Advances in Cardiovascular Biomarker Discovery

 , , ,
, , ,  and
and
Abstract
:1. Hypertension
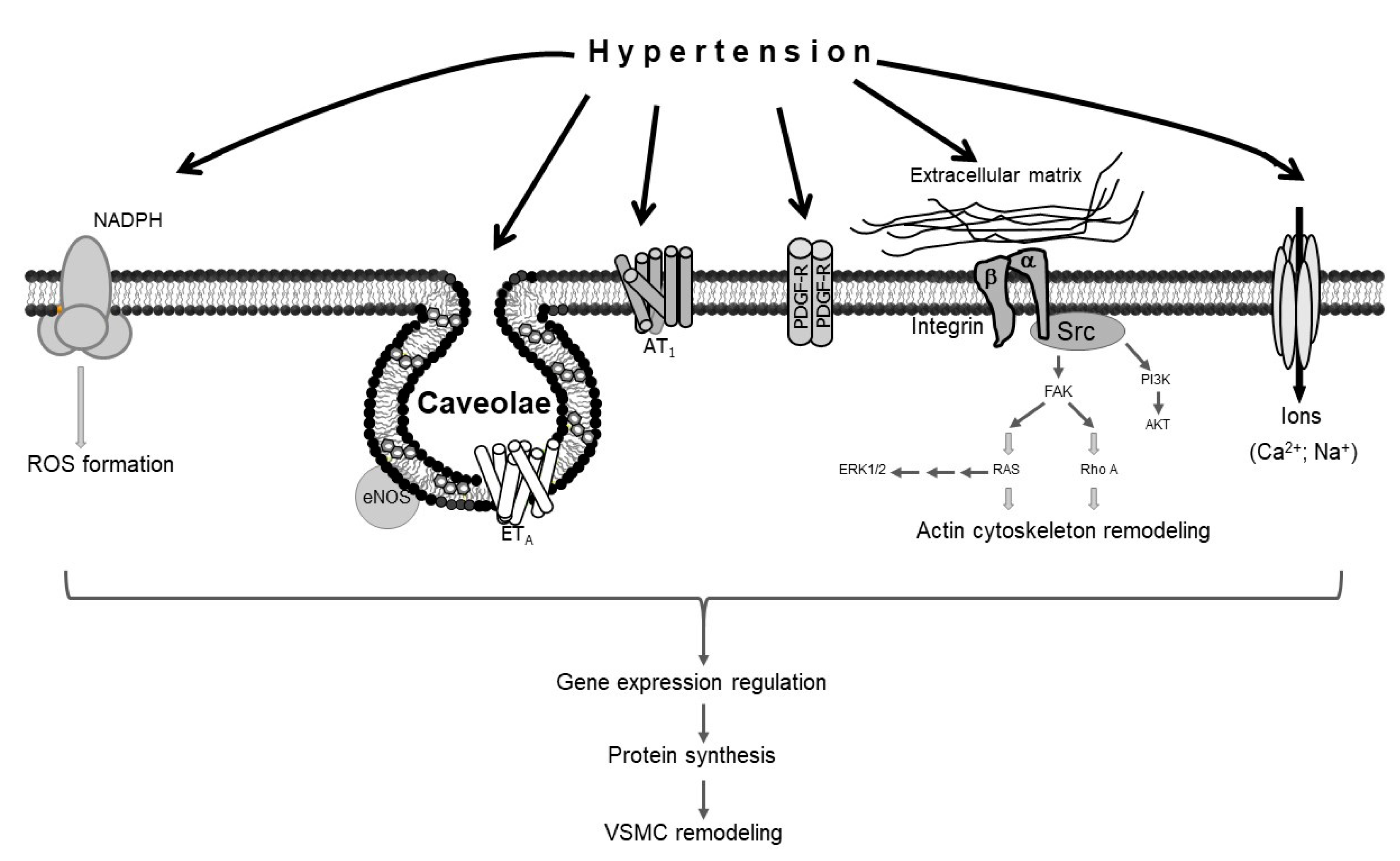
1.1. Hypertension and Vascular Smooth Muscle Cell Remodeling
1.2. Hypertension and Endothelial Dysfunction
2. Biomarkers
2.1. Classical Biomarkers of Cardiovascular Disease
2.2. Early Stage Biomarkers of Cardiovascular Disease
2.3. Second-Generation Biomarkers of Cardiovascular Disease
3. “Omics” and Systems Biology
3.1. Omics
3.2. Proteomic Advances in Detecting Vascular Diseases
4. Biomarkers Reflecting Hypertension Pathogenesis
4.1. Biomarkers Reflecting Oxidative Stress
4.2. Protein Biomarkers Reflecting Inflammation
4.3. Adipokines as Biomarkers of Hypertension
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Medicine, I.O. Cardiovascular disease. In A Nationwide Framework for Surveillance of Cardiovascular and Chronic Lung Diseases; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar]
- World Health Organization. Cardiovascular Diseases (cvds) Fact Sheet. Available online: http://www.who.int/mediacentre/factsheets/fs317/en/ (accessed on 17 October 2020).
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart disease and stroke statistics-2020 update: A report from the american heart association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef]
- Wang, G.; Grosse, S.D.; Schooley, M.W. Conducting research on the economics of hypertension to improve cardiovascular health. Am. J. Prev. Med. 2017, 53, S115–S117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levenson, J.W.; Skerrett, P.J.; Gaziano, J.M. Reducing the global burden of cardiovascular disease: The role of risk factors. Prev. Cardiol. 2002, 5, 188–199. [Google Scholar] [CrossRef]
- Carretero, O.A.; Oparil, S. Essential hypertension. Part I: Definition and etiology. Circulation 2000, 101, 329–335. [Google Scholar] [CrossRef]
- Sheppard, J.P.; Fletcher, K.; McManus, R.J.; Mant, J. Prevalence and costs of treating uncomplicated stage 1 hypertension in primary care: A cross-sectional analysis. Br. J. Gen. Pract. J. R. Coll. Gen. Pract. 2014, 64, e641–e648. [Google Scholar] [CrossRef] [Green Version]
- Giles, T.D.; Materson, B.J. Treating stage 2 hypertension. J. Clin. Hypertens. 2005, 7, 464–470. [Google Scholar] [CrossRef] [Green Version]
- Marteau, J.B.; Zaiou, M.; Siest, G.; Visvikis-Siest, S. Genetic determinants of blood pressure regulation. J. Hypertens. 2005, 23, 2127–2143. [Google Scholar] [CrossRef]
- Chiong, J.R.; Aronow, W.S.; Khan, I.A.; Nair, C.K.; Vijayaraghavan, K.; Dart, R.A.; Behrenbeck, T.R.; Geraci, S.A. Secondary hypertension: Current diagnosis and treatment. Int. J. Cardiol. 2008, 124, 6–21. [Google Scholar] [CrossRef]
- Lifton, R.P.; Gharavi, A.G.; Geller, D.S. Molecular mechanisms of human hypertension. Cell 2001, 104, 545–556. [Google Scholar] [CrossRef] [Green Version]
- Shyu, K.G. Cellular and molecular effects of mechanical stretch on vascular cells and cardiac myocytes. Clin. Sci. 2009, 116, 377–389. [Google Scholar] [CrossRef] [Green Version]
- Dharmashankar, K.; Widlansky, M.E. Vascular endothelial function and hypertension: Insights and directions. Curr. Hypertens. Rep. 2010, 12, 448–455. [Google Scholar] [CrossRef] [Green Version]
- Aalkjaer, C.; Heagerty, A.M.; Petersen, K.K.; Swales, J.D.; Mulvany, M.J. Evidence for increased media thickness, increased neuronal amine uptake, and depressed excitation—Contraction coupling in isolated resistance vessels from essential hypertensives. Circ. Res. 1987, 61, 181–186. [Google Scholar] [CrossRef] [Green Version]
- Arribas, S.M.; Hillier, C.; Gonzalez, C.; McGrory, S.; Dominiczak, A.F.; McGrath, J.C. Cellular aspects of vascular remodeling in hypertension revealed by confocal microscopy. Hypertension 1997, 30, 1455–1464. [Google Scholar] [CrossRef]
- Ghantous, C.M.; Kobeissy, F.H.; Soudani, N.; Rahman, F.A.; Al-Hariri, M.; Itani, H.A.; Sabra, R.; Zeidan, A. Mechanical stretch-induced vascular hypertrophy occurs through modulation of leptin synthesis-mediated ros formation and gata-4 nuclear translocation. Front. Pharm. 2015, 6, 240. [Google Scholar] [CrossRef]
- Nour-Eldine, W.; Ghantous, C.M.; Zibara, K.; Dib, L.; Issaa, H.; Itani, H.A.; El-Zein, N.; Zeidan, A. Adiponectin attenuates angiotensin ii-induced vascular smooth muscle cell remodeling through nitric oxide and the rhoa/rock pathway. Front. Pharm. 2016, 7, 86. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Zhang, M.J.; Li, B.H.; Chen, L.; Pi, Y.; Yin, Y.W.; Long, C.Y.; Wang, X.; Sun, M.J.; Chen, X.; et al. Ppargamma inhibits vsmc proliferation and migration via attenuating oxidative stress through upregulating ucp2. PLoS ONE 2016, 11, e0154720. [Google Scholar]
- Yoshizumi, M.; Kyotani, Y.; Zhao, J.; Nakahira, K. Targeting the mitogen-activated protein kinase-mediated vascular smooth muscle cell remodeling by angiotensin ii. Ann. Transl. Med. 2020, 8, 157. [Google Scholar] [CrossRef]
- Liu, P.; Gu, Y.; Luo, J.; Ye, P.; Zheng, Y.; Yu, W.; Chen, S. Inhibition of src activation reverses pulmonary vascular remodeling in experimental pulmonary arterial hypertension via akt/mtor/hif-1<alpha> signaling pathway. Exp. Cell Res. 2019, 380, 36–46. [Google Scholar] [CrossRef]
- Forrester, S.J.; Elliott, K.J.; Kawai, T.; Obama, T.; Boyer, M.J.; Preston, K.J.; Yan, Z.; Eguchi, S.; Rizzo, V. Caveolin-1 deletion prevents hypertensive vascular remodeling induced by angiotensin ii. Hypertension 2017, 69, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Lian, X.; Matthaeus, C.; Kassmann, M.; Daumke, O.; Gollasch, M. Pathophysiological role of caveolae in hypertension. Front. Med. 2019, 6, 153. [Google Scholar] [CrossRef]
- Titus, A.; Marappa-Ganeshan, R. Physiology, Endothelin; Statpearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Hinoki, A.; Kimura, K.; Higuchi, S.; Eguchi, K.; Takaguri, A.; Ishimaru, K.; Frank, G.D.; Gerthoffer, W.T.; Sommerville, L.J.; Autieri, M.V.; et al. P21-activated kinase 1 participates in vascular remodeling in vitro and in vivo. Hypertension 2010, 55, 161–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaminon, A.; Reesink, K.; Kroon, A.; Schurgers, L. The role of vascular smooth muscle cells in arterial remodeling: Focus on calcification-related processes. Int. J. Mol. Sci. 2019, 20, 5694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, I.A.M.; Diederich, L.; Good, M.E.; DeLalio, L.J.; Murphy, S.A.; Cortese-Krott, M.M.; Hall, J.L.; Le, T.H.; Isakson, B.E. Vascular smooth muscle remodeling in conductive and resistance arteries in hypertension. Arter. Thromb. Vasc. Biol. 2018, 38, 1969–1985. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Wen, J.; Wang, N.; Wang, C.; Xu, Q.; Yang, Y. Ion channels and vascular diseases. Arter. Thromb. Vasc. Biol. 2019, 39, e146–e156. [Google Scholar] [CrossRef] [PubMed]
- Vanhoutte, P.M.; Tang, E.H. Endothelium-dependent contractions: When a good guy turns bad! J. Physiol. 2008, 586, 5295–5304. [Google Scholar] [CrossRef]
- Versari, D.; Daghini, E.; Virdis, A.; Ghiadoni, L.; Taddei, S. Endothelium-dependent contractions and endothelial dysfunction in human hypertension. Br. J. Pharmacol. 2009, 157, 527–536. [Google Scholar] [CrossRef] [Green Version]
- Feletou, M.; Vanhoutte, P.M. Endothelial dysfunction: A multifaceted disorder (the wiggers award lecture). Am. J. Physiol. Heart Circ. Physiol. 2006, 291, H985–H1002. [Google Scholar] [CrossRef]
- Jia, G.; Durante, W.; Sowers, J.R. Endothelium-derived hyperpolarizing factors: A potential therapeutic target for vascular dysfunction in obesity and insulin resistance. Diabetes 2016, 65, 2118–2120. [Google Scholar] [CrossRef] [Green Version]
- Sitia, S.; Tomasoni, L.; Atzeni, F.; Ambrosio, G.; Cordiano, C.; Catapano, A.; Tramontana, S.; Perticone, F.; Naccarato, P.; Camici, P.; et al. From endothelial dysfunction to atherosclerosis. Autoimmun. Rev. 2010, 9, 830–834. [Google Scholar] [CrossRef]
- Taddei, S.; Ghiadoni, L.; Virdis, A.; Buralli, S.; Salvetti, A. Vasodilation to bradykinin is mediated by an ouabain-sensitive pathway as a compensatory mechanism for impaired nitric oxide availability in essential hypertensive patients. Circulation 1999, 100, 1400–1405. [Google Scholar] [CrossRef] [Green Version]
- Garcia de Tena, J. Inflammation, atherosclerosis, and coronary artery disease. N. Engl. J. Med. 2005, 353, 429–430; author reply 429–430. [Google Scholar] [PubMed] [Green Version]
- Li, J.J.; Chen, J.L. Inflammation may be a bridge connecting hypertension and atherosclerosis. Med. Hypotheses 2005, 64, 925–929. [Google Scholar] [CrossRef] [PubMed]
- Elkind, M.S. Inflammation, atherosclerosis, and stroke. Neurologist 2006, 12, 140–148. [Google Scholar] [CrossRef]
- Olin, J.W.; Sealove, B.A. Peripheral artery disease: Current insight into the disease and its diagnosis and management. Mayo Clin. Proc. 2010, 85, 678–692. [Google Scholar] [CrossRef] [Green Version]
- Berliner, J.A.; Navab, M.; Fogelman, A.M.; Frank, J.S.; Demer, L.L.; Edwards, P.A.; Watson, A.D.; Lusis, A.J. Atherosclerosis: Basic mechanisms. Oxidation, inflammation, and genetics. Circulation 1995, 91, 2488–2496. [Google Scholar] [CrossRef] [PubMed]
- Biomarkers Definitions Working, G. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar]
- Finley Austin, M.J.; Babiss, L. Commentary: Where and how could biomarkers be used in 2016? Aaps. J. 2006, 8, E185–E189. [Google Scholar] [CrossRef] [Green Version]
- Muszynski, P.; Groblewska, M.; Kulczynska-Przybik, A.; Kulakowska, A.; Mroczko, B. Ykl-40 as a potential biomarker and a possible target in therapeutic strategies of alzheimer’s disease. Curr. Neuropharmacol. 2017, 15, 906–917. [Google Scholar] [CrossRef] [Green Version]
- Krumholz, H.M. Biomarkers, risk factors, and risk: Clarifying the controversy about surrogate end points and clinical outcomes. Circ. Cardiovasc. Qual. Outcomes 2015, 8, 457–459. [Google Scholar] [CrossRef] [Green Version]
- Vasan, R.S. Biomarkers of cardiovascular disease: Molecular basis and practical considerations. Circulation 2006, 113, 2335–2362. [Google Scholar] [CrossRef]
- Wilson, P.W.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of coronary heart disease using risk factor categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef] [Green Version]
- Lowe, G.D.; Yarnell, J.W.; Rumley, A.; Bainton, D.; Sweetnam, P.M. C-reactive protein, fibrin d-dimer, and incident ischemic heart disease in the speedwell study: Are inflammation and fibrin turnover linked in pathogenesis? Arter. Thromb. Vasc. Biol. 2001, 21, 603–610. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.Y.; Chan, C.C.; Su, T.C. Particulate and gaseous pollutants on inflammation, thrombosis, and autonomic imbalance in subjects at risk for cardiovascular disease. Environ. Pollut. 2017, 223, 403–408. [Google Scholar] [CrossRef]
- Omland, T.; White, H.D. State of the art: Blood biomarkers for risk stratification in patients with stable ischemic heart disease. Clin. Chem. 2017, 63, 165–176. [Google Scholar] [CrossRef] [Green Version]
- Strandberg, T.E.; Tilvis, R.S. C-reactive protein, cardiovascular risk factors, and mortality in a prospective study in the elderly. Arter. Thromb. Vasc. Biol. 2000, 20, 1057–1060. [Google Scholar] [CrossRef] [Green Version]
- Pfutzner, A.; Forst, T. High-sensitivity c-reactive protein as cardiovascular risk marker in patients with diabetes mellitus. Diabetes Technol. Ther. 2006, 8, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Apple, F.S.; Collinson, P.O.; Biomarkers, I.T.F.o.C.A.o.C. Analytical characteristics of high-sensitivity cardiac troponin assays. Clin. Chem. 2012, 58, 54–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scirica, B.M.; Morrow, D.A. Troponins in acute coronary syndromes. Prog. Cardiovasc. Dis. 2004, 47, 177–188. [Google Scholar] [CrossRef]
- Di Angelantonio, E.; Chowdhury, R.; Sarwar, N.; Ray, K.K.; Gobin, R.; Saleheen, D.; Thompson, A.; Gudnason, V.; Sattar, N.; Danesh, J. B-type natriuretic peptides and cardiovascular risk: Systematic review and meta-analysis of 40 prospective studies. Circulation 2009, 120, 2177–2187. [Google Scholar] [CrossRef]
- Tokita, Y.; Kusama, Y.; Kodani, E.; Tadera, T.; Nakagomi, A.; Atarashi, H.; Mizuno, K. Utility of rapid d-dimer measurement for screening of acute cardiovascular disease in the emergency setting. J. Cardiol. 2009, 53, 334–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alehagen, U.; Dahlstrom, U.; Lindahl, T.L. Elevated d-dimer level is an independent risk factor for cardiovascular death in out-patients with symptoms compatible with heart failure. Thromb. Haemost. 2004, 92, 1250–1258. [Google Scholar] [PubMed] [Green Version]
- Landry, A.; Docherty, P.; Ouellette, S.; Cartier, L.J. Causes and outcomes of markedly elevated c-reactive protein levels. Can. Fam. Physician Med. Fam. Can. 2017, 63, e316–e323. [Google Scholar]
- Zimmermann, O.; Li, K.; Zaczkiewicz, M.; Graf, M.; Liu, Z.; Torzewski, J. C-reactive protein in human atherogenesis: Facts and fiction. Mediat. Inflamm 2014, 2014, 561428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Han, H.; Yan, X.; Ding, F.; Su, X.; Wang, H.; Chen, Q.; Lu, L.; Zhang, R.; Jin, W. Tetranectin as a potential biomarker for stable coronary artery disease. Sci. Rep. 2015, 5, 17632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, Y.; Zhao, S.; Gong, Y.; Hou, G.; Li, X.; Li, L. Serum cyclin-dependent kinase 9 is a potential biomarker of atherosclerotic inflammation. Oncotarget 2016, 7, 1854–1862. [Google Scholar] [CrossRef] [PubMed]
- Simonini, M.; Pozzoli, S.; Bignami, E.; Casamassima, N.; Messaggio, E.; Lanzani, C.; Frati, E.; Botticelli, I.M.; Rotatori, F.; Alfieri, O.; et al. Endogenous ouabain: An old cardiotonic steroid as a new biomarker of heart failure and a predictor of mortality after cardiac surgery. Biomed. Res. Int. 2015, 2015, 714793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brea, D.; Sobrino, T.; Blanco, M.; Fraga, M.; Agulla, J.; Rodriguez-Yanez, M.; Rodriguez-Gonzalez, R.; Perez de la Ossa, N.; Leira, R.; Forteza, J.; et al. Usefulness of haptoglobin and serum amyloid a proteins as biomarkers for atherothrombotic ischemic stroke diagnosis confirmation. Atherosclerosis 2009, 205, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Ceholski, D.K.; Trieber, C.A.; Young, H.S. Hydrophobic imbalance in the cytoplasmic domain of phospholamban is a determinant for lethal dilated cardiomyopathy. J. Biol. Chem. 2012, 287, 16521–16529. [Google Scholar] [CrossRef] [Green Version]
- Hochholzer, W.; Morrow, D.A.; Giugliano, R.P. Novel biomarkers in cardiovascular disease: Update 2010. Am. Heart J. 2010, 160, 583–594. [Google Scholar] [CrossRef]
- Heslop, C.L.; Frohlich, J.J.; Hill, J.S. Myeloperoxidase and c-reactive protein have combined utility for long-term prediction of cardiovascular mortality after coronary angiography. J. Am. Coll. Cardiol. 2010, 55, 1102–1109. [Google Scholar] [CrossRef] [Green Version]
- Calmarza, P.; Lapresta, C.; Martinez, M.; Lahoz, R.; Povar, J. Utility of Myeloperoxidase in the Differential Diagnosis of Acute Coronary Syndrome; Universidad de Zaragoza Repository: Zaragoza, Spain, 2017. [Google Scholar]
- Huang, A.; Huang, Y. Role of sfrps in cardiovascular disease. Ther. Adv. Chronic. Dis. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Askevold, E.T.; Aukrust, P.; Nymo, S.H.; Lunde, I.G.; Kaasboll, O.J.; Aakhus, S.; Florholmen, G.; Ohm, I.K.; Strand, M.E.; Attramadal, H.; et al. The cardiokine secreted frizzled-related protein 3, a modulator of wnt signalling, in clinical and experimental heart failure. J. Intern. Med. 2014, 275, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Meuwese, M.C.; Stroes, E.S.; Hazen, S.L.; van Miert, J.N.; Kuivenhoven, J.A.; Schaub, R.G.; Wareham, N.J.; Luben, R.; Kastelein, J.J.; Khaw, K.T.; et al. Serum myeloperoxidase levels are associated with the future risk of coronary artery disease in apparently healthy individuals: The epic-norfolk prospective population study. J. Am. Coll. Cardiol. 2007, 50, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Ndrepepa, G.; Braun, S.; Mehilli, J.; von Beckerath, N.; Schomig, A.; Kastrati, A. Myeloperoxidase level in patients with stable coronary artery disease and acute coronary syndromes. Eur. J. Clin. Investig. 2008, 38, 90–96. [Google Scholar] [CrossRef]
- Zhang, R.; Brennan, M.L.; Fu, X.; Aviles, R.J.; Pearce, G.L.; Penn, M.S.; Topol, E.J.; Sprecher, D.L.; Hazen, S.L. Association between myeloperoxidase levels and risk of coronary artery disease. Jama 2001, 286, 2136–2142. [Google Scholar] [CrossRef]
- Shridas, P.; Tannock, L.R. Role of serum amyloid a in atherosclerosis. Curr. Opin. Lipidol. 2019, 30, 320–325. [Google Scholar] [CrossRef]
- He, Y.; Ma, C.; Xing, J.; Wang, S.; Ji, C.; Han, Y.; Zhang, J. Serum amyloid a protein as a potential biomarker in predicting acute onset and association with in-hospital death in acute aortic dissection. Bmc Cardiovasc. Disord. 2019, 19, 282. [Google Scholar] [CrossRef]
- Johnson, B.D.; Kip, K.E.; Marroquin, O.C.; Ridker, P.M.; Kelsey, S.F.; Shaw, L.J.; Pepine, C.J.; Sharaf, B.; Bairey Merz, C.N.; Sopko, G.; et al. Serum amyloid a as a predictor of coronary artery disease and cardiovascular outcome in women: The national heart, lung, and blood institute-sponsored women’s ischemia syndrome evaluation (wise). Circulation 2004, 109, 726–732. [Google Scholar] [CrossRef] [Green Version]
- Krishack, P.A.; Bhanvadia, C.V.; Lukens, J.; Sontag, T.J.; De Beer, M.C.; Getz, G.S.; Reardon, C.A. Serum amyloid a facilitates early lesion development in ldlr-/- mice. J. Am. Heart Assoc. 2015, 4, e001858. [Google Scholar] [CrossRef] [Green Version]
- Wilson, A.M.; Kimura, E.; Harada, R.K.; Nair, N.; Narasimhan, B.; Meng, X.Y.; Zhang, F.; Beck, K.R.; Olin, J.W.; Fung, E.T.; et al. Beta2-microglobulin as a biomarker in peripheral arterial disease: Proteomic profiling and clinical studies. Circulation 2007, 116, 1396–1403. [Google Scholar] [CrossRef] [Green Version]
- Curaj, A.; Wu, Z.; Rix, A.; Gresch, O.; Sternkopf, M.; Alampour-Rajabi, S.; Lammers, T.; van Zandvoort, M.; Weber, C.; Koenen, R.R.; et al. Molecular ultrasound imaging of junctional adhesion molecule a depicts acute alterations in blood flow and early endothelial dysregulation. Arter. Thromb. Vasc. Biol. 2018, 38, 40–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soeki, T.; Tamura, Y.; Shinohara, H.; Sakabe, K.; Onose, Y.; Fukuda, N. Increased soluble platelet/endothelial cell adhesion molecule-1 in the early stages of acute coronary syndromes. Int. J. Cardiol. 2003, 90, 261–268. [Google Scholar] [CrossRef]
- Ku, E.J.; Cho, K.C.; Lim, C.; Kang, J.W.; Oh, J.W.; Choi, Y.R.; Park, J.M.; Han, N.Y.; Oh, J.J.; Oh, T.J.; et al. Discovery of plasma biomarkers for predicting the severity of coronary artery atherosclerosis by quantitative proteomics. BMJ Open Diabetes Res. Care 2020, 8, e001152. [Google Scholar] [CrossRef] [Green Version]
- Soung, Y.H.; Ford, S.; Zhang, V.; Chung, J. Exosomes in cancer diagnostics. Cancers 2017, 9, 8. [Google Scholar] [CrossRef] [Green Version]
- Sarko, D.K.; McKinney, C.E. Exosomes: Origins and therapeutic potential for neurodegenerative disease. Front. Neurosci. 2017, 11, 82. [Google Scholar] [CrossRef] [Green Version]
- Cheow, E.S.; Cheng, W.C.; Lee, C.N.; de Kleijn, D.; Sorokin, V.; Sze, S.K. Plasma-derived extracellular vesicles contain predictive biomarkers and potential therapeutic targets for myocardial ischemic injury. Mol. Cell. Proteom. Mcp 2016, 15, 2628–2640. [Google Scholar] [CrossRef] [Green Version]
- Poe, A.J.; Knowlton, A.A. Exosomes as agents of change in the cardiovascular system. J. Mol. Cell Cardiol. 2017, 111, 40–50. [Google Scholar] [CrossRef]
- Valadi, H.; Ekstrom, K.; Bossios, A.; Sjostrand, M.; Lee, J.J.; Lotvall, J.O. Exosome-mediated transfer of mrnas and micrornas is a novel mechanism of genetic exchange between cells. Nat. Cell Biol. 2007, 9, 654–659. [Google Scholar] [CrossRef] [Green Version]
- Cordes, K.R.; Srivastava, D. Microrna regulation of cardiovascular development. Circ. Res. 2009, 104, 724–732. [Google Scholar] [CrossRef]
- Hunter, M.P.; Ismail, N.; Zhang, X.; Aguda, B.D.; Lee, E.J.; Yu, L.; Xiao, T.; Schafer, J.; Lee, M.L.; Schmittgen, T.D.; et al. Detection of microrna expression in human peripheral blood microvesicles. PLoS ONE 2008, 3, e3694. [Google Scholar] [CrossRef] [Green Version]
- Zernecke, A.; Bidzhekov, K.; Noels, H.; Shagdarsuren, E.; Gan, L.; Denecke, B.; Hristov, M.; Koppel, T.; Jahantigh, M.N.; Lutgens, E.; et al. Delivery of microrna-126 by apoptotic bodies induces cxcl12-dependent vascular protection. Sci. Signal. 2009, 2, ra81. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, J.D.; Chevillet, J.R.; Kroh, E.M.; Ruf, I.K.; Pritchard, C.C.; Gibson, D.F.; Mitchell, P.S.; Bennett, C.F.; Pogosova-Agadjanyan, E.L.; Stirewalt, D.L.; et al. Argonaute2 complexes carry a population of circulating micrornas independent of vesicles in human plasma. Proc. Natl. Acad. Sci. USA 2011, 108, 5003–5008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vickers, K.C.; Palmisano, B.T.; Shoucri, B.M.; Shamburek, R.D.; Remaley, A.T. Micrornas are transported in plasma and delivered to recipient cells by high-density lipoproteins. Nat. Cell Biol. 2011, 13, 423–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corsten, M.F.; Dennert, R.; Jochems, S.; Kuznetsova, T.; Devaux, Y.; Hofstra, L.; Wagner, D.R.; Staessen, J.A.; Heymans, S.; Schroen, B. Circulating microrna-208b and microrna-499 reflect myocardial damage in cardiovascular disease. Circ. Cardiovasc. Genet. 2010, 3, 499–506. [Google Scholar] [CrossRef]
- Huang, Z.; Huang, D.; Ni, S.; Peng, Z.; Sheng, W.; Du, X. Plasma micrornas are promising novel biomarkers for early detection of colorectal cancer. Int. J. Cancer. J. Int. Du Cancer 2010, 127, 118–126. [Google Scholar] [CrossRef]
- Khalyfa, A.; Gozal, D. Exosomal mirnas as potential biomarkers of cardiovascular risk in children. J. Transl. Med. 2014, 12, 162. [Google Scholar] [CrossRef] [Green Version]
- Ji, X.; Takahashi, R.; Hiura, Y.; Hirokawa, G.; Fukushima, Y.; Iwai, N. Plasma mir-208 as a biomarker of myocardial injury. Clin. Chem. 2009, 55, 1944–1949. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Yuan, Y.; Yang, P.; Li, X. Extracellular vesicles-mediated transfer of mir-208a/b exaggerate hypoxia/reoxygenation injury in cardiomyocytes by reducing qki expression. Mol. Cell Biochem. 2017, 431, 187–195. [Google Scholar] [CrossRef]
- Schroen, B.; Heymans, S. Small but smart--micrornas in the centre of inflammatory processes during cardiovascular diseases, the metabolic syndrome, and ageing. Cardiovasc. Res. 2012, 93, 605–613. [Google Scholar] [CrossRef] [Green Version]
- Kuehbacher, A.; Urbich, C.; Zeiher, A.M.; Dimmeler, S. Role of dicer and drosha for endothelial microrna expression and angiogenesis. Circ. Res. 2007, 101, 59–68. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Gorski, D.H. Regulation of angiogenesis through a microrna (mir-130a) that down-regulates antiangiogenic homeobox genes gax and hoxa5. Blood 2008, 111, 1217–1226. [Google Scholar] [CrossRef] [PubMed]
- Urbich, C.; Kuehbacher, A.; Dimmeler, S. Role of micrornas in vascular diseases, inflammation, and angiogenesis. Cardiovasc. Res. 2008, 79, 581–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Gomez, M.C.; Garcia-Mejia, K.A.; Perez-Diaz Conti, M.; Diaz-Rosas, G.; Palma-Lara, I.; Sanchez-Urbina, R.; Klunder-Klunder, M.; Botello-Flores, J.A.; Balderrabano-Saucedo, N.A.; Contreras-Ramos, A. Micrornas association in the cardiac hypertrophy secondary to complex congenital heart disease in children. Pediatric Cardiol. 2017, 38, 991–1003. [Google Scholar] [CrossRef] [PubMed]
- Abu-Halima, M.; Meese, E.; Keller, A.; Abdul-Khaliq, H.; Radle-Hurst, T. Analysis of circulating micrornas in patients with repaired tetralogy of fallot with and without heart failure. J. Transl. Med. 2017, 15, 156. [Google Scholar] [CrossRef] [PubMed]
- Maciejak, A.; Kiliszek, M.; Opolski, G.; Segiet, A.; Matlak, K.; Dobrzycki, S.; Tulacz, D.; Sygitowicz, G.; Burzynska, B.; Gora, M. Mir-22-5p revealed as a potential biomarker involved in the acute phase of myocardial infarction via profiling of circulating micrornas. Mol. Med. Rep. 2016, 14, 2867–2875. [Google Scholar] [CrossRef]
- Njock, M.S.; Fish, J.E. Endothelial mirnas as cellular messengers in cardiometabolic diseases. Trends Endocrinol. Metab. 2017, 28, 237–246. [Google Scholar] [CrossRef]
- Rotllan, N.; Price, N.; Pati, P.; Goedeke, L.; Fernandez-Hernando, C. Micrornas in lipoprotein metabolism and cardiometabolic disorders. Atherosclerosis 2016, 246, 352–360. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Cao, H.; Zhuang, J.; Wan, J.; Guan, M.; Yu, B.; Li, X.; Zhang, W. Identification of mir-130a, mir-27b and mir-210 as serum biomarkers for atherosclerosis obliterans. Clin. Chim. Acta 2011, 412, 66–70. [Google Scholar] [CrossRef]
- Han, H.; Qu, G.; Han, C.; Wang, Y.; Sun, T.; Li, F.; Wang, J.; Luo, S. Mir-34a, mir-21 and mir-23a as potential biomarkers for coronary artery disease: A pilot microarray study and confirmation in a 32 patient cohort. Exp. Mol. Med. 2015, 47, e138. [Google Scholar] [CrossRef] [Green Version]
- Schlosser, K.; White, R.J.; Stewart, D.J. Mir-26a linked to pulmonary hypertension by global assessment of circulating extracellular micrornas. Am. J. Respir. Crit. Care Med. 2013, 188, 1472–1475. [Google Scholar] [CrossRef]
- Derda, A.A.; Thum, S.; Lorenzen, J.M.; Bavendiek, U.; Heineke, J.; Keyser, B.; Stuhrmann, M.; Givens, R.C.; Kennel, P.J.; Schulze, P.C.; et al. Blood-based microrna signatures differentiate various forms of cardiac hypertrophy. Int. J. Cardiol. 2015, 196, 115–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, C.; Wang, Q.; You, W.; Chen, M.; Xia, J. Mirnas as biomarkers of myocardial infarction: A meta-analysis. PLoS ONE 2014, 9, e88566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, W.; Shao, J.; Bai, X.; Zhang, G. Expression of plasma microrna-1/21/ 208a/499 in myocardial ischemic reperfusion injury. Cardiology 2015, 130, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Song, Y.; Huang, J.; Qu, M.; Zhang, Y.; Geng, J.; Zhang, Z.; Liu, J.; Yang, G.Y. Increased circulating exosomal mirna-223 is associated with acute ischemic stroke. Front. Neurol. 2017, 8, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, S.H.; Huang, M.; Kelly, R.S.; Benedetti, E.; Siddiqui, J.K.; Zeleznik, O.A.; Pereira, A.; Herrington, D.; Wheelock, C.E.; Krumsiek, J.; et al. Integration of metabolomic and other omics data in population-based study designs: An epidemiological perspective. Metabolites 2019, 9, 117. [Google Scholar] [CrossRef] [Green Version]
- Mbasu, R.J.; Heaney, L.M.; Molloy, B.J.; Hughes, C.J.; Ng, L.L.; Vissers, J.P.; Langridge, J.I.; Jones, D.J. Advances in quadrupole and time-of-flight mass spectrometry for peptide mrm based translational research analysis. Proteomics 2016, 16, 2206–2220. [Google Scholar] [CrossRef] [Green Version]
- Bruggeman, F.J.; Westerhoff, H.V. The nature of systems biology. Trends Microbiol. 2007, 15, 45–50. [Google Scholar] [CrossRef]
- Kislinger, T.; Emili, A. Going global: Protein expression profiling using shotgun mass spectrometry. Curr. Opin. Mol. Ther. 2003, 5, 285–293. [Google Scholar]
- Izquierdo, I.; Rosa, I.; Bravo, S.B.; Guitian, E.; Perez-Serra, A.; Campuzano, O.; Brugada, R.; Mangas, A.; Garcia, A.; Toro, R. Proteomic identification of putative biomarkers for early detection of sudden cardiac death in a family with a lmna gene mutation causing dilated cardiomyopathy. J. Proteom. 2016, 148, 75–84. [Google Scholar] [CrossRef]
- Binek, A.; Fernandez-Jimenez, R.; Jorge, I.; Camafeita, E.; Lopez, J.A.; Bagwan, N.; Galan-Arriola, C.; Pun, A.; Aguero, J.; Fuster, V.; et al. Proteomic footprint of myocardial ischemia/reperfusion injury: Longitudinal study of the at-risk and remote regions in the pig model. Sci. Rep. 2017, 7, 12343. [Google Scholar] [CrossRef]
- Nagai-Okatani, C.; Minamino, N. Aberrant glycosylation in the left ventricle and plasma of rats with cardiac hypertrophy and heart failure. PLoS ONE 2016, 11, e0150210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossing, K.; Bosselmann, H.S.; Gustafsson, F.; Zhang, Z.Y.; Gu, Y.M.; Kuznetsova, T.; Nkuipou-Kenfack, E.; Mischak, H.; Staessen, J.A.; Koeck, T.; et al. Urinary proteomics pilot study for biomarker discovery and diagnosis in heart failure with reduced ejection fraction. PLoS ONE 2016, 11, e0157167. [Google Scholar] [CrossRef]
- Slevin, M.; Elasbali, A.B.; Miguel Turu, M.; Krupinski, J.; Badimon, L.; Gaffney, J. Identification of differential protein expression associated with development of unstable human carotid plaques. Am. J. Pathol. 2006, 168, 1004–1021. [Google Scholar] [CrossRef] [Green Version]
- Montezano, A.C.; Touyz, R.M. Molecular mechanisms of hypertension--reactive oxygen species and antioxidants: A basic science update for the clinician. Can. J. Cardiol. 2012, 28, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Nagababu, E.; Rifkind, J.M. Measurement of plasma nitrite by chemiluminescence. Methods Mol. Biol. 2010, 610, 41–49. [Google Scholar]
- Casey, D.P.; Beck, D.T.; Braith, R.W. Systemic plasma levels of nitrite/nitrate (nox) reflect brachial flow-mediated dilation responses in young men and women. Clin. Exp. Pharm. Physiol. 2007, 34, 1291–1293. [Google Scholar] [CrossRef]
- Palm, F.; Onozato, M.L.; Luo, Z.; Wilcox, C.S. Dimethylarginine dimethylaminohydrolase (ddah): Expression, regulation, and function in the cardiovascular and renal systems. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H3227–H3245. [Google Scholar] [CrossRef] [Green Version]
- Xiao, S.; Wagner, L.; Mahaney, J.; Baylis, C. Uremic levels of urea inhibit l-arginine transport in cultured endothelial cells. Am. J. Physiol. Ren. Physiol. 2001, 280, F989–F995. [Google Scholar] [CrossRef]
- Paiva, H.; Kahonen, M.; Lehtimaki, T.; Alfthan, G.; Viikari, J.; Laaksonen, R.; Hutri-Kahonen, N.; Laitinen, T.; Taittonen, L.; Raitakari, O.T.; et al. Levels of asymmetrical dimethylarginine are predictive of brachial artery flow-mediated dilation 6 years later. The cardiovascular risk in young finns study. Atherosclerosis 2010, 212, 512–515. [Google Scholar] [CrossRef]
- Juonala, M.; Viikari, J.S.; Alfthan, G.; Marniemi, J.; Kahonen, M.; Taittonen, L.; Laitinen, T.; Raitakari, O.T. Brachial artery flow-mediated dilation and asymmetrical dimethylarginine in the cardiovascular risk in young finns study. Circulation 2007, 116, 1367–1373. [Google Scholar] [CrossRef] [Green Version]
- Loeffler, L.F.; Navas-Acien, A.; Brady, T.M.; Miller, E.R., 3rd; Fadrowski, J.J. Uric acid level and elevated blood pressure in us adolescents: National health and nutrition examination survey, 1999–2006. Hypertension 2012, 59, 811–817. [Google Scholar] [CrossRef] [Green Version]
- Valkonen, V.P.; Paiva, H.; Salonen, J.T.; Lakka, T.A.; Lehtimaki, T.; Laakso, J.; Laaksonen, R. Risk of acute coronary events and serum concentration of asymmetrical dimethylarginine. Lancet 2001, 358, 2127–2128. [Google Scholar] [CrossRef]
- Rassaf, T.; Heiss, C.; Hendgen-Cotta, U.; Balzer, J.; Matern, S.; Kleinbongard, P.; Lee, A.; Lauer, T.; Kelm, M. Plasma nitrite reserve and endothelial function in the human forearm circulation. Free Radic. Biol. Med. 2006, 41, 295–301. [Google Scholar] [CrossRef]
- Touyz, R.M.; Briones, A.M. Reactive oxygen species and vascular biology: Implications in human hypertension. Hypertens. Res. Off. J. Jpn. Soc. Hypertens. 2011, 34, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.J.; Kang, D.H.; Feig, D.; Kivlighn, S.; Kanellis, J.; Watanabe, S.; Tuttle, K.R.; Rodriguez-Iturbe, B.; Herrera-Acosta, J.; Mazzali, M. Is there a pathogenetic role for uric acid in hypertension and cardiovascular and renal disease? Hypertension 2003, 41, 1183–1190. [Google Scholar] [CrossRef] [Green Version]
- Harrison, D.G.; Guzik, T.J.; Lob, H.E.; Madhur, M.S.; Marvar, P.J.; Thabet, S.R.; Vinh, A.; Weyand, C.M. Inflammation, immunity, and hypertension. Hypertension 2011, 57, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Sprague, A.H.; Khalil, R.A. Inflammatory cytokines in vascular dysfunction and vascular disease. Biochem. Pharmacol. 2009, 78, 539–552. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, S.F.; de Oliveira, M.A.; dos Santos, R.A.; Soares, A.G.; de Cassia Tostes, R.; Carvalho, M.H.; Fortes, Z.B. Hydralazine reduces leukocyte migration through different mechanisms in spontaneously hypertensive and normotensive rats. Eur. J. Pharm. 2008, 589, 206–214. [Google Scholar] [CrossRef]
- De Ciuceis, C.; Amiri, F.; Brassard, P.; Endemann, D.H.; Touyz, R.M.; Schiffrin, E.L. Reduced vascular remodeling, endothelial dysfunction, and oxidative stress in resistance arteries of angiotensin ii-infused macrophage colony-stimulating factor-deficient mice: Evidence for a role in inflammation in angiotensin-induced vascular injury. Arter. Thromb. Vasc. Biol. 2005, 25, 2106–2113. [Google Scholar] [CrossRef] [Green Version]
- Preston, R.A.; Ledford, M.; Materson, B.J.; Baltodano, N.M.; Memon, A.; Alonso, A. Effects of severe, uncontrolled hypertension on endothelial activation: Soluble vascular cell adhesion molecule-1, soluble intercellular adhesion molecule-1 and von willebrand factor. J. Hypertens. 2002, 20, 871–877. [Google Scholar] [CrossRef]
- Barbaro, N.R.; Fontana, V.; Modolo, R.; De Faria, A.P.; Sabbatini, A.R.; Fonseca, F.H.; Anhe, G.F.; Moreno, H. Increased arterial stiffness in resistant hypertension is associated with inflammatory biomarkers. Blood Press 2015, 24, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Bautista, L.E.; Vera, L.M.; Arenas, I.A.; Gamarra, G. Independent association between inflammatory markers (c-reactive protein, interleukin-6, and tnf-alpha) and essential hypertension. J. Hum. Hypertens. 2005, 19, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Shalia, K.K.; Mashru, M.R.; Vasvani, J.B.; Mokal, R.A.; Mithbawkar, S.M.; Thakur, P.K. Circulating levels of cell adhesion molecules in hypertension. Indian J. Clin. Biochem. 2009, 24, 388–397. [Google Scholar] [CrossRef] [Green Version]
- Oguz, M.M.; Oguz, A.D.; Sanli, C.; Cevik, A. Serum levels of soluble icam-1 in children with pulmonary artery hypertension. Tex. Heart Inst. J. 2014, 41, 159–164. [Google Scholar] [CrossRef]
- Kuklinska, A.M.; Mroczko, B.; Musial, W.J.; Usowicz-Szarynska, M.; Sawicki, R.; Borowska, H.; Knapp, M.; Szmitkowski, M. Diagnostic biomarkers of essential arterial hypertension: The value of prostacyclin, nitric oxide, oxidized-ldl, and peroxide measurements. Int. Heart J. 2009, 50, 341–351. [Google Scholar] [CrossRef]
- Hage, F.G. C-reactive protein and hypertension. J. Hum. Hypertens. 2014, 28, 410–415. [Google Scholar] [CrossRef]
- Mehaffey, E.; Majid, D.S.A. Tumor necrosis factor-alpha, kidney function, and hypertension. Am. J. Physiol. Ren. Physiol. 2017, 313, F1005–F1008. [Google Scholar] [CrossRef] [Green Version]
- Yang, P.; Liu, Y.F.; Yang, L.; Wei, Q.; Zeng, H. Mechanism and clinical significance of the prothrombotic state in patients with essential hypertension. Clin. Cardiol. 2010, 33, E81–E86. [Google Scholar] [CrossRef]
- Jan Danser, A.H. Renin and prorenin as biomarkers in hypertension. Curr. Opin. Nephrol. Hypertens. 2012, 21, 508–514. [Google Scholar] [CrossRef]
- Asferg, C.; Mogelvang, R.; Flyvbjerg, A.; Frystyk, J.; Jensen, J.S.; Marott, J.L.; Appleyard, M.; Jensen, G.B.; Jeppesen, J. Leptin, not adiponectin, predicts hypertension in the copenhagen city heart study. Am J Hypertens. 2010, 23, 327–333. [Google Scholar] [CrossRef]
- Shankar, A.; Xiao, J. Positive relationship between plasma leptin level and hypertension. Hypertension 2010, 56, 623–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.H.; Kim, C.; Ding, E.L.; Townsend, M.K.; Lipsitz, L.A. Adiponectin levels and the risk of hypertension: A systematic review and meta-analysis. Hypertension 2013, 62, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghantous, C.M.; Azrak, Z.; Hanache, S.; Abou-Kheir, W.; Zeidan, A. Differential role of leptin and adiponectin in cardiovascular system. Int. J. Endocrinol. 2015, 2015, 534320. [Google Scholar] [CrossRef] [PubMed]
- Kaisar, O.M.; Johnson, D.W.; Prins, J.B.; Isbel, N. The role of novel biomarkers of cardiovascular disease in chronic kidney disease: Focus on adiponectin and leptin. Curr. Cardiol. Rev. 2008, 4, 287–292. [Google Scholar] [CrossRef] [Green Version]
- Soudani, N.; Ghantous, C.M.; Farhat, Z.; Shebaby, W.N.; Zibara, K.; Zeidan, A. Calcineurin/nfat activation-dependence of leptin synthesis and vascular growth in response to mechanical stretch. Front. Physiol. 2016, 7, 433. [Google Scholar] [CrossRef] [Green Version]
- de Haro Moraes, C.; Figueiredo, V.N.; de Faria, A.P.; Barbaro, N.R.; Sabbatini, A.R.; Quinaglia, T.; Ferreira-Melo, S.E.; Martins, L.C.; Demacq, C.; Junior, H.M. High-circulating leptin levels are associated with increased blood pressure in uncontrolled resistant hypertension. J. Hum. Hypertens. 2013, 27, 225–230. [Google Scholar] [CrossRef] [Green Version]
- Schafer, K.; Halle, M.; Goeschen, C.; Dellas, C.; Pynn, M.; Loskutoff, D.J.; Konstantinides, S. Leptin promotes vascular remodeling and neointimal growth in mice. Arter. Thromb. Vasc. Biol. 2004, 24, 112–117. [Google Scholar] [CrossRef] [Green Version]
- Ebrahimi-Mamaeghani, M.; Mohammadi, S.; Arefhosseini, S.R.; Fallah, P.; Bazi, Z. Adiponectin as a potential biomarker of vascular disease. Vasc. Health Risk Manag. 2015, 11, 55–70. [Google Scholar]
- Shibata, R.; Sato, K.; Pimentel, D.R.; Takemura, Y.; Kihara, S.; Ohashi, K.; Funahashi, T.; Ouchi, N.; Walsh, K. Adiponectin protects against myocardial ischemia-reperfusion injury through ampk- and cox-2-dependent mechanisms. Nat. Med. 2005, 11, 1096–1103. [Google Scholar] [CrossRef] [PubMed]
- Shibata, R.; Ouchi, N.; Ito, M.; Kihara, S.; Shiojima, I.; Pimentel, D.R.; Kumada, M.; Sato, K.; Schiekofer, S.; Ohashi, K.; et al. Adiponectin-mediated modulation of hypertrophic signals in the heart. Nat. Med. 2004, 10, 1384–1389. [Google Scholar] [CrossRef] [Green Version]
- Gonon, A.T.; Widegren, U.; Bulhak, A.; Salehzadeh, F.; Persson, J.; Sjoquist, P.O.; Pernow, J. Adiponectin protects against myocardial ischaemia-reperfusion injury via amp-activated protein kinase, akt, and nitric oxide. Cardiovasc. Res. 2008, 78, 116–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghantous, C.M.; Farhat, R.; Djouhri, L.; Alashmar, S.; Anlar, G.; Korashy, H.M.; Agouni, A.; Zeidan, A. Molecular mechanisms of adiponectin-induced attenuation of mechanical stretch-mediated vascular remodeling. Oxidative Med. Cell. Longev. 2020, 2020, 6425782. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Proteins Associated with CVD | Function/Description | Type of CVD They Help Diagnose | Levels in CVD | Reference(s) |
|---|---|---|---|---|
| C-reactive protein (CRP) | Pattern recognition molecule that is increased in inflammation or tissue injury | Inflammatory conditions (atherosclerosis) | Elevated | [55,56] |
| Cardiac troponin I (cTnI) | The subunit of troponin that binds to actin and maintains the troponin-tropomyosin complex | Acute myocardial infarction and acute coronary syndrome | Elevated | [50] |
| Cardiac troponin T (cTnT) | The subunit of troponin that binds to tropomyosin to form a troponin-tropomyosin complex | Acute myocardial infarction and acute coronary syndrome | Elevated | [50] |
| B-type natriuretic peptides (BNP and NT-proBNP) | Reduces plasma volume and blood pressure | Ventricular hypertrophy and acute and chronic heart failure | Elevated | [52] |
| D-dimer | Fibrin degradation product from fibrinolysis of blood clots | Thrombosis, ischemic heart disease, acute aortic dissection, cardiovascular mortality | Elevated | [46,53] |
| Tetranectin | Binds to kringle 4 of circulating plasminogen, upregulating the activation of plasminogen into plasmin in fibrinolysis | Presence and severity of diseased coronary arteries | Elevated | [57] |
| Serum cyclin-dependent kinase 9 | Regulation of cell cycle and activation of inflammatory response genes | Atherosclerotic inflammation | Elevated | [58] |
| Endogenous ouabain | Glycoside that inhibits the Na+/K+-ATPase | Heart Failure | Elevated | [59] |
| Haptoglobin | Acute phase protein that binds to hemoglobin and also has antioxidant activity | Atherothrombotic ischemic stroke | Elevated | [60] |
| Serum amyloid A | Acute phase protein that increases the expression of pro-thrombotic and pro-inflammatory molecules | Atherothrombotic ischemic stroke | Elevated | [60] |
| Proteins Associated with CVD | Function/Description | Type of CVD They Help Diagnose | Changes/Levels in CVD | Reference(s) |
|---|---|---|---|---|
| Phospholamban | Regulates cardiac contractility by inhibiting sarco/endoplasmic reticulum calcium transport ATPase (SERCA) in its dephosphorylated form | Early onset of dilated cardiomyopathy and heart failure | Dominant Arg-> Cys mutation at residue 9 (loss-of-function mutation) | [61] |
| Myeloperoxidase (MPO) | - Catalyzes the formation of hyperchlorite from chloride and hydrogen peroxide - Bactericidal agent produced by monocytes and activated neutrophils - Promotes oxidation of LDL and oxidative modification of apolipoprotein A-I | Unstable atheroma, coronary artery disease, ischemic heart disease, stroke | Elevated | [67,68,69] |
| Secreted frizzled related proteins (sFRPs) | Modulate Wnt signaling | Myocardial infarction and heart failure | Elevated | [65,66] |
| Serum amyloid A | Acute phase protein that increases the expression of pro-thrombotic and pro-inflammatory molecules | Coronary artery disease, atherosclerotic plaque destabilization, acute aortic dissection | Elevated | [70,71,72,73] |
| β 2-microglobulin | Membrane protein that associates with heavy chains of class I major histocompatibility complex proteins | Peripheral arterial disease | Elevated | [74] |
| Junctional adhesion molecule A (JAM-A) | Regulates tight junction permeability and integrity of endothelial and epithelial cells | Acute endothelial activation and dysfunction | Elevated | [75] |
| Platelet/endothelial cell adhesion molecule-1 (PECAM-1) | Transduces mechanical signals in endothelial cells and regulates migration of leukocytes through the endothelium | Acute coronary syndromes | Elevated | [76] |
| Vitamin D-binding protein (VTDB) | Binds to vitamin D and its plasma metabolites and transports them to target tissues | Coronary artery stenosis | Reduced | [77] |
| Non-Proteins Associated with CVD | Type of CVD They Help Diagnose | Changes/Levels in CVD | Reference(s) |
|---|---|---|---|
| miR-208b and miR-499 | Acute myocardial infarction | Elevated | [88,91] |
| miR-21, miR-130a, miR-27b, and miR-210 | Atherosclerosis obliterans and peripheral arterial disease | Elevated | [102] |
| miR-221 and miR-222 | Atherosclerosis obliterans and peripheral arterial disease | Decreased | [102] |
| miR-34a, miR-21 and miR-23a | Coronary artery disease | Elevated | [103] |
| miR-26a | Hypertension | Decreased | [104] |
| miR-29a | Obstructive cardiomyopathy | Elevated | [105] |
| miR-29c | Aortic stenosis | Elevated | [105] |
| miR-499 and miR-133a | Myocardial infarction | Elevated | [106] |
| miR-1, miR-208a, and miR-499 | Myocardial ischemic reperfusion injury | Elevated | [107] |
| miR-223 | Acute ischemic stroke | Elevated | [108] |
| Molecule | Function/Description | Levels in Hypertension | Reference(s) |
|---|---|---|---|
| Nitrate and nitrite | Physiological reservoir of NO that can be reduced to NO to regulate signal transduction | Elevated | [120,127] |
| Asymmetric dimethylarginine (ADMA) | Inhibits nitric oxide synthase | Elevated | [123] |
| Reactive oxygen species (ROS) | Highly reactive signal transduction molecules that cause nucleic acid, lipid, and protein damage when present in high concentrations (oxidative stress) | Elevated | [118,128] |
| Uric acid | Final oxidation product of purine metabolism | Elevated | [125,129] |
| Inflammatory Mediators | Function/Description | Levels in Hypertension | Reference(s) |
|---|---|---|---|
| Vascular cell adhesion molecule (VCAM) | Endothelial cell surface glycoprotein that allows endothelial cell-leukocyte adhesion in inflammation | Elevated | [137] |
| Intercellular adhesion molecule (ICAM) | Endothelial cell surface glycoprotein that aids in endothelial cell-leukocyte adhesion | Elevated | [138] |
| Platelet endothelial cell adhesion molecule (PECAM) | Cell surface protein of platelets, monocytes, neutrophils, subsets of T cells that aids in leukocyte transendothelial migration, and a constituent of the endothelial intercellular junctions | Elevated | [132] |
| 6-keto-prostaglandin F1a | Stable and active metabolite of prostacyclin that promotes vasodilation and inhibits platelet aggregation | Reduced | [139] |
| C-reactive protein (CRP) | Activates complement and binds to foreign and damaged cells and tissue | Elevated | [140] |
| Tumor necrosis factor (TNF-α) | Pro-inflammatory cytokine involved in apoptosis, cell proliferation, differentiation, and platelet activation | Elevated | [136,141] |
| IL-10, IL-1β | IL-10: Cytokine involved in mediating the inflammatory response, B cell survival, proliferation and antibody production, and nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) activity IL-1β: Cytokine involved in regulating the inflammatory response, cell proliferation, differentiation, apoptosis, and cyclooxygenase-2 induction | Elevated | [135] |
| IL-6 | Immune response in inflammation | Elevated | [136] |
| P-selectin | Cell adhesion molecule of platelets and endothelial cells that works in the interaction of leukocytes with platelets or endothelial cells | Elevated | [142] |
| Oxidized-LDL | Taken up by macrophages to form foam cells, a key step in atherosclerosis development | Elevated | [139] |
| Renin and prorenin | Renin hydrolyzes angiotensinogen to angiotensin I, while prorenin is its inactive precursor | Elevated | [143] |
| Leptin | - Hormone mainly produced by adipocytes that acts as a satiety factor to increase energy expenditure by signaling at the hypothalamus - Promotes VSMC hypertrophy - Pro-inflammatory cytokine - Regulates puberty, menstrual cycles, and reproductive function | Elevated | [144,145] |
| Adiponectin | - Insulin-sensitization and fatty acid oxidation - Anti-inflammatory - Cardioprotective | Reduced | [146] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghantous, C.M.; Kamareddine, L.; Farhat, R.; Zouein, F.A.; Mondello, S.; Kobeissy, F.; Zeidan, A. Advances in Cardiovascular Biomarker Discovery. Biomedicines 2020, 8, 552. https://doi.org/10.3390/biomedicines8120552
Ghantous CM, Kamareddine L, Farhat R, Zouein FA, Mondello S, Kobeissy F, Zeidan A. Advances in Cardiovascular Biomarker Discovery. Biomedicines. 2020; 8(12):552. https://doi.org/10.3390/biomedicines8120552
Chicago/Turabian StyleGhantous, Crystal M., Layla Kamareddine, Rima Farhat, Fouad A. Zouein, Stefania Mondello, Firas Kobeissy, and Asad Zeidan. 2020. "Advances in Cardiovascular Biomarker Discovery" Biomedicines 8, no. 12: 552. https://doi.org/10.3390/biomedicines8120552