


Fronto–Cerebellar Diaschisis and Cognitive Dysfunction after Pontine Stroke: A Case Series and Systematic Review

Abstract
:
1. Introduction
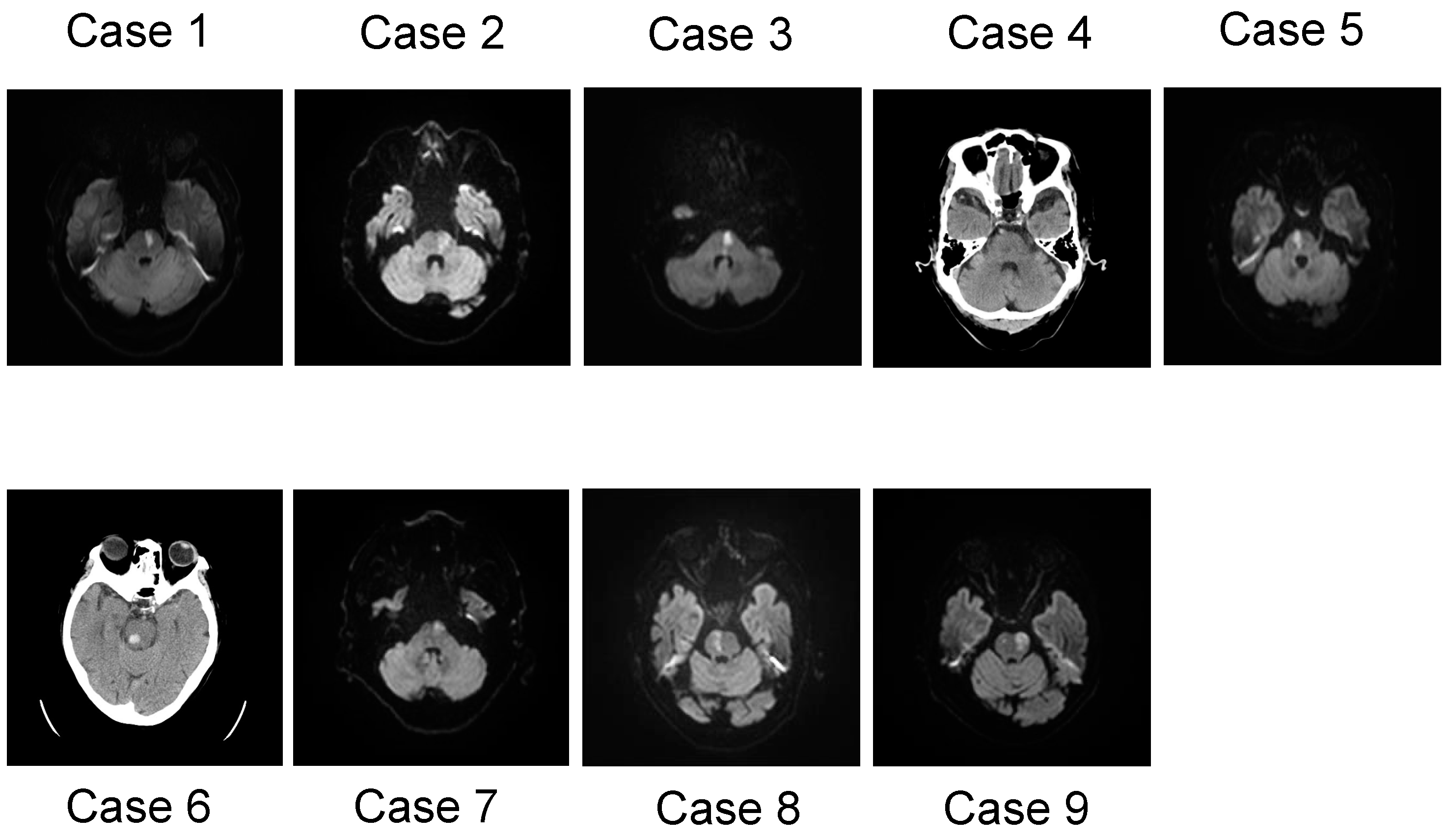
2. Case Series Description
2.1. Case 1
2.2. Case 2
2.3. Case 3
2.4. Case 4
2.5. Case 5
2.6. Case 6
2.7. Case 7
2.8. Case 8
2.9. Case 9
3. Summary of Clinical Data and Review of the Literature
3.1. Summary of Case Series
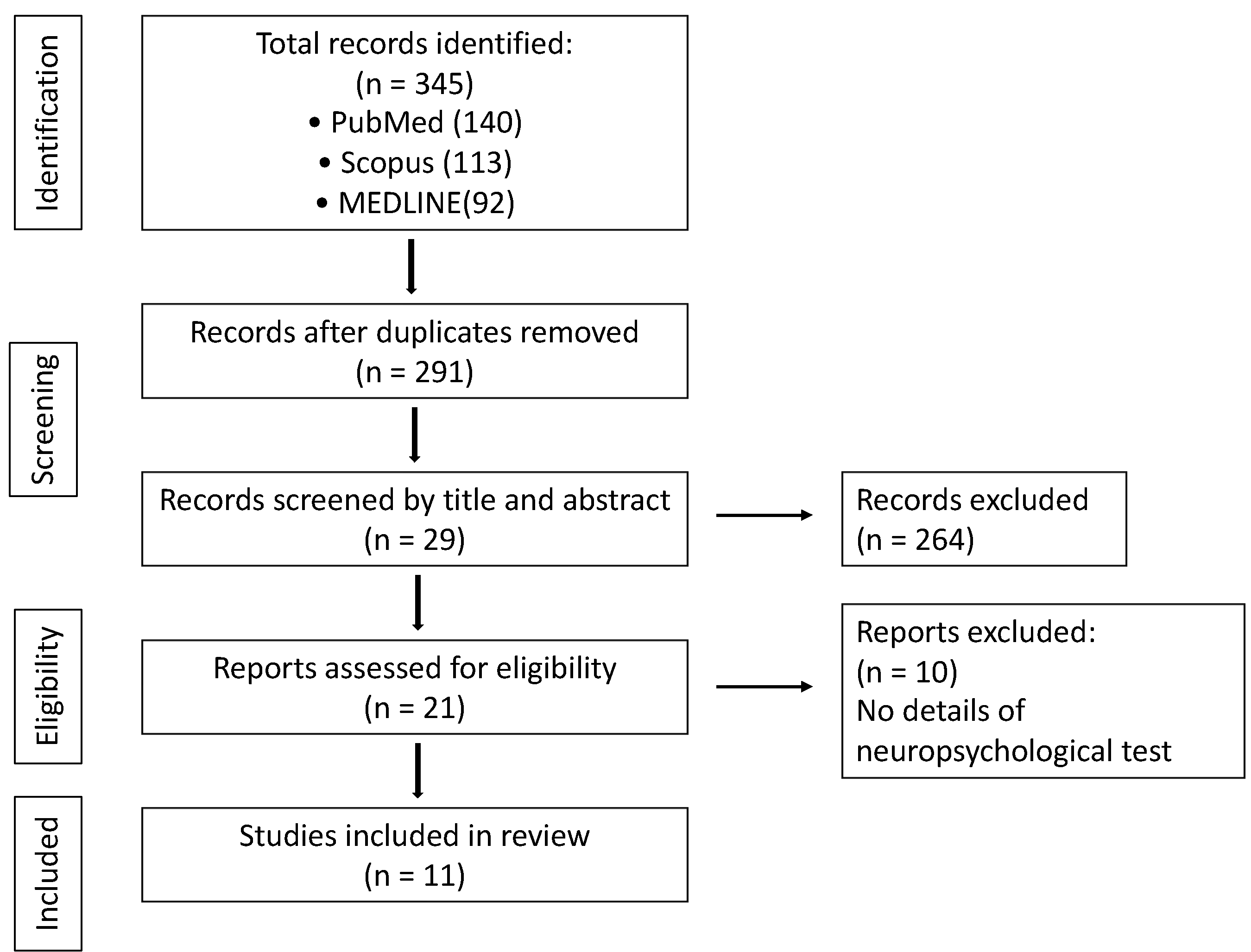
3.2. Literature Search and Study Eligibility
3.3. Methodological Quality and Risk of Bias
3.4. Synthesis
3.5. Characteristics of Cognitive Impairment after Pontine Stroke
4. Discussion
4.1. Neurobiology of Executive Function, Attention, and Memory
4.2. Short- and Long-Term Changes in Cognitive Decline Poststroke
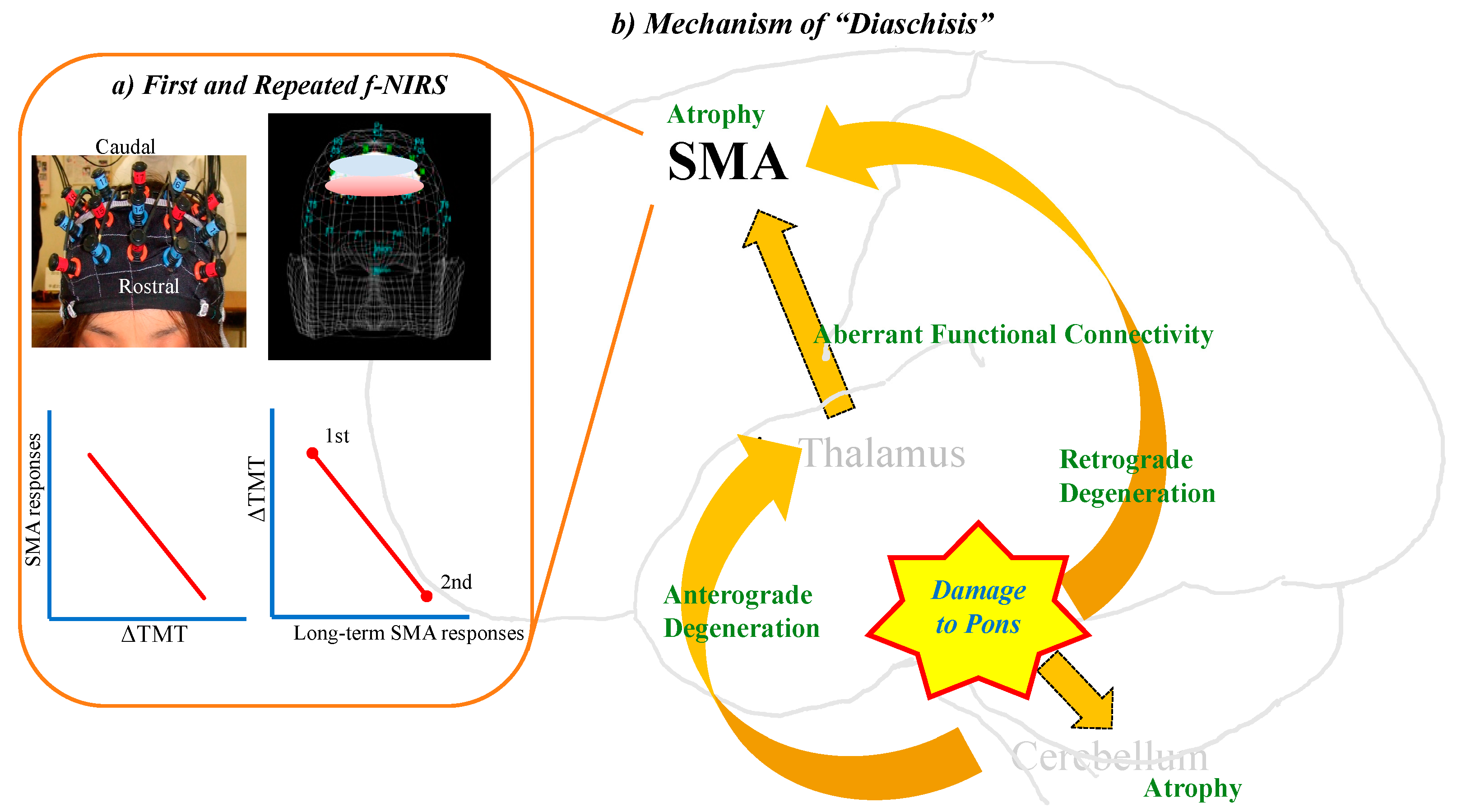
4.3. Profile of “Diaschisis”
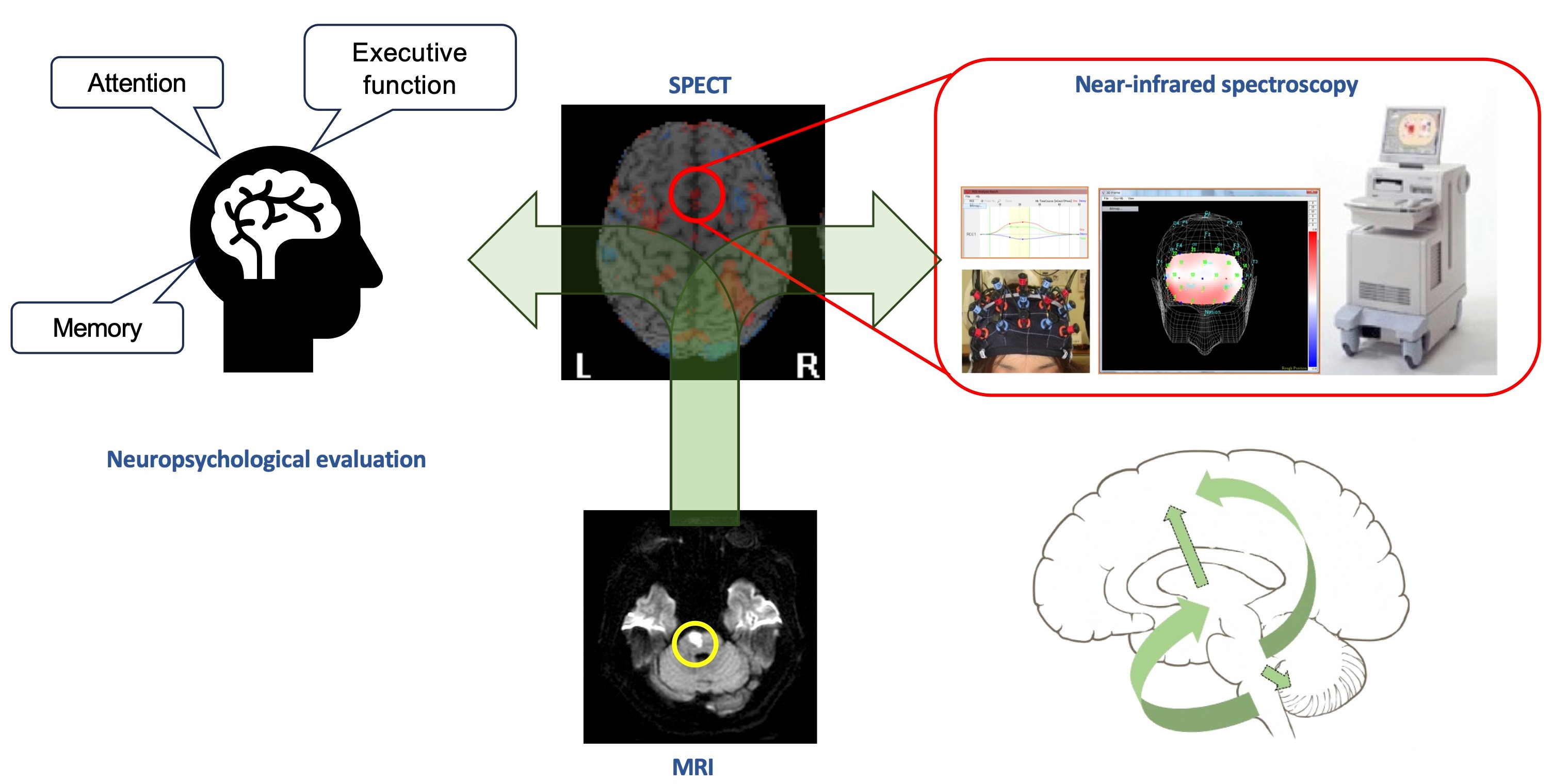
4.4. Neuroimaging of “Diaschisis”: Single Photon Emission Tomography (SPECT)
4.5. Morphological and Neurodegenerative Changes Induced by Pontine Stroke: MRI Studies
4.6. Insights from Near-Infrared Spectroscopy
4.7. Similarities and Differences of Functions among Pons, Cerebellum, and Thalamus
4.8. Limitations and Future Direction
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nys, G.M.S.; van Zandvoort, M.J.E.; de Kort, P.L.M.; van der Worp, H.B.; Jansen, B.P.W.; Algra, A.; de Haan, E.H.F.; Kappelle, L.J. The prognostic value of domain-specific cognitive abilities in acute first-ever stroke. Neurology 2005, 64, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Weimar, C.; Konig, I.R.; Kraywinkel, K.; Ziegler, A.; Diener, H.C.; German Stroke Study, C. Age and National Institutes of Health Stroke Scale Score within 6 hours after onset are accurate predictors of outcome after cerebral ischemia: Development and external validation of prognostic models. Stroke 2004, 35, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, H.S.; Reith, J.; Nakayama, H.; Kammersgaard, L.P.; Raaschou, H.O.; Olsen, T.S. What determines good recovery in patients with the most severe strokes? The Copenhagen Stroke Study. Stroke 1999, 30, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Hankey, G.J.; Jamrozik, K.; Broadhurst, R.J.; Forbes, S.; Anderson, C.S. Long-term disability after first-ever stroke and related prognostic factors in the Perth Community Stroke Study, 1989–1990. Stroke 2002, 33, 1034–1040. [Google Scholar] [CrossRef] [PubMed]
- Miyai, I.; Suzuki, T.; Kang, J.; Volpe, B.T. Improved functional outcome in patients with hemorrhagic stroke in putamen and thalamus compared with those with stroke restricted to the putamen or thalamus. Stroke 2000, 31, 1365–1369. [Google Scholar] [CrossRef] [PubMed]
- Thijs, V.N.; Lansberg, M.G.; Beaulieu, C.; Marks, M.P.; Moseley, M.E.; Albers, G.W. Is early ischemic lesion volume on diffusion-weighted imaging an independent predictor of stroke outcome? A multivariable analysis. Stroke 2000, 31, 2597–2602. [Google Scholar] [CrossRef] [PubMed]
- Malm, J.; Kristensen, B.; Karlsson, T.; Carlberg, B.; Fagerlund, M.; Olsson, T. Cognitive impairment in young adults with infratentorial infarcts. Neurology 1998, 51, 433–440. [Google Scholar] [CrossRef]
- Moliis, H.; Jokinen, H.; Parkkonen, E.; Kaste, M.; Erkinjuntti, T.; Melkas, S. Post-Stroke Cognitive Impairment is Frequent After Infra-Tentorial Infarct. J. Stroke Cerebrovasc. Dis. 2021, 30, 106108. [Google Scholar] [CrossRef]
- Ferro, J.M. Hyperacute cognitive stroke syndromes. J. Neurol. 2001, 248, 841–849. [Google Scholar] [CrossRef]
- van Zandvoort, M.J.; Kessels, R.P.; Nys, G.M.; de Haan, E.H.; Kappelle, L.J. Early neuropsychological evaluation in patients with ischaemic stroke provides valid information. Clin. Neurol. Neurosurg. 2005, 107, 385–392. [Google Scholar] [CrossRef]
- Galski, T.; Bruno, R.L.; Zorowitz, R.; Walker, J. Predicting length of stay, functional outcome, and aftercare in the rehabilitation of stroke patients. The dominant role of higher-order cognition. Stroke 1993, 24, 1794–1800. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, S.; Antonucci, G.; Gialloreti, L.E.; Traballesi, M.; Lubich, S.; Pratesi, L.; Palombi, L. Predicting stroke inpatient rehabilitation outcome: The prominent role of neuropsychological disorders. Eur. Neurol. 1996, 36, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Tatemichi, T.K.; Desmond, D.W.; Stern, Y.; Paik, M.; Sano, M.; Bagiella, E. Cognitive impairment after stroke: Frequency, patterns, and relationship to functional abilities. J. Neurol. Neurosurg. Psychiatry 1994, 57, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Nys, G.M.S.; van Zandvoort, M.J.E.; de Kort, P.L.M.; Jansen, B.P.; de Haan, E.H.F.; Kappelle, L.J. Cognitive disorders in acute stroke: Prevalence and clinical determinants. Cerebrovasc. Dis. 2007, 23, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Schmahmann, J.D.; Sherman, J.C. Cerebellar cognitive affective syndrome. Int. Rev. Neurobiol. 1997, 41, 433–440. [Google Scholar] [PubMed]
- De Smet, H.J.; Paquier, P.; Verhoeven, J.; Marien, P. The cerebellum: Its role in language and related cognitive and affective functions. Brain Lang. 2013, 127, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Baillieux, H.; De Smet, H.J.; Paquier, P.F.; De Deyn, P.P.; Marien, P. Cerebellar neurocognition: Insights into the bottom of the brain. Clin. Neurol. Neurosurg. 2008, 110, 763–773. [Google Scholar] [CrossRef] [PubMed]
- Schmahmann, J.D.; Sherman, J.C. The cerebellar cognitive affective syndrome. Brain 1998, 121 Pt 4, 561–579. [Google Scholar] [CrossRef]
- D’Aes, T.; Marien, P. Cognitive and affective disturbances following focal brainstem lesions: A review and report of three cases. Cerebellum 2015, 14, 317–340. [Google Scholar] [CrossRef]
- Fazekas, F.; Payer, F.; Valetitsch, H.; Schmidt, R.; Flooh, E. Brain stem infarction and diaschisis. A SPECT cerebral perfusion study. Stroke 1993, 24, 1162–1166. [Google Scholar] [CrossRef]
- Garrard, P.; Bradshaw, D.; Jäger, H.R.; Thompson, A.J.; Losseff, N.; Playford, D. Cognitive dysfunction after isolated brain stem insult. An underdiagnosed cause of long term morbidity. J. Neurol. Neurosurg. Psychiatry 2002, 73, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Watts, A. Cognitive dysfunction in isolated brainstem stroke: A neuropsychological and SPECT study. J. Stroke Cerebrovasc. Dis. 1998, 7, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Obayashi, S. Frontal dynamic activity as a predictor of cognitive dysfunction after pontine ischemia. NeuroRehabilitation 2019, 44, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Omar, R.; Warren, J.D.; Ron, M.A.; Lees, A.J.; Rossor, M.N.; Kartsounis, L.D. The neuro-behavioural syndrome of brainstem disease. Neurocase 2007, 13, 452–465. [Google Scholar] [CrossRef] [PubMed]
- Evyapan, D.; Kumral, E. Pontine anosognosia for hemiplegia. Neurology 1999, 53, 647–649. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Malek, A. Motor aprosodia due to isolated brainstem stroke in a young woman. Acta Neurol. Scand. 2005, 112, 197–198. [Google Scholar] [CrossRef] [PubMed]
- Hurley, R.A.; Flashman, L.A.; Chow, T.W.; Taber, K.H. The brainstem: Anatomy, assessment, and clinical syndromes. J. Neuropsychiatry Clin. Neurosci. 2010, 22, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Trimble, M.R.; Cummings, J.L. Neuropsychiatric disturbances following brainstem lesions. Br. J. Psychiatry 1981, 138, 56–59. [Google Scholar] [CrossRef]
- Arseni, C.; Goldenberg, M. Psychic disturbances in infiltrative gliomata of the brain stem. Acta Neurochir. 1959, 7, 292–300. [Google Scholar] [CrossRef]
- Minabe, Y.; Kadono, Y.; Kurachi, M. A schizophrenic syndrome associated with a midbrain tegmental lesion. Biol. Psychiatry 1990, 27, 661–663. [Google Scholar] [CrossRef]
- Greenberg, D.B.; Brown, G.L. Mania resulting from brain stem tumor. J. Nerv. Ment. Dis. 1985, 173, 434–436. [Google Scholar] [CrossRef] [PubMed]
- Netsky, M.G.; Strobos, R.R. Neoplasms within the midbrain. AMA Arch. Neurol. Psychiatry 1952, 68, 116–129. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.; Bang, O.Y.; Chung, C.S.; Lee, K.H.; Chang, W.H.; Kim, G.M. Topographic location of acute pontine infarction is associated with the development of progressive motor deficits. Stroke 2012, 43, 708–713. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, C.; Bogousslavsky, J.; Barth, A.; Regli, F. Isolated infarcts of the pons. Neurology 1996, 46, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Carrera, E.; Tononi, G. Diaschisis: Past, present, future. Brain 2014, 137, 2408–2422. [Google Scholar] [CrossRef] [PubMed]
- Salgado, J.V.; Costa-Silva, M.; Malloy-Diniz, L.F.; Siqueira, J.M.; Teixeira, A.L. Prefrontal cognitive dysfunction following brainstem lesion. Clin. Neurol. Neurosurg. 2007, 109, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Meyer, J.S.; Obara, K.; Muramatsu, K. Diaschisis. Neurol. Res. 1993, 15, 362–366. [Google Scholar] [CrossRef]
- Feeney, D.M.; Baron, J.C. Diaschisis. Stroke 1986, 17, 817–830. [Google Scholar] [CrossRef]
- Miyazawa, N.; Uchida, M.; Fukamachi, A.; Fukasawa, I.; Sasaki, H.; Nukui, H. Xenon contrast-enhanced CT imaging of supratentorial hypoperfusion in patients with brain stem infarction. AJNR Am. J. Neuroradiol. 1999, 20, 1858–1862. [Google Scholar]
- Wei, Y.; Wu, L.; Wang, Y.; Liu, J.; Miao, P.; Wang, K.; Wang, C.; Cheng, J. Disrupted Regional Cerebral Blood Flow and Functional Connectivity in Pontine Infarction: A Longitudinal MRI Study. Front. Aging Neurosci. 2020, 12, 577899. [Google Scholar] [CrossRef]
