Oral and Psychological Alterations in Haemophiliac Patients

 , ,
, ,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Material and Methods
2.1. Protocol and Registration
2.2. Focus Question
- Is there a correlation between haemophilia and oral and dental alterations? Is their main pathology a risk factor for oral diseases?
- Is there a correlation between haemophilia and psychological conditions?
2.3. Information Sources
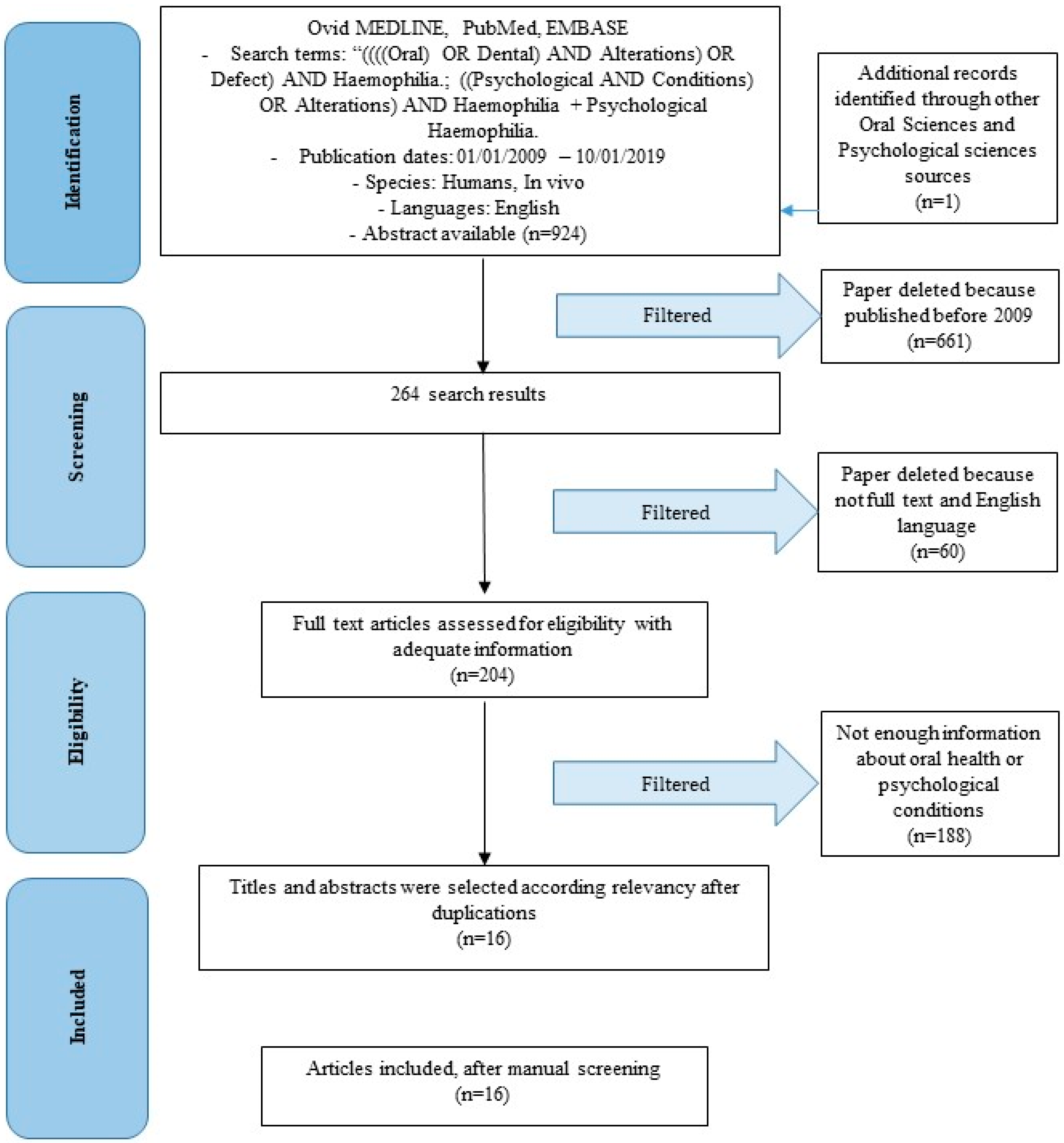
2.4. Search
- ((((Oral) OR Dental) AND Alterations) OR Defect) AND Haemophilia + Dental Haemophilia.
