
Circulating Surfactant Protein D: A Biomarker for Acute Lung Injury?


Abstract
:
1. Introduction
2. SP-D in Clinical Studies
3. SP-D in Preclinical Studies
4. Recombinant SP-D and Its Potential Benefits as a Treatment for ALI
5. Challenges and Future Directions
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ragaller, M.; Richter, T. Acute lung injury and acute respiratory distress syndrome. J. Emerg. Trauma Shock. 2010, 3, 43–51. [Google Scholar] [CrossRef]
- Lew, T.W.; Kwek, T.K.; Tai, D.; Earnest, A.; Loo, S.; Singh, K.; Kwan, K.M.; Chan, Y.; Yim, C.F.; Bek, S.L.; et al. Acute respiratory distress syndrome in critically ill patients with severe acute respiratory syndrome. JAMA 2003, 290, 374–380. [Google Scholar] [CrossRef]
- Matthay, M.A.; Zimmerman, G.A. Acute lung injury and the acute respiratory distress syndrome: Four decades of inquiry into pathogenesis and rational management. Am. J. Respir. Cell Mol. Biol. 2005, 33, 319–327. [Google Scholar] [CrossRef]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Rubenfeld, G.D.; Caldwell, E.; Peabody, E.; Weaver, J.; Martin, D.P.; Neff, M.; Stern, E.J.; Hudson, L.D. Incidence and outcomes of acute lung injury. N. Engl. J. Med. 2005, 353, 1685–1693. [Google Scholar] [CrossRef] [PubMed]
- Matthay, M.A.; Zemans, R.L.; Zimmerman, G.A.; Arabi, Y.M.; Beitler, J.R.; Mercat, A.; Herridge, M.; Randolph, A.G.; Calfee, C.S. Acute respiratory distress syndrome. Nat. Rev. Dis. Primers 2019, 5, 18. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, J.N.; Lucas, R.; Verin, A.D. The Acute Respiratory Distress Syndrome: Mechanisms and Perspective Therapeutic Approaches. Austin. J. Vasc. Med. 2015, 2, 1009. [Google Scholar]
- Welker, C.; Huang, J.; Gil, I.J.N.; Ramakrishna, H. 2021 Acute Respiratory Distress Syndrome Update, With Coronavirus Disease 2019 Focus. J. Cardiothorac. Vasc. Anesth. 2022, 36, 1188–1195. [Google Scholar] [CrossRef]
- Garcia-Laorden, M.I.; Lorente, J.A.; Flores, C.; Slutsky, A.S.; Villar, J. Biomarkers for the acute respiratory distress syndrome: How to make the diagnosis more precise. Ann. Transl. Med. 2017, 5, 283. [Google Scholar] [CrossRef]
- Lopez-Rodriguez, E.; Gay-Jordi, G.; Mucci, A.; Lachmann, N.; Serrano-Mollar, A. Lung surfactant metabolism: Early in life, early in disease and target in cell therapy. Cell Tissue Res. 2017, 367, 721–735. [Google Scholar] [CrossRef]
- Han, S.; Mallampalli, R.K. The Role of Surfactant in Lung Disease and Host Defense against Pulmonary Infections. Ann. Am. Thorac. Soc. 2015, 12, 765–774. [Google Scholar] [CrossRef]
- Vieira, F.; Kung, J.W.; Bhatti, F. Structure, genetics and function of the pulmonary associated surfactant proteins A and D: The extra-pulmonary role of these C type lectins. Ann. Anat. 2017, 211, 184–201. [Google Scholar] [CrossRef] [PubMed]
- Parra, E.; Alcaraz, A.; Cruz, A.; Aguilella, V.M.; Perez-Gil, J. Hydrophobic pulmonary surfactant proteins SP-B and SP-C induce pore formation in planar lipid membranes: Evidence for proteolipid pores. Biophys. J. 2013, 104, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Griese, M.; Lorenz, E.; Hengst, M.; Schams, A.; Wesselak, T.; Rauch, D.; Wittmann, T.; Kirchberger, V.; Escribano, A.; Schaible, T.; et al. Surfactant proteins in pediatric interstitial lung disease. Pediatr. Res. 2016, 79, 34–41. [Google Scholar] [CrossRef]
- Mulugeta, S.; Beers, M.F. Surfactant protein C: Its unique properties and emerging immunomodulatory role in the lung. Microbes Infect. 2006, 8, 2317–2323. [Google Scholar] [CrossRef]
- Singh, G.; Katyal, S.L. Clara cells and Clara cell 10 kD protein (CC10). Am. J. Respir. Cell Mol. Biol. 1997, 17, 141–143. [Google Scholar] [CrossRef]
- Fehrenbach, H. Alveolar epithelial type II cell: Defender of the alveolus revisited. Respir. Res. 2001, 2, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Walther, F.J.; Waring, A.J.; Sherman, M.A.; Zasadzinski, J.A.; Gordon, L.M. Hydrophobic surfactant proteins and their analogues. Neonatology 2007, 91, 303–310. [Google Scholar] [CrossRef]
- Sorensen, G.L.; Husby, S.; Holmskov, U. Surfactant protein A and surfactant protein D variation in pulmonary disease. Immunobiology 2007, 212, 381–416. [Google Scholar] [CrossRef]
- Kishore, U.; Greenhough, T.J.; Waters, P.; Shrive, A.K.; Ghai, R.; Kamran, M.F.; Bernal, A.L.; Reid, K.B.; Madan, T.; Chakraborty, T. Surfactant proteins SP-A and SP-D: Structure, function and receptors. Mol. Immunol. 2006, 43, 1293–1315. [Google Scholar] [CrossRef]
- Watson, A.; Madsen, J.; Clark, H.W. SP-A and SP-D: Dual Functioning Immune Molecules With Antiviral and Immunomodulatory Properties. Front. Immunol. 2020, 11, 622598. [Google Scholar] [CrossRef]
- Jiang, H.; Zhang, Y.; Hu, G.; Shang, X.; Ming, J.; Deng, M.; Li, Y.; Ma, Y.; Liu, S.; Zhou, Y. Innate/Inflammatory Bioregulation of Surfactant Protein D Alleviates Rat Osteoarthritis by Inhibiting Toll-Like Receptor 4 Signaling. Front. Immunol. 2022, 13, 913901. [Google Scholar] [CrossRef]
- Arroyo, R.; Kingma, P.S. Surfactant protein D and bronchopulmonary dysplasia: A new way to approach an old problem. Respir. Res. 2021, 22, 141. [Google Scholar] [CrossRef]
- Crouch, E.C. Surfactant protein-D and pulmonary host defense. Respir. Res. 2000, 1, 93–108. [Google Scholar] [CrossRef]
- Arroyo, R.; Echaide, M.; Wilmanowski, R.; Martin-Gonzalez, A.; Batllori, E.; Galindo, A.; Rosenbaum, J.S.; Moreno-Herrero, F.; Kingma, P.S.; Perez-Gil, J. Structure and activity of human surfactant protein D from different natural sources. Am. J. Physiol. Lung Cell Mol. Physiol. 2020, 319, L148–L158. [Google Scholar] [CrossRef] [PubMed]
