
A Retrospective Study on tDCS Treatment in Patients with Drug-Resistant Chronic Pain
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Transcranial Direct Current Stimulation and Placement of Electrodes
2.3. Clinical Assessment
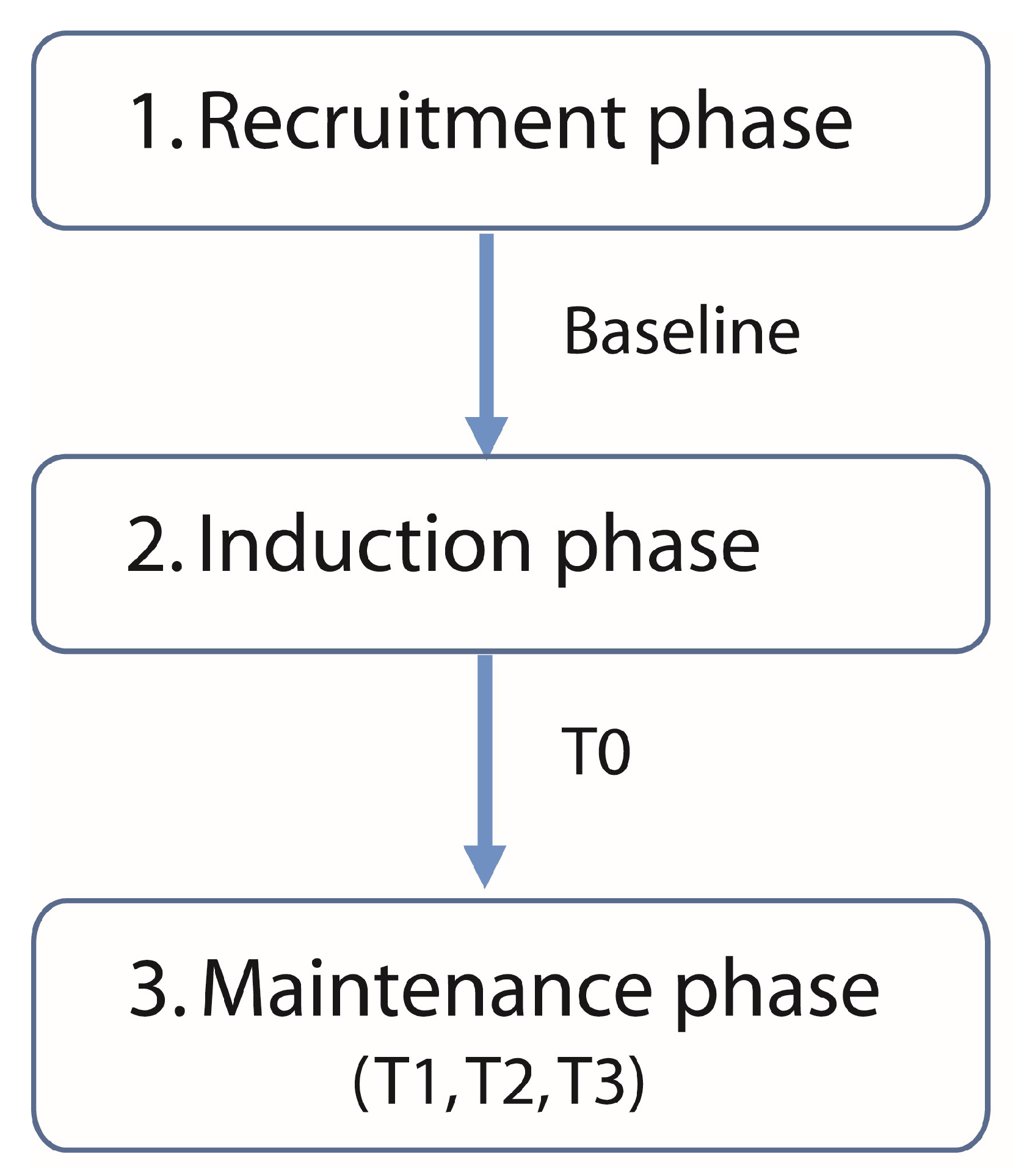
2.4. Phases of the Protocol and Experimental Design
2.5. Statistical Analysis
3. Results
3.1. Description of the Sample
3.2. Description of the Treatment Effects
3.2.1. Safety and Discomfort Caused by tDCS
3.2.2. “Responders”
3.2.3. Influence of Type of Stimulation
3.2.4. tDCS Effects on Pain Intensity in the “Responder” Group
3.2.5. Probability to Predict the “Responders” at Baseline Evaluation
3.2.6. “Responders” and PGIC
4. Discussion
4.1. Safety of the Treatment
4.2. Efficacy of the Treatment
4.3. Treatment Success Factors
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Loeser, J.D.; Treede, R.D. The Kyoto Protocol of IASP Basic Pain Terminology. Pain 2008, 137, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. A Classification of Chronic Pain for ICD-11. Pain 2015, 156, 1003–1007. [Google Scholar] [CrossRef] [PubMed]
- Jensen, T.S.; Baron, R.; Haanpää, M.; Kalso, E.; Loeser, J.D.; Rice, A.S.; Treede, R.D. A New Definition of Neuropathic Pain. Pain 2011, 152, 2204–2205. [Google Scholar] [CrossRef] [PubMed]
- Pasero, C. Pathophysiology of Neuropathic Pain. Pain Manag. Nurs. 2004, 5, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Mannerkorpi, K.; Burckhardt, C.S.; Bjelle, A. Physical Performance Characteristics of Women with Fibromyalgia. Arthritis Rheumatol. 1994, 7, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Cabo-Meseguer, A.; Cerdá-Olmedo, G.; Trillo-Mata, J.L. Fibromialgia: Prevalencia, Perfiles Epidemiológicos y Costes Económicos. Med. Clin. 2017, 149, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Arthritis Rheumatol. 1990, 33, 160–172. [Google Scholar] [CrossRef]
- Pacheco-Barrios, K.; Cardenas-Rojas, A.; Thibaut, A.; Costa, B.; Ferreira, I.; Caumo, W.; Fregni, F. Methods and Strategies of TDCS for the Treatment of Pain: Current Status and Future Directions. Expert Rev. Med. Dev. 2020, 17, 879–898. [Google Scholar] [CrossRef]
- Lefaucheur, J.P.; Antal, A.; Ayache, S.S.; Benninger, D.H.; Brunelin, J.; Cogiamanian, F.; Cotelli, M.; De Ridder, D.; Ferrucci, R.; Langguth, B.; et al. Evidence-Based Guidelines on the Therapeutic Use of Transcranial Direct Current Stimulation (TDCS). Clin. Neurophysiol. 2017, 128, 56–92. [Google Scholar] [CrossRef]
- Pérez-Borrego, Y.A.; Campolo, M.; Soto-León, V.; Rodriguez-Matas, M.J.; Ortega, E.; Oliviero, A. Pain Treatment Using TDCS in a Single Patient: Tele-Medicine Approach in Non-Invasive Brain Simulation. Brain Stimul. 2014, 7, 334–335. [Google Scholar] [CrossRef]
- Palm, U.; Kumpf, U.; Behler, N.; Wulf, L.; Kirsch, B.; Wörsching, J.; Keeser, D.; Hasan, A.; Padberg, F. Home Use, Remotely Supervised, and Remotely Controlled Transcranial Direct Current Stimulation: A Systematic Review of the Available Evidence. Neuromodulation 2018, 21, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Fregni, F.; Boggio, P.S.; Lima, M.C.; Ferreira, M.J.L.; Wagner, T.; Rigonatti, S.P.; Castro, A.W.; Souza, D.R.; Riberto, M.; Freedman, S.D.; et al. A Sham-Controlled, Phase II Trial of Transcranial Direct Current Stimulation for the Treatment of Central Pain in Traumatic Spinal Cord Injury. Pain 2006, 122, 197–209. [Google Scholar] [CrossRef] [PubMed]
- Antal, A.; Terney, D.; Kühnl, S.; Paulus, W. Anodal Transcranial Direct Current Stimulation of the Motor Cortex Ameliorates Chronic Pain and Reduces Short Intracortical Inhibition. J. Pain Symptom Manag. 2010, 39, 890–903. [Google Scholar] [CrossRef] [PubMed]
- Cruccu, G.; Aziz, T.Z.; Garcia-Larrea, L.; Hansson, P.; Jensen, T.S.; Lefaucheur, J.P.; Simpson, B.A.; Taylor, R.S. EFNS Guidelines on Neurostimulation Therapy for Neuropathic Pain. Eur. J. Neurol. 2007, 14, 952–970. [Google Scholar] [CrossRef] [PubMed]
- Katz, N. Enriched Enrollment Randomized Withdrawal Trial Designs of Analgesics: Focus on Methodology. Clin. J. Pain 2009, 25, 797–807. [Google Scholar] [CrossRef]
- Lefaucheur, J.-P.; Drouot, X.; Menard-Lefaucheur, I.; Zerah, F.; Bendib, B.; Cesaro, P.; Keravel, Y.; Nguyen, J.-P. Neurogenic Pain Relief by Repetitive Transcranial Magnetic Cortical Stimulation Depends on the Origin and the Site of Pain. J. Neurol. Neurosurg. Psychiatry 2004, 75, 612–616. [Google Scholar] [CrossRef] [PubMed]
- Bikson, M.; Grossman, P.; Thomas, C.; Zannou, A.L.; Jiang, J.; Adnan, T.; Mourdoukoutas, A.P.; Kronberg, G.; Truong, D.; Boggio, P.; et al. Safety of Transcranial Direct Current Stimulation: Evidence Based Update 2016. Brain Stimul. 2016, 9, 641–661. [Google Scholar] [CrossRef]
- Poreisz, C.; Boros, K.; Antal, A.; Paulus, W. Safety Aspects of Transcranial Direct Current Stimulation Concerning Healthy Subjects and Patients. Brain Res. Bull. 2007, 72, 208–214. [Google Scholar] [CrossRef]
- Brunoni, A.R.; Amadera, J.; Berbel, B.; Volz, M.S.; Rizzerio, B.G.; Fregni, F. A Systematic Review on Reporting and Assessment of Adverse Effects Associated with Transcranial Direct Current Stimulation. Int. J. Neuropsychopharmacol. 2011, 14, 1133–1145. [Google Scholar] [CrossRef]
- McFadden, J.L.; Borckardt, J.J.; George, M.S.; Beam, W. Reducing Procedural Pain and Discomfort Associated with Transcranial Direct Current Stimulation. Brain Stimul. 2011, 4, 38–42. [Google Scholar] [CrossRef]
- Loo, C.K.; Martin, D.M.; Alonzo, A.; Gandevia, S.; Mitchell, P.B.; Sachdev, P. Avoiding Skin Burns with Transcranial Direct Current Stimulation: Preliminary Considerations. Int. J. Neuropsychopharmacol. 2011, 14, 425–426. [Google Scholar] [CrossRef] [PubMed]
- Palm, U.; Feichtner, K.B.; Hasan, A.; Gauglitz, G.; Langguth, B.; Nitsche, M.A.; Keeser, D.; Padberg, F. The Role of Contact Media at the Skin-Electrode Interface during Transcranial Direct Current Stimulation (TDCS). Brain Stimul. 2014, 7, 762–764. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Hjermstad, M.J.; Fayers, P.M.; Haugen, D.F.; Caraceni, A.; Hanks, G.W.; Loge, J.H.; Fainsinger, R.; Aass, N.; Kaasa, S.; European Palliative Care Research Collaborative (EPCRC). Studies Comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for Assessment of Pain Intensity in Adults: A Systematic Literature Review. J. Pain Symptom Manag. 2011, 41, 1073–1093. [Google Scholar] [CrossRef] [PubMed]
- Scott, W.; McCracken, L.M. Patients’ Impression of Change Following Treatment for Chronic Pain: Global, Specific, a Single Dimension, or Many? J. Pain 2015, 16, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Fertonani, A.; Ferrari, C.; Miniussi, C. What Do You Feel If I Apply Transcranial Electric Stimulation? Safety, Sensations and Secondary Induced Effects. Clin. Neurophysiol. 2015, 126, 2181–2188. [Google Scholar] [CrossRef]
- Zewdie, E.; Ciechanski, P.; Kuo, H.C.; Giuffre, A.; Kahl, C.; King, R.; Cole, L.; Godfrey, H.; Seeger, T.; Swansburg, R.; et al. Safety and Tolerability of Transcranial Magnetic and Direct Current Stimulation in Children: Prospective Single Center Evidence from 3.5 Million Stimulations. Brain Stimul. 2020, 13, 565–575. [Google Scholar] [CrossRef]
- Nikolin, S.; Martin, D.; Loo, C.K.; Boonstra, T.W. Effects of TDCS Dosage on Working Memory in Healthy Participants. Brain Stimul. 2018, 11, 518–527. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Nitsche, M.S.; Klein, C.C.; Tergau, F.; Rothwell, J.C.; Paulus, W. Level of Action of Cathodal DC Polarisation Induced Inhibition of the Human Motor Cortex. Clin. Neurophysiol. 2003, 114, 600–604. [Google Scholar] [CrossRef]
- Baber, N. International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH). Br. J. Clin. Pharmacol. 1994, 37, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Fregni, F.; El-Hagrassy, M.M.; Pacheco-Barrios, K.; Carvalho, S.; Leite, J.; Simis, M.; Brunelin, J.; Nakamura-Palacios, E.M.; Marangolo, P.; Venkatasubramanian, G.; et al. Evidence-Based Guidelines and Secondary Meta-Analysis for the Use of Transcranial Direct Current Stimulation in Neurological and Psychiatric Disorders. Int. J. Neuropsychopharmacol. 2021, 24, 256–313. [Google Scholar] [CrossRef] [PubMed]
- Brocalero-Camacho, A.; Pérez-Borrego, Y.A.; Soto-León, V.; Rodriguez-Matas, M.J.; Foffani, G.; Oliviero, A. Effects of COVID-19 Lockdown on Chronic Drug-Resistant Pain Patients Treated Using Brain Stimulation Approaches. Brain Stimul. 2020, 13, 1089–1090. [Google Scholar] [CrossRef]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical Importance of Changes in Chronic Pain Intensity Measured on an 11-Point Numerical Pain Rating Scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Perrot, S.; Lantéri-Minet, M. Patients’ Global Impression of Change in the Management of Peripheral Neuropathic Pain: Clinical Relevance and Correlations in Daily Practice. Eur. J. Pain 2019, 23, 1117–1128. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Subjects (N) | 155 |
|---|---|
| Gender (males N (%)) | 60 (38.7%) |
| Age, years (mean ± SD) | 49.26 ± 11.69 |
| Duration of Pain, years (median [IQR]) | 6 [3–12] |
| MMSE (median [IQR]) | 29 [27–30] |
| BDI (median [IQR]) | 19 [12–28] |
| VAS_Baseline, mm (median [IQR]) | 77 [62.5–86.5] |
| Diagnostic Groups (N (%)) | |
| SCI | 51 (32.9%) |
| FBSS | 15 (9.7%) |
| FM | 40 (25.8%) |
| Others | 49 (31.6%) |
| Baseline Medication (N (%)) | |
| Antidepressant | 90 (58.1%) |
| Gabapentin | 20 (12.9%) |
| Pregabalin | 7 (4.5%) |
| Other Anticonvulsant | 68 (43.8%) |
| Opioids (Minor and Major) | 57 (36.7%) |
| Cannabinoid | 2 (1.3%) |
| Benzodiazepine | 62 (40%) |
| NSAID | 25 (16.1%) |
| Other Analgesic | 28 (18%) |
| Baclofen | 17 (10.9%) |
| Capsaicine/Local Administration | 8 (5.2%) |
| Other Medications | 58 (37.4%) |
| N | SCI (51) | FBSS (15) | FM (40) | OTHERS (49) | p |
|---|---|---|---|---|---|
| Gender (male (%)) | 68.6% | 33.3% | 7.5% | 34.6% | p < 0.001 |
| Age, years (mean ± SD) | 48.2 ± 11.3 | 50.5 ± 9.0 | 48.8 ± 9.2 | 50.4 ± 14.5 | p = 0.780 |
| Duration of Pain, years (median [IQR]) | 6 [2–12] | 6 [4–13] | 10 [6–17] | 4 [2–7] | p < 0.001 |
| MMSE (median [IQR]) | 28 [27–30] | 29 [28–30] | 29 [27–30] | 29 [28–30] | p = 0.470 |
| BDI (median [IQR]) | 16 [11–25] | 21 [16–27] | 26 [16–34] | 18 [10–26] | p < 0.003 |
| VAS_Baseline, mm (median [IQR]) | 77 [64–87] | 84 [76–92] | 76 [60–88] | 74 [59–81] | p = 0.168 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Borrego, Y.A.; Soto-León, V.; Brocalero-Camacho, Á.; Oliviero, A.; Carrasco-López, C. A Retrospective Study on tDCS Treatment in Patients with Drug-Resistant Chronic Pain. Biomedicines 2024, 12, 115. https://doi.org/10.3390/biomedicines12010115
Pérez-Borrego YA, Soto-León V, Brocalero-Camacho Á, Oliviero A, Carrasco-López C. A Retrospective Study on tDCS Treatment in Patients with Drug-Resistant Chronic Pain. Biomedicines. 2024; 12(1):115. https://doi.org/10.3390/biomedicines12010115
Chicago/Turabian StylePérez-Borrego, Yolanda A., Vanesa Soto-León, Ángela Brocalero-Camacho, Antonio Oliviero, and Carmen Carrasco-López. 2024. "A Retrospective Study on tDCS Treatment in Patients with Drug-Resistant Chronic Pain" Biomedicines 12, no. 1: 115. https://doi.org/10.3390/biomedicines12010115