- ((Psychological AND Conditions) OR Alterations) AND Haemophilia + Psychological Haemophilia.
2.5. Selection of Studies
2.6. Types of Selected Manuscripts
2.7. Types of Studies
2.8. Disease Definition
2.8.1. Haemophilia
2.8.2. Oral Alterations with Genetic Diseases
2.8.3. Psychological Aspects of Patients with Systemic Diseases
2.8.4. Dentistry and Psychology
2.9. Inclusion and Exclusion Criteria
- Correlation between oral, dental alterations and haemophilia
- Psychological condition of haemophilic patients
- Articles published prior to 1 January 2009
- Studies involving patients with other specific diseases
- Not enough information supporting this review
- No access to the title and abstract
2.10. Sequential Search Strategy
2.11. Data Extraction
2.12. Data Collections
2.13. Risk of Bias Assessment
3. Results
3.1. Study Selection
3.2. Study Characteristics
- Dental Caries.
- Gengivitis/parodontitis.
- DMFT.
- Hemarthrosis.
- Bleeding.
- Pain.
- Psychological issues.
- Sexual Dysfunction and psychological issues.
3.3. Risk of Bias within Studies
3.4. Risk of Bias across Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Harold, R.R. Haemophilia and Haemostasis: A Case-Based Approach to Management; Wiley-Blackwell: Hoboken, NJ, USA, 2008; ISBN 978-0-470-76643-9. [Google Scholar]
- Green, D. Haemophilia and Von Willebrand Disease; Academic Press: Cambridge, MA, USA, 2018; ISBN 9780128129548. [Google Scholar]
- Peyvandi, F.; Garagiola, I.; Young, G. The past and future of haemophilia: Diagnosis, treatments, and its complications. Lancet 2016, 388, 187–197. [Google Scholar] [CrossRef]
- Brody, H. Haemophilia. Nature 2014, 515, S157. [Google Scholar] [CrossRef]
- Bertamino, M.; Riccardi, F.; Banov, L.; Svahn, J.; Molinari, A.C. Hemophilia Care in the Pediatric Age. J. Clin. Med. 2017, 6, 54. [Google Scholar] [CrossRef]
- Giampaolo, A.; Abbonizio, F.; Arcieri, R.; Hassan, H.J. Italian Registry of Congenital Bleeding Disorders. J. Clin. Med. 2017, 6, 34. [Google Scholar] [CrossRef]
- Torres-Ortuño, A.; Cid-Sabatel, R.; Barbero, J.; García-Dasí, M. Life experience of the adult and ageing patient with haemophilia. Practical aspects for psychological support. Vox. Sang. 2017, 112, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Cicciù, M.; Matacena, G.; Signorino, F.; Brugaletta, A.; Cicciù, A.; Bramanti, E. Relationship between oral health and its impact on the quality life of Alzheimer’s disease patients: A supportive care trial. Int. J. Clin. Exp. Med. 2013, 6, 766–772. [Google Scholar] [PubMed]
- Isola, G.; Ramaglia, L.; Cordasco, G.; Lucchese, A.; Fiorillo, L.; Matarese, G. The effect of a functional appliance in the management of temporomandibular joint disorders in patients with juvenile idiopathic arthritis. Minerva Stomatol. 2017, 66, 1–8. [Google Scholar]
- Crespel, A.; Ferlazzo, E.; Franceschetti, S.; Genton, P.; Gouider, R.; Kälviäinen, R.; Korja, M.; Lehtinen, K.M.; Mervaala, E.; Simonato, M.; et al. Unverricht-Lundborg disease. Epileptic Disord. 2016, 18. [Google Scholar] [CrossRef]
- Ferlazzo, E.; Gagliano, A.; Calarese, T.; Magaudda, A.; Striano, P.; Cortese, L.; Cedro, C.; Laguitton, V.; Bramanti, P.; Carbonaro, M.; et al. Neuropsychological findings in patients with Unverricht-Lundborg disease. Epilepsy Behav. 2009, 14, 545–549. [Google Scholar] [CrossRef]
- Hithersay, R.; Hamburg, S.; Knight, B.; Strydom, A. Cognitive decline and dementia in Down syndrome. Curr. Opin. Psychiatry. 2017, 30, 102–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seligman, L.D.; Hovey, J.D.; Chacon, K.; Ollendick, T.H. Dental anxiety: An understudied problem in youth. Clin Psychol Rev. 2017, 55, 25–40. [Google Scholar] [CrossRef]
- Beaudette, J.R.; Fritz, P.C.; Sullivan, P.J.; Ward, W.E. Oral Health, Nutritional Choices, and Dental Fear and Anxiety. Dent. J. 2017, 5, 8. [Google Scholar] [CrossRef] [PubMed]
- Lamarca, G.A.; Vettore, M.V.; Monteiro da Silva, A.M. The Influence of Stress and Anxiety on the Expectation, Perception and Memory of Dental Pain in Schoolchildren. Dent. J. 2018, 6, 60. [Google Scholar] [CrossRef] [PubMed]
- van Wijk, A.J.; Hoogstraten, J. Anxiety and pain during dental injections. J. Dent. 2009, 37, 700–704. [Google Scholar] [CrossRef]
- Adeyemo, T.A.; Adeyemo, W.L.; Adediran, A.; Akinbami, A.J.; Akanmu, A.S. Orofacial manifestations of hematological disorders: Anemia and hemostatic disorders. Indian J. Dent. Res. 2011, 22, 454–461. [Google Scholar] [CrossRef]
- Zaliuniene, R.; Peciuliene, V.; Brukiene, V.; Aleksejuniene, J. Hemophilia and oral health. Stomatologija 2014, 16, 127–131. [Google Scholar]
- Segna, E.; Artoni, A.; Giannì, A.B. Oral Surgery in Patients withGianzmann Thrombasthenia: A Case Series. J. Oral Maxillofac. Surg. 2017, 75, 256–259. [Google Scholar] [CrossRef]
- Kumar, R.; Carcao, M. Inherited Abnormalities of Coagulation. Pediatric Clin. North Am. 2013, 60, 1419–1441. [Google Scholar] [CrossRef] [PubMed]
- Krüger, S.; Hoffmeister, M.; Hilberg, T. Pain and structural alterations in knee joints in patients with haemophilia. Haemophilia 2018, 24, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Krüger, S.; Boettger, M.K.; Hilberg, T. Somatosensory profile of patients with haemophilia. Haemophilia 2018, 24, 97–103. [Google Scholar] [CrossRef]
- Roussel, N.A. Gaining insight into the complexity of pain in patients with haemophilia: State-of-the-art review on pain processing. Haemophilia 2018, 24 (Suppl. 6), 3–8. [Google Scholar] [CrossRef] [Green Version]
- McLintock, C. Women with bleeding disorders: Clinical and psychological issues. Haemophilia 2018, 24 (Suppl. 6), 22–28. [Google Scholar] [CrossRef] [PubMed]
- Limperg, P.F.; Haverman, L.; Beijlevelt, M.; van der Pot, M.; Zaal, G.; de Boer, W.A.; Fijnvandraat, K.; Peters, M.; Grootenhuis, M.A. Psychosocial care for children with haemophilia and their parents in the Netherlands. Haemophilia 2017, 23, 362–369. [Google Scholar] [CrossRef] [PubMed]
- García-Dasí, M.; Torres-Ortuño, A.; Cid-Sabatel, R.; Barbero, J. Practical aspects of psychological support to the patient with haemophilia from diagnosis in infancy through childhood and adolescence. Haemophilia 2016, 22, e349–e358. [Google Scholar] [CrossRef] [PubMed]
- Giordano, P.; Lassandro, G.; Valente, M.; Molinari, A.C.; Ieranò, P.; Coppola, A. Current management of the hemophilic child: A demanding interlocutor. Quality of life and adequate cost-efficacy analysis. Pediatr. Hematol. Oncol. 2014, 31, 687–702. [Google Scholar] [CrossRef] [PubMed]
- Cassis, F.R.; Querol, F.; Forsyth, A.; Iorio, A.; HERO International Advisory Board. Psychosocial aspects of haemophilia: A systematic review of methodologies and findings. Haemophilia 2012, 18, e101–e114. [Google Scholar] [CrossRef] [PubMed]
- Bar-Chama, N.; Snyder, S.; Aledort, L. Sexual evaluation and treatment of ageing males with haemophilia. Haemophilia 2011, 17, 875–883. [Google Scholar] [CrossRef]
- Coppola, A.; Cerbone, A.M.; Mancuso, G.; Mansueto, M.F.; Mazzini, C.; Zanon, E. Confronting the psychological burden of haemophilia. Haemophilia 2011, 17, 21–27. [Google Scholar] [CrossRef]
- Mauser-Bunschoten, E.P.; Fransen Van De Putte, D.E.; Schutgens, R.E. Co-morbidity in the ageing haemophilia patient: The down side of increased life expectancy. Haemophilia 2009, 15, 853–863. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G. Assessing Risk of Bias in Included Studies. In Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series; Higgins, J.P.T., Green, S., Eds.; Wiley Online Library: Hoboken, NJ, USA, 2008; pp. 187–241. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/9780470712184.ch8 (accessed on 19 April 2019).
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Fiorillo, L.; Cervino, G.; Herford, A.S.; Lauritano, F.; D’Amico, C.; Lo Giudice, R.; Laino, L.; Troiano, G.; Crimi, S.; Cicciù, M. Interferon crevicular fluid profile and correlation with periodontal disease and wound healing: A systemic review of recent data. Int. J. Mol. Sci. 2018, 19, 1908. [Google Scholar] [CrossRef] [PubMed]
- Matarese, G.; Ramaglia, L.; Fiorillo, L.; Cervino, G.; Lauritano, F.; Isola, G. Implantology and Periodontal Disease: The Panacea to Problem Solving? Open Dent. J. 2017, 11, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Cicciù, M.; Cervino, G.; Herford, A.S.; Famà, F.; Bramanti, E.; Fiorillo, L.; Lauritano, F.; Sambataro, S.; Troiano, G.; Laino, L. Facial Bone Reconstruction Using both Marine or Non-Marine Bone Substitutes: Evaluation of Current Outcomes in a Systematic Literature Review. Mar. Drugs 2018, 16, 27. [Google Scholar] [CrossRef] [PubMed]
- Cicciù, M. Neurodegenerative Disorders and Periodontal Disease: Is There a Logical Connection? Neuroepidemiology 2016, 47, 94–95. [Google Scholar] [CrossRef] [PubMed]
- Cervino, G.; Fiorillo, L.; Spagnuolo, G.; Bramanti, E.; Laino, L.; Lauritano, F.; Cicciù, M. Interface between MTA and dental bonding agents: Scanning electron microscope evaluation. J. Int. Soc. Prev. Community Dent. 2017, 7, 64–68. [Google Scholar]
- Kaneda, T.; Nagayama, M.; Ohmori, M.; Minato, F.; Nakajima, J.; Shikimori, M. Hemarthrosis of the temporomandibular joint in a patient with hemophilia B: Report of case. J. Oral Surg. 1979, 37, 513–514. [Google Scholar]
- Nishioka, G.J.; Van Sickels, J.E.; Tilson, H.B. Hemophilic arthropathy of the temporomandibular joint: Review of the literature, a case report, and discussion. Oral Surg. Oral Med. Oral Pathol. 1988, 65, 145–150. [Google Scholar] [CrossRef]
- Sonis, A.L.; Musselman, R.J. Oral bleeding in classic haemophilia. Oral Surg. Oral Med. Oral Pathol. 1982, 53, 363–366. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Laino, L.; Herford, A.S.; Lauritano, F.; Lo Giudice, G.; Famà, F.; Santoro, R.; Troiano, G.; Iannello, G.; et al. Oral health impact profile in celiac patients: Analysis of recent findings in a literature review. Gastroenterol. Res. Pract. 2018. [Google Scholar] [CrossRef]
- Nelson, L.P.; Getzin, A.; Graham, D.; Zhou, J.; Wagle, E.M.; McQuiston, J.; McLaughlin, S.; Govind, A.; Sadof, M.; Huntington, N.L. Unmet dental needs and barriers to care for children with significant special health care needs. Pediatr. Dent. 2011, 33, 29–36. [Google Scholar]
- Cervino, G.; Terranova, A.; Briguglio, F.; De Stefano, R.; Famà, F.; D’Amico, C.; Amoroso, G.; Marino, S.; Gorassini, F.; Mastroieni, R.; et al. Diabetes: Oral health related quality of life and oral alterations. BioMed Res. Int. 2019. [Google Scholar] [CrossRef]
- Laino, L.; Cicciù, M.; Fiorillo, L.; Crimi, S.; Bianchi, A.; Amoroso, G.; Monte, I.P.; Herford, A.S.; Cervino, G. Surgical Risk on Patients with Coagulopathies: Guidelines on Hemophiliac Patients for Oro-Maxillofacial Surgery. Int. J. Environ. Res. Public Health 2019, 16, 1386. [Google Scholar] [CrossRef]
- Beretta, M.; Cicciù, M.; Bramanti, E.; Maiorana, C. Schneider membrane elevation in presence of sinus septa: Anatomic features and surgical management. Int. J. Dent. 2012. [Google Scholar] [CrossRef] [PubMed]
- Rancitelli, D.; Borgonovo, A.E.; Cicciù, M.; Re, D.; Rizza, F.; Frigo, A.C.; Maiorana, C. Maxillary sinus septa and anatomic correlation with the Schneiderian membrane. J. Craniofacial Surg. 2015, 26, 1394–1398. [Google Scholar] [CrossRef] [PubMed]
- Maridati, P.; Stoffella, E.; Speroni, S.; Cicciu, M.; Maiorana, C. Alveolar antral artery isolation during sinus lift procedure with the double window technique. Open Dent. J. 2014, 8, 95–103. [Google Scholar] [CrossRef]
- Poli, P.P.; Beretta, M.; Cicciù, M.; Maiorana, C. Alveolar ridge augmentation with titanium mesh. A retrospective clinical study. Open Dent. J. 2014, 8, 148–158. [Google Scholar] [CrossRef]
- Lombardi, T.; Bernardello, F.; Berton, F.; Porrelli, D.; Rapani, A.; Piloni, A.C.; Fiorillo, L.; DI Lenarda, R.; Stacchi, C.; Tozum, T. Efficacy of Alveolar Ridge Preservation after Maxillary Molar Extraction in Reducing Crestal Bone Resorption and Sinus Pneumatization: A Multicenter Prospective Case-Control Study. BioMed Res. Int. 2018, 2018, 9352130. [Google Scholar] [CrossRef] [PubMed]
- Cervino, G.; Fiorillo, L.; Herford, A.S.; Romeo, U.; Bianchi, A.; Crimi, S.; D’Amico, C.; De Stefano, R.; Troiano, G.; Santoro, R.; et al. Molecular biomarkers related to oral carcinoma: Clinical trial outcome evaluation in a literature review. Dis. Markers 2019, 2019, 8040361. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year of Publications | Alterations and Conditions Highlighted |
|---|---|---|
| Adeyemo, et al. [17] | 2011 | Temporo-mandibular Joint (TMJ) hemarthrosis, TMJ pain, Oral district bleeding |
| Zaliuniene, et al. [18] | 2014 | Higher DMFT index, inflammatory disorders (gingivitis, periodontitis), bone loss, dental caries, gum health |
| Segna, et al [19] | 2017 | Oral district bleeding |
| Kumar, et al. [20] | 2013 | Oral district bleeding |