- Rao, M.L.; Rao, G.S.; Eckel, J.; Breuer, H. Factors involved in the uptake of corticosterone by rat liver cells. Biochim. Biophys. Acta 1977, 500, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Doyle, I.R.; Bersten, A.D.; Nicholas, T.E. Surfactant proteins-A and -B are elevated in plasma of patients with acute respiratory failure. Am. J. Respir. Crit. Care Med. 1997, 156, 1217–1229. [Google Scholar] [CrossRef] [PubMed]
- Ohlmeier, S.; Vuolanto, M.; Toljamo, T.; Vuopala, K.; Salmenkivi, K.; Myllarniemi, M.; Kinnula, V.L. Proteomics of human lung tissue identifies surfactant protein A as a marker of chronic obstructive pulmonary disease. J. Proteome Res. 2008, 7, 5125–5132. [Google Scholar] [CrossRef]
- Greene, K.E.; King, T.E., Jr.; Kuroki, Y.; Bucher-Bartelson, B.; Hunninghake, G.W.; Newman, L.S.; Nagae, H.; Mason, R.J. Serum surfactant proteins-A and -D as biomarkers in idiopathic pulmonary fibrosis. Eur. Respir. J. 2002, 19, 439–446. [Google Scholar] [CrossRef]
- Ware, L.B.; Koyama, T.; Zhao, Z.; Janz, D.R.; Wickersham, N.; Bernard, G.R.; May, A.K.; Calfee, C.S.; Matthay, M.A. Biomarkers of lung epithelial injury and inflammation distinguish severe sepsis patients with acute respiratory distress syndrome. Crit. Care 2013, 17, R253. [Google Scholar] [CrossRef]
- Park, J.; Pabon, M.; Choi, A.M.K.; Siempos, I.I.; Fredenburgh, L.E.; Baron, R.M.; Jeon, K.; Chung, C.R.; Yang, J.H.; Park, C.M.; et al. Plasma surfactant protein-D as a diagnostic biomarker for acute respiratory distress syndrome: Validation in US and Korean cohorts. BMC Pulm. Med. 2017, 17, 204. [Google Scholar] [CrossRef] [PubMed]
- Endo, S.; Sato, N.; Nakae, H.; Yamada, Y.; Makabe, H.; Abe, H.; Imai, S.; Wakabayashi, G.; Inada, K.; Sato, S. Surfactant protein A and D (SP-A, AP-D) levels in patients with septic ARDS. Res. Commun. Mol. Pathol. Pharmacol. 2002, 111, 245–251. [Google Scholar]
- Yang, Q.; Li, Z.Q.; Lan, H.B.; Xiong, S.S.; Wang, S.S.; Yan, C.S. Research of the biomarkers in pulmonary and extrapulmonary acute respiratory distress syndrome. Zhonghua Yi Xue Za Zhi 2017, 97, 2023–2027. [Google Scholar] [CrossRef]
- Calfee, C.S.; Janz, D.R.; Bernard, G.R.; May, A.K.; Kangelaris, K.N.; Matthay, M.A.; Ware, L.B. Distinct molecular phenotypes of direct vs indirect ARDS in single-center and multicenter studies. Chest 2015, 147, 1539–1548. [Google Scholar] [CrossRef] [PubMed]
- Peukert, K.; Seeliger, B.; Fox, M.; Feuerborn, C.; Sauer, A.; Schuss, P.; Schneider, M.; David, S.; Welte, T.; Putensen, C.; et al. SP-D Serum Levels Reveal Distinct Epithelial Damage in Direct Human ARDS. J. Clin. Med. 2021, 10, 737. [Google Scholar] [CrossRef]
- Delgado, C.; Krotzsch, E.; Jimenez-Alvarez, L.A.; Ramirez-Martinez, G.; Marquez-Garcia, J.E.; Cruz-Lagunas, A.; Moran, J.; Hernandez, C.; Sierra-Vargas, P.; Avila-Moreno, F.; et al. Serum surfactant protein D (SP-D) is a prognostic marker of poor outcome in patients with A/H1N1 virus infection. Lung 2015, 193, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Cheng, I.W.; Ware, L.B.; Greene, K.E.; Nuckton, T.J.; Eisner, M.D.; Matthay, M.A. Prognostic value of surfactant proteins A and D in patients with acute lung injury. Crit. Care Med. 2003, 31, 20–27. [Google Scholar] [CrossRef]
- Wutzler, S.; Lehnert, T.; Laurer, H.; Lehnert, M.; Becker, M.; Henrich, D.; Vogl, T.; Marzi, I. Circulating levels of Clara cell protein 16 but not surfactant protein D identify and quantify lung damage in patients with multiple injuries. J. Trauma 2011, 71, E31–E36. [Google Scholar] [CrossRef]
- Determann, R.M.; Royakkers, A.A.; Haitsma, J.J.; Zhang, H.; Slutsky, A.S.; Ranieri, V.M.; Schultz, M.J. Plasma levels of surfactant protein D and KL-6 for evaluation of lung injury in critically ill mechanically ventilated patients. BMC Pulm. Med. 2010, 10, 6. [Google Scholar] [CrossRef]
- Greene, K.E.; Wright, J.R.; Steinberg, K.P.; Ruzinski, J.T.; Caldwell, E.; Wong, W.B.; Hull, W.; Whitsett, J.A.; Akino, T.; Kuroki, Y.; et al. Serial changes in surfactant-associated proteins in lung and serum before and after onset of ARDS. Am. J. Respir. Crit. Care Med. 1999, 160, 1843–1850. [Google Scholar] [CrossRef]
- Eisner, M.D.; Parsons, P.; Matthay, M.A.; Ware, L.; Greene, K.; Acute Respiratory Distress Syndrome, N. Plasma surfactant protein levels and clinical outcomes in patients with acute lung injury. Thorax 2003, 58, 983–988. [Google Scholar] [CrossRef]
- Chakrabarti, A.; Nguyen, A.; Newhams, M.M.; Ohlson, M.B.; Yang, X.; Ulufatu, S.; Liu, S.; Park, S.; Xu, M.; Jiang, J.; et al. Surfactant protein D is a biomarker of influenza-related pediatric lung injury. Pediatr. Pulmonol. 2022, 57, 519–528. [Google Scholar] [CrossRef]
- Dahmer, M.K.; Flori, H.; Sapru, A.; Kohne, J.; Weeks, H.M.; Curley, M.A.Q.; Matthay, M.A.; Quasney, M.W.; BALI and RESTORE Study Investigators and Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network. Surfactant Protein D Is Associated With Severe Pediatric ARDS, Prolonged Ventilation, and Death in Children With Acute Respiratory Failure. Chest 2020, 158, 1027–1035. [Google Scholar] [CrossRef]
- Ward, S.L.; Dahmer, M.K.; Weeks, H.M.; Sapru, A.; Quasney, M.W.; Curley, M.A.Q.; Liu, K.D.; Matthay, M.A.; Flori, H.R. Association of patient weight status with plasma surfactant protein D, a biomarker of alveolar epithelial injury, in children with acute respiratory failure. Pediatr. Pulmonol. 2020, 55, 2730–2736. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.J.; Zinter, M.S.; Chen, L.; Wong, K.M.Y.; Bhalla, A.; Gala, K.; Guglielmo, M.; Alkhouli, M.; Huard, L.L.; Hanudel, M.R.; et al. Beyond the Alveolar Epithelium: Plasma Soluble Receptor for Advanced Glycation End Products Is Associated With Oxygenation Impairment, Mortality, and Extrapulmonary Organ Failure in Children With Acute Respiratory Distress Syndrome. Crit. Care Med. 2022, 50, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Peukert, K.; Sauer, A.; Seeliger, B.; Feuerborn, C.; Fox, M.; Schulz, S.; Wild, L.; Borger, V.; Schuss, P.; Schneider, M.; et al. Increased Alveolar Epithelial Damage Markers and Inflammasome-Regulated Cytokines Are Associated with Pulmonary Superinfection in ARDS. J. Clin. Med. 2023, 12, 3649. [Google Scholar] [CrossRef] [PubMed]
- Orloff, K.E.; Turner, D.A.; Rehder, K.J. The Current State of Pediatric Acute Respiratory Distress Syndrome. Pediatr. Allergy Immunol. Pulmonol. 2019, 32, 35–44. [Google Scholar] [CrossRef]
- Hon, K.L.; Leung, K.K.Y.; Oberender, F.; Leung, A.K. Paediatrics: How to manage acute respiratory distress syndrome. Drugs Context 2021, 10, 1–12. [Google Scholar] [CrossRef]
- Carlton, E.F.; Flori, H.R. Biomarkers in pediatric acute respiratory distress syndrome. Ann. Transl. Med. 2019, 7, 505. [Google Scholar] [CrossRef]
- Punsawad, C.; Viriyavejakul, P.; Techarang, T. Surfactant Protein D Is Altered in Experimental Malaria-Associated Acute Lung Injury/Acute Respiratory Distress Syndrome. J. Trop. Med. 2019, 2019, 9281605. [Google Scholar] [CrossRef]
- Gaunsbaek, M.Q.; Rasmussen, K.J.; Beers, M.F.; Atochina-Vasserman, E.N.; Hansen, S. Lung surfactant protein D (SP-D) response and regulation during acute and chronic lung injury. Lung 2013, 191, 295–303. [Google Scholar] [CrossRef]
- Murata, M.; Otsuka, M.; Ashida, N.; Yamada, G.; Kuronuma, K.; Chiba, H.; Takahashi, H. Surfactant protein D is a useful biomarker for monitoring acute lung injury in rats. Exp. Lung Res. 2016, 42, 314–321. [Google Scholar] [CrossRef]
- King, B.A.; Kingma, P.S. Surfactant protein D deficiency increases lung injury during endotoxemia. Am. J. Respir. Cell Mol. Biol. 2011, 44, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Casey, J.; Kaplan, J.; Atochina-Vasserman, E.N.; Gow, A.J.; Kadire, H.; Tomer, Y.; Fisher, J.H.; Hawgood, S.; Savani, R.C.; Beers, M.F. Alveolar surfactant protein D content modulates bleomycin-induced lung injury. Am. J. Respir. Crit. Care Med. 2005, 172, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Meng, Q.; Sharif, A.; Abdel-Razek, O.A.; Zhang, L.; Wang, G.; Cooney, R.N. Surfactant Proteins SP-A and SP-D Ameliorate Pneumonia Severity and Intestinal Injury in a Murine Model of Staphylococcus aureus Pneumonia. Shock 2016, 46, 164–172. [Google Scholar] [CrossRef]
- Du, J.; Abdel-Razek, O.; Shi, Q.; Hu, F.; Ding, G.; Cooney, R.N.; Wang, G. Surfactant protein D attenuates acute lung and kidney injuries in pneumonia-induced sepsis through modulating apoptosis, inflammation and NF-kappaB signaling. Sci. Rep. 2018, 8, 15393. [Google Scholar] [CrossRef]
- Hsieh, M.H.; Chen, P.C.; Hsu, H.Y.; Liu, J.C.; Ho, Y.S.; Lin, Y.J.; Kuo, C.W.; Kuo, W.S.; Kao, H.F.; Wang, S.D.; et al. Surfactant protein D inhibits lipid-laden foamy macrophages and lung inflammation in chronic obstructive pulmonary disease. Cell Mol. Immunol. 2023, 20, 38–50. [Google Scholar] [CrossRef] [PubMed]
- Hillaire, M.L.; van Eijk, M.; Vogelzang-van Trierum, S.E.; Fouchier, R.A.; Osterhaus, A.D.; Haagsman, H.P.; Rimmelzwaan, G.F. Recombinant porcine surfactant protein D inhibits influenza A virus replication ex vivo. Virus Res. 2014, 181, 22–26. [Google Scholar] [CrossRef]
- Al-Ahdal, M.N.; Murugaiah, V.; Varghese, P.M.; Abozaid, S.M.; Saba, I.; Al-Qahtani, A.A.; Pathan, A.A.; Kouser, L.; Nal, B.; Kishore, U. Entry Inhibition and Modulation of Pro-Inflammatory Immune Response Against Influenza A Virus by a Recombinant Truncated Surfactant Protein D. Front. Immunol. 2018, 9, 1586. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, R.; Grant, S.N.; Colombo, M.; Salvioni, L.; Corsi, F.; Truffi, M.; Ottolina, D.; Hurst, B.; Salzberg, M.; Prosperi, D.; et al. Full-Length Recombinant hSP-D Binds and Inhibits SARS-CoV-2. Biomolecules 2021, 11, 1114. [Google Scholar] [CrossRef] [PubMed]
- Beirag, N.; Kumar, C.; Madan, T.; Shamji, M.H.; Bulla, R.; Mitchell, D.; Murugaiah, V.; Neto, M.M.; Temperton, N.; Idicula-Thomas, S.; et al. Human surfactant protein D facilitates SARS-CoV-2 pseudotype binding and entry in DC-SIGN expressing cells, and downregulates spike protein induced inflammation. Front. Immunol. 2022, 13, 960733. [Google Scholar] [CrossRef]
- Ikegami, M.; Scoville, E.A.; Grant, S.; Korfhagen, T.; Brondyk, W.; Scheule, R.K.; Whitsett, J.A. Surfactant protein-D and surfactant inhibit endotoxin-induced pulmonary inflammation. Chest 2007, 132, 1447–1454. [Google Scholar] [CrossRef] [PubMed]
- Sato, A.; Whitsett, J.A.; Scheule, R.K.; Ikegami, M. Surfactant protein-d inhibits lung inflammation caused by ventilation in premature newborn lambs. Am. J. Respir. Crit. Care Med. 2010, 181, 1098–1105. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surfactant Protein | Solubility | Molecular Weight | Predominant Structure | Biological Roles in the Lung |
|---|---|---|---|---|
| SP-A | Hydrophilic | 36 kDa | Hexamer |
|
| SP-B | Hydrophobic | 8 kDa | Homodimer |
|
| SP-C | Hydrophobic | 21 kDa | Monomer |
|
| SP-D | Hydrophilic | 43 kDa | Dodecamer |
|
| Main Findings | Reference |
|---|---|
| Higher SP-D levels were significantly associated with fewer ventilator-free days | [43] |
| Higher SP-D levels were significantly associated with fewer organ-failure-free days | |
| SP-D was significantly associated with the number of days on a ventilator and length of stay in hospital | [41] |
| The baseline correlation of SP-D with lung injury score was significant | |
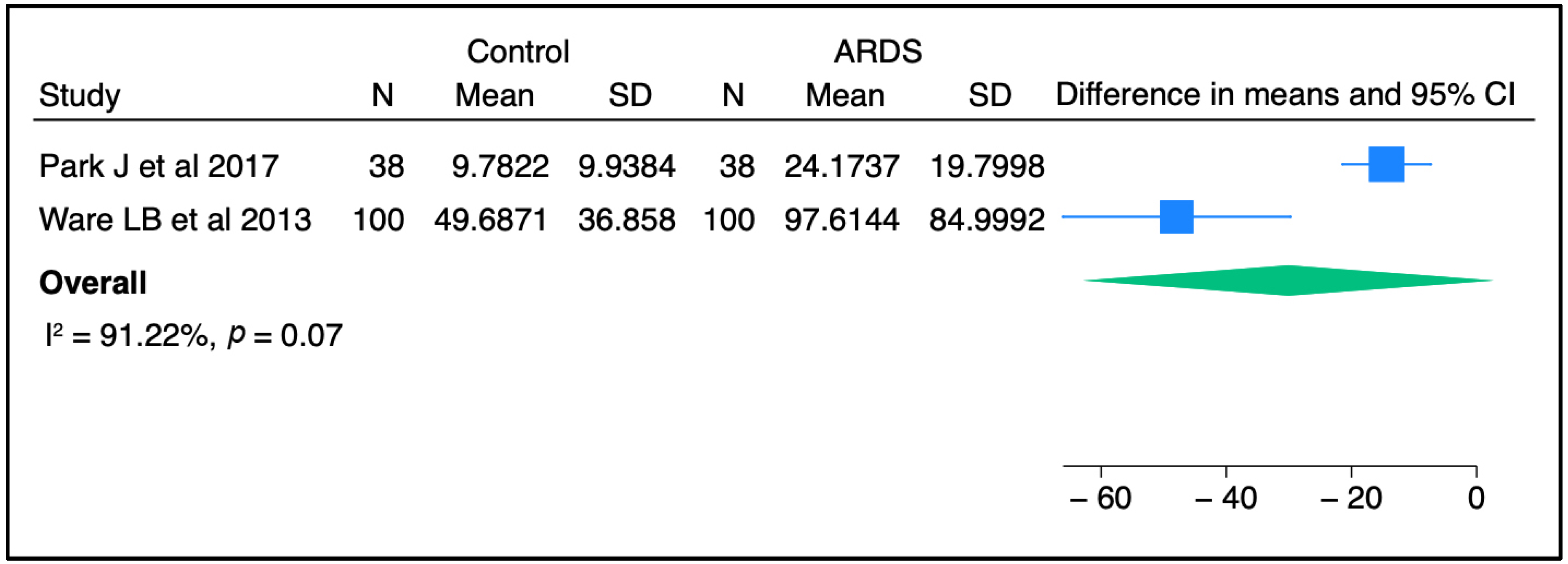
| SP-D was significantly correlated with the lung injury score on day 3 of ARDS | [42] |
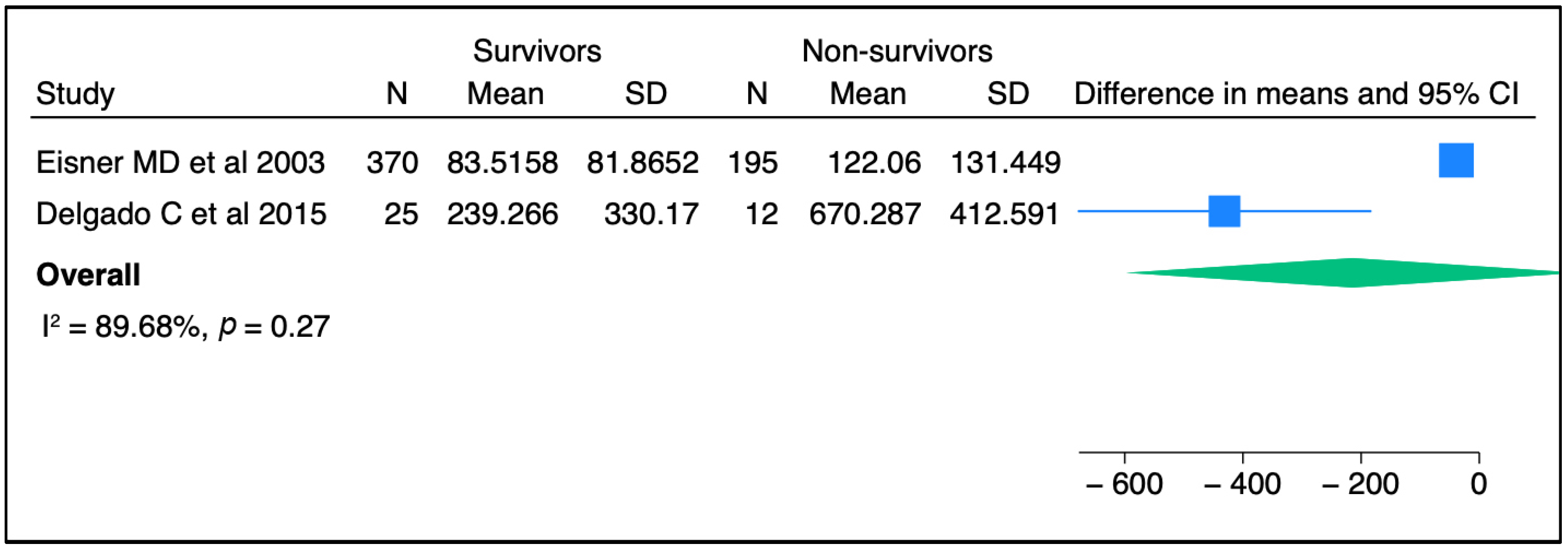
| Circulating SP-D was neither a specific nor sensitive predictor of mortality after the progression of ARDS | |
| Higher levels of SP-D were significantly associated with fatal outcomes in ARDS patients caused by influenza A virus (H1N1) | [36] |
| Circulating SP-D was significantly correlated with a diagnosis of moderate to severe PARDS, mechanical ventilator, ICU, and hospital length of stay in influenza-infected children | [44] |
| Plasma SP-D peaked on day 4 and remained elevated until day 9 | |
| SP-D significantly correlated with PRISM III score | |
| Multivariable regression analyses indicated that elevated SP-D concentrations were significantly associated with risk of death, duration of mechanical ventilation, pediatric ICU length of stay, and higher oxygenation index | [45] |
| SP-D was significantly higher in non-survivors than in living children | |
| SP-D concentrations were significantly and positively correlated with age | |
| Obesity was significantly associated with lower circulating SP-D levels among children with PARDS | [46] |
| Elevated plasma SP-D was significantly associated with oxygenation index (OI) and lung injury severity (LIS) on day 1 among PARDS patients | [47] |
| Direct lung injury led to higher SP-D levels in children than indirect lung injury | |
| There was a significant association between day 1 SP-D levels and in-hospital mortality | |
| The serum concentrations of SP-D were significantly increased in ARDS patients with pulmonary superinfections in comparison to ARDS patients without pulmonary superinfections | [48] |
| Reference | Experimental Model | Conclusion | Change in SP-D |
|---|---|---|---|
| [55] | LPS induced ALI | Lung levels of interleukin 6 (IL-6) and tumor necrosis factor alpha (TNF-α) were higher in SP-D knockout (KO) mice than in wild-type (WT) mice and were elevated more after indirect than direct lung injury. | - |
| The number of macrophage-specific antibody (MAC-3)-positive cells increased approximately 2-fold in SP-D KO mice after indirect lung injury. | - | ||
| The level of granulocyte-macrophage colony-stimulating factor (GM-CSF) was approximately 5-fold greater in SP-D KO mice than in WT mice in response to indirect injury. | - | ||
| [53] | LPS, bleomycin, or Pneumocystis carinii induced ALI | Serum SP-D levels increased continuously during chronic lung injury compared to acute injury. | ↑ |
| Strong immunoreactivity for SP-D was seen on macrophages and type II pneumocytes upon LPS exposure. | - | ||
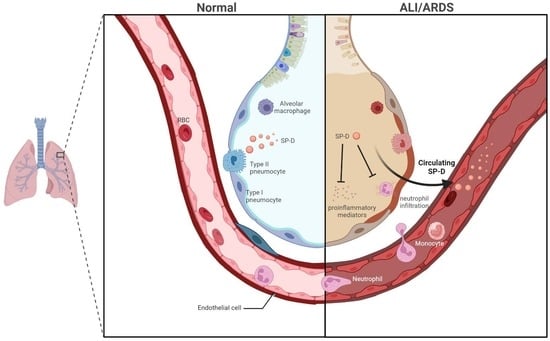
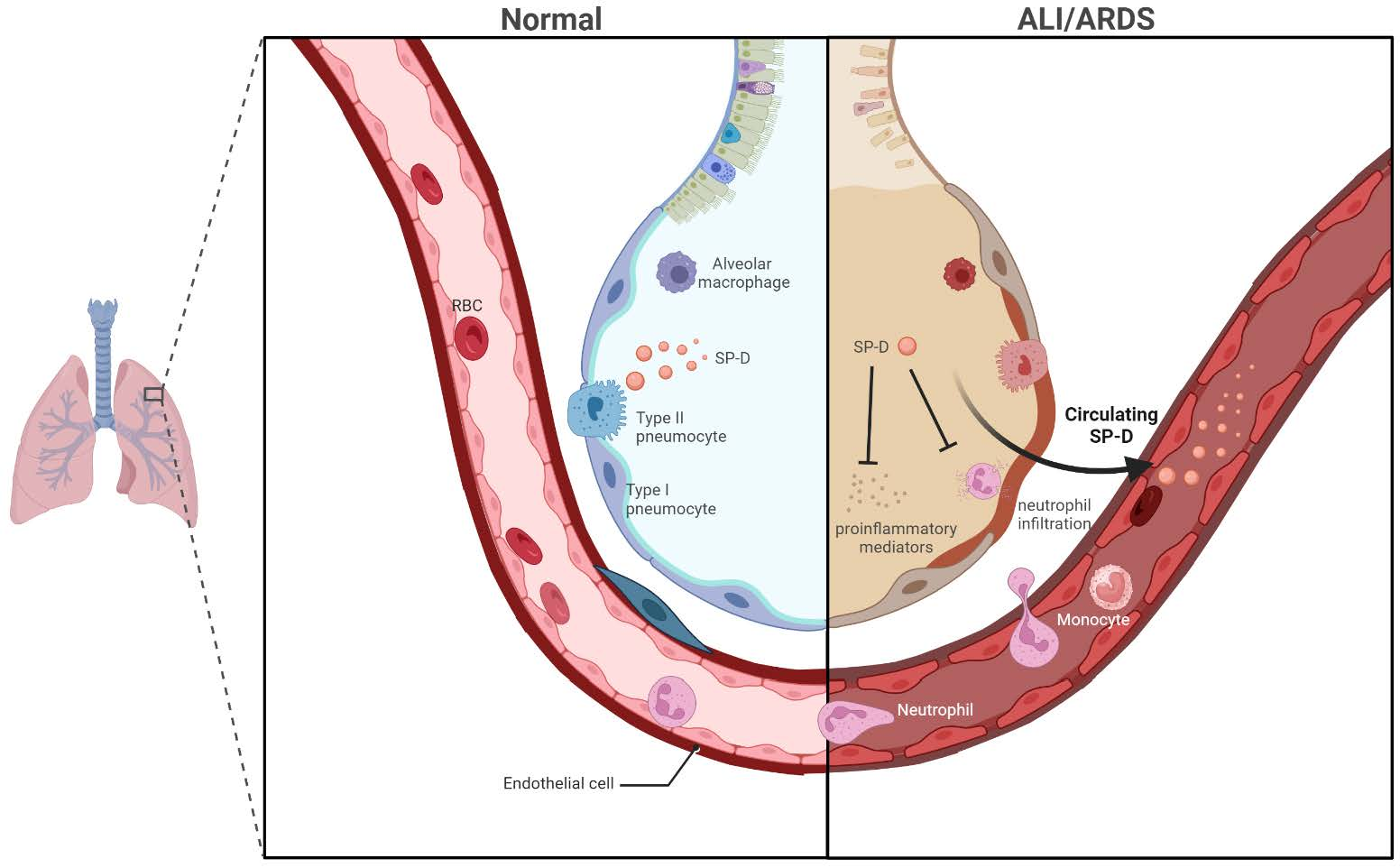
| SP-D translocated from the airways into the vascular system. | - | ||
| [54] | Bleomycin induced ALI | Serum SP-D levels reflected pathological alterations in the lungs, and the measurement of SP-D was a useful tool for detecting lung injury. | ↑ |
| SP-D immunoreactivity was seen on type II pneumocytes, Club cells, and alveolar macrophages. | - | ||
| Elevated SP-D expression was noted in alveolar type II cell hyperplasia on day 3. | - | ||
| SP-D levels in BALF increased and peaked on day 3 and significantly correlated with the total cell count, the granulocyte cell count, the serum albumin level, and the wet lung weight/body weight ratio. | ↑ | ||
| SP-D levels in serum were significantly elevated on day 5 and peaked on day 10. | ↑ | ||
| [56] | Bleomycin induced ALI | Higher mortality, greater respiratory distress, and weight loss were seen in SP-D KO mice after receiving bleomycin compared to WT. | - |
| More pulmonary parenchymal inflammation and BAL cellularity were seen in SP-D KO mice. | - | ||
| More trichrome staining and higher hydroxyproline levels were noted in the lung tissues of SP-D KO mice. | - | ||
| SP-D-overexpressing mice were significantly resistant to bleomycin-induced severity and mortality. | - | ||
| [57] | Staphylococcus aureus induced ALI | More severe infection was seen in double knockout (SP-A/D KO) mice than in WT controls. | - |
| [58] | Pseudomonas aeruginosa induced ALI | SP-D KO mice showed greater injury scores in the lung than WT. | - |
| A higher mortality rate was observed in infected KO mice compared to infected WT. | - | ||
| BALF neutrophil and macrophage counts were higher in KO mice than in WT after infection. | - | ||
| SP-D concentrations in the lung were reduced at 48 h after infection in WT. | ↓ | ||
| [44] | Influenza induced ALI | Circulating SP-D showed a greater increase in mice following influenza infection than other proteins. | ↑ |
| [52] | Malaria induced ALI | Malaria-infected mice had an increased protein level of SP-D in the plasma and lungs compared to uninfected mice. | ↑ |
| A significant positive correlation was seen between SP-D in the plasma and the lung. | ↑ | ||
| Positive staining of SP-D was found in alveolar type II cells and alveolar macrophages. | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elmore, A.; Almuntashiri, A.; Wang, X.; Almuntashiri, S.; Zhang, D. Circulating Surfactant Protein D: A Biomarker for Acute Lung Injury? Biomedicines 2023, 11, 2517. https://doi.org/10.3390/biomedicines11092517
Elmore A, Almuntashiri A, Wang X, Almuntashiri S, Zhang D. Circulating Surfactant Protein D: A Biomarker for Acute Lung Injury? Biomedicines. 2023; 11(9):2517. https://doi.org/10.3390/biomedicines11092517
Chicago/Turabian StyleElmore, Alