
The Predictive Value of 8-Hydroxy-Deoxyguanosine (8-OHdG) Serum Concentrations in Irradiated Non-Small Cell Lung Carcinoma (NSCLC) Patients
 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Treatment Schedule
2.3. Patient Assessment
2.4. Sample Collection and Preparation
2.5. Statistical Analysis
3. Results
3.1. Patients
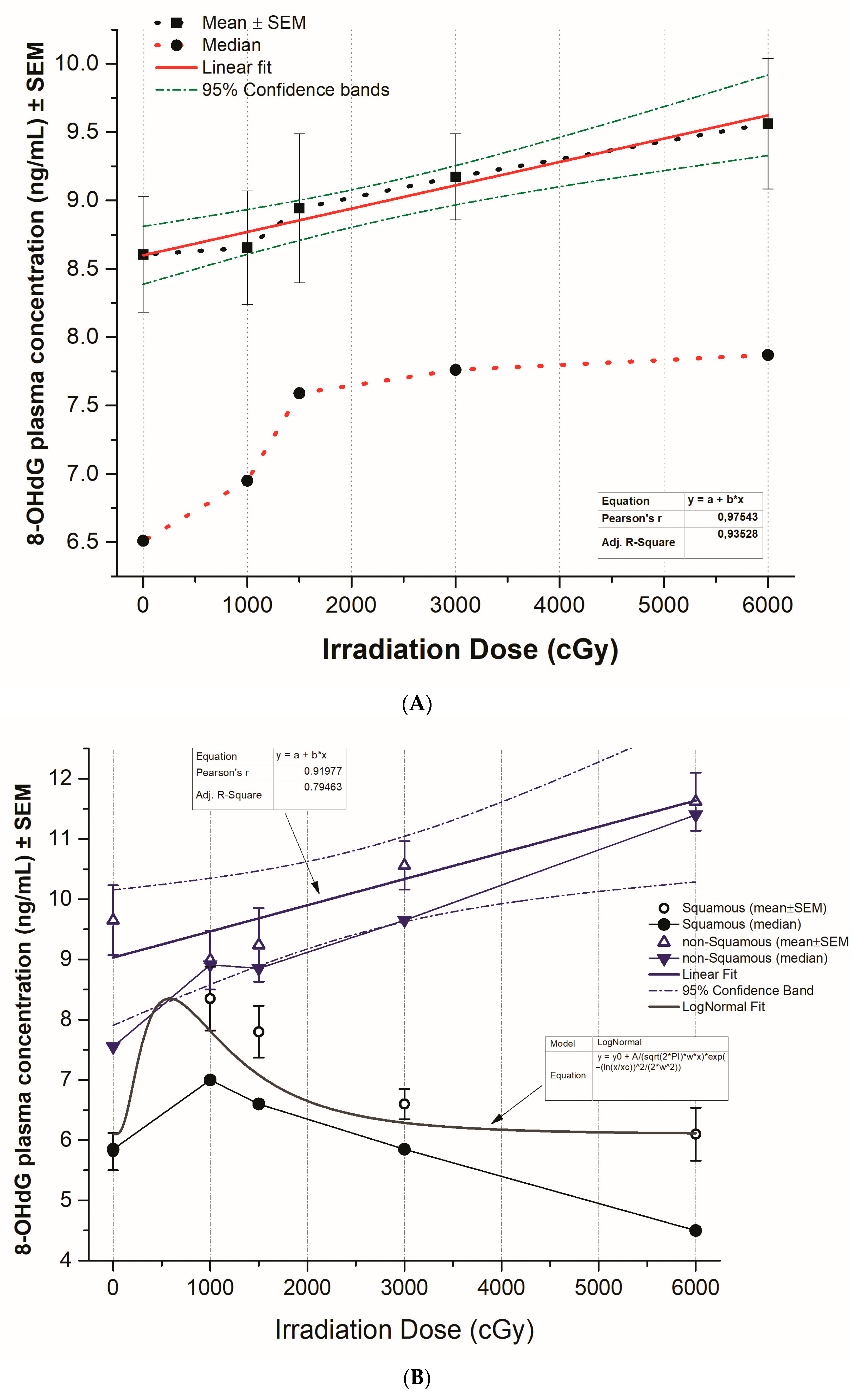
3.2. Plasma 8-OHdG Levels in Patients Receiving Radiotherapy
3.3. The Pattern of 8-OHdG Levels in Squamous versus Non-Squamous NSCLC
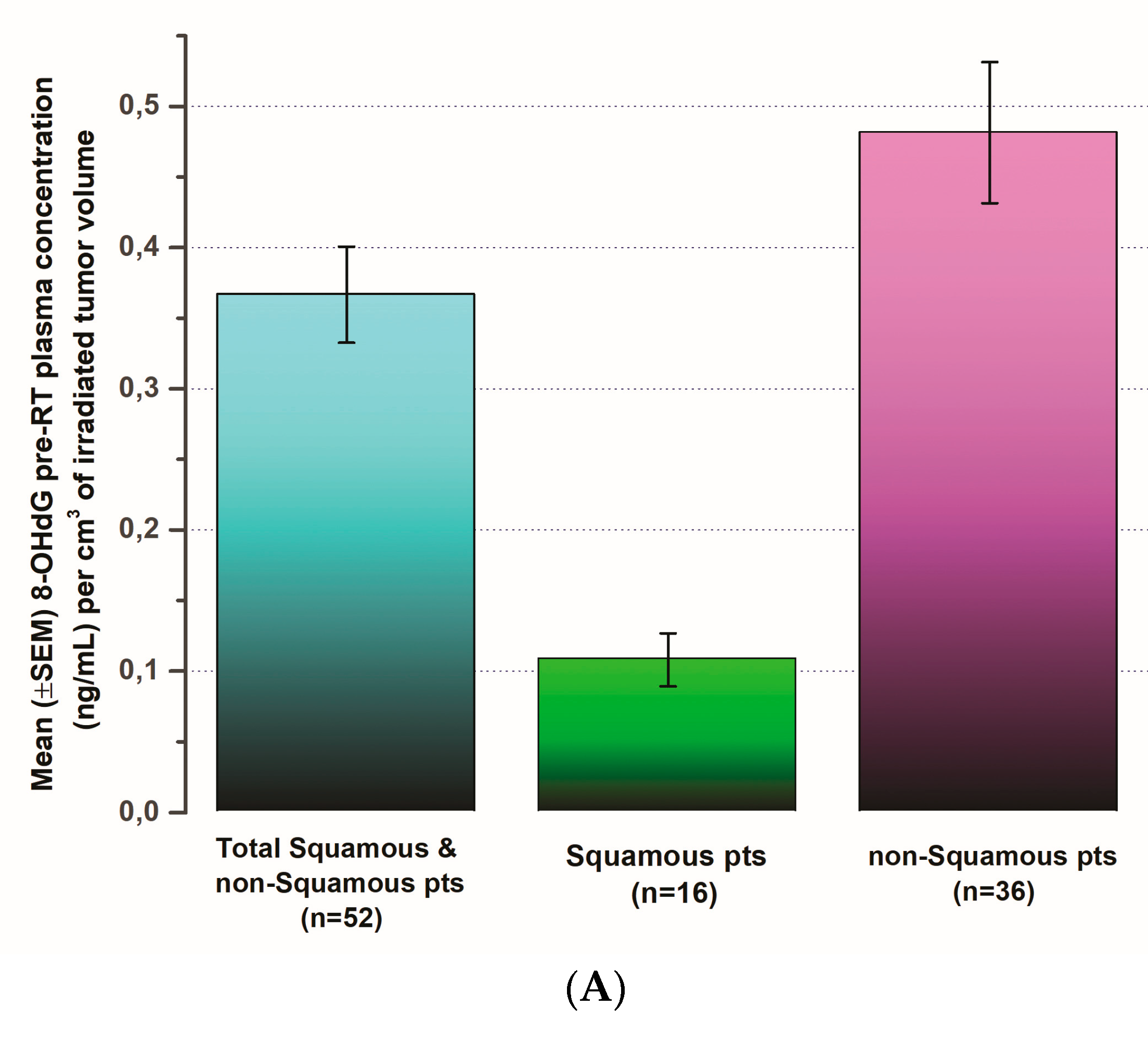
3.4. The Pattern of 8-OHdG Levels in Comparison to Pre-Operative Tumor Volume
3.5. 8-OHdG Plasma Concentration Changes and the Tumor Response Rate
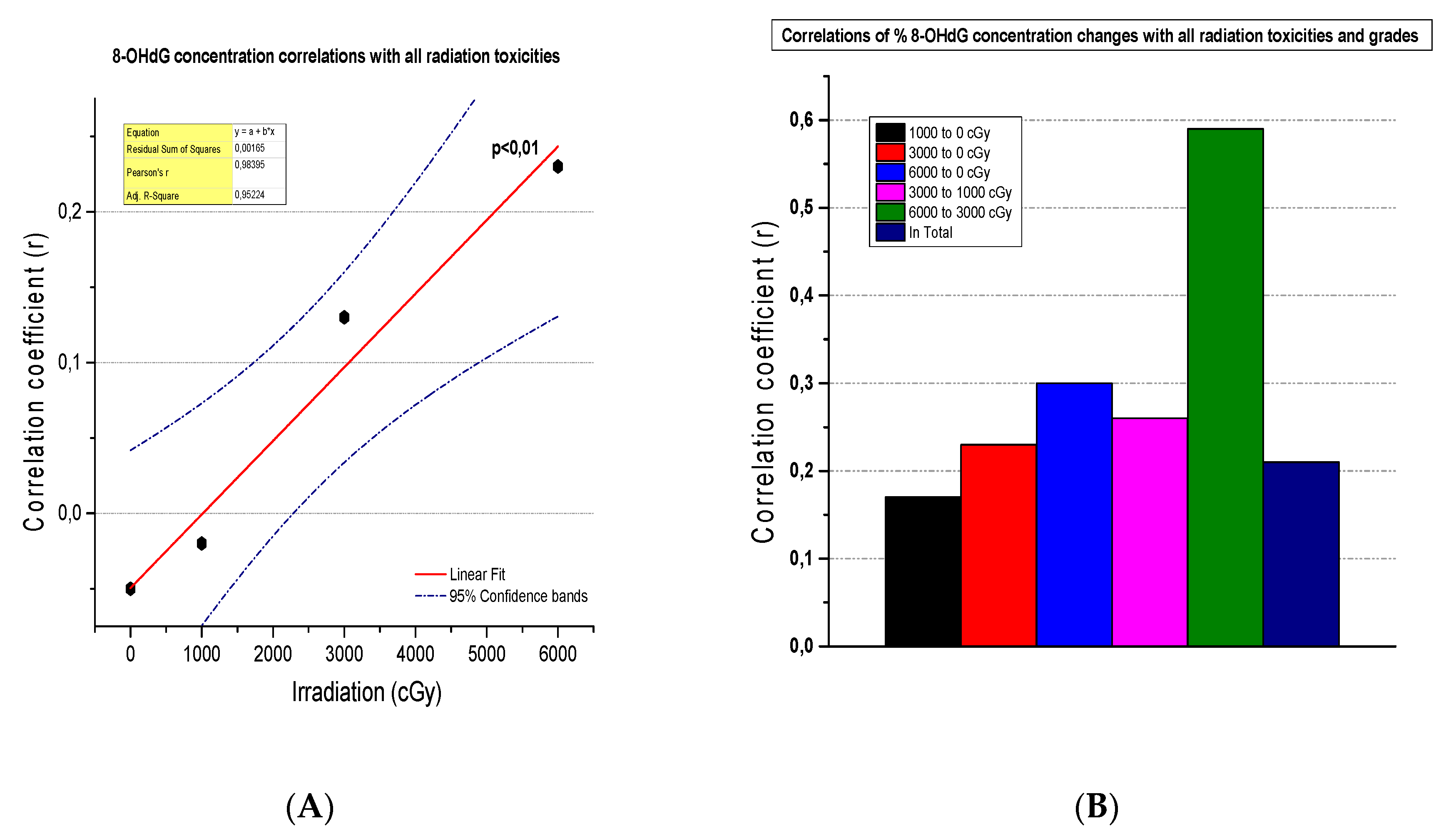
3.6. The Correlation of 8-OHdG Plasma Concentrations and Toxicities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer Statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. (Eds.) SEER Cancer Statistics Review, 1975–2016; National Cancer Institute: Bethesda, MD, USA, 2020. Available online: https://seer.cancer.gov/csr/1975_2016/ (accessed on 20 January 2023).
- SEER. Cancer Stat Facts: Lung and Bronchus Cancer. Available online: https://seer.cancer.gov/statfacts/html/lungb.html (accessed on 20 January 2023).
- Trafalis, D.T.; Alifieris, C.; Stathopoulos, G.P.; Sitaras, N. Phase II Study of Bevacizumab plus Irinotecan on the Treatment of Relapsed Resistant Small Cell Lung Cancer. Cancer Chemother. Pharmacol. 2016, 77, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Masuda, Y.; Kamiya, K. Molecular Nature of Radiation Injury and DNA Repair Disorders Associated with Radiosensitivity. Int. J. Hematol. 2012, 95, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Verigos, K.E.; Sagredou, S.; Orfanakos, K.; Dalezis, P.; Trafalis, D.T. 8-Hydroxy-2′-Deoxyguanosine and 8-Nitroguanine Production and Detection in Blood Serum of Breast Cancer Patients in Response to Postoperative Complementary External Ionizing Irradiation of Normal Tissues. Dose. Res. 2020, 18, 1559325820982172. [Google Scholar] [CrossRef] [PubMed]
- Borrego-Soto, G.; Ortiz-López, R.; Rojas-Martínez, A. Ionizing Radiation-Induced DNA Injury and Damage Detection in Patients with Breast Cancer. Genet. Mol. Biol. 2015, 38, 420–432. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.R.; Arthur, D.W. The Emergence of Advanced Brachytherapy Techniques for Common Malignancies. Hematol. Oncol. Clin. N. Am. 2006, 20, 97–118. [Google Scholar] [CrossRef]
- Hall, E.J.; Astor, M.; Bedford, J.; Borek, C.; Curtis, S.B.; Fry, M.; Geard, C.; Hei, T.; Mitchell, J.; Oleinick, N.; et al. Basic Radiobiology. Am. J. Clin. Oncol. Cancer Clin. Trials 1988, 11, 220–252. [Google Scholar] [CrossRef]
- O’Neill, P.; Wardman, P. Radiation Chemistry Comes before Radiation Biology. Int. J. Radiat. Biol. 2009, 85, 9–25. [Google Scholar] [CrossRef]
- Ahmad, I.M.; Abdalla, M.Y.; Moore, T.A.; Bartenhagen, L.; Case, A.J.; Zimmerman, M.C. Healthcare Workers Occupationally Exposed to Ionizing Radiation Exhibit Altered Levels of Inflammatory Cytokines and Redox Parameters. Antioxidants 2019, 8, 12. [Google Scholar] [CrossRef]
- Gao, Y.; Wang, P.; Wang, Z.; Han, L.; Li, J.; Tian, C.; Zhao, F.; Wang, J.; Zhao, F.; Zhang, Q.; et al. Serum 8-Hydroxy-2′-Deoxyguanosine Level as a Potential Biomarker of Oxidative DNA Damage Induced by Ionizing Radiation in Human Peripheral Blood. Dose. Res. 2019, 17, 1559325818820649. [Google Scholar] [CrossRef]
- Pilger, A.; Rüdiger, H.W. 8-Hydroxy-2′-Deoxyguanosine as a Marker of Oxidative DNA Damage Related to Occupational and Environmental Exposures. Int. Arch. Occup. Environ. Health 2006, 80, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Petkau, A. Role of Superoxide Dismutase in Modification of Radiation Injury. Br. J. Cancer 1987, 55, 87–95. [Google Scholar]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Schilsky, R.L.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. American Joint Committee on Cancer (AJCC). In AJCC Cancer Staging Manual; Springer: Cham, Switzerland, 2017; ISBN 9783319406176. [Google Scholar]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (Version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Basch, E.; Reeve, B.B.; Mitchell, S.A.; Clauser, S.B.; Minasian, L.M.; Dueck, A.C.; Mendoza, T.R.; Hay, J.; Atkinson, T.M.; Abernethy, A.P.; et al. Development of the National Cancer Institute’s Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). J. Natl. Cancer Inst. 2014, 106, dju244. [Google Scholar] [CrossRef] [PubMed]
- Erhola, M.; Toyokuni, S.; Okada, K.; Tanaka, T.; Hiai, H.; Ochi, H.; Uchida, K.; Osawa, T.; Nieminen, M.M.; Alho, H.; et al. Biomarker Evidence of DNA Oxidation in Lung Cancer Patients: Association of Urinary 8-Hydroxy-2′-Deoxyguanosine Excretion with Radiotherapy, Chemotherapy, and Response to Treatment. FEBS Lett. 1997, 409, 287–291. [Google Scholar] [CrossRef]
- Yamazaki, H.; Inoue, T.; Koizumi, M.; Tanaka, E.; Yoshioka, Y.; Nakamura, H.; Shuo, X.; Inoue, T. Urinary 8-Hydroxy-2′-Deoxyguanosine Excretion as a Biomarker for Estimating DNA Oxidation in Patients Undergoing External Radiotherapy and/or Brachytherapy. Oncol. Rep. 2005, 13, 847–851. [Google Scholar] [CrossRef]
- AbuArrah, M.; Yuli Setianto, B.; Faisal, A.; Hamim Sadewa, A. 8-Hydroxy-2-Deoxyguanosine as Oxidative DNA Damage Biomarker of Medical Ionizing Radiation: A Scoping Review. J. Biomed. Phys. Eng. 2021, 11, 389–402. [Google Scholar] [CrossRef]
- Mrdjanovic, J.; Sudji, J.; Srdjenovic, B.; Dojcinovic, S.; Bogdanovic, V.; Jakovljevic, D.K.; Jurisic, V. Accidental Use of Milk With an Increased Concentration of Aflatoxins Causes Significant DNA Damage in Hospital Workers Exposed to Ionizing Radiation. Front. Public Health 2020, 8, 323. [Google Scholar] [CrossRef]
- Salehi, A.; Ebrahimpour, K.; Forouharmajd, F.; Zarean, M. The Relationship between Collective Effective Doses of Radiation and Urinary Concentration of 8-Dihydroxy-2′-Deoxyguanosine among Radiography Staff. Int. J. Radiat. Res. 2020, 18, 587–592. [Google Scholar]
- Kato, S.; Yoshimura, K.; Kimata, T.; Mine, K.; Uchiyama, T.; Kaneko, K. Urinary 8-Hydroxy-2′-Deoxyguanosine: A Biomarker for Radiation-Induced Oxidative DNA Damage in Pediatric Cardiac Catheterization. J. Pediatr. 2015, 167, 1369–1374.e1. [Google Scholar] [CrossRef]
- Bubici, C.; Papa, S.; Dean, K.; Franzoso, G. Mutual Cross-Talk between Reactive Oxygen Species and Nuclear Factor-Kappa B: Molecular Basis and Biological Significance. Oncogene 2006, 25, 6731–6748. [Google Scholar] [CrossRef]
- Crohns, M.; Saarelainen, S.; Erhola, M.; Alho, H.; Kellokumpu-Lehtinen, P. Impact of Radiotherapy and Chemotherapy on Biomarkers of Oxidative DNA Damage in Lung Cancer Patients. Clin. Biochem. 2009, 42, 1082–1090. [Google Scholar] [CrossRef] [PubMed]
- Qing, X.; Shi, D.; Lv, X.; Wang, B.; Chen, S.; Shao, Z. Prognostic Significance of 8-Hydroxy-2′-Deoxyguanosine in Solid Tumors: A Meta-Analysis. BMC Cancer 2019, 19, 997. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Li, X.; Wang, R.; Yu, J.; Ye, M.; Mao, L.; Zhang, S.; Zheng, S. Association between Oxidative DNA Damage and Risk of Colorectal Cancer: Sensitive Determination of Urinary 8-Hydroxy-2′-Deoxyguanosine by UPLC-MS/MS Analysis. Sci. Rep. 2016, 6, 32581. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.W.; Chou, S.Y.; Hu, T.W.; Wu, F.Y.; Chen, D.J. Urinary 8-Hydroxy-2′-Deoxyguanosine (8-OHdG) and Genetic Polymorphisms in Breast Cancer Patients. Mutat. Res. 2007, 631, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Karihtala, P.; Soini, Y.; Vaskivuo, L.; Bloigu, R.; Puistola, U. DNA Adduct 8-Hydroxydeoxyguanosine, a Novel Putative Marker of Prognostic Significance in Ovarian Carcinoma. Int. J. Gynecol. Cancer 2009, 19, 1047–1051. [Google Scholar] [CrossRef] [PubMed]
- Pylväs-Eerola, M.; Karihtala, P.; Puistola, U. Preoperative Serum 8-Hydroxydeoxyguanosine Is Associated with Chemoresistance and Is a Powerful Prognostic Factor in Endometrioid-Type Epithelial Ovarian Cancer. BMC Cancer 2015, 15, 493. [Google Scholar] [CrossRef]
- Loft, S.; Vistisen, K.; Ewertz, M.; Tjønneland, A.; Overvad, K.; Poulsen, H.E. Oxidative DNA Damage Estimated by 8-Hydroxydeoxyguanosine Excretion in Humans: Influence of Smoking, Gender and Body Mass Index. Carcinogenesis 1992, 13, 2241–2247. [Google Scholar] [CrossRef]
- Akçay, T.; Saygili, I.; Andican, G.; Yalçin, V. Increased Formation of 8-Hydroxy-2′-Deoxyguanosine in Peripheral Blood Leukocytes in Bladder Cancer. Urol. Int. 2003, 71, 271–274. [Google Scholar] [CrossRef]
- Perdyan, A.; Jassem, J. Impact of Tobacco Smoking on Outcomes of Radiotherapy: A Narrative Review. Curr. Oncol. 2022, 29, 2284–2300. [Google Scholar] [CrossRef]
- Rades, D.; Setter, C.; Schild, S.E.; Dunst, J. Effect of Smoking during Radiotherapy, Respiratory Insufficiency, and Hemoglobin Levels on Outcome in Patients Irradiated for Non-Small-Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 1134–1142. [Google Scholar] [CrossRef]
- Hernando, M.L.; Marks, L.B.; Bentel, G.C.; Zhou, S.M.; Hollis, D.; Das, S.K.; Fan, M.; Munley, M.T.; Shafman, T.D.; Anscher, M.S.; et al. Radiation-Induced Pulmonary Toxicity: A Dose-Volume Histogram Analysis in 201 Patients with Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Huang, X.; Cao, Y.; Mao, Y.; Zhu, Y.; Zhang, Q.; Zhang, T.; Chang, L.; Wang, C. Dynamic Analysis of Predictive Biomarkers for Radiation Therapy Efficacy in Non-Small Cell Lung Cancer Patients by next-Generation Sequencing Based on Blood Specimens. Pathol. Res. Pract. 2023, 253, 154972. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Zhang, S.; Pang, J.; Yin, J.C.; Mu, D.; Wang, J.; Ge, H.; Ma, J.; Yang, Z.; Zheng, X.; et al. Genomic Profiling Reveals Novel Predictive Biomarkers for Chemo-Radiotherapy Efficacy and Thoracic Toxicity in Non-Small-Cell Lung Cancer. Front. Oncol. 2022, 12, 928605. [Google Scholar] [CrossRef] [PubMed]
- Turnu, L.; Porro, B.; Alfieri, V.; Di Minno, A.; Russo, E.; Barbieri, S.; Bonomi, A.; Dello Russo, A.; Tondo, C.; D’Alessandra, Y.; et al. Does Fluoroscopy Induce DNA Oxidative Damage in Patients Undergoing Catheter Ablation? Antioxid. Redox Signal. 2018, 28, 1137–1143. [Google Scholar] [CrossRef] [PubMed]
- Pirich, C.; Pilger, A.; Schwameis, E.; Germadnik, D.; Prüfert, U.; Havlik, E.; Lang, S.; Kvaternik, H.; Flores, J.A.; Angelberger, P.; et al. Radiation Synovectomy Using 165Dy Ferric-Hydroxide and Oxidative DNA Damage in Patients with Different Types of Arthritis. J. Nucl. Med. 2000, 41, 250–256. [Google Scholar]
- Graille, M.; Wild, P.; Sauvain, J.J.; Hemmendinger, M.; Canu, I.G.; Hopf, N.B. Urinary 8-OHdG as a Biomarker for Oxidative Stress: A Systematic Literature Review and Meta-Analysis. Int. J. Mol. Sci. 2020, 21, 3743. [Google Scholar] [CrossRef]
- Kroese, L.J.; Scheffer, P.G. 8-Hydroxy-2′-Deoxyguanosine and Cardiovascular Disease: A Systematic Review. Curr. Atheroscler. Rep. 2014, 16, 452. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Total number (N) of patients | 52 |
| Sex (N) | |
| Male | 37 |
| Female | 15 |
| Age (y) in average (range) | 66.8 (53–76) |
| Smoking n, (%) | 52 (100%) |
| Histology (N) | |
| Squamous (SQ) | 16 |
| Non-squamous (NSQ) | 36 |
| Stage (N) | |
| IIIA | 4 |
| IIIB | 17 |
| IIIC | 31 |
| Chemotherapy 1 (N) | |
| Before radiotherapy | 20 |
| Post radiotherapy | 11 |
| Pre- and Post-radiotherapy | 14 |
| Concurrently | 0 |
| No chemotherapy | 7 |
| Overall Response Rate, n (%) | |
| Squamous | 11 (68.8%) |
| Non-squamous | 21 (58.3%) |
| Body Surface Area (BSA) (m2), mean (range) | 1.80 (1.45–2.02) |
| Body Mass Index (BMI) (kg/m2), mean (range) | 26.76 (20.16–30.42) |
| Irradiated Tumor Volume (TV) (cm3), mean (range) | |
| Squamous (SQ) | 163.56 (30.5–376.8) |
| Non-squamous (NSQ) | 178.14 (18.1–811.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orfanakos, K.; Alifieris, C.E.; Verigos, E.K.; Deligiorgi, M.V.; Verigos, K.E.; Panayiotidis, M.I.; Nikolaou, M.; Trafalis, D.T. The Predictive Value of 8-Hydroxy-Deoxyguanosine (8-OHdG) Serum Concentrations in Irradiated Non-Small Cell Lung Carcinoma (NSCLC) Patients. Biomedicines 2024, 12, 134. https://doi.org/10.3390/biomedicines12010134
Orfanakos K, Alifieris CE, Verigos EK, Deligiorgi MV, Verigos KE, Panayiotidis MI, Nikolaou M, Trafalis DT. The Predictive Value of 8-Hydroxy-Deoxyguanosine (8-OHdG) Serum Concentrations in Irradiated Non-Small Cell Lung Carcinoma (NSCLC) Patients. Biomedicines. 2024; 12(1):134. https://doi.org/10.3390/biomedicines12010134
Chicago/Turabian StyleOrfanakos, Kyriakos, Constantinos E. Alifieris, Emmanouil K. Verigos, Maria V. Deligiorgi, Kosmas E. Verigos, Mihalis I. Panayiotidis, Michail Nikolaou, and Dimitrios T. Trafalis. 2024. "The Predictive Value of 8-Hydroxy-Deoxyguanosine (8-OHdG) Serum Concentrations in Irradiated Non-Small Cell Lung Carcinoma (NSCLC) Patients" Biomedicines 12, no. 1: 134. https://doi.org/10.3390/biomedicines12010134