| Krüger, et al. [21] | 2018 | Enhanced pain sensitivity |
| Krüger, et al. [22] | 2018 | Alterations of the somatosensory profile |
| Roussel, et al. [23] | 2018 | Nociceptive alterations |
| McLintock, et al. [24] | 2018 | Psychological issues in women with Bleeding Disorders |
| Limperg, et al. [25] | 2017 | Psychosocial risk |
| Torres-Ortuño, et al. [7] | 2017 | Psychological issues |
| García-Dasí, et al. [26] | 2016 | Psychological issues |
| Giordano, et al. [27] | 2014 | Psychological issues |
| Cassis, et al. [28] | 2012 | Psychological issues and quality of life |
| Bar-Chama, et al. [29] | 2011 | Psychological issues and sexual dysfunctions |
| Coppola, et al. [30] | 2011 | Psychological issues |
| Mauser-Bunschoten, et al. [31] | 2009 | Psychosocial issues during ageing |
| Steps | Instructions |
|---|---|
| 1 | Dental extraction or surgical procedures carried out within the oral cavity should be performed with a plan for haemostasis management, in consultation with the haematologist. |
| 2 | Tranexamic acid or epsilon aminocaproic acid (EACA) is often used after dental procedures to reduce the need for replacement therapy. |
| 3 | Oral antibiotics should only be prescribed if clinically necessary. |
| 4 | Local haemostatic measures may also be used whenever possible following a dental extraction. Typical products include oxidized cellulose and fibrin glue. |
| 5 | Following a tooth extraction, the patient should be advised to avoid hot food and drinks until normal feeling has returned. Smoking should be avoided as this can cause problems with healing. Regular warm salt water mouthwashes (a teaspoon of salt in a glass of warm water) should begin the day after treatment and continue for 5–7 days or until the mouth has healed. |
| 6 | Prolonged bleeding and/or difficulty in speaking, swallowing, or breathing following dental manipulation should be reported to the haematologist/dental surgeon immediately. |
| 7 | Non-steroidal anti-inflammatory drugs (NSAIDs) and aspirin must be avoided. |
| 8 | An appropriate dose of paracetamol/acetaminophen every 6 h for 2–3 days will help prevent pain following an extraction. |
| 9 | The presence of blood-borne infections should not affect the availability of dental treatment. |
| 10 | Prevention of bleeding at the time of dental procedures in patients with inhibitors to FVIII or FIX requires careful planning. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiorillo, L.; De Stefano, R.; Cervino, G.; Crimi, S.; Bianchi, A.; Campagna, P.; Herford, A.S.; Laino, L.; Cicciù, M. Oral and Psychological Alterations in Haemophiliac Patients. Biomedicines 2019, 7, 33. https://doi.org/10.3390/biomedicines7020033
Fiorillo L, De Stefano R, Cervino G, Crimi S, Bianchi A, Campagna P, Herford AS, Laino L, Cicciù M. Oral and Psychological Alterations in Haemophiliac Patients. Biomedicines. 2019; 7(2):33. https://doi.org/10.3390/biomedicines7020033
Chicago/Turabian StyleFiorillo, Luca, Rosa De Stefano, Gabriele Cervino, Salvatore Crimi, Alberto Bianchi, Paola Campagna, Alan Scott Herford, Luigi Laino, and Marco Cicciù. 2019. "Oral and Psychological Alterations in Haemophiliac Patients" Biomedicines 7, no. 2: 33. https://doi.org/10.3390/biomedicines7020033