.03 * |
| Left | 45.64 ± 0.06 | 27.16 ± 0.02 | 29.78 ± 0.03 | 32.89 ± 0.04 * |
| Porosity (%) | ||||
| Legs | Sham | OP | SW(F) | SW(T) |
| Right | 54.17 ± 3.15 | 72.16 ± 1.35 | 71.33 ± 4.76 | 68.15 ± 2.82 ** |
| Left | 53.83 ± 4.53 | 72.84 ± 1.57 | 70.06 ± 3.10 | 67.38 ± 3.89 ** |
| Bone Mineral Density (BMD; g/mm3) | ||||
| Legs | Sham | OP | SW(F) a | SW(T) a |
| Right | 0.42 ± 0.02 *** | 0.19 ± 0.01 | 0.18 ± 0.01 | 0.23 ± 0.01 * |
| Left | 0.41 ± 0.02 *** | 0.18 ± 0.01 | 0.18 ± 0.01 | 0.23 ± 0.01 * |
| Trabecular Thickness (TbTh; mm) | ||||
| Legs | Sham | OP | SW(F) | SW(T) |
| Right | 0.1 ± 0.01 | 0.1 ± 0.01 | 0.11 ± 0.01 | 0.1 ± 0.01 |
| Left | 0.1 ± 0.01 | 0.1 ± 0.01 | 0.1 ± 0.01 | 0.1 ± 0.01 |
| Bone Volume/Tissue Volume (BV/TV; %) | ||||
| Legs | Sham | OP | SW(F) | SW(T) |
| Right | 40.83 ± 1.67 *** | 19.33 ± 0.72 | 18.5 ± 0.62 | 23.97 ± 1.22 * |
| Left | 39.77 ± 1.60 *** | 19.03 ± 1.15 | 19.34 ± 0.77 | 23.38 ± 0.89 * |
| Porosity (%) | ||||
| Legs | Sham | OP | SW(F) | SW(T) |
| Right | 59.16 ± 1.67 *** | 80.67 ± 0.72 | 81.5 ± 0.62 | 76.03 ± 1.22 * |
| Left | 60.22 ± 1.60 *** | 80.97 ± 1.15 | 80.66 ± 0.77 | 75.6 ± 0.69 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, S.-L.; Chou, W.-Y.; Hsu, C.-C.; Ko, J.-Y.; Jhan, S.-W.; Wang, C.-J.; Lee, M.-S.; Hsu, T.-C.; Cheng, J.-H. Shockwave Therapy Modulates the Expression of BMP2 for Prevention of Bone and Cartilage Loss in the Lower Limbs of Postmenopausal Osteoporosis Rat Model. Biomedicines 2020, 8, 614. https://doi.org/10.3390/biomedicines8120614
Hsu S-L, Chou W-Y, Hsu C-C, Ko J-Y, Jhan S-W, Wang C-J, Lee M-S, Hsu T-C, Cheng J-H. Shockwave Therapy Modulates the Expression of BMP2 for Prevention of Bone and Cartilage Loss in the Lower Limbs of Postmenopausal Osteoporosis Rat Model. Biomedicines. 2020; 8(12):614. https://doi.org/10.3390/biomedicines8120614
Chicago/Turabian StyleHsu, Shan-Ling, Wen-Yi Chou, Chieh-Cheng Hsu, Jih-Yang Ko, Shun-Wun Jhan, Ching-Jen Wang, Meng-Shiou Lee, Tsai-Chin Hsu, and Jai-Hong Cheng. 2020. "Shockwave Therapy Modulates the Expression of BMP2 for Prevention of Bone and Cartilage Loss in the Lower Limbs of Postmenopausal Osteoporosis Rat Model" Biomedicines 8, no. 12: 614. https://doi.org/10.3390/biomedicines8120614