
Advances in Histological and Molecular Classification of Hepatocellular Carcinoma

Abstract
:1. Introduction
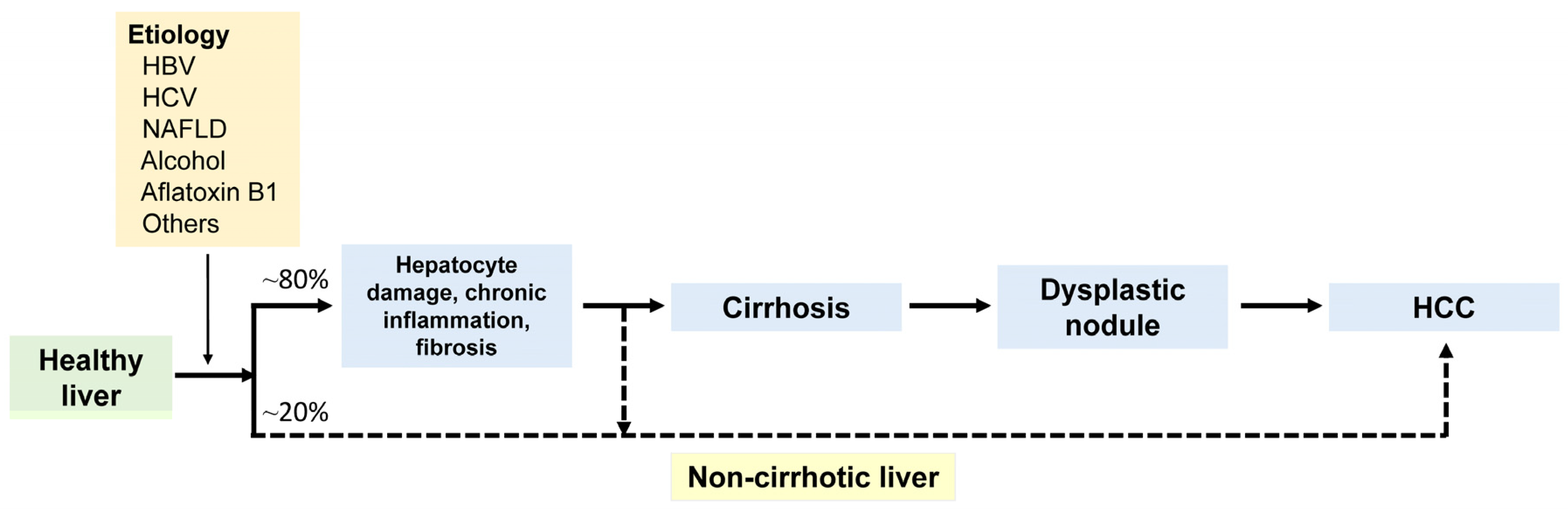
2. Etiology
3. Pathogenesis
4. Clinical Features
5. Radiological Features
6. Molecular Features
7. Immunohistochemical Features
8. Pathological Features of Conventional Hepatocellular Carcinoma
8.1. Macroscopic Features
8.2. Microscopic Features
9. Subtypes of Hepatocellular Carcinoma
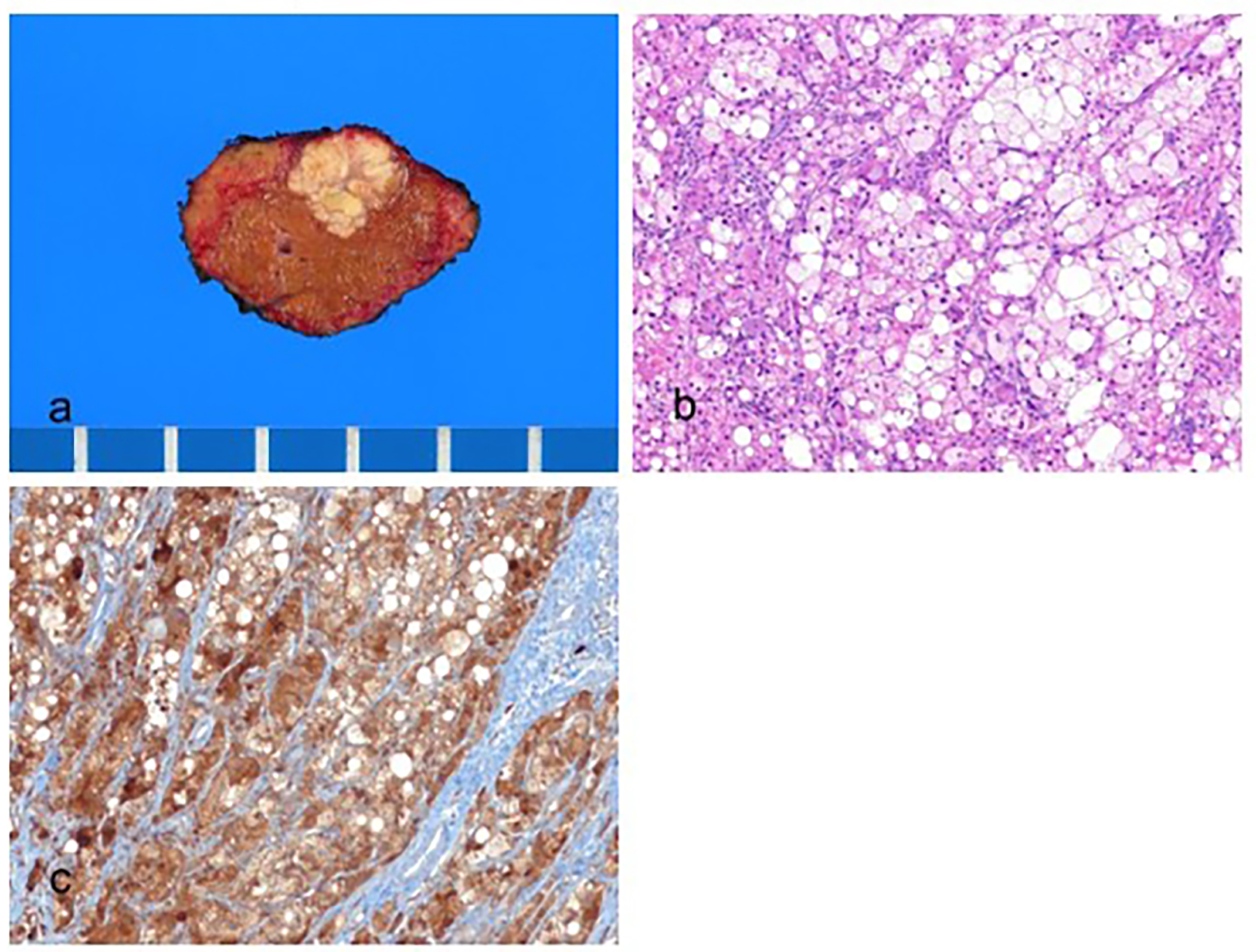
9.1. Steatohepatitic Hepatocellular Carcinoma
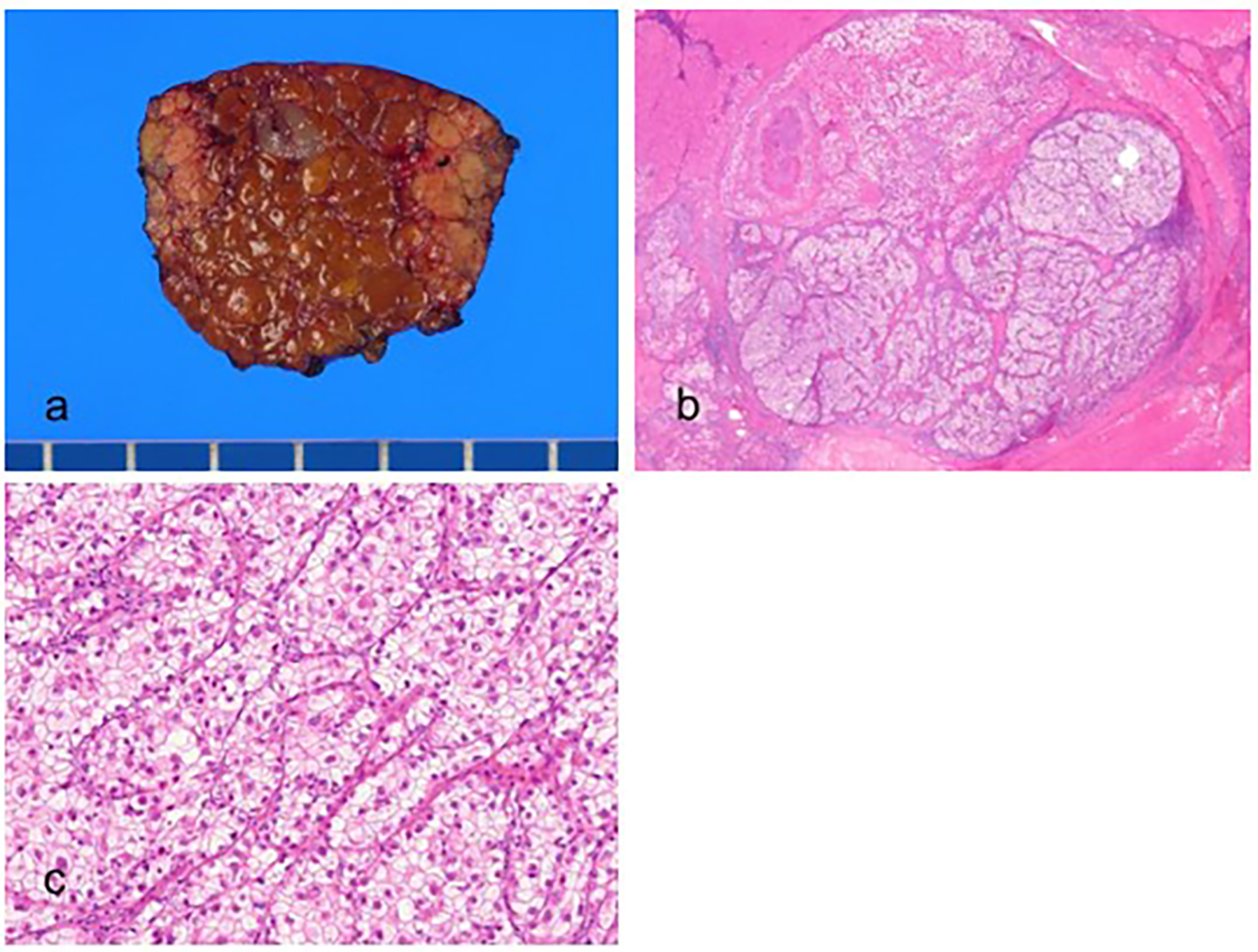
9.2. Clear Cell Hepatocellular Carcinoma
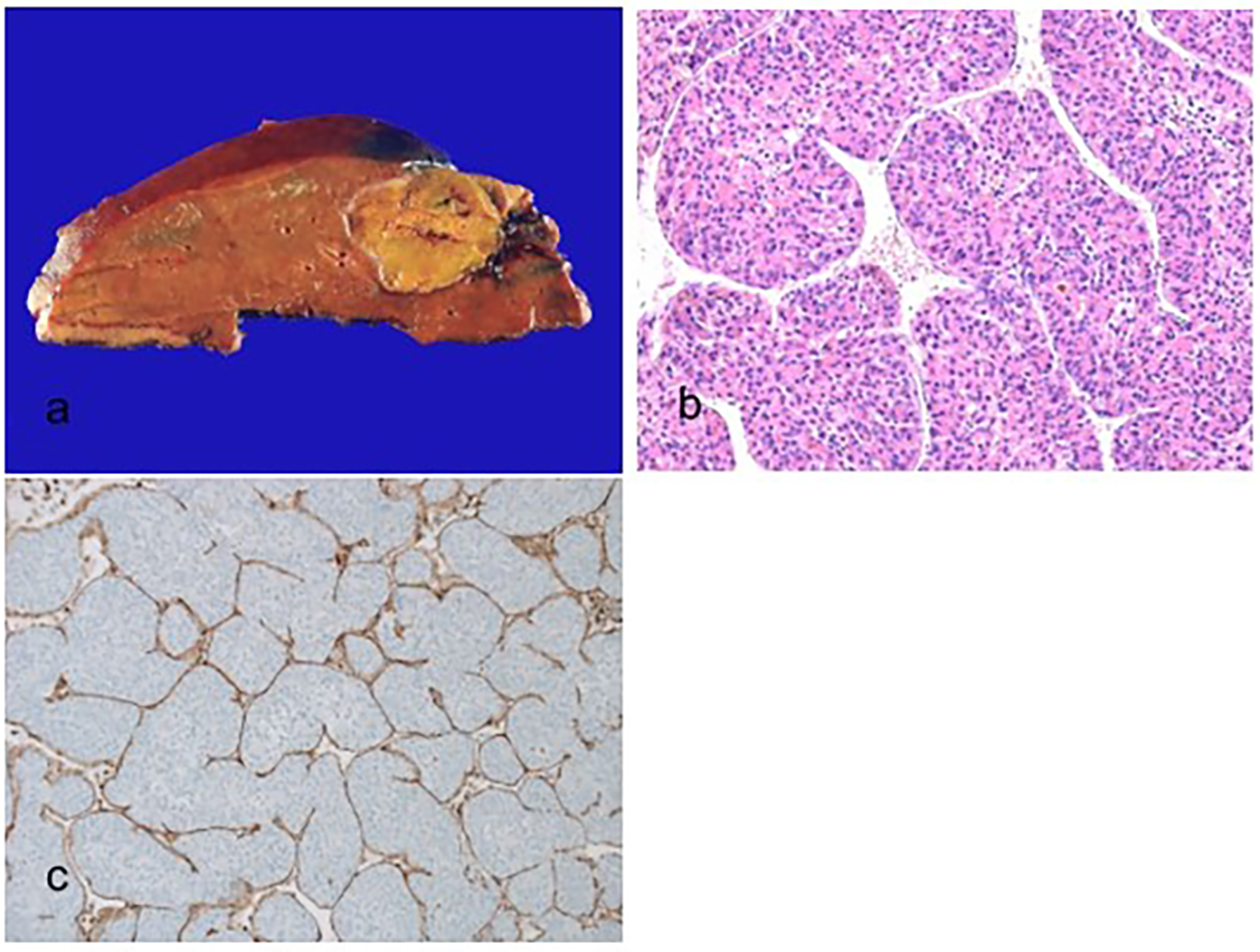
9.3. Macrotrabecular Massive Hepatocellular Carcinoma
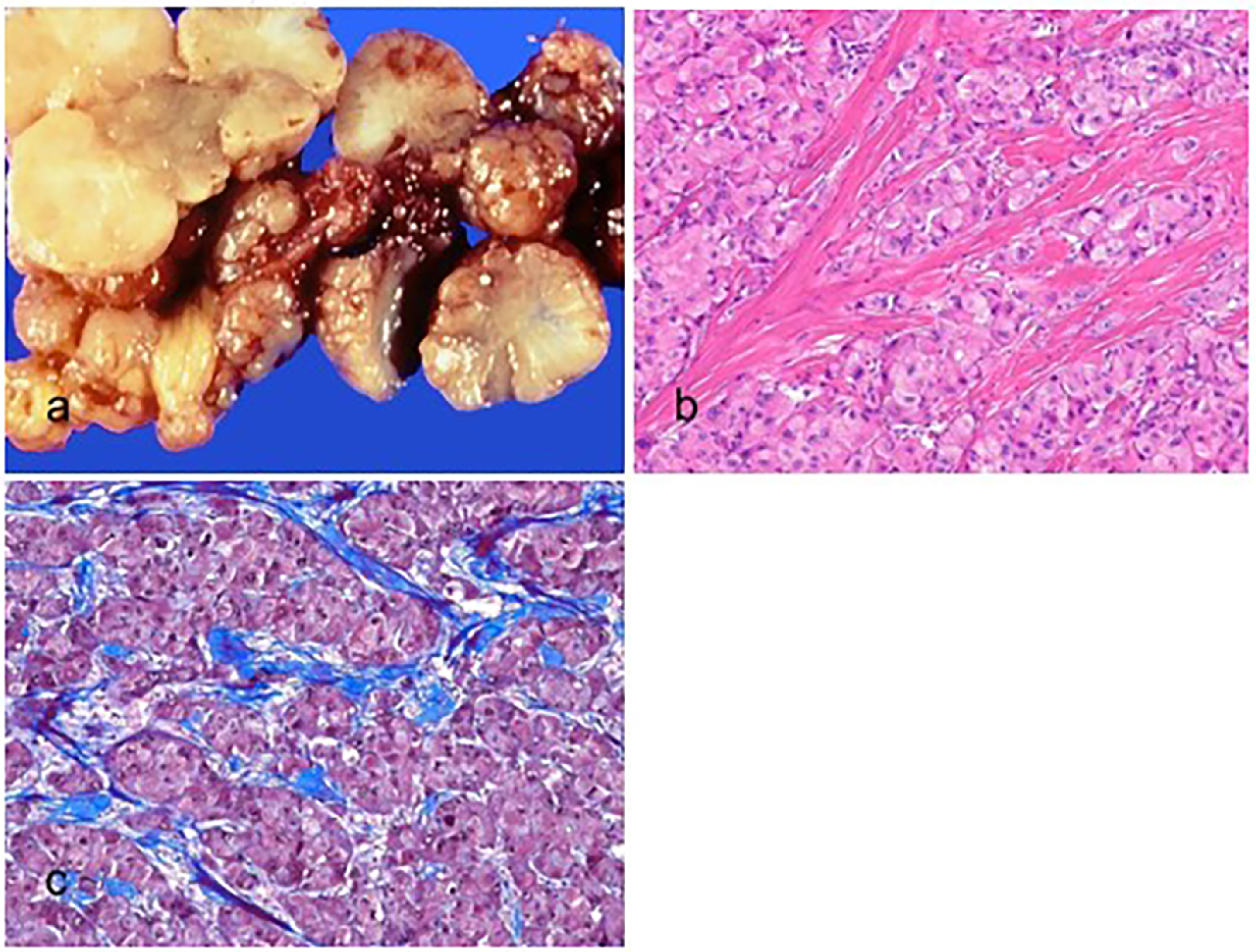
9.4. Scirrhous Hepatocellular Carcinoma
9.5. Chromophobe Hepatocellular Carcinoma
9.6. Fibrolamellar Carcinoma
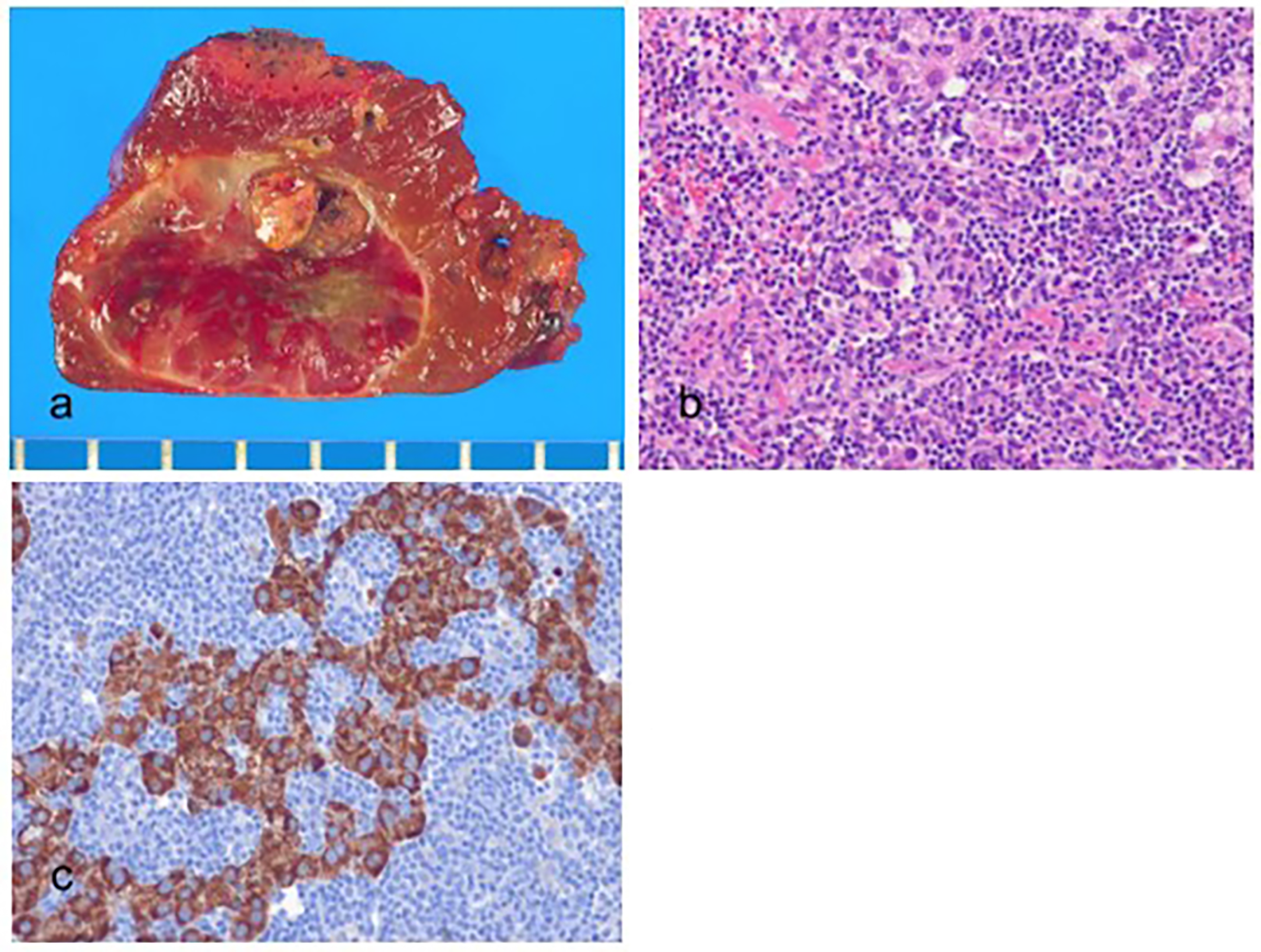
9.7. Neutrophil-Rich Hepatocellular Carcinoma
9.8. Lymphocyte-Rich Hepatocellular Carcinoma
10. New Provisional Subtypes of Hepatocellular Carcinoma Not Recognized in the 2019 WHO Classification
10.1. CTNNB1-Mutated Hepatocellular Carcinoma
10.2. Sarcomatoid Hepatocellular Carcinoma
10.3. Lipid-Rich Hepatocellular Carcinoma
10.4. Myxoid Hepatocellular Carcinoma
10.5. Hepatocellular Carcinoma with Syncytial Giant Cells
10.6. BAP1 Mutated and Protein Kinase A Activated Hepatocellular Carcinoma
10.7. Transitional Liver Cell Tumor
10.8. Cirrhotomimetic Hepatocellular Carcinoma
10.9. Progenitor Hepatocellular Carcinoma
11. Molecular and Immune Classes
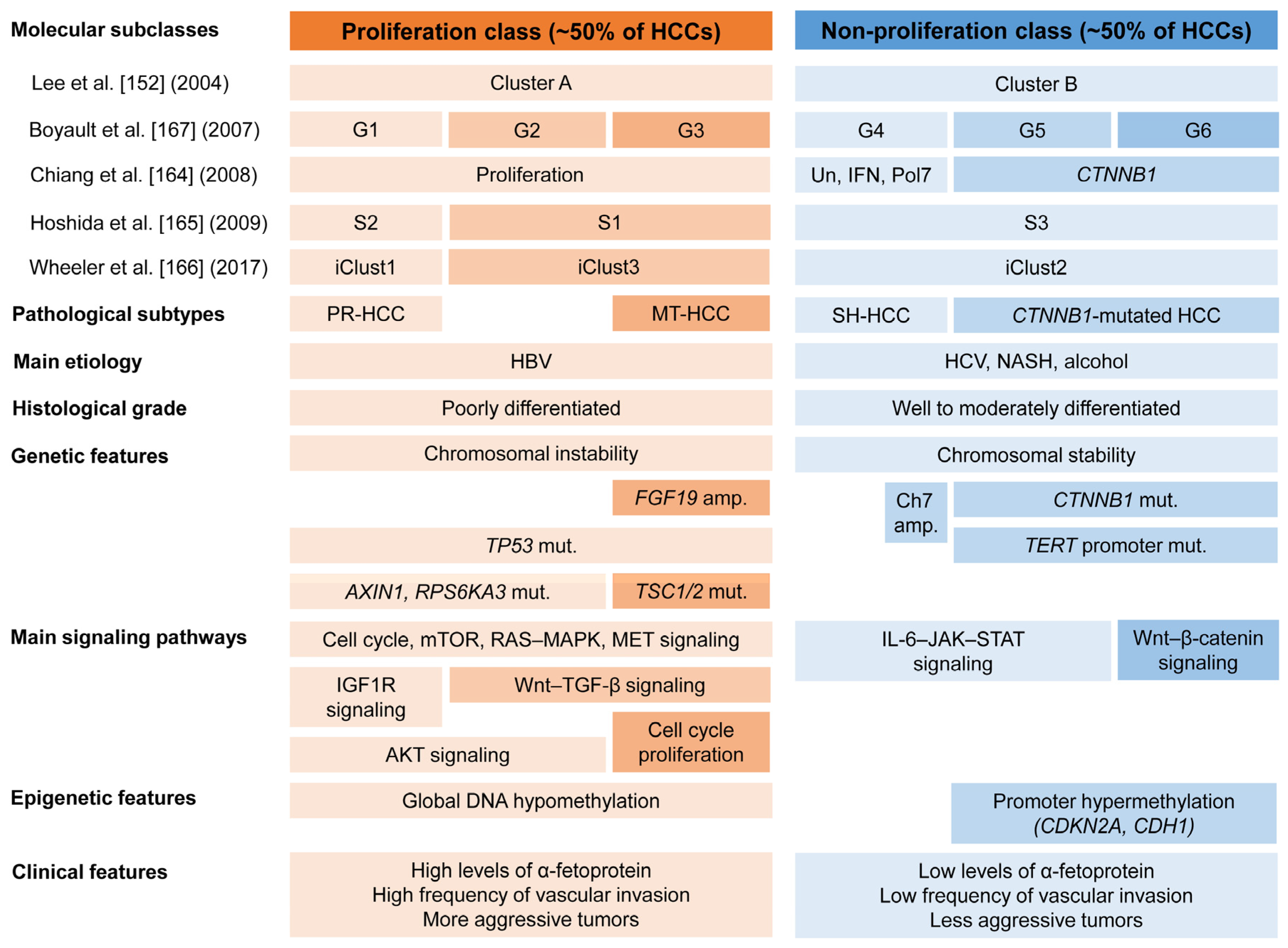
11.1. Molecular Classes
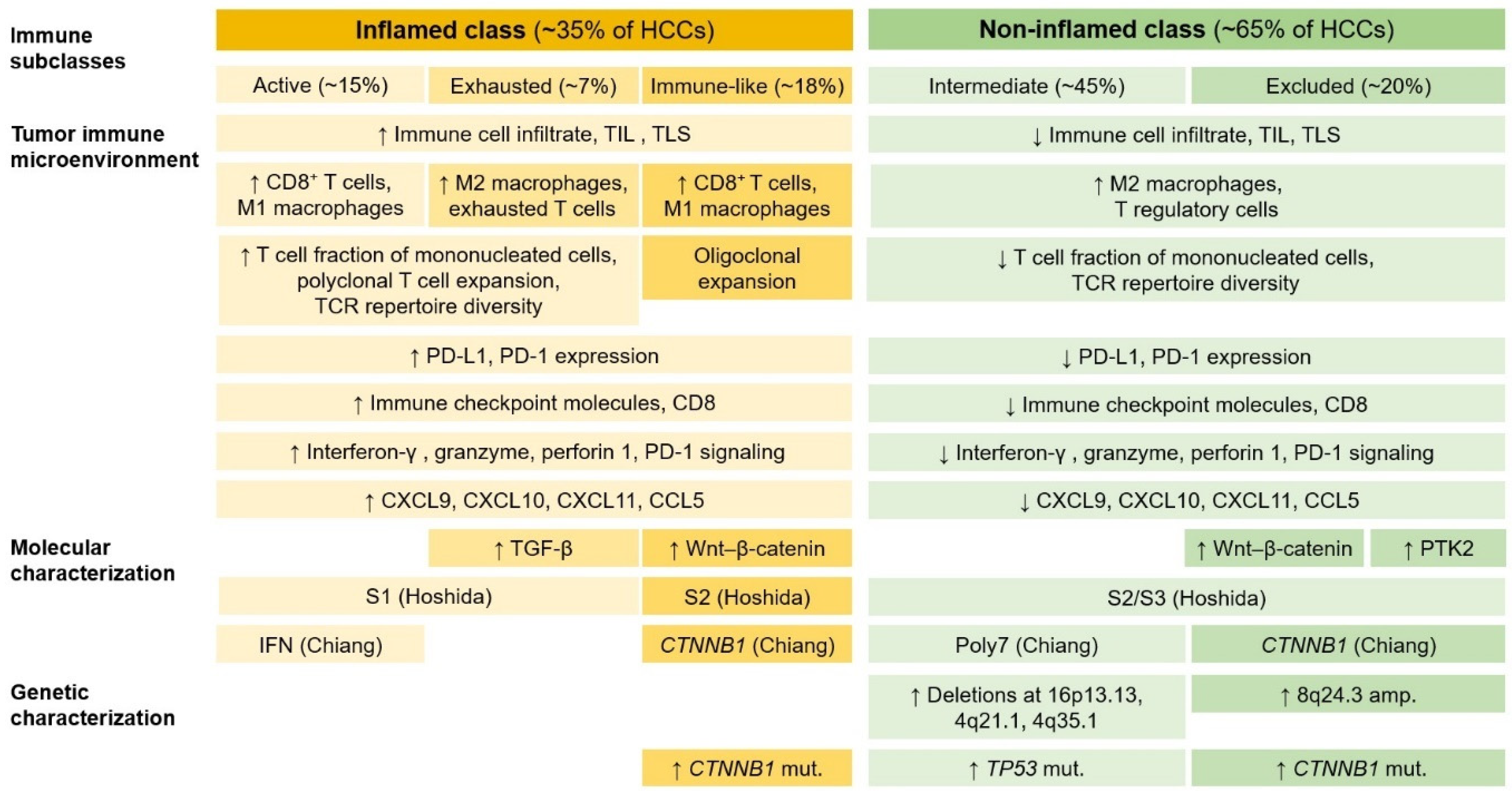
11.2. Immune Classes
12. Pathological Diagnostic Approach
12.1. Specimen Handling
12.1.1. Biopsy Specimens
12.1.2. Hepatectomy Specimens
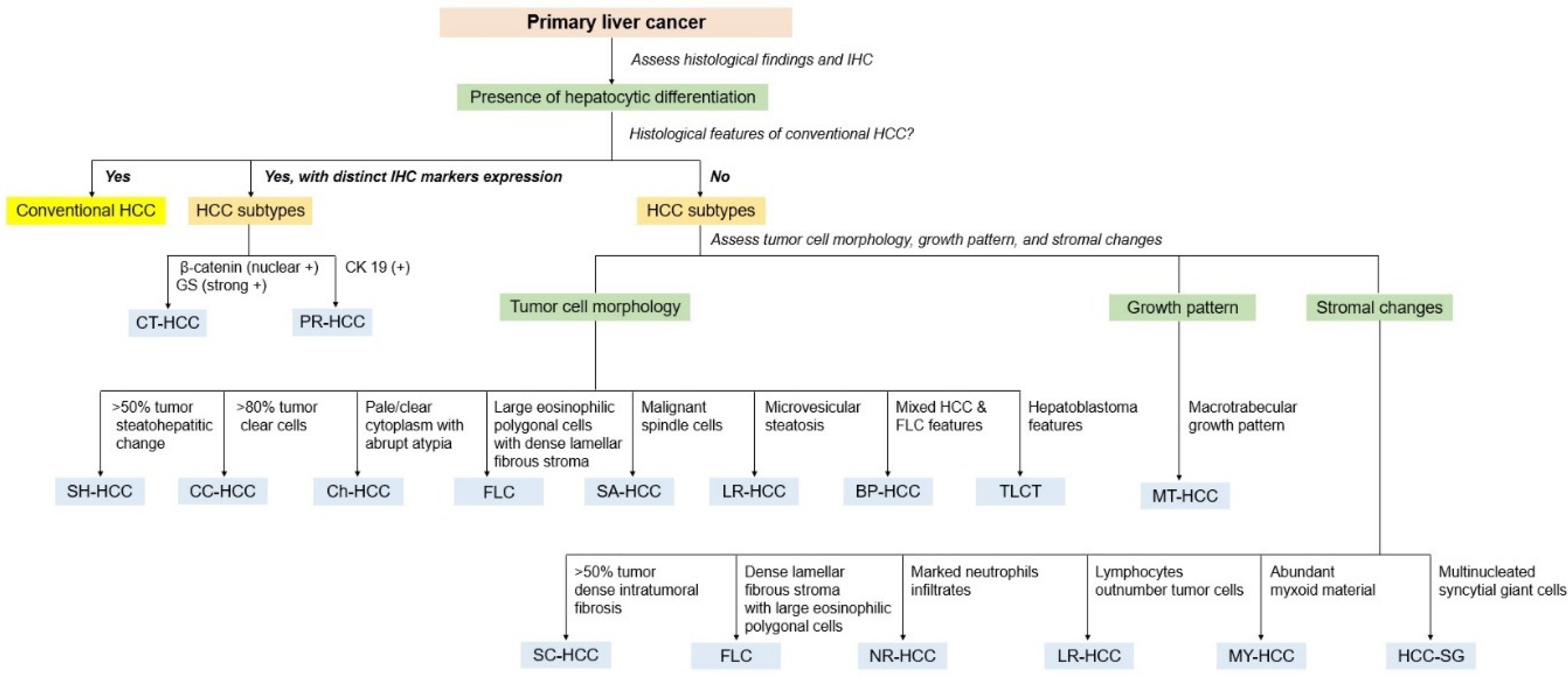
12.2. Pathological Diagnostic Approach
13. Non-Invasive Biomarkers
14. Future Perspectives
14.1. Treatment of Hepatocellular Carcinoma
14.2. Artificial Intelligence
15. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Torbenson, M.; Ng, I.O.; Park, Y.N.; Roncalli, M.; Sakamoto, M. Hepatocellular carcinoma. In WHO Classification of Tumours: Digestive System Tumours, 5th ed.; The WHO Classification of Tumours Editorial Board, Ed.; IARC Press: Lyon, France, 2019; pp. 229–239. ISBN 978-92-832-4499-8. [Google Scholar]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Ho, D.W.; Lo, R.C.; Chan, L.K.; Ng, I.O. Molecular pathogenesis of hepatocellular carcinoma. Liver Cancer 2016, 5, 290–302. [Google Scholar] [CrossRef] [PubMed]
- Schulze, K.; Imbeaud, S.; Letouzé, E.; Alexandrov, L.B.; Calderaro, J.; Rebouissou, S.; Couchy, G.; Meiller, C.; Shinde, J.; Soysouvanh, F.; et al. Exome sequencing of hepatocellular carcinomas identifies new mutational signatures and potential therapeutic targets. Nat. Genet. 2015, 47, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Sawey, E.T.; Chanrion, M.; Cai, C.; Wu, G.; Zhang, J.; Zender, L.; Zhao, A.; Busuttil, R.W.; Yee, H.; Stein, L.; et al. Identification of a therapeutic strategy targeting amplified FGF19 in liver cancer by oncogenomic screening. Cancer Cell 2011, 19, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Seshachalam, V.P.; Sekar, K.; Hui, K.M. Insights into the etiology-associated gene regulatory networks in hepatocellular carcinoma from The Cancer Genome Atlas. J. Gastroenterol. Hepatol. 2018, 33, 2037–2047. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, R.S.; Raza, A.; Propst, R.; Adeyi, O.; Bateman, J.; Sopha, S.C.; Shaw, J.; Auerbach, A. Recent advances in digestive tract tumors: Updates from the 5th edition of the World Health Organization “Blue Book”. Arch. Pathol. Lab. Med. 2021, 145, 607–626. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef]
- Akinyemiju, T.; Abera, S.; Ahmed, M.; Alam, N.; Alemayohu, M.A.; Allen, C.; Al-Raddadi, R.; Alvis-Guzman, N.; Amoako, Y.; Artaman, A.; et al. The burden of primary liver cancer and underlying etiologies from 1990 to 2015 at the global, regional, and national level: Results from the global burden of disease study 2015. JAMA Oncol. 2017, 3, 1683–1691. [Google Scholar] [CrossRef]
- Sanyal, A.J.; Yoon, S.K.; Lencioni, R. The etiology of hepatocellular carcinoma and consequences for treatment. Oncologist 2010, 15 (Suppl. S4), 14–22. [Google Scholar] [CrossRef]
- Wang, Q.; Luan, W.; Villanueva, G.A.; Rahbari, N.N.; Yee, H.T.; Manizate, F.; Hiotis, S.P. Clinical prognostic variables in young patients (under 40 years) with hepatitis B virus-associated hepatocellular carcinoma. J. Dig. Dis. 2012, 13, 214–218. [Google Scholar] [CrossRef]
- Raimondi, S.; Bruno, S.; Mondelli, M.U.; Maisonneuve, P. Hepatitis C virus genotype 1b as a risk factor for hepatocellular carcinoma development: A meta-analysis. J. Hepatol. 2009, 50, 1142–1154. [Google Scholar] [CrossRef] [PubMed]
- Kanwal, F.; Kramer, J.R.; Ilyas, J.; Duan, Z.; El-Serag, H.B. HCV genotype 3 is associated with an increased risk of cirrhosis and hepatocellular cancer in a national sample of U.S. Veterans with HCV. Hepatology 2014, 60, 98–105. [Google Scholar] [CrossRef]
- Schlesinger, S.; Aleksandrova, K.; Pischon, T.; Jenab, M.; Fedirko, V.; Trepo, E.; Overvad, K.; Roswall, N.; Tjønneland, A.; Boutron-Ruault, M.C.; et al. Diabetes mellitus, insulin treatment, diabetes duration, and risk of biliary tract cancer and hepatocellular carcinoma in a European cohort. Ann. Oncol. 2013, 24, 2449–2455. [Google Scholar] [CrossRef] [PubMed]
- Calle, E.E.; Rodriguez, C.; Walker-Thurmond, K.; Thun, M.J. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N. Engl. J. Med. 2003, 348, 1625–1638. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.J.; Yang, H.I.; Wu, H.C.; Lee, M.H.; Liu, J.; Wang, L.Y.; Lu, S.N.; Jen, C.L.; You, S.L.; Santella, R.M.; et al. Aflatoxin B1 exposure increases the risk of hepatocellular carcinoma associated with hepatitis C virus infection or alcohol consumption. Eur. J. Cancer 2018, 94, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Micchelli, S.T.; Vivekanandan, P.; Boitnott, J.K.; Pawlik, T.M.; Choti, M.A.; Torbenson, M. Malignant transformation of hepatic adenomas. Mod. Pathol. 2008, 21, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Kern, M.A.; Breuhahn, K.; Schirmacher, P. Molecular pathogenesis of human hepatocellular carcinoma. Adv. Cancer Res. 2002, 86, 67–112. [Google Scholar] [CrossRef]
- El-Serag, H.B.; Rudolph, K.L. Hepatocellular carcinoma: Epidemiology and molecular carcinogenesis. Gastroenterology 2007, 132, 2557–2576. [Google Scholar] [CrossRef]
- Farazi, P.A.; DePinho, R.A. Hepatocellular carcinoma pathogenesis: From genes to environment. Nat. Rev. Cancer 2006, 6, 674–687. [Google Scholar] [CrossRef]
- Bonilla Guerrero, R.; Roberts, L.R. The role of hepatitis B virus integrations in the pathogenesis of human hepatocellular carcinoma. J. Hepatol. 2005, 42, 760–777. [Google Scholar] [CrossRef]
- Hsu, I.C.; Metcalf, R.A.; Sun, T.; Welsh, J.A.; Wang, N.J.; Harris, C.C. Mutational hotspot in the p53 gene in human hepatocellular carcinomas. Nature 1991, 350, 427–428. [Google Scholar] [CrossRef] [PubMed]
- Bressac, B.; Kew, M.; Wands, J.; Ozturk, M. Selective G to T mutations of p53 gene in hepatocellular carcinoma from southern Africa. Nature 1991, 350, 429–431. [Google Scholar] [CrossRef] [PubMed]
- Lan, K.H.; Sheu, M.L.; Hwang, S.J.; Yen, S.H.; Chen, S.Y.; Wu, J.C.; Wang, Y.J.; Kato, N.; Omata, M.; Chang, F.Y.; et al. HCV NS5A interacts with p53 and inhibits p53-mediated apoptosis. Oncogene 2002, 21, 4801–4811. [Google Scholar] [CrossRef] [PubMed]
- Dubourdeau, M.; Miyamura, T.; Matsuura, Y.; Alric, L.; Pipy, B.; Rousseau, D. Infection of HepG2 cells with recombinant adenovirus encoding the HCV core protein induces p21WAF1 down-regulation—Effect of transforming growth factor β. J. Hepatol. 2002, 37, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Oikawa, T.; Ojima, H.; Yamasaki, S.; Takayama, T.; Hirohashi, S.; Sakamoto, M. Multistep and multicentric development of hepatocellular carcinoma: Histological analysis of 980 resected nodules. J. Hepatol. 2005, 42, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Ng, I.O.; Guan, X.Y.; Poon, R.T.; Fan, S.T.; Lee, J.M. Determination of the molecular relationship between multiple tumour nodules in hepatocellular carcinoma differentiates multicentric origin from intrahepatic metastasis. J. Pathol. 2003, 199, 345–353. [Google Scholar] [CrossRef]
- Renzulli, M.; Biselli, M.; Brocchi, S.; Granito, A.; Vasuri, F.; Tovoli, F.; Sessagesimi, E.; Piscaglia, F.; D’Errico, A.; Bolondi, L.; et al. New hallmark of hepatocellular carcinoma, early hepatocellular carcinoma and high-grade dysplastic nodules on Gd-EOB-DTPA MRI in patients with cirrhosis: A new diagnostic algorithm. Gut 2018, 67, 1674–1682. [Google Scholar] [CrossRef]
- Khemlina, G.; Ikeda, S.; Kurzrock, R. The biology of hepatocellular carcinoma: Implications for genomic and immune therapies. Mol. Cancer 2017, 16, 149. [Google Scholar] [CrossRef]
- Villanueva, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef]
- Llovet, J.M.; Montal, R.; Sia, D.; Finn, R.S. Molecular therapies and precision medicine for hepatocellular carcinoma. Nat. Rev. Clin. Oncol. 2018, 15, 599–616. [Google Scholar] [CrossRef]
- Llovet, J.M.; Pinyol, R.; Kelley, R.K.; El-Khoueiry, A.; Reeves, H.L.; Wang, X.W.; Gores, G.J.; Villanueva, A. Molecular pathogenesis and systemic therapies for hepatocellular carcinoma. Nat. Cancer 2022, 3, 386–401. [Google Scholar] [CrossRef] [PubMed]
- Marquardt, J.U.; Seo, D.; Andersen, J.B.; Gillen, M.C.; Kim, M.S.; Conner, E.A.; Galle, P.R.; Factor, V.M.; Park, Y.N.; Thorgeirsson, S.S. Sequential transcriptome analysis of human liver cancer indicates late stage acquisition of malignant traits. J. Hepatol. 2014, 60, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Nault, J.C.; Mallet, M.; Pilati, C.; Calderaro, J.; Bioulac-Sage, P.; Laurent, C.; Laurent, A.; Cherqui, D.; Balabaud, C.; Zucman-Rossi, J. High frequency of telomerase reverse-transcriptase promoter somatic mutations in hepatocellular carcinoma and preneoplastic lesions. Nat. Commun. 2013, 4, 2218. [Google Scholar] [CrossRef] [PubMed]
- Nault, J.C.; Calderaro, J.; Di Tommaso, L.; Balabaud, C.; Zafrani, E.S.; Bioulac-Sage, P.; Roncalli, M.; Zucman-Rossi, J. Telomerase reverse transcriptase promoter mutation is an early somatic genetic alteration in the transformation of premalignant nodules in hepatocellular carcinoma on cirrhosis. Hepatology 2014, 60, 1983–1992. [Google Scholar] [CrossRef] [PubMed]
- Lagana, S.M.; Salomao, M.; Remotti, H.E.; Knisely, A.S.; Moreira, R.K. Bile salt export pump: A sensitive and specific immunohistochemical marker of hepatocellular carcinoma. Histopathology 2015, 66, 598–602. [Google Scholar] [CrossRef]
- Kim, H.; Choi, G.H.; Na, D.C.; Ahn, E.Y.; Kim, G.I.; Lee, J.E.; Cho, J.Y.; Yoo, J.E.; Choi, J.S.; Park, Y.N. Human hepatocellular carcinomas with “Stemness”-related marker expression: Keratin 19 expression and a poor prognosis. Hepatology 2011, 54, 1707–1717. [Google Scholar] [CrossRef] [PubMed]
- Torbenson, M.; Zen, Y.; Yeh, M.M. Hepatocellular carcinoma. In Tumors of the Liver: AFIP Atlas of Tumor Pathology; Series 4, Fascicle 27; American Registry of Pathology: Washington, DC, USA, 2018; pp. 39–87. ISBN 978-1-9334477-41-1. [Google Scholar]
- Torbenson, M.S. Atlas of Liver Pathology: A Pattern-Based Approach; Wolters Kluwer: Philadelphia, PA, USA, 2020; pp. 363–402. ISBN 978-1-4963-9697-6. [Google Scholar]
- Torbenson, M.S. Hepatocellular pseudotumors and tumors. In Biopsy Interpretation of the Liver, 4th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2020; pp. 770–771. ISBN 978-1-975157-29-6. [Google Scholar]
- Collins, K.; Newcomb, P.H.; Cartun, R.W.; Ligato, S. Utility and limitations of albumin mRNA in situ hybridization detection in the diagnosis of hepatobiliary lesions and metastatic carcinoma to the liver. Appl. Immunohistochem. Mol. Morphol. 2021, 29, 180–187. [Google Scholar] [CrossRef]
- Cai, M.Y.; Tong, Z.T.; Zheng, F.; Liao, Y.J.; Wang, Y.; Rao, H.L.; Chen, Y.C.; Wu, Q.L.; Liu, Y.H.; Guan, X.Y.; et al. EZH2 protein: A promising immunomarker for the detection of hepatocellular carcinomas in liver needle biopsies. Gut 2011, 60, 967–976. [Google Scholar] [CrossRef]
- Hajósi-Kalcakosz, S.; Dezső, K.; Bugyik, E.; Bödör, C.; Paku, S.; Pávai, Z.; Halász, J.; Schlachter, K.; Schaff, Z.; Nagy, P. Enhancer of zeste homologue 2 (EZH2) is a reliable immunohistochemical marker to differentiate malignant and benign hepatic tumors. Diagn. Pathol. 2012, 7, 86. [Google Scholar] [CrossRef]
- Ferrone, C.R.; Ting, D.T.; Shahid, M.; Konstantinidis, I.T.; Sabbatino, F.; Goyal, L.; Rice-Stitt, T.; Mubeen, A.; Arora, K.; Bardeesey, N.; et al. The ability to diagnose intrahepatic cholangiocarcinoma definitively using novel branched DNA-enhanced albumin RNA in situ hybridization technology. Ann. Surg. Oncol. 2016, 23, 290–296. [Google Scholar] [CrossRef]
- Rhee, H.; Chung, T.; Yoo, J.E.; Nahm, J.H.; Woo, H.Y.; Choi, G.H.; Han, D.H.; Park, Y.N. Gross type of hepatocellular carcinoma reflects the tumor hypoxia, fibrosis, and stemness-related marker expression. Hepatol. Int. 2020, 14, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Edmondson, H.A.; Steiner, P.E. Primary carcinoma of the liver: A study of 100 cases among 48,900 necropsies. Cancer 1954, 7, 462–503. [Google Scholar] [CrossRef] [PubMed]
- Nzeako, U.C.; Goodman, Z.D.; Ishak, K.G. Comparison of tumor pathology with duration of survival of North American patients with hepatocellular carcinoma. Cancer 1995, 76, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Burt, A.D.; Alves, V.; Bedossa, P.; Clouston, A.; Guido, M.; Hübscher, S.; Kakar, S.; Ng, I.; Park, Y.N.; Reeves, H.; et al. Data set for the reporting of intrahepatic cholangiocarcinoma, perihilar cholangiocarcinoma and hepatocellular carcinoma: Recommendations from the International Collaboration on Cancer Reporting (ICCR). Histopathology 2018, 73, 369–385. [Google Scholar] [CrossRef] [PubMed]
- Han, D.H.; Choi, G.H.; Kim, K.S.; Choi, J.S.; Park, Y.N.; Kim, S.U.; Park, J.Y.; Ahn, S.H.; Han, K.H. Prognostic significance of the worst grade in hepatocellular carcinoma with heterogeneous histologic grades of differentiation. J. Gastroenterol. Hepatol. 2013, 28, 1384–1390. [Google Scholar] [CrossRef] [PubMed]
- Salomao, M.; Remotti, H.; Vaughan, R.; Siegel, A.B.; Lefkowitch, J.H.; Moreira, R.K. The steatohepatitic variant of hepatocellular carcinoma and its association with underlying steatohepatitis. Hum. Pathol. 2012, 43, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Qin, J.; Higashi, T.; Nakagawa, S.; Fujiwara, N.; Yamashita, Y.I.; Beppu, T.; Baba, H.; Kobayashi, M.; Kumada, H.; Gunasekaran, G.; et al. Steatohepatitic variant of hepatocellular carcinoma is associated with both alcoholic steatohepatitis and nonalcoholic steatohepatitis: A study of 2 cohorts with molecular insights. Am. J. Surg. Pathol. 2020, 44, 1406–1412. [Google Scholar] [CrossRef]
- Yeh, M.M.; Liu, Y.; Torbenson, M. Steatohepatitic variant of hepatocellular carcinoma in the absence of metabolic syndrome or background steatosis: A clinical, pathological, and genetic study. Hum. Pathol. 2015, 46, 1769–1775. [Google Scholar] [CrossRef]
- Shibahara, J.; Ando, S.; Sakamoto, Y.; Kokudo, N.; Fukayama, M. Hepatocellular carcinoma with steatohepatitic features: A clinicopathological study of Japanese patients. Histopathology 2014, 64, 951–962. [Google Scholar] [CrossRef]
- Jain, D.; Nayak, N.C.; Kumaran, V.; Saigal, S. Steatohepatitic hepatocellular carcinoma, a morphologic indicator of associated metabolic risk factors: A study from India. Arch. Pathol. Lab. Med. 2013, 137, 961–966. [Google Scholar] [CrossRef]
- Salomao, M.; Yu, W.M.; Brown, R.S., Jr.; Emond, J.C.; Lefkowitch, J.H. Steatohepatitic hepatocellular carcinoma (SH-HCC): A distinctive histological variant of HCC in hepatitis C virus-related cirrhosis with associated NAFLD/NASH. Am. J. Surg. Pathol. 2010, 34, 1630–1636. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Shin, D.H.; Park, W.Y.; Shin, N.; Kim, A.; Lee, H.J.; Kim, Y.K.; Choi, K.U.; Kim, J.Y.; Yang, Y.I.; et al. IDH1 R132C mutation is detected in clear cell hepatocellular carcinoma by pyrosequencing. World J. Surg. Oncol. 2017, 15, 82. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Fan, J.; Qin, L.X.; Zhou, J.; Sun, H.C.; Qiu, S.J.; Ye, Q.H.; Wang, L.; Tang, Z.Y. Risk factors, prognosis, and management of early and late intrahepatic recurrence after resection of primary clear cell carcinoma of the liver. Ann. Surg. Oncol. 2011, 18, 1955–1963. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Ge, P.; Liao, W.; Ren, J.; Yang, H.; Xu, H.; Sang, X.; Lu, X.; Zhong, S.; Mao, Y. Edmondson grade predicts survival of patients with primary clear cell carcinoma of liver after curative resection: A retrospective study with long-term follow-up. Asia Pac. J. Clin. Oncol. 2017, 13, e312–e320. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Ma, W.; Li, H.; Li, Q. Clinicopathological and prognostic features of primary clear cell carcinoma of the liver. Hepatol. Res. 2008, 38, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.H.; Watanabe, J.; Nakashima, O.; Kojiro, M. Clinicopathologic study on clear cell hepatocellular carcinoma. Pathol. Int. 1996, 46, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Murakata, L.A.; Ishak, K.G.; Nzeako, U.C. Clear cell carcinoma of the liver: A comparative immunohistochemical study with renal clear cell carcinoma. Mod. Pathol. 2000, 13, 874–881. [Google Scholar] [CrossRef] [PubMed]
- Ziol, M.; Poté, N.; Amaddeo, G.; Laurent, A.; Nault, J.C.; Oberti, F.; Costentin, C.; Michalak, S.; Bouattour, M.; Francoz, C.; et al. Macrotrabecular-massive hepatocellular carcinoma: A distinctive histological subtype with clinical relevance. Hepatology 2018, 68, 103–112. [Google Scholar] [CrossRef]
- Renne, S.L.; Woo, H.Y.; Allegra, S.; Rudini, N.; Yano, H.; Donadon, M.; Viganò, L.; Akiba, J.; Lee, H.S.; Rhee, H.; et al. Vessels encapsulating tumor clusters (VETC) is a powerful predictor of aggressive hepatocellular carcinoma. Hepatology 2020, 71, 183–195. [Google Scholar] [CrossRef]
- Calderaro, J.; Meunier, L.; Nguyen, C.T.; Boubaya, M.; Caruso, S.; Luciani, A.; Amaddeo, G.; Regnault, H.; Nault, J.C.; Cohen, J.; et al. ESM1 as a marker of macrotrabecular-massive hepatocellular carcinoma. Clin. Cancer Res. 2019, 25, 5859–5865. [Google Scholar] [CrossRef]
- Fujii, T.; Zen, Y.; Harada, K.; Niwa, H.; Masuda, S.; Kaizaki, Y.; Watanabe, K.; Kawashima, A.; Nakanuma, Y. Participation of liver cancer stem/progenitor cells in tumorigenesis of scirrhous hepatocellular carcinoma—Human and cell culture study. Hum. Pathol. 2008, 39, 1185–1196. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Choi, M.S.; Gwak, G.Y.; Lee, J.H.; Koh, K.C.; Paik, S.W.; Yoo, B.C.; Choi, D.; Park, C.K. Clinicopathologic characteristics and long-term prognosis of scirrhous hepatocellular carcinoma. Dig. Dis. Sci. 2012, 57, 1698–1707. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.J.; Rhee, H.; Yoo, J.E.; Ko, J.E.; Lee, J.S.; Kim, H.; Choi, J.S.; Park, Y.N. Increased expression of CCN2, epithelial membrane antigen, and fibroblast activation protein in hepatocellular carcinoma with fibrous stroma showing aggressive behavior. PLoS ONE 2014, 9, e105094. [Google Scholar] [CrossRef] [PubMed]
- Seok, J.Y.; Na, D.C.; Woo, H.G.; Roncalli, M.; Kwon, S.M.; Yoo, J.E.; Ahn, E.Y.; Kim, G.I.; Choi, J.S.; Kim, Y.B.; et al. A fibrous stromal component in hepatocellular carcinoma reveals a cholangiocarcinoma-like gene expression trait and epithelial-mesenchymal transition. Hepatology 2012, 55, 1776–1786. [Google Scholar] [CrossRef] [PubMed]
- Kurogi, M.; Nakashima, O.; Miyaaki, H.; Fujimoto, M.; Kojiro, M. Clinicopathological study of scirrhous hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2006, 21, 1470–1477. [Google Scholar] [CrossRef] [PubMed]
- Krings, G.; Ramachandran, R.; Jain, D.; Wu, T.T.; Yeh, M.M.; Torbenson, M.; Kakar, S. Immunohistochemical pitfalls and the importance of glypican 3 and arginase in the diagnosis of scirrhous hepatocellular carcinoma. Mod. Pathol. 2013, 26, 782–791. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, S.; Aishima, S.; Taguchi, K.; Asayama, Y.; Terashi, T.; Honda, H.; Tsuneyoshi, M. ‘Scirrhous’ type hepatocellular carcinomas: A special reference to expression of cytokeratin 7 and hepatocyte paraffin 1. Histopathology 2005, 47, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Limaiem, F.; Bouraoui, S.; Sboui, M.; Bouslama, S.; Lahmar, A.; Mzabi, S. Fibrolamellar carcinoma versus scirrhous hepatocellular carcinoma: Diagnostic usefulness of CD68. Acta Gastroenterol. Belg. 2015, 78, 393–398. [Google Scholar]
- Hatano, M.; Ojima, H.; Masugi, Y.; Tsujikawa, H.; Hiraoka, N.; Kanai, Y.; Shimada, K.; Shinoda, M.; Sakamoto, M. Steatotic and nonsteatotic scirrhous hepatocellular carcinomas reveal distinct clinicopathological features. Hum. Pathol. 2019, 86, 222–232. [Google Scholar] [CrossRef]
- Wood, L.D.; Heaphy, C.M.; Daniel, H.D.; Naini, B.V.; Lassman, C.R.; Arroyo, M.R.; Kamel, I.R.; Cosgrove, D.P.; Boitnott, J.K.; Meeker, A.K.; et al. Chromophobe hepatocellular carcinoma with abrupt anaplasia: A proposal for a new subtype of hepatocellular carcinoma with unique morphological and molecular features. Mod. Pathol. 2013, 26, 1586–1593. [Google Scholar] [CrossRef]
- Torbenson, M. Fibrolamellar carcinoma: 2012 update. Scientifica 2012, 2012, 743790. [Google Scholar] [CrossRef]
- Darcy, D.G.; Malek, M.M.; Kobos, R.; Klimstra, D.S.; DeMatteo, R.; La Quaglia, M.P. Prognostic factors in fibrolamellar hepatocellular carcinoma in young people. J. Pediatr. Surg. 2015, 50, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Graham, R.P.; Lackner, C.; Terracciano, L.; González-Cantú, Y.; Maleszewski, J.J.; Greipp, P.T.; Simon, S.M.; Torbenson, M.S. Fibrolamellar carcinoma in the Carney complex: PRKAR1A loss instead of the classic DNAJB1-PRKACA fusion. Hepatology 2018, 68, 1441–1447. [Google Scholar] [CrossRef] [PubMed]
- LeBrun, D.P.; Silver, M.M.; Freedman, M.H.; Phillips, M.J. Fibrolamellar carcinoma of the liver in a patient with Fanconi anemia. Hum. Pathol. 1991, 22, 396–398. [Google Scholar] [CrossRef] [PubMed]
- Terracciano, L.M.; Tornillo, L.; Avoledo, P.; Von Schweinitz, D.; Kühne, T.; Bruder, E. Fibrolamellar hepatocellular carcinoma occurring 5 years after hepatocellular adenoma in a 14-year-old girl: A case report with comparative genomic hybridization analysis. Arch. Pathol. Lab. Med. 2004, 128, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Kakar, S.; Burgart, L.J.; Batts, K.P.; Garcia, J.; Jain, D.; Ferrell, L.D. Clinicopathologic features and survival in fibrolamellar carcinoma: Comparison with conventional hepatocellular carcinoma with and without cirrhosis. Mod. Pathol. 2005, 18, 1417–1423. [Google Scholar] [CrossRef] [PubMed]
- Njei, B.; Konjeti, V.R.; Ditah, I. Prognosis of patients with fibrolamellar hepatocellular carcinoma versus conventional hepatocellular carcinoma: A systematic review and meta-analysis. Gastrointest. Cancer Res. 2014, 7, 49–54. [Google Scholar] [PubMed]
- Graham, R.P.; Yeh, M.M.; Lam-Himlin, D.; Roberts, L.R.; Terracciano, L.; Cruise, M.W.; Greipp, P.T.; Zreik, R.T.; Jain, D.; Zaid, N.; et al. Molecular testing for the clinical diagnosis of fibrolamellar carcinoma. Mod. Pathol. 2018, 31, 141–149. [Google Scholar] [CrossRef]
- Yamamoto, S.; Takashima, S.; Ogawa, H.; Kuroda, T.; Yamamoto, M.; Takeda, A.; Nakmaura, H. Granulocyte-colony-stimulating-factor-producing hepatocellular carcinoma. J. Gastroenterol. 1999, 34, 640–644. [Google Scholar] [CrossRef]
- Aita, K.; Seki, K. Carcinosarcoma of the liver producing granulocyte-colony stimulating factor. Pathol. Int. 2006, 56, 413–419. [Google Scholar] [CrossRef]
- Kohno, M.; Shirabe, K.; Mano, Y.; Muto, J.; Motomura, T.; Takeishi, K.; Toshima, T.; Yoshimatsu, M.; Ijichi, H.; Harada, N.; et al. Granulocyte colony-stimulating-factor-producing hepatocellular carcinoma with extensive sarcomatous changes: Report of a case. Surg. Today 2013, 43, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Araki, K.; Kishihara, F.; Takahashi, K.; Matsumata, T.; Shimura, T.; Suehiro, T.; Kuwanom, H. Hepatocellular carcinoma producing a granulocyte colony-stimulating factor: Report of a resected case with a literature review. Liver Int. 2007, 27, 716–721. [Google Scholar] [CrossRef]
- Amano, H.; Itamoto, T.; Emoto, K.; Hino, H.; Asahara, T.; Shimamoto, F. Granulocyte colony-stimulating factor-producing combined hepatocellular/cholangiocellular carcinoma with sarcomatous change. J. Gastroenterol. 2005, 40, 1158–1159. [Google Scholar] [CrossRef] [PubMed]
- Joshita, S.; Nakazawa, K.; Koike, S.; Kamijo, A.; Matsubayashi, K.; Miyabayashi, H.; Furuta, K.; Kitano, K.; Yoshizawa, K.; Tanaka, E. A case of granulocyte-colony stimulating factor-producing hepatocellular carcinoma confirmed by immunohistochemistry. J. Korean Med. Sci. 2010, 25, 476–480. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.; Tong, J.H.; Pan, Y.; Chan, S.L.; Wong, G.L.; Wong, V.W.; Lai, P.B.; To, K.F. Lymphoepithelioma-like hepatocellular carcinoma: An uncommon variant of hepatocellular carcinoma with favorable outcome. Am. J. Surg. Pathol. 2015, 39, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.R.; Liu, T.C.; Vaccharajani, N.; Chapman, W.C.; Brunt, E.M. Characterization of inflammatory (lymphoepithelioma-like) hepatocellular carcinoma: A study of 8 cases. Arch. Pathol. Lab. Med. 2014, 138, 1193–1202. [Google Scholar] [CrossRef]
- Chan, A.W.; Zhang, Z.; Chong, C.C.; Tin, E.K.; Chow, C.; Wong, N. Genomic landscape of lymphoepithelioma-like hepatocellular carcinoma. J. Pathol. 2019, 249, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.R.; Leow, W.Q.; Lo, R.; Mendoza, P.G.L.; Chan, A.W.H. Atlas of Hepatocellular Carcinoma Pathology; Springer: New York, NY, USA, 2022; pp. 51–55. ISBN 978-981-16-8499-9. [Google Scholar]
- Calderaro, J.; Couchy, G.; Imbeaud, S.; Amaddeo, G.; Letouzé, E.; Blanc, J.F.; Laurent, C.; Hajji, Y.; Azoulay, D.; Bioulac-Sage, P.; et al. Histological subtypes of hepatocellular carcinoma are related to gene mutations and molecular tumour classification. J. Hepatol. 2017, 67, 727–738. [Google Scholar] [CrossRef]
- Ando, S.; Shibahara, J.; Hayashi, A.; Fukayama, M. β-catenin alteration is rare in hepatocellular carcinoma with steatohepatitic features: Immunohistochemical and mutational study. Virchows Arch. 2015, 467, 535–542. [Google Scholar] [CrossRef]
- Vyas, M.; Jain, D. An update on subtypes of hepatocellular carcinoma: From morphology to molecular. Indian J. Pathol. Microbiol. 2021, 64, S112–S120. [Google Scholar] [CrossRef]
- Torbenson, M.S. Morphologic subtypes of hepatocellular carcinoma. Gastroenterol. Clin. N. Am. 2017, 46, 365–391. [Google Scholar] [CrossRef] [PubMed]
- Fan, Z.; van de Rijn, M.; Montgomery, K.; Rouse, R.V. Hep Par 1 antibody stain for the differential diagnosis of hepatocellular carcinoma: 676 tumors tested using tissue microarrays and conventional tissue sections. Mod. Pathol. 2003, 16, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Kishi, K.; Shikata, T.; Hirohashi, S.; Hasegawa, H.; Yamazaki, S.; Makuuchi, M. Hepatocellular carcinoma. A clinical and pathologic analysis of 57 hepatectomy cases. Cancer 1983, 51, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Ishak, K.; Goodman, Z.D.; Stocker, J.T. Tumors of the Liver and Intrahepatic Bile Ducts: Atlas of Tumor Pathology (AFIP); 3rd Series; Armed Forces Institute of Pathology: Washington, DC, USA, 1999; Volume 31, pp. 212–213. ISBN 1-881041-69-7. [Google Scholar]
- Mounajjed, T.; Chandan, V.S.; Torbenson, M.S. Surgical Pathology of Liver Tumors; Springer: New York, NY, USA, 2015; pp. 174–177. ISBN 978-3-319-16088-7. [Google Scholar]
- Calderaro, J.; Ziol, M.; Paradis, V.; Zucman-Rossi, J. Molecular and histological correlations in liver cancer. J. Hepatol. 2019, 71, 616–630. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.U.; Kang, H.J. Recent updates on the classification of hepatoblastoma according to the International Pediatric Liver Tumors Consensus. J. Liver Cancer 2022, 22, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Dehner, L.P.; Manivel, J.C. Hepatoblastoma: An analysis of the relationship between morphologic subtypes and prognosis. Am. J. Pediatr. Hematol. Oncol. 1988, 10, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Saxena, R.; Quaglia, A. Hepatoblastoma. In WHO Classification of Tumours: Digestive System Tumours, 5th ed.; The WHO Classification of Tumours Editorial Board, Ed.; IARC Press: Lyon, France, 2019; pp. 240–244. ISBN 978-92-832-4499-8. [Google Scholar]
- Torbenson, M.S. Hepatocellular carcinoma: Making sense of morphological heterogeneity, growth patterns, and subtypes. Hum. Pathol. 2021, 112, 86–101. [Google Scholar] [CrossRef] [PubMed]
- Ross, H.M.; Daniel, H.D.; Vivekanandan, P.; Kannangai, R.; Yeh, M.M.; Wu, T.T.; Makhlouf, H.R.; Torbenson, M. Fibrolamellar carcinomas are positive for CD68. Mod. Pathol. 2011, 24, 390–395. [Google Scholar] [CrossRef]
- Graham, R.P.; Jin, L.; Knutson, D.L.; Kloft-Nelson, S.M.; Greipp, P.T.; Waldburger, N.; Roessler, S.; Longerich, T.; Roberts, L.R.; Oliveira, A.M.; et al. DNAJB1-PRKACA is specific for fibrolamellar carcinoma. Mod. Pathol. 2015, 28, 822–829. [Google Scholar] [CrossRef]
- Heaphy, C.M.; Subhawong, A.P.; Hong, S.M.; Goggins, M.G.; Montgomery, E.A.; Gabrielson, E.; Netto, G.J.; Epstein, J.I.; Lotan, T.L.; Westra, W.H.; et al. Prevalence of the alternative lengthening of telomeres telomere maintenance mechanism in human cancer subtypes. Am. J. Pathol. 2011, 179, 1608–1615. [Google Scholar] [CrossRef]
- Meeker, A.K.; Gage, W.R.; Hicks, J.L.; Simon, I.; Coffman, J.R.; Platz, E.A.; March, G.E.; De Marzo, A.M. Telomere length assessment in human archival tissues: Combined telomere fluorescence in situ hybridization and immunostaining. Am. J. Pathol. 2002, 160, 1259–1268. [Google Scholar] [CrossRef] [PubMed]
- Graham, R.P.; Terracciano, L.M.; Meves, A.; Vanderboom, P.M.; Dasari, S.; Yeh, M.M.; Torbenson, M.S.; Cruise, M.W. Hepatic adenomas with synchronous or metachronous fibrolamellar carcinomas: Both are characterized by LFABP loss. Mod. Pathol. 2016, 29, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Goodman, Z.D.; Ishak, K.G.; Langloss, J.M.; Sesterhenn, I.A.; Rabin, L. Combined hepatocellular-cholangiocarcinoma. A histologic and immunohistochemical study. Cancer 1985, 55, 124–135. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, M.; Akiba, J.; Kawaguchi, T.; Niizeki, T.; Arinaga-Hino, T.; Sata, M.; Nakashima, O.; Yano, H.; Kage, M. Intrahepatic cholangiocarcinoma with sarcomatous change producing granulocyte-colony stimulating factor. Pathol. Int. 2013, 63, 233–235. [Google Scholar] [CrossRef] [PubMed]
- Shimakawa, T.; Asaka, S.; Usuda, A.; Yamaguchi, K.; Yoshimatsu, K.; Shiozawa, S.; Katsube, T.; Naritaka, Y. Granulocyte-colony stimulating factor (G-CSF)-producing esophageal squamous cell carcinoma: A case report. Int. Surg. 2014, 99, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Calderaro, J.; Rousseau, B.; Amaddeo, G.; Mercey, M.; Charpy, C.; Costentin, C.; Luciani, A.; Zafrani, E.S.; Laurent, A.; Azoulay, D.; et al. Programmed death ligand 1 expression in hepatocellular carcinoma: Relationship with clinical and pathological features. Hepatology 2016, 64, 2038–2046. [Google Scholar] [CrossRef] [PubMed]
- Kitao, A.; Matsui, O.; Yoneda, N.; Kozaka, K.; Kobayashi, S.; Sanada, J.; Koda, W.; Minami, T.; Inoue, D.; Yoshida, K.; et al. Hepatocellular carcinoma with β-catenin mutation: Imaging and pathologic characteristics. Radiology 2015, 275, 708–717. [Google Scholar] [CrossRef]
- Dal Bello, B.; Rosa, L.; Campanini, N.; Tinelli, C.; Torello Viera, F.; D’Ambrosio, G.; Rossi, S.; Silini, E.M. Glutamine synthetase immunostaining correlates with pathologic features of hepatocellular carcinoma and better survival after radiofrequency thermal ablation. Clin. Cancer Res. 2010, 16, 2157–2166. [Google Scholar] [CrossRef]
- Torbenson, M.; McCabe, C.E.; O’Brien, D.R.; Yin, J.; Bainter, T.; Tran, N.H.; Yasir, S.; Chen, Z.E.; Dhanasekaran, R.; Ahn, K.S.; et al. Morphological heterogeneity in beta-catenin-mutated hepatocellular carcinomas: Implications for tumor molecular classification. Hum. Pathol. 2022, 119, 15–27. [Google Scholar] [CrossRef]
- Audard, V.; Grimber, G.; Elie, C.; Radenen, B.; Audebourg, A.; Letourneur, F.; Soubrane, O.; Vacher-Lavenu, M.C.; Perret, C.; Cavard, C.; et al. Cholestasis is a marker for hepatocellular cacinomas displaying beta-catenin mutations. J. Pathol. 2007, 212, 345–352. [Google Scholar] [CrossRef]
- Nishi, H.; Taguchi, K.; Asayama, Y.; Aishima, S.; Sugimachi, K.; Nawata, H.; Tsuneyoshi, M. Sarcomatous hepatocellular carcinoma: A special reference to ordinary hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2003, 18, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Theise, N.D.; Curado, M.P.; Franceschi, S.; Hytiroglou, P.; Kudo, M.; Park, Y.N.; Sakamoto, M.; Torbenson, M.; Wee, A. Hepatocellular carcinoma. In WHO Classification of Tumours of Digestive System, 4th ed.; Bosman, F.T., Carneiro, F., Hruban, R.H., Theise, N.D., Eds.; IARC Press: Lyon, France, 2010; pp. 205–216. ISBN 978-92-832-4499-8. [Google Scholar]
- Orikasa, H.; Ohyama, R.; Tsuka, N.; Eyden, B.P.; Yamazaki, K. Lipid-rich clear-cell hepatocellular carcinoma arising in non-alcoholic steatohepatitis in a patient with diabetes mellitus. J. Submicrosc. Cytol. Pathol. 2001, 33, 195–200. [Google Scholar] [PubMed]
- Mitchell, C.M.; Sturgis, C.D. Lipid-rich hepatocellular carcinoma in fine-needle aspiration biopsy. Diagn. Cytopathol. 2009, 37, 36–37. [Google Scholar] [CrossRef] [PubMed]
- Chetty, R.; Serra, S. Lipid-rich and clear cell neuroendocrine tumors (“carcinoids”) of the appendix: Potential confusion with goblet cell carcinoid. Am. J. Surg. Pathol. 2010, 34, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Salaria, S.N.; Graham, R.P.; Aishima, S.; Mounajjed, T.; Yeh, M.M.; Torbenson, M.S. Primary hepatic tumors with myxoid change: Morphologically unique hepatic adenomas and hepatocellular carcinomas. Am. J. Surg. Pathol. 2015, 39, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Young, J.T.; Kurup, A.N.; Graham, R.P.; Torbenson, M.S.; Venkatesh, S.K. Myxoid hepatocellular neoplasms: Imaging appearance of a unique mucinous tumor variant. Abdom. Radiol. 2016, 41, 2115–2122. [Google Scholar] [CrossRef] [PubMed]
- Atra, A.; Al-Asiri, R.; Wali, S.; Al-Husseini, H.; Al-Bassas, A.; Zimmermann, A. Hepatocellular carcinoma, syncytial giant cell: A novel variant in children: A case report. Ann. Diagn. Pathol. 2007, 11, 61–63. [Google Scholar] [CrossRef]
- Hirsch, T.Z.; Negulescu, A.; Gupta, B.; Caruso, S.; Noblet, B.; Couchy, G.; Bayard, Q.; Meunier, L.; Morcrette, G.; Scoazec, J.Y.; et al. BAP1 mutations define a homogeneous subgroup of hepatocellular carcinoma with fibrolamellar-like features and activated PKA. J. Hepatol. 2020, 72, 924–936. [Google Scholar] [CrossRef]
- Prokurat, A.; Kluge, P.; Kościesza, A.; Perek, D.; Kappeler, A.; Zimmermann, A. Transitional liver cell tumors (TLCT) in older children and adolescents: A novel group of aggressive hepatic tumors expressing beta-catenin. Med. Pediatr. Oncol. 2002, 39, 510–518. [Google Scholar] [CrossRef]
- Kanematsu, M.; Semelka, R.C.; Leonardou, P.; Mastropasqua, M.; Lee, J.K. Hepatocellular carcinoma of diffuse type: MR imaging findings and clinical manifestations. J. Magn. Reason. Imaging 2003, 18, 189–195. [Google Scholar] [CrossRef]
- Okuda, K.; Noguchi, T.; Kubo, Y.; Shimokawa, Y.; Kojiro, M.; Nakashima, T. A clinical and pathological study of diffuse type hepatocellular carcinoma. Liver 1981, 1, 280–289. [Google Scholar] [CrossRef] [PubMed]
- Xiong, M.J.; Patel, C.R.; Manne, U.; Al Diffalha, S. Cirrhotomimetic hepatocellular carcinoma: Experience of a single institution and review of the literature. Hepatic Oncol. 2020, 8, HEP28. [Google Scholar] [CrossRef] [PubMed]
- Jakate, S.; Yabes, A.; Giusto, D.; Naini, B.; Lassman, C.; Yeh, M.M.; Ferrell, L.D. Diffuse cirrhosis-like hepatocellular carcinoma: A clinically and radiographically undetected variant mimicking cirrhosis. Am. J. Surg. Pathol. 2010, 34, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Uenishi, T.; Kubo, S.; Yamamoto, T.; Shuto, T.; Ogawa, M.; Tanaka, H.; Tanaka, S.; Kaneda, K.; Hirohashi, K. Cytokeratin 19 expression in hepatocellular carcinoma predicts early postoperative recurrence. Cancer Sci. 2003, 94, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Durnez, A.; Verslype, C.; Nevens, F.; Fevery, J.; Aerts, R.; Pirenne, J.; Lesaffre, E.; Libbrecht, L.; Desmet, V.; Roskams, T. The clinicopathological and prognostic relevance of cytokeratin 7 and 19 expression in hepatocellular carcinoma. A possible progenitor cell origin. Histopathology 2006, 49, 138–151. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Heo, J.; Libbrecht, L.; Chu, I.S.; Kaposi-Novak, P.; Calvisi, D.F.; Mikaelyan, A.; Roberts, L.R.; Demetris, A.J.; Sun, Z.; et al. A novel prognostic subtype of human hepatocellular carcinoma derived from hepatic progenitor cells. Nat. Med. 2006, 12, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.P.; Conley, A.; Knudsen, B.S.; Guindi, M. Hypoxia after transarterial chemoembolization may trigger a progenitor cell phenotype in hepatocellular carcinoma. Histopathology 2015, 67, 442–450. [Google Scholar] [CrossRef]
- Rhee, H.; Nahm, J.H.; Kim, H.; Choi, G.H.; Yoo, J.E.; Lee, H.S.; Koh, M.J.; Park, Y.N. Poor outcome of hepatocellular carcinoma with stemness marker under hypoxia: Resistance to transarterial chemoembolization. Mod. Pathol. 2016, 29, 1038–1049. [Google Scholar] [CrossRef]
- Rhee, H.; Kim, H.; Park, Y.N. Clinico-radio-pathological and molecular features of hepatocellular carcinomas with keratin 19 expression. Liver Cancer 2020, 9, 663–681. [Google Scholar] [CrossRef]
- Theise, N.D.; Yao, J.L.; Harada, K.; Hytiroglou, P.; Portmann, B.; Thung, S.N.; Tsui, W.; Ohta, H.; Nakanuma, Y. Hepatic ‘stem cell’ malignancies in adults: Four cases. Histopathology 2003, 43, 263–271. [Google Scholar] [CrossRef]
- Monga, S.P. β-catenin signaling and roles in liver homeostasis, injury, and tumorigenesis. Gastroenterology 2015, 148, 1294–1310. [Google Scholar] [CrossRef] [PubMed]
- Gougelet, A.; Torre, C.; Veber, P.; Sartor, C.; Bachelot, L.; Denechaud, P.D.; Godard, C.; Moldes, M.; Burnol, A.F.; Dubuquoy, C.; et al. T-cell factor 4 and β-catenin chromatin occupancies pattern zonal liver metabolism in mice. Hepatology 2014, 59, 2344–2357. [Google Scholar] [CrossRef] [PubMed]
- Bioulac-Sage, P.; Kakar, S.; Nault, J.C. Hepatocellular adenoma. In WHO Classification of Tumours: Digestive System Tumours, 5th ed.; The WHO Classification of Tumours Editorial Board, Ed.; IARC Press: Lyon, France, 2019; pp. 224–228. ISBN 978-92-832-4499-8. [Google Scholar]
- Kim, H.; Park, Y.N. Hepatocellular adenomas: Recent updates. J. Pathol. Transl. Med. 2021, 55, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Luo, W. Nasopharyngeal carcinoma ecology theory: Cancer as multidimensional spatiotemporal “unity of ecology and evolution” pathological ecosystem. Theranostics 2023, 13, 1607–1631. [Google Scholar] [CrossRef] [PubMed]
- Sempoux, C.; Kakar, S.; Kondo, F.; Schirmacher, P. Combined hepatocellular-cholangiocarcinoma and undifferentiated primary liver carcinoma. In WHO Classification of Tumours: Digestive System Tumours, 5th ed.; The WHO Classification of Tumours Editorial Board, Ed.; IARC Press: Lyon, France, 2019; pp. 260–262. ISBN 978-92-832-4499-8. [Google Scholar]
- Sugiyama, T.; Tajiri, T.; Hiraiwa, S.; Inomoto, C.; Kajiwara, H.; Kojima, S.; Tobita, K.; Nakamura, N. Hepatic adrenal rest tumor: Diagnostic pitfall and proposed algorithms to prevent misdiagnosis as lipid-rich hepatocellular carcinoma. Pathol. Int. 2015, 65, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Galassi, A.; Pasquinelle, G.; Guerini, A.; Martinelli, G.; Venza, E. Benign myxoid hepatocellular tumor: A variant of liver cell adenoma. Liver 1995, 15, 233–235. [Google Scholar] [CrossRef] [PubMed]
- De Vos, N.; Van der Meulen, J.; Van Der Linden, M.; Claes, K.; Candaele, A.S.; Vanlander, A.; Troisi, R.I.; Van Vlierberghe, H.; Smeets, P.; Van Dorpe, J.; et al. Myxoid hepatocellular adenoma, a rare variant of hepatocellular adenoma with distinct imaging features: A case report with immunohistochemical and molecular analysis and literature review. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101478. [Google Scholar] [CrossRef]
- Kuwano, H.; Sonoda, T.; Hashimoto, H.; Enjoji, M. Hepatocellular carcinoma with osteoclast-like giant cells. Cancer 1984, 54, 837–842. [Google Scholar] [CrossRef]
- Hood, D.L.; Bauer, T.W.; Leibel, S.A.; McMahon, J.T. Hepatic giant cell carcinoma. An ultrastructural and immunohistochemical study. Am. J. Clin. Pathol. 1990, 93, 111–116. [Google Scholar] [CrossRef]
- Sasaki, A.; Yokoyama, S.; Nakayama, I.; Nakashima, K.; Kim, Y.I.; Kitano, S. Sarcomatoid hepatocellular carcinoma with osteoclast-like giant cells: Case report and immunohistochemical observations. Pathol. Int. 1997, 47, 318–324. [Google Scholar] [CrossRef]
- Lee, K.B. Sarcomatoid hepatocellular carcinoma with mixed osteoclast-like giant cells and chondroid differentiation. Clin. Mol. Hepatol. 2014, 20, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Griffith, O.L.; Griffith, M.; Krysiak, K.; Magrini, V.; Ramu, A.; Skidmore, Z.L.; Kunisaki, J.; Austin, R.; McGrath, S.; Zhang, J.; et al. A genomic case study of mixed fibrolamellar hepatocellular carcinoma. Ann. Oncol. 2016, 27, 1148–1154. [Google Scholar] [CrossRef]
- Torbenson, M.S. Benign and malignant pediatric tumors. In Biopsy Interpretation of the Liver, 4th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2020; pp. 627–659. ISBN 978-1-975157-29-6. [Google Scholar]
- Zimmermann, A.; Saxena, R. Hepatoblastoma. In WHO Classification of Tumours of the Digestive System, 4th ed.; Bosman, F.T., Carneiro, F., Hruban, R.H., Theise, N.D., Eds.; IARC Press: Lyon, France, 2010; pp. 228–235. ISBN 978-92-832-2432-7. [Google Scholar]
- López-Terrada, D.; Alaggio, R.; de Dávila, M.T.; Czauderna, P.; Hiyama, E.; Katzenstein, H.; Leuschner, I.; Malogolowkin, M.; Meyers, R.; Ranganathan, S.; et al. Towards an international pediatric liver tumor consensus classification: Proceedings of the Los Angeles COG liver tumors symposium. Mod. Pathol. 2014, 27, 472–491. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Ren, J.; O’Neil, M.; Zhao, J.; Bridges, B.; Cox, J.; Abdulkarim, B.; Schmitt, T.M.; Kumer, S.C.; Weinman, S.A. Impact of stem cell marker expression on recurrence of TACE-treated hepatocellular carcinoma post liver transplantation. BMC Cancer 2012, 12, 584. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, K.; Komuta, M.; Yasui, Y.; Tamaki, N.; Hosokawa, T.; Ueda, K.; Kuzuya, T.; Itakura, J.; Nakanishi, H.; Takahashi, Y.; et al. Expression of keratin 19 is related to high recurrence of hepatocellular carcinoma after radiofrequency ablation. Oncology 2011, 80, 278–288. [Google Scholar] [CrossRef]
- Rhee, H.; Kim, H.Y.; Choi, J.H.; Woo, H.G.; Yoo, J.E.; Nahm, J.H.; Choi, J.S.; Park, Y.N. Keratin 19 expression in hepatocellular carcinoma is regulated by fibroblast-derived HGF via a MET-ERK1/2-AP1 and SP1 axis. Cancer Res. 2018, 78, 1619–1631. [Google Scholar] [CrossRef]
- Brunt, E.; Aishima, S.; Clavien, P.A.; Fowler, K.; Goodman, Z.; Gores, G.; Gouw, A.; Kagen, A.; Klimstra, D.; Komuta, M.; et al. cHCC-CCA: Consensus terminology for primary liver carcinomas with both hepatocytic and cholangiocytic differentiation. Hepatology 2018, 68, 113–126. [Google Scholar] [CrossRef]
- Llovet, J.M.; Zucman-Rossi, J.; Pikarsky, E.; Sangro, B.; Schwartz, M.; Sherman, M.; Gores, G. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2016, 2, 16018. [Google Scholar] [CrossRef]
- Zucman-Rossi, J.; Villanueva, A.; Nault, J.C.; Llovet, J.M. Genetic landscape and biomarkers of hepatocellular carcinoma. Gastroenterology 2015, 149, 1226–1239.e4. [Google Scholar] [CrossRef]
- Rebouissou, S.; Nault, J.C. Advances in molecular classification and precision oncology in hepatocellular carcinoma. J. Hepatol. 2020, 72, 215–229. [Google Scholar] [CrossRef]
- Chiang, D.Y.; Villanueva, A.; Hoshida, Y.; Peix, J.; Newell, P.; Minguez, B.; LeBlanc, A.C.; Donovan, D.J.; Thung, S.N.; Solé, M.; et al. Focal gains of VEGFA and molecular classification of hepatocellular carcinoma. Cancer Res. 2008, 68, 6779–6788. [Google Scholar] [CrossRef] [PubMed]
- Hoshida, Y.; Nijman, S.M.; Kobayashi, M.; Chan, J.A.; Brunet, J.P.; Chiang, D.Y.; Villanueva, A.; Newell, P.; Ikeda, K.; Hashimoto, M.; et al. Integrative transcriptome analysis reveals common molecular subclasses of human hepatocellular carcinoma. Cancer Res. 2009, 69, 7385–7392. [Google Scholar] [CrossRef] [PubMed]
- The Cancer Genome Atlas Research Network. Comprehensive and integrative genomic characterization of hepatocellular carcinoma. Cell 2017, 169, 1327–1341.e23. [Google Scholar] [CrossRef]
- Boyault, S.; Rickman, D.S.; de Reyniès, A.; Balabaud, C.; Rebouissou, S.; Jeannot, E.; Hérault, A.; Saric, J.; Belghiti, J.; Franco, D.; et al. Transcriptome classification of HCC is related to gene alterations and to new therapeutic targets. Hepatology 2007, 45, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Morita, M.; Nishida, N.; Aoki, T.; Chishina, H.; Takita, M.; Ida, H.; Hagiwara, S.; Minami, Y.; Ueshima, K.; Kudo, M. Role of β-catenin activation in the tumor immune microenvironment and immunotherapy of hepatocellular carcinoma. Cancers 2023, 15, 2311. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Castet, F.; Heikenwalder, M.; Maini, M.K.; Mazzaferro, V.; Pinato, D.J.; Pikarsky, E.; Zhu, A.X.; Finn, R.S. Immunotherapies for hepatocellular carcinoma. Nat. Rev. Clin. Oncol. 2022, 19, 151–172. [Google Scholar] [CrossRef] [PubMed]
- Thorsson, V.; Gibbs, D.L.; Brown, S.D.; Wolf, D.; Bortone, D.S.; Ou Yang, T.H.; Porta-Pardo, E.; Gao, G.F.; Plaisier, C.L.; Eddy, J.A.; et al. the immune landscape of cancer. Immunity 2018, 48, 812–830.e14. [Google Scholar] [CrossRef]
- Sia, D.; Jiao, Y.; Martinez-Quetglas, I.; Kuchuk, O.; Villacorta-Martin, C.; Castro de Moura, M.; Putra, J.; Camprecios, G.; Bassaganyas, L.; Akers, N.; et al. Identification of an immune-specific class of hepatocellular carcinoma, based on molecular features. Gastroenterology 2017, 153, 812–826. [Google Scholar] [CrossRef]
- Montironi, C.; Castet, F.; Haber, P.K.; Pinyol, R.; Torres-Martin, M.; Torrens, L.; Mesropian, A.; Wang, H.; Puigvehi, M.; Maeda, M.; et al. Inflamed and non-inflamed classes of HCC: A revised immunogenomic classification. Gut 2023, 72, 129–140. [Google Scholar] [CrossRef]
- Haber, P.K.; Castet, F.; Torres-Martin, M.; Andreu-Oller, C.; Puigvehí, M.; Miho, M.; Radu, P.; Dufour, J.F.; Verslype, C.; Zimpel, C.; et al. Molecular markers of response to anti-PD1 therapy in advanced hepatocellular carcinoma. Gastroenterology 2023, 164, 72–88.e18. [Google Scholar] [CrossRef]
- Kurebayashi, Y.; Matsuda, K.; Ueno, A.; Tsujikawa, H.; Yamazaki, K.; Masugi, Y.; Kwa, W.T.; Effendi, K.; Hasegawa, Y.; Yagi, H.; et al. Immunovascular classification of HCC reflects reciprocal interaction between immune and angiogenic tumor microenvironments. Hepatology 2022, 75, 1139–1153. [Google Scholar] [CrossRef] [PubMed]
- Sautès-Fridman, C.; Lawand, M.; Giraldo, N.A.; Kaplon, H.; Germain, C.; Fridman, W.H.; Dieu-Nosjean, M.C. Tertiary lymphoid structures in cancers: Prognostic value, regulation, and manipulation for therapeutic intervention. Front. Immunol. 2016, 7, 407. [Google Scholar] [CrossRef] [PubMed]
- Calderaro, J.; Petitprez, F.; Becht, E.; Laurent, A.; Hirsch, T.Z.; Rousseau, B.; Luciani, A.; Amaddeo, G.; Derman, J.; Charpy, C.; et al. Intra-tumoral tertiary lymphoid structures are associated with a low risk of early recurrence of hepatocellular carcinoma. J. Hepatol. 2019, 70, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Komuta, M. Histological heterogeneity of primary liver cancers: Clinical relevance, diagnostic pitfalls and the pathologist’s role. Cancers 2021, 13, 2871. [Google Scholar] [CrossRef] [PubMed]
- Torbenson, M.S. Liver. In Surgical Pathology Dissection: An Illustrated Guide, 2nd ed.; Westra, W.H., Hruban, R.H., Phelps, T.H., Isacson, C., Eds.; Springer: New York, NY, USA, 2003; pp. 76–81. ISBN 9-780387-95599. [Google Scholar]
- Torbenson, M.S. Diagnostic approach to well-differentiated hepatocellular carcinoma. Diagn. Histopathol. 2021, 28, 69–78. [Google Scholar] [CrossRef]
- Torbenson, M. Masses of the liver. In Mills and Sternberg’s Diagnostic Surgical Pathology, 7th ed.; Longacre, T.A., Greenson, J.K., Hornick, J.L., Reuter, V.E., Eds.; Wolters Kluwer: Philadelphia, PA, USA, 2022; pp. 1890–1949. ISBN 978-1-975150-72-3. [Google Scholar]
- Saraf, S.A.; Tan, L.L.Y.; Leow, W.Q. A diagnostic approach to combined hepatocellular-cholangocarcinomas (cHCC-CCA). Am. J. Clin. Case Rep. 2021, 2, 1020. [Google Scholar]
- Hirokawa, F.; Hayashi, M.; Asakuma, M.; Shimizu, T.; Inoue, Y.; Uchiyama, K. Risk factors and patterns of early recurrence after curative hepatectomy for hepatocellular carcinoma. Surg. Oncol. 2016, 25, 24–29. [Google Scholar] [CrossRef]
- Shi, M.; Guo, R.P.; Lin, X.J.; Zhang, Y.Q.; Chen, M.S.; Zhang, C.Q.; Lau, W.Y.; Li, J.Q. Partial hepatectomy with wide versus narrow resection margin for solitary hepatocellular carcinoma: A prospective randomized trial. Ann. Surg. 2007, 245, 36–43. [Google Scholar] [CrossRef]
- Westerhoff, M.; Lamps, L.W.; Kakar, S. Hepatectomy specimen handling. In Diagnostic Pathology: Hepatobiliary and Pancreas, 3rd ed.; Elsevier: Philadelphia, PA, USA, 2022; pp. 348–349. ISBN 978-0-323-77620-2. [Google Scholar]
- Suriawinata, A.A.; Thung, S.N. Liver Pathology: An Atlas and Concise Guide; Demos Medical Publishing: New York, NY, USA, 2011; pp. 1–15. ISBN 9-781933-864945. [Google Scholar]
- Pallozzi, M.; Di Tommaso, N.; Maccauro, V.; Santopaolo, F.; Gasbarrini, A.; Ponziani, F.R.; Pompili, M. Non-invasive biomarkers for immunotherapy in patients with hepatocellular carcinoma: Current knowledge and future perspectives. Cancers 2022, 14, 4631. [Google Scholar] [CrossRef]
- Wu, X.; Li, J.; Gassa, A.; Buchner, D.; Alakus, H.; Dong, Q.; Ren, N.; Liu, M.; Odenthal, M.; Stippel, D.; et al. Circulating tumor DNA as an emerging liquid biopsy biomarker for early diagnosis and therapeutic monitoring in hepatocellular carcinoma. Int. J. Biol. Sci. 2020, 16, 1551–1562. [Google Scholar] [CrossRef]
- Wang, J.; Huang, A.; Wang, Y.P.; Yin, Y.; Fu, P.Y.; Zhang, X.; Zhou, J. Circulating tumor DNA correlates with microvascular invasion and predicts tumor recurrence of hepatocellular carcinoma. Ann. Transl. Med. 2020, 8, 237. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Chen, L. Exosomes in pathogenesis, diagnosis, and treatment of hepatocellular carcinoma. Front. Oncol. 2022, 12, 793432. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Yu, L.; Huang, P.; Zhou, Y.; Zheng, W.; Meng, N.; He, R.; Xu, Y.; Keong, T.S.; Cui, Y. Tumor-associated exosomes are involved in hepatocellular carcinoma tumorigenesis, diagnosis, and treatment. J. Clin. Transl. Hepatol. 2022, 10, 496–508. [Google Scholar] [CrossRef] [PubMed]
- Yasser, M.B.; Abdellatif, M.; Emad, E.; Jafer, A.; Ahmed, S.; Nageb, L.; Abdelshafy, H.; Al-Anany, A.M.; Al-Arab, M.A.E.; Gibriel, A.A. Circulatory miR-221 & miR-542 expression profiles as potential molecular biomarkers in hepatitis C virus mediated liver cirrhosis and hepatocellular carcinoma. Virus Res. 2021, 296, 198341. [Google Scholar] [CrossRef]
- Gibriel, A.A.; Al-Anany, A.M.; Al-Arab, M.A.E.; Azzazy, H.M.E. Investigating circulatory microRNA expression profiles in Egyptian patients infected with hepatitis C virus mediated hepatic disorders. Meta Gene 2020, 26, 100792. [Google Scholar] [CrossRef]
- Murai, H.; Kodama, T.; Maesaka, K.; Tange, S.; Motooka, D.; Suzuki, Y.; Shigematsu, Y.; Inamura, K.; Mise, Y.; Saiura, A.; et al. Multiomics identifies the link between intratumor steatosis and the exhausted tumor immune microenvironment in hepatocellular carcinoma. Hepatology 2023, 77, 77–91. [Google Scholar] [CrossRef] [PubMed]
- Cui, K.; Ou, Y.; Shen, Y.; Li, S.; Sun, Z. Clinical value of circulating tumor cells for the diagnosis and prognosis of hepatocellular carcinoma (HCC): A systematic review and meta-analysis. Medicine 2020, 99, e22242. [Google Scholar] [CrossRef] [PubMed]
- Trevisan França de Lima, L.; Broszczak, D.; Zhang, X.; Bridle, K.; Crawford, D.; Punyadeera, C. The use of minimally invasive biomarkers for the diagnosis and prognosis of hepatocellular carcinoma. Biochim. Biophys. Acta Rev. Cancer 2020, 1874, 188451. [Google Scholar] [CrossRef]
- Baj, J.; Bryliński, Ł.; Woliński, F.; Granat, M.; Kostelecka, K.; Duda, P.; Flieger, J.; Teresiński, G.; Buszewicz, G.; Furtak-Niczyporuk, M.; et al. Biomarkers and genetic markers of hepatocellular carcinoma and cholangiocarcinoma-what do we already know. Cancers 2022, 14, 1493. [Google Scholar] [CrossRef]
- Souissi, A.; Ben Said, M.; Ben Ayed, I.; Elloumi, I.; Bouzid, A.; Mosrati, M.A.; Hasnaoui, M.; Belcadhi, M.; Idriss, N.; Kamoun, H.; et al. Novel pathogenic mutations and further evidence for clinical relevance of genes and variants causing hearing impairment in Tunisian population. J. Adv. Res. 2021, 31, 13–24. [Google Scholar] [CrossRef]
- Marzi, L.; Mega, A.; Gitto, S.; Pelizzaro, F.; Seeber, A.; Spizzo, G. Impact and novel perspective of immune checkpoint inhibitors in patients with early and intermediate stage HCC. Cancers 2022, 14, 3332. [Google Scholar] [CrossRef]
- Rimassa, L.; Finn, R.S.; Sangro, B. Combination immunotherapy for hepatocellular carcinoma. J. Hepatol. 2023, 79, 506–515. [Google Scholar] [CrossRef]
- Calderaro, J.; Seraphin, T.P.; Luedde, T.; Simon, T.G. Artificial intelligence for the prevention and clinical management of hepatocellular carcinoma. J. Hepatol. 2022, 76, 1348–1361. [Google Scholar] [CrossRef]
- Schmauch, B.; Romagnoni, A.; Pronier, E.; Saillard, C.; Maillé, P.; Calderaro, J.; Kamoun, A.; Sefta, M.; Toldo, S.; Zaslavskiy, M.; et al. A deep learning model to predict RNA-Seq expression of tumours from whole slide images. Nat. Commun. 2020, 11, 3877. [Google Scholar] [CrossRef]
- Coudray, N.; Ocampo, P.S.; Sakellaropoulos, T.; Narula, N.; Snuderl, M.; Fenyö, D.; Moreira, A.L.; Razavian, N.; Tsirigos, A. Classification and mutation prediction from non-small cell lung cancer histopathology images using deep learning. Nat. Med. 2018, 24, 1559–1567. [Google Scholar] [CrossRef]
- Pellat, A.; Barat, M.; Coriat, R.; Soyer, P.; Dohan, A. Artificial intelligence: A review of current applications in hepatocellular carcinoma imaging. Diagn. Interv. Imaging 2023, 104, 24–36. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2000 WHO Classification (3rd Edition) | 2010 WHO Classification (4th Edition) | 2019 WHO Classification (5th Edition) | |
|---|---|---|---|
| Tumor category | Epithelial tumors, malignant | Epithelial tumors: hepatocellular, malignant | Malignant hepatocellular tumors |
| Tumor subtypes | HCC | HCC | HCC, NOS |
| Fibrolamellar carcinoma | Fibrolamellar carcinoma | Fibrolamellar carcinoma | |
| Scirrhous HCC | HCC, scirrhous | ||
| Lymphoepithelioma-like carcinoma | HCC, clear cell | ||
| Sarcomatoid HCC | HCC, steatohepatitic | ||
| HCC, macrotrabecular massive | |||
| HCC, chromophobe | |||
| HCC, neutrophil-rich | |||
| HCC, lymphocyte-rich |
| Genes | Approximate Frequency | Signaling Pathways and Roles |
|---|---|---|
| TERT promoter | 60% | Controls the transcription of the TERT gene which encodes for the catalytic subunit of telomerase; increased TERT expression and telomerase activity in HCC cells |
| TP53 | 50% | DNA repair and surveillance; frequency varies by risk factors, with the highest risk in areas of chronic aflatoxin B1 exposure |
| CTNNB1 | 40% | Wnt–β-catenin signaling pathway |
| ARID1A | 10–20% | Chromatin remodeling |
| AXIN1 | 10–15% | Wnt–β-catenin signaling pathway |
| FGF19 amplification | 5–10% | Encodes FGF19 protein that is a member of the FGF family; regulates bile acid synthesis and hepatocyte proliferation by activation of its receptor FGFR4 |
| RB1 | 5–10% | DNA repair and surveillance |
| RPS6KA3 | 5–10% | Oncogenic MAPK signaling |
| NFE2L2 | 5% | Oxidative stress |
| TSC1/2 | 5% | Tumor suppressor genes that encode TSC1 (hamartin) and TSC2 (tuberin), respectively; controls mTOR signaling by inhibiting the activity of the mTOR complex 1 |
| CDKN2A | 5% | DNA repair and surveillance |
| CCND1 | 5% | Encodes cyclin D1 protein which plays a critical role in cell cycle progression |
| Markers | Nature | Staining Pattern | Approximate Sensitivity (a) | Notes | References |
|---|---|---|---|---|---|
| Markers for Hepatocytic Differentiation | |||||
| Arginase-1 | Manganese metalloenzyme; plays a crucial role in the urea cycle; expressed in hepatocytes | Cytoplasmic and nuclear | 45–95% | Better than Hep Par-1 in poorly differentiated HCCs; negative in 10% of well-differentiated HCCs | [1,38,39,40] |
| Hep Par-1 | Carbamoyl phosphate synthetase 1, rate-limiting enzyme in the urea cycle; located in hepatocyte mitochondria | Cytoplasmic | 70–85% | Better than arginase-1 in well-differentiated HCCs | [1,38,39,40] |
| Polyclonal CEA | Glycoprotein produced during fetal development; cross-react with biliary glycoprotein I on the surface of bile canaliculi | Canalicular | 45–80% | Limited sensitivity in poorly differentiated HCCs; ambiguous staining patterns are not uncommon in moderately to poorly differentiated HCCs | [1,38,39,40] |
| CD10 | Zinc-dependent metalloproteinase; expressed along the bile canaliculi and luminal borders of bile ducts | Canalicular | 50–75% | Limited sensitivity in poorly differentiated HCCs; ambiguous staining patterns are not uncommon in moderately to poorly differentiated HCCs | [1,38,39,40] |
| α-fetoprotein | Oncofetal protein produced by the fetal liver and yolk sac during fetal development | Cytoplasmic | 30% | Frequently negative in well-differentiated HCCs | [1,38,39,40] |
| Bile salt export protein | Transmembrane protein; plays a critical role in the transport of bile salts; exclusively expressed at the bile canaliculi | Canalicular | 90% | High sensitivity and specificity for HCCs | [36] |
| Albumin mRNA in situ hybridization | Protein synthesized only in liver | Cytoplasmic | >95% | Positive in 80–95% of cholangiocarcinomas and some cases of metastatic adenocarcinomas | [38,39,40,41] |
| Markers for distinguishing benign and malignant hepatocellular tumors | |||||
| Glypican-3 | Heparin sulfate proteoglycan; play a role in the regulation of cell differentiation and growth | Cytoplasmic | 50–80% | More likely to be positive in poorly differentiated HCCs than Hep Par-1 and arginase-1; not expressed in normal and livers and therefore a good marker for malignant liver lesions | [1,38,39,40] |
| Glutamine synthetase | Enzyme involved in nitrogen metabolism; expressed in normal hepatocytes around the central vein | Cytoplasmic | 80% | Strong and diffuse staining supports the diagnosis of HCC in cirrhotic liver; also positive for focal nodular hyperplasia (map-like pattern) and hepatocellular adenoma | [1,38,39,40]. |
| Heat shock protein 70 | Highly conserved protein; plays a critical role in maintaining the function and survival of liver cells under stress | Cytoplasm | 50–60% | Could be a sensitive marker for the differential diagnosis of early HCC from precancerous lesion or noncancerous liver; low expression in normal hepatocytes and bile ducts | [1,38] |
| β-catenin | Protein encoded by the CTNNB1 gene; functions in cell adhesion; plays a central role as a key mediator in the Wnt signaling pathway | Nuclear | 30–40% | Positive staining supports HCC; not very sensitive, so negative staining is not informative; expressed in the cytoplasm and cell membrane of normal hepatocytes | [38,39,40] |
| EZH2 | Histone methyltransferase; catalytic subunit of PRC2; plays a critical role in the epigenetic regulation of gene expression | Cytoplasmic | 80% | Overexpression supports the diagnosis of HCC; expressed in hepatocytes and bile ducts | [42] |
| Ki67 | Nuclear protein associated with cell proliferation; used as a marker for cell proliferation | Nuclear | Most helpful if significantly higher than background liver; not all HCCs show a high proliferation rate | [38,39] | |
| CD34 | Transmembrane phosphoglycoprotein; expressed in endothelial cells | Cytoplasmic | Positive staining in HCC sinusoids (capillarization); strong diffuse staining is more common in HCC than in hepatocellular adenoma | [38,39,40] | |
| Reticulin | Constituent of the supporting framework of hepatic parenchyma | Reticulin loss in HCCs; widened cell plates (>2 cells thick) | [1,38,39,40] | ||
| Subtype | Relative Frequency | Clinical Features | Pathological Features | Molecular Features | Prognosis (b) | References |
|---|---|---|---|---|---|---|
| Steatohepatitic HCC | 5–20% | Steatohepatitis due to metabolic syndrome or alcohol abuse can occur in the background liver | >50% of tumor has histological features of steatohepatitis; fat, inflammation, and fibrosis | IL-6–JAK–STAT signaling activation; lower frequency of CTNNB1, TERT promoter, and TP53 mutations | Similar | [50,51,52,53,54,55] |
| Clear cell HCC | 3–7% | No distinct findings to date | >80% of tumor shows clear cell morphology due to glycogen accumulation; some steatosis is acceptable | No distinct findings to date | Better | [56,57,58,59,60,61] |
| Macrotrabecular massive HCC | 5% | High serum α-fetoprotein | >50% of tumor shows macrotrabecular growth pattern (>10 cells thick); vascular invasion common | TP53 mutations and FGF19 amplifications | Worse | [62,63,64] |
| Scirrhous HCC | 4% | Often mimics cholangiocarcinoma on imaging | >50% of tumor shows dense intratumoral fibrosis | TSC1/2 mutations; TGF-β signaling activation | Variable, no consensus in the literature | [65,66,67,68,69,70,71,72,73] |
| Chromophobe HCC | 3% | No distinct findings to date | Light, eosinophilic to clear (chromophobic) cytoplasm; mainly bland tumor nuclei, but scattered foci of more conspicuous nuclear atypia; microscopic pseudocysts | Alternative lengthening of telomeres | Similar | [74] |
| Fibrolamellar carcinoma | 1% | Young median age (25 years); no background liver disease | Large eosinophilic tumor cells with prominent nucleoli; dense intratumoral fibrosis with lamellar pattern | Activation of PKA via a DNAJB1::PRKACA fusion gene | Similar to HCC in non-cirrhotic liver | [75,76,77,78,79,80,81,82] |
| Neutrophil-rich HCC | <1% | Elevated serum white blood cell count, C-reactive protein, and IL-6 | Numerous and diffuse neutrophils within tumor; may have sarcomatoid areas | Tumor produces G-CSF | Worse | [83,84,85,86,87,88] |
| Lymphocyte-rich HCC | <1% | No distinct findings to date | Lymphocytes outnumber tumor cells in most areas | No distinct findings to date; not EBV-related | Better | [89,90,91] |
| Subtype | Relative Frequency | Clinical Features | Pathological Features | Molecular Features | Prognosis (b) | References |
|---|---|---|---|---|---|---|
| CTNNB1-mutated HCC | <1% | Enriched for the man; less likely to respond to ICI therapies | Well differentiated with thin trabecular pattern; prominent pseudoglands; bile production | CTNNB1 mutation | Better | [115,116,117,118] |
| Sarcomatoid HCC | <1% | Similar risk factors to conventional HCC; can be induced by anticancer therapy, such as chemoembolization | Both the HCC component and major ≥10% spindle cell component lacking specific differentiation | No distinct findings to date | Worse | [119,120] |
| Lipid-rich HCC | <1% | Non-alcoholic fatty liver disease in the background liver (subset) | Tumor cells have abundant cytoplasm filled with numerous small lipid droplets, resembling microvesicular steatosis | No distinct findings to date | Unclear | [121,122,123] |
| Myxoid HCC | <1% | Unique radiological findings | Tumor sinusoids are dissected by abundant myxoid material | No distinct findings to date | Unclear | [124,125] |
| HCC with syncytial giant cells | <1% | No distinct findings to date | Distinctive syncytial multinucleated giant cells | No distinct findings to date | Unclear | [126] |
| BAP1 mutated and PKA activated HCC | <1% | Elderly patients, often women; no underlying liver disease | Mixed histological features of HCC and fibrolamellar carcinoma; abundant fibrous stroma | BAP1 gene mutation | Worse | [127] |
| Transitional liver cell tumor | <1% | Older children and adolescents; elevated serum α-fetoprotein | Tumor cells are well to moderately differentiated; focal areas resembling hepatoblastomas | No distinct findings to date | Similar | [128] |
| Cirrhotomimetic HCC | <1% | Background liver cirrhosis in most cases; tumor burden can be underestimated by imaging studies | Numerous tumor nodules (>30); tumor cells are well to moderately differentiated | No distinct findings to date | Worse | [129,130,131,132] |
| Progenitor HCC | <5% | Increased serum α-fetoprotein | Morphologically compatible with HCC but >5% of tumor express cytokeratin 19; infiltrative growth, large tumors, frequent vascular invasion, poor differentiation | TP53 mutation; chromosomal instability | Worse | [133,134,135,136,137,138,139] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, J.H.; Thung, S.N. Advances in Histological and Molecular Classification of Hepatocellular Carcinoma. Biomedicines 2023, 11, 2582. https://doi.org/10.3390/biomedicines11092582
Choi JH, Thung SN. Advances in Histological and Molecular Classification of Hepatocellular Carcinoma. Biomedicines. 2023; 11(9):2582. https://doi.org/10.3390/biomedicines11092582
Chicago/Turabian StyleChoi, Joon Hyuk, and Swan N. Thung. 2023. "Advances in Histological and Molecular Classification of Hepatocellular Carcinoma" Biomedicines 11, no. 9: 2582. https://doi.org/10.3390/biomedicines11092582