- Wang, P.; Jia, X.; Zhang, M.; Cao, Y.; Zhao, Z.; Shan, Y.; Ma, Q.; Qian, T.; Wang, J.; Lu, J.; et al. Correlation of Longitudinal Gray Matter Volume Changes and Motor Recovery in Patients After Pontine Infarction. Front. Neurol. 2018, 9, 312. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, C.; Miao, P.; Liu, J.; Wei, Y.; Wu, L.; Wang, K.; Cheng, J. An imbalance between functional segregation and integration in patients with pontine stroke: A dynamic functional network connectivity study. Neuroimage Clin. 2020, 28, 102507. [Google Scholar] [CrossRef]
- Wang, C.; Zhao, L.; Luo, Y.; Liu, J.; Miao, P.; Wei, S.; Shi, L.; Cheng, J. Structural covariance in subcortical stroke patients measured by automated MRI-based volumetry. Neuroimage Clin. 2019, 22, 101682. [Google Scholar] [CrossRef] [PubMed]
- Tien, R.D.; Ashdown, B.C. Crossed cerebellar diaschisis and crossed cerebellar atrophy: Correlation of MR findings, clinical symptoms, and supratentorial diseases in 26 patients. Am. J. Roentgraphy 1992, 158, 1155–1159. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Zeng, J.; Zhang, C.; Liu, S.; Ling, X.; Xu, A.; Ling, L.; Wang, F.; Pei, Z. Longitudinal investigations on the anterograde and retrograde degeneration in the pyramidal tract following pontine infarction with diffusion tensor imaging. Cerebrovasc. Dis. 2008, 25, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Lin, Q.; Lu, J.; Rong, D.; Zhao, Z.; Ma, Q.; Liu, H.; Shu, N.; He, Y.; Li, K. Pontine infarction: Diffusion-tensor imaging of motor pathways-a longitudinal study. Radiology 2015, 274, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Zeng, J.; Zhang, C.; Liu, S.; Ling, X.; Wang, F.; Ling, L.; Hou, Q.; Xing, S.; Pei, Z. Progression of pathological changes in the middle cerebellar peduncle by diffusion tensor imaging correlates with lesser motor gains after pontine infarction. Neurorehabil. Neural. Repair 2009, 23, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, C.; Wei, Y.; Miao, P.; Liu, J.; Wu, L.; Li, Z.; Li, X.; Wang, K.; Cheng, J. Abnormal functional connectivities patterns of multidomain cognitive impairments in pontine stroke patients. Hum. Brain Mapp. 2022, 43, 4676–4688. [Google Scholar] [CrossRef]
- Wu, L.; Wang, C.; Liu, J.; Guo, J.; Wei, Y.; Wang, K.; Miao, P.; Wang, Y.; Cheng, J. Voxel-Mirrored Homotopic Connectivity Associated With Change of Cognitive Function in Chronic Pontine Stroke. Front. Aging Neurosci. 2021, 13, 621767. [Google Scholar] [CrossRef]
- Jiang, L.; Geng, W.; Chen, H.; Zhang, H.; Bo, F.; Mao, C.N.; Chen, Y.C.; Yin, X. Decreased functional connectivity within the default-mode network in acute brainstem ischemic stroke. Eur. J. Radiol. 2018, 105, 221–226. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Reitan, R.M. The relation of the trail making test to organic brain damage. J. Consult. Psychol. 1955, 19, 393–394. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Cubillo, I.; Perianez, J.A.; Adrover-Roig, D.; Rodriguez-Sanchez, J.M.; Rios-Lago, M.; Tirapu, J.; Barcelo, F. Construct validity of the Trail Making Test: Role of task-switching, working memory, inhibition/interference control, and visuomotor abilities. J. Int. Neuropsychol. Soc. JINS 2009, 15, 438–450. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. The FAB: A Frontal Assessment Battery at bedside. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef] [PubMed]
- Adachi, K.; Ijuin, M.; Otsuki, M.; Koike, A.; Ishiai, S. Examining validity of the standardized verbal paired associates learning test. High Brain Func. Res. 2018, 38, 414–421. [Google Scholar] [CrossRef]
- Shin, M.S.; Park, S.Y.; Park, S.R.; Seol, S.H.; Kwon, J.S. Clinical and empirical applications of the Rey-Osterrieth Complex Figure Test. Nat. Protoc. 2006, 1, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Brunnstrom, S. Motor testing procedures in hemiplegia: Based on sequential recovery stages. Phys. Ther. 1966, 46, 357–375. [Google Scholar] [CrossRef]
- Seo, H.J.; Kim, S.Y.; Lee, Y.J.; Park, J.E. RoBANS 2: A Revised Risk of Bias Assessment Tool for Nonrandomized Studies of Interventions. Korean J. Fam. Med. 2023, 44, 249–260. [Google Scholar] [CrossRef]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef]
- van Zandvoort, M.; de Haan, E.; van Gijn, J.; Kappelle, L.J. Cognitive functioning in patients with a small infarct in the brainstem. J. Int. Neuropsychol. Soc. JINS 2003, 9, 490–494. [Google Scholar] [CrossRef]
- Fu, X.; Lu, Z.; Wang, Y.; Huang, L.; Wang, X.; Zhang, H.; Xiao, Z. A Clinical Research Study of Cognitive Dysfunction and Affective Impairment after Isolated Brainstem Stroke. Front. Aging Neurosci. 2017, 9, 400. [Google Scholar] [CrossRef] [PubMed]
- Maeshima, S.; Osawa, A.; Kunishio, K. Cognitive dysfunction in a patient with brainstem hemorrhage. Neurol. Sci. 2010, 31, 495–499. [Google Scholar] [CrossRef]
- Nishio, Y.; Ishii, K.; Kazui, H.; Hosokai, Y.; Mori, E. Frontal-lobe syndrome and psychosis after damage to the brainstem dopaminergic nuclei. J. Neurol. Sci. 2007, 260, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Neki, H.; Yamane, F.; Osawa, A.; Maeshima, S.; Ishihara, S. Cognitive Dysfunction in Patients with Pontine Hemorrhage. No Shinkei Geka 2014, 42, 109–113. [Google Scholar] [PubMed]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A Product from the ESRC Methods Programme Version 1; University of Lancaster: Lancaster, UK, 2006. [Google Scholar]
- Schmahmann, J.D.; Pandya, D.N. Anatomic organization of the basilar pontine projections from prefrontal cortices in rhesus monkey. J. Neurosci. 1997, 17, 438–458. [Google Scholar] [CrossRef] [PubMed]
- Vataja, R.; Pohjasvaara, T.; Mantyla, R.; Ylikoski, R.; Leppavuori, A.; Leskela, M.; Kalska, H.; Hietanen, M.; Aronen, H.J.; Salonen, O.; et al. MRI correlates of executive dysfunction in patients with ischaemic stroke. Eur. J. Neurol. 2003, 10, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Fassbender, C.; Murphy, K.; Foxe, J.J.; Wylie, G.R.; Javitt, D.C.; Robertson, I.H.; Garavan, H. A topography of executive functions and their interactions revealed by functional magnetic resonance imaging. Brain Res. Cogn. Brain Res. 2004, 20, 132–143. [Google Scholar] [CrossRef]
- Baker, S.C.; Rogers, R.D.; Owen, A.M.; Frith, C.D.; Dolan, R.J.; Frackowiak, R.S.; Robbins, T.W. Neural systems engaged by planning: A PET study of the Tower of London task. Neuropsychologia 1996, 34, 515–526. [Google Scholar] [CrossRef]
- Aron, A.R.; Durston, S.; Eagle, D.M.; Logan, G.D.; Stinear, C.M.; Stuphorn, V. Converging evidence for a fronto-basal-ganglia network for inhibitory control of action and cognition. J. Neurosci. 2007, 27, 11860–11864. [Google Scholar] [CrossRef]
- Uddin, L.Q. Cognitive and behavioural flexibility: Neural mechanisms and clinical considerations. Nat. Rev. Neurosci. 2021, 22, 167–179. [Google Scholar] [CrossRef]
- Joy, M.T.; Ben Assayag, E.; Shabashov-Stone, D.; Liraz-Zaltsman, S.; Mazzitelli, J.; Arenas, M.; Abduljawad, N.; Kliper, E.; Korczyn, A.D.; Thareja, N.S.; et al. CCR5 Is a Therapeutic Target for Recovery after Stroke and Traumatic Brain Injury. Cell 2019, 176, 1143–1157. [Google Scholar] [CrossRef] [PubMed]
- Desimone, R.; Duncan, J. Neural mechanisms of selective visual attention. Annu. Rev. Neurosci. 1995, 18, 193–222. [Google Scholar] [CrossRef] [PubMed]
- Treisman, A.M.; Gelade, G. A feature-integration theory of attention. Cogn. Psychol. 1980, 12, 97–136. [Google Scholar] [CrossRef] [PubMed]
- Chun, M.M.; Potter, M.C. A two-stage model for multiple target detection in rapid serial visual presentation. J. Exp. Psychol. Hum. Percept Perform. 1995, 21, 109–127. [Google Scholar] [CrossRef] [PubMed]
- Walther, D.; Koch, C. Modeling attention to salient proto-objects. Neural Netw. 2006, 19, 1395–1407. [Google Scholar] [CrossRef] [PubMed]
- Posner, M.I.; Petersen, S.E. The attention systems of the human brain. Annu. Rev. Neurosci. 1990, 13, 25–42. [Google Scholar] [CrossRef] [PubMed]
- Posner, M.I. Orienting of attention. Q. J. Exp. Psychol. 1980, 32, 3–25. [Google Scholar] [CrossRef]
- Petersen, S.E.; Posner, M.I. The attention system of the human brain: 20 years after. Annu. Rev. Neurosci. 2012, 35, 73–89. [Google Scholar] [CrossRef]
- Fan, J.; McCandliss, B.D.; Sommer, T.; Raz, A.; Posner, M.I. Testing the efficiency and independence of attentional networks. J. Cogn. Neurosci. 2002, 14, 340–347. [Google Scholar] [CrossRef]
- Moscovitch, M.; Cabeza, R.; Winocur, G.; Nadel, L. Episodic Memory and Beyond: The Hippocampus and Neocortex in Transformation. Annu. Rev. Psychol. 2016, 67, 105–134. [Google Scholar] [CrossRef]
- Tonegawa, S.; Pignatelli, M.; Roy, D.S.; Ryan, T.J. Memory engram storage and retrieval. Curr. Opin. Neurobiol. 2015, 35, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Kandel, E.R. The molecular biology of memory storage—A dialogue between genes and synapses. Science 2001, 294, 1030–1038. [Google Scholar] [CrossRef]
- Squire, L.R.; Wixted, J.T. The cognitive neuroscience of human memory since H.M. Annu. Rev. Neurosci. 2011, 34, 259–288. [Google Scholar] [CrossRef] [PubMed]
- Asok, A.; Leroy, F.; Rayman, J.B.; Kandel, E.R. Molecular Mechanisms of the Memory Trace. Trends Neurosci. 2019, 42, 14–22. [Google Scholar] [CrossRef] [PubMed]
- McGaugh, J.L. Memory—A Century of Consolidation. Science 2000, 287, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Tulving, E. Episodic memory: From mind to brain. Annu. Rev. Psychol. 2002, 53, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, K.; Osada, T.; Adachi, Y.; Matsui, T.; Kimura, H.M.; Miyashita, Y. Functional differentiation of memory retrieval network in macaque posterior parietal cortex. Neuron 2013, 77, 787–799. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, Y. Perirhinal circuits for memory processing. Nat. Rev. Neurosci. 2019, 20, 577–592. [Google Scholar] [CrossRef]
- Sakai, K.; Hikosaka, O.; Miyauchi, S.; Takino, R.; Sasaki, Y.; Putz, B. Transition of brain activation from frontal to parietal areas in visuomotor sequence learning. J. Neurosci. 1998, 18, 1827–1840. [Google Scholar] [CrossRef]
- Obayashi, S.; Suhara, T.; Kawabe, K.; Okauchi, T.; Maeda, J.; Akine, Y.; Onoe, H.; Iriki, A. Functional brain mapping of monkey tool use. Neuroimage 2001, 14, 853–861. [Google Scholar] [CrossRef]
- Obayashi, S.; Suhara, T.; Kawabe, K.; Okauchi, T.; Maeda, J.; Nagai, Y.; Iriki, A. Fronto-parieto-cerebellar interaction associated with intermanual transfer of monkey tool-use learning. Neurosci. Lett. 2003, 339, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Obayashi, S. Possible mechanism for transfer of motor skill learning: Implication of the cerebellum. Cerebellum 2004, 3, 204–211. [Google Scholar] [CrossRef]
- Rajan, K.B.; Aggarwal, N.T.; Wilson, R.S.; Everson-Rose, S.A.; Evans, D.A. Association of cognitive functioning, incident stroke, and mortality in older adults. Stroke 2014, 45, 2563–2567. [Google Scholar] [CrossRef] [PubMed]
- Tham, W.; Auchus, A.P.; Thong, M.; Goh, M.L.; Chang, H.M.; Wong, M.C.; Chen, C.P. Progression of cognitive impairment after stroke: One year results from a longitudinal study of Singaporean stroke patients. J. Neurol. Sci. 2002, 203–204, 49–52. [Google Scholar] [CrossRef]
- Wentzel, C.; Rockwood, K.; MacKnight, C.; Hachinski, V.; Hogan, D.B.; Feldman, H.; Ostbye, T.; Wolfson, C.; Gauthier, S.; Verreault, R.; et al. Progression of impairment in patients with vascular cognitive impairment without dementia. Neurology 2001, 57, 714–716. [Google Scholar] [CrossRef] [PubMed]
- Levine, D.A.; Galecki, A.T.; Langa, K.M.; Unverzagt, F.W.; Kabeto, M.U.; Giordani, B.; Wadley, V.G. Trajectory of Cognitive Decline After Incident Stroke. JAMA 2015, 314, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Schaapsmeerders, P.; Maaijwee, N.A.; van Dijk, E.J.; Rutten-Jacobs, L.C.; Arntz, R.M.; Schoonderwaldt, H.C.; Dorresteijn, L.D.; Kessels, R.P.; de Leeuw, F.E. Long-term cognitive impairment after first-ever ischemic stroke in young adults. Stroke 2013, 44, 1621–1628. [Google Scholar] [CrossRef]
- Delavaran, H.; Jonsson, A.C.; Lovkvist, H.; Iwarsson, S.; Elmstahl, S.; Norrving, B.; Lindgren, A. Cognitive function in stroke survivors: A 10-year follow-up study. Acta Neurol. Scand. 2017, 136, 187–194. [Google Scholar] [CrossRef]
- Buvarp, D.; Rafsten, L.; Abzhandadze, T.; Sunnerhagen, K.S. A prospective cohort study on longitudinal trajectories of cognitive function after stroke. Sci. Rep. 2021, 11, 17271. [Google Scholar] [CrossRef]
- Aam, S.; Einstad, M.S.; Munthe-Kaas, R.; Lydersen, S.; Ihle-Hansen, H.; Knapskog, A.B.; Ellekjaer, H.; Seljeseth, Y.; Saltvedt, I. Post-stroke Cognitive Impairment-Impact of Follow-Up Time and Stroke Subtype on Severity and Cognitive Profile: The Nor-COAST Study. Front. Neurol. 2020, 11, 699. [Google Scholar] [CrossRef]
- Elgh, E.; Hu, X. Dynamic Trajectory of Long-Term Cognitive Improvement Up to 10 Years in Young Community-Dwelling Stroke Survivors: A Cohort Study. Front. Neurol. 2019, 10, 97. [Google Scholar] [CrossRef] [PubMed]
- Tang, E.Y.; Amiesimaka, O.; Harrison, S.L.; Green, E.; Price, C.; Robinson, L.; Siervo, M.; Stephan, B.C. Longitudinal Effect of Stroke on Cognition: A Systematic Review. J. Am. Heart Assoc. 2018, 7, e006443. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.I.; Alexander, M.P.; Mandell, A.M. Dementia following strokes in the mesencephalon and diencephalon. Arch. Neurol. 1987, 44, 1127–1133. [Google Scholar] [CrossRef] [PubMed]
- Meador, K.J.; Loring, D.W.; Sethi, K.D.; Yaghmai, F.; Styren, S.D.; DeKosky, S.T. Dementia associated with dorsal midbrain lesion. J. Int. Neuropsychol. Soc. JINS 1996, 2, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Rasquin, S.M.; Lodder, J.; Visser, P.J.; Lousberg, R.; Verhey, F.R. Predictive accuracy of MCI subtypes for Alzheimer’s disease and vascular dementia in subjects with mild cognitive impairment: A 2-year follow-up study. Dement. Geriatr. Cogn. Disord. 2005, 19, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Savva, G.M.; Stephan, B.C.; Alzheimer’s Society Vascular Dementia Systematic Review Group. Epidemiological studies of the effect of stroke on incident dementia: A systematic review. Stroke 2010, 41, e41–e46. [Google Scholar] [CrossRef] [PubMed]
- Pohjasvaara, T.; Mantyla, R.; Ylikoski, R.; Kaste, M.; Erkinjuntti, T. Clinical features of MRI-defined subcortical vascular disease. Alzheimer Dis. Assoc. Disord. 2003, 17, 236–242. [Google Scholar] [CrossRef]
- Roman, G.C.; Royall, D.R. Executive control function: A rational basis for the diagnosis of vascular dementia. Alzheimer Dis. Assoc. Disord. 1999, 13 (Suppl. S3), S69–S80. [Google Scholar] [CrossRef]
- Ballard, C.; Rowan, E.; Stephens, S.; Kalaria, R.; Kenny, R.A. Prospective follow-up study between 3 and 15 months after stroke: Improvements and decline in cognitive function among dementia-free stroke survivors >75 years of age. Stroke 2003, 34, 2440–2444. [Google Scholar] [CrossRef]
- Desmond, D.W.; Moroney, J.T.; Sano, M.; Stern, Y. Recovery of cognitive function after stroke. Stroke 1996, 27, 1798–1803. [Google Scholar] [CrossRef]
- Oh, H.; Park, J.; Seo, W. A 2-year prospective follow-up study of temporal changes associated with post-stroke cognitive impairment. Int. J. Nurs. Pract. 2018, 24, e12618. [Google Scholar] [CrossRef] [PubMed]
- Kempinsky, W.H. Experimental study of distant effects of acute focal brain injury; a study of diaschisis. AMA Arch. Neurol. Psychiatry 1958, 79, 376–389. [Google Scholar] [CrossRef] [PubMed]
- Pantano, P.; Baron, J.C.; Samson, Y.; Bousser, M.G.; Derouesne, C.; Comar, D. Crossed cerebellar diaschisis. Further studies. Brain 1986, 109 Pt 4, 677–694. [Google Scholar] [CrossRef] [PubMed]
- Tsuda, Y.; Ayada, Y.; Izumi, Y.; Ichihara, S.; Hosomi, N.; Ohkawa, M.; Matsuo, H. Cerebellar diaschisis in pontine infarctions: A report of five cases. Eur. J. Nucl. Med. 1995, 22, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Rousseaux, M.; Steinling, M.; Mazingue, A.; Benaim, C.; Froger, J. Cerebral blood flow in lateral medullary infarcts. Stroke 1995, 26, 1404–1408. [Google Scholar] [CrossRef] [PubMed]
- Botez, M.I.; Léveillé, J.; Lambert, R.; Botez, T. Single photon emission computed tomography (SPECT) in cerebellar disease: Cerebello-cerebral diaschisis. Eur. Neurol. 1991, 31, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Greenhill, S.; Huang, S.; Silva, T.K.; Sano, Y.; Wu, S.; Cai, Y.; Nagaoka, Y.; Sehgal, M.; Cai, D.J.; et al. CCR5 is a suppressor for cortical plasticity and hippocampal learning and memory. eLife 2016, 5, e20985. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Wang, C.; Liu, J.; Miao, P.; Wu, L.; Wang, Y.; Wang, K.; Cheng, J. Progressive Gray Matter Atrophy and Abnormal Structural Covariance Network in Ischemic Pontine Stroke. Neuroscience 2020, 448, 255–265. [Google Scholar] [CrossRef]
- Dang, C.; Liu, G.; Xing, S.; Xie, C.; Peng, K.; Li, C.; Li, J.; Zhang, J.; Chen, L.; Pei, Z.; et al. Longitudinal cortical volume changes correlate with motor recovery in patients after acute local subcortical infarction. Stroke 2013, 44, 2795–2801. [Google Scholar] [CrossRef]
- Thomalla, G.; Glauche, V.; Weiller, C.; Rother, J. Time course of wallerian degeneration after ischaemic stroke revealed by diffusion tensor imaging. J. Neurol. Neurosurg. Psychiatry 2005, 76, 266–268. [Google Scholar] [CrossRef]
- Lu, J.; Liu, H.; Zhang, M.; Wang, D.; Cao, Y.; Ma, Q.; Rong, D.; Wang, X.; Buckner, R.L.; Li, K. Focal pontine lesions provide evidence that intrinsic functional connectivity reflects polysynaptic anatomical pathways. J. Neurosci. 2011, 31, 15065–15071. [Google Scholar] [CrossRef] [PubMed]
- Fox, M.D.; Raichle, M.E. Spontaneous fluctuations in brain activity observed with functional magnetic resonance imaging. Nat. Rev. Neurosci. 2007, 8, 700–711. [Google Scholar] [CrossRef] [PubMed]
- Fontaine, D.; Capelle, L.; Duffau, H. Somatotopy of the supplementary motor area: Evidence from correlation of the extent of surgical resection with the clinical patterns of deficit. Neurosurgery 2002, 50, 297–303; discussion 303–305. [Google Scholar] [PubMed]
- Tremblay, P.; Gracco, V.L. Contribution of the pre-SMA to the production of words and non-speech oral motor gestures, as revealed by repetitive transcranial magnetic stimulation (rTMS). Brain Res. 2009, 1268, 112–124. [Google Scholar] [CrossRef] [PubMed]
- Fried, I.; Katz, A.; McCarthy, G.; Sass, K.J.; Williamson, P.; Spencer, S.S.; Spencer, D.D. Functional organization of human supplementary motor cortex studied by electrical stimulation. J. Neurosci. 1991, 11, 3656–3666. [Google Scholar] [CrossRef] [PubMed]
- Obayashi, S.; Hara, Y. Hypofrontal activity during word retrieval in older adults: A near-infrared spectroscopy study. Neuropsychologia 2013, 51, 418–424. [Google Scholar] [CrossRef]
- Kwon, Y.H.; Kwon, J.W. Response Inhibition Induced in the Stop-signal Task by Transcranial Direct Current Stimulation of the Pre-supplementary Motor Area and Primary Sensoriomotor Cortex. J. Phys. Ther. Sci. 2013, 25, 1083–1086. [Google Scholar] [CrossRef]
- Alario, F.X.; Chainay, H.; Lehericy, S.; Cohen, L. The role of the supplementary motor area (SMA) in word production. Brain Res. 2006, 1076, 129–143. [Google Scholar] [CrossRef]
- Shima, K.; Mushiake, H.; Saito, N.; Tanji, J. Role for cells in the presupplementary motor area in updating motor plans. Proc. Natl. Acad. Sci. USA 1996, 93, 8694–8698. [Google Scholar] [CrossRef]
- Tanji, J.; Shima, K. Supplementary motor cortex in organization of movement. Eur. Neurol. 1996, 36 (Suppl. 1), 13–19. [Google Scholar] [CrossRef]
- Shima, K.; Tanji, J. Neuronal activity in the supplementary and presupplementary motor areas for temporal organization of multiple movements. J. Neurophysiol. 2000, 84, 2148–2160. [Google Scholar] [CrossRef] [PubMed]
- Shima, K.; Tanji, J. Both supplementary and presupplementary motor areas are crucial for the temporal organization of multiple movements. J. Neurophysiol. 1998, 80, 3247–3260. [Google Scholar] [CrossRef] [PubMed]
- Penfield, W. The supplementary motor area in the cerebral cortex of man. Arch. Psychiatr. Nervenkr. Z. Gesamte Neurol. Psychiatr. 1950, 185, 670–674. [Google Scholar] [CrossRef] [PubMed]
- Penfield, W.; Welch, K. The supplementary motor area of the cerebral cortex; a clinical and experimental study. AMA Arch. Neurol. Psychiatry 1951, 66, 289–317. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaka, Y.; Aizawa, H.; Tanji, J. A motor area rostral to the supplementary motor area (presupplementary motor area) in the monkey: Neuronal activity during a learned motor task. J. Neurophysiol. 1992, 68, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Tanji, J. New concepts of the supplementary motor area. Curr. Opin. Neurobiol. 1996, 6, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Tanji, J.; Shima, K. Role for supplementary motor area cells in planning several movements ahead. Nature 1994, 371, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Jurgens, U. The efferent and afferent connections of the supplementary motor area. Brain Res. 1984, 300, 63–81. [Google Scholar] [CrossRef]
- Akkal, D.; Dum, R.P.; Strick, P.L. Supplementary motor area and presupplementary motor area: Targets of basal ganglia and cerebellar output. J. Neurosci. 2007, 27, 10659–10673. [Google Scholar] [CrossRef]
- Schmahmann, J.D.; Weilburg, J.B.; Sherman, J.C. The neuropsychiatry of the cerebellum—Insights from the clinic. Cerebellum 2007, 6, 254–267. [Google Scholar] [CrossRef]
- Schmahmann, J.D.; Guell, X.; Stoodley, C.J.; Halko, M.A. The Theory and Neuroscience of Cerebellar Cognition. Annu. Rev. Neurosci. 2019, 42, 337–364. [Google Scholar] [CrossRef] [PubMed]
- Wolff, M.; Vann, S.D. The Cognitive Thalamus as a Gateway to Mental Representations. J. Neurosci. 2019, 39, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Valenstein, E.; Bowers, D.; Verfaellie, M.; Heilman, K.M.; Day, A.; Watson, R.T. Retrosplenial amnesia. Brain 1987, 110 Pt 6, 1631–1646. [Google Scholar] [CrossRef] [PubMed]
- Aggleton, J.P.; O’Mara, S.M.; Vann, S.D.; Wright, N.F.; Tsanov, M.; Erichsen, J.T. Hippocampal-anterior thalamic pathways for memory: Uncovering a network of direct and indirect actions. Eur. J. Neurosci. 2010, 31, 2292–2307. [Google Scholar] [CrossRef]
- Van der Werf, Y.D.; Scheltens, P.; Lindeboom, J.; Witter, M.P.; Uylings, H.B.; Jolles, J. Deficits of memory, executive functioning and attention following infarction in the thalamus; a study of 22 cases with localised lesions. Neuropsychologia 2003, 41, 1330–1344. [Google Scholar] [CrossRef] [PubMed]
- Carrera, E.; Bogousslavsky, J. The thalamus and behavior: Effects of anatomically distinct strokes. Neurology 2006, 66, 1817–1823. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.D.; Ojemann, G.A. The role of the human thalamus in language and memory: Evidence from electrophysiological studies. Brain Cogn. 2000, 42, 218–230. [Google Scholar] [CrossRef]
- Crosson, B. Thalamic mechanisms in language: A reconsideration based on recent findings and concepts. Brain Lang. 2013, 126, 73–88. [Google Scholar] [CrossRef]
- De Witte, L.; Brouns, R.; Kavadias, D.; Engelborghs, S.; De Deyn, P.P.; Marien, P. Cognitive, affective and behavioural disturbances following vascular thalamic lesions: A review. Cortex 2011, 47, 273–319. [Google Scholar] [CrossRef]
- Obayashi, S. The Supplementary Motor Area Responsible for Word Retrieval Decline After Acute Thalamic Stroke Revealed by Coupled SPECT and Near-Infrared Spectroscopy. Brain Sci. 2020, 10, 247. [Google Scholar] [CrossRef]
- Obayashi, S. Cognitive and linguistic dysfunction after thalamic stroke and recovery process: Possible mechanism. AIMS Neurosci. 2022, 9, 1–11. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age | Gender | Type of Stroke | Laterality | Volume (mm3) | BRS on Admission | BRS at Discharge |
|---|---|---|---|---|---|---|---|
| Case 1 | 63 | M | BAD | Left | 273.5 | 6,5,6 | 6,6,6 |
| Case 2 | 72 | M | BAD | Left | 1328.5 | 6,6,6 | 6,6,6 |
| Case 3 | 75 | F | BAD | Left | 259 | 3,3,4 | 3,3,4 |
| Case 4 | 76 | M | Lacunar infarct | Median | 325 | No paresis | |
| Case 5 | 77 | M | BAD | Right | 873 | 4,4,5 | 6,6,6 |
| Case 6 | 77 | F | Hemorrhage | Right | 870.5 | 6,6,6 | 6,6,6 |
| Case 7 | 79 | M | BAD | Left | 372.5 | No paresis | |
| Case 8 | 82 | M | BAD | Right | 1147.5 | 5,5,5 | 5,5,5 |
| Case 9 | 86 | F | BAD | Left | 1126 | 2,2,4 | 3,4,3 |
| Executive Dysfunction (FAB; TMT-B; ROCFT Copy) | Visual Memory Disturbance (ROCFT Recall) | Verbal Memory Disturbance (S-PA) | Inattention (TMT-A) | |
|---|---|---|---|---|
| Case 1 | + (16/18; 106 s; 26/36) | + (16/36) | + | − (43 s) |
| Case 2 | + 16/18; 156 s; 31/36 | NA | NA | + (110 s) |
| Case 3 | + (16/18; 116 s; 36/36) | + (16/36) | +/− | − (42 s) |
| Case 4 | + (15/18; 292 s; 31/36) | + (11/36) | +/− | + (118 s) |
| Case 5 | + (14/18; 209 s; 20/36) | NA | − | − (60 s) |
| Case 6 | + (15/18; 79 s; 32/36) | + (11/36) | NA | − (60 s) |
| Case 7 | + (14/18; 98 s; 34/36) | + (16/36) | NA | + (84 s) |
| Case 8 | + (10/18; NA; NA) | NA | NA | + (243 s) |
| Case 9 | + (15/18; NA; NA) | NA | NA | NA |
| Author | Year | Comparability of the Target Group | Target GroupSelection | Confounders | Measurement of Intervention/Exposure | Blinding of Assessors | Outcome Assessment | Incomplete Outcome Data | Selective Outcome Reporting |
|---|---|---|---|---|---|---|---|---|---|
| Van Zandvoort [60] | 2003 | Low | Low | Low | High | Low | Low | Low | Low |
| Fu [61] | 2017 | Low | Low | Low | High | Low | Low | Low | Low |
| Wang [48] | 2022 | Low | Low | Low | High | Low | Low | Low | Low |
| Author | Year | Documentation | Uniqueness | Educational Value | Objectivity | Interpretation |
|---|---|---|---|---|---|---|
| Our case series | Present | 2 | 1 | 2 | 2 | 2 |
| Hoffman and Watts [58] | 1998 | 2 | 2 | 2 | 2 | 2 |
| Hoffman and Malek [26] | 2005 | 2 | 2 | 2 | 2 | 2 |
| Garrard et al. [21] | 2002 | 2 | 1 | 2 | 2 | 2 |
| Nishio et al. [62] | 2007 | 2 | 1 | 2 | 2 | 2 |
| Maeshima et al. [63] | 2010 | 2 | 1 | 2 | 2 | 2 |
| D’aes and Marien [19] | 2014 | 2 | 1 | 2 | 2 | 2 |
| Neki et al. [64] | 2014 | 2 | 1 | 2 | 2 | 2 |
| Obayashi [23] | 2019 | 2 | 1 | 2 | 2 | 2 |
| Authors (Year) [Reference Number] | Classification | Executive Dysfunction | Inattention | Memory Disturbance | Linguistic Difficulty | Visuospatial Disability | General Intelligence |
|---|---|---|---|---|---|---|---|
| Hoffman and Watts (1998) [58] | 5 cases | ++ | NA | ± | NA | + | NA |
| Garrard et al. (2002) [21] | 7 cases | ++ | + | + | − | − | ± |
| Hoffman and Malek (2005) [26] | 1 case | ± | NA | − | + | + | NA |
| Nishio et al. (2007) [62] | 1 case | ++ | + | ± | − | − | ± |
| Maeshima et al. (2010) [63] | 1 case | + | + | + | − | − | |
| D’aes and Marien (2014) [19] | 3 cases | ++ | ++ | + | + | + | ++ |
| Neki et al. (2014) [64] | 10 cases | + | NA | NA | NA | NA | + |
| Obayashi (2019) [23] | 25 cases | + | ++ | + | − | NA | ± |
| Van Zandvoort et al. (2003) [60] | Group comparison, 17 PS patients | + | + | NA | + | + | NA |
| Wang et al. (2022) [48] | Group comparison, 47 PS patients | ++ | − | + | NA | NA | NA |
| Fu et al. (2017) [61] | Group comparison, 34 PS patients | ± | + | − | + | + | NA |
| Executive Dysfunction | Inattention | Memory Disturbance | Linguistic Difficulties | Spatial Cognition Difficulties | Personality Changes | |
|---|---|---|---|---|---|---|
| Pons | ||||||
| Cerebellum | ||||||
| Thalamus |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimmyo, K.; Obayashi, S. Fronto–Cerebellar Diaschisis and Cognitive Dysfunction after Pontine Stroke: A Case Series and Systematic Review. Biomedicines 2024, 12, 623. https://doi.org/10.3390/biomedicines12030623
Shimmyo K, Obayashi S. Fronto–Cerebellar Diaschisis and Cognitive Dysfunction after Pontine Stroke: A Case Series and Systematic Review. Biomedicines. 2024; 12(3):623. https://doi.org/10.3390/biomedicines12030623
Chicago/Turabian StyleShimmyo, Kei, and Shigeru Obayashi. 2024. "Fronto–Cerebellar Diaschisis and Cognitive Dysfunction after Pontine Stroke: A Case Series and Systematic Review" Biomedicines 12, no. 3: 623. https://doi.org/10.3390/biomedicines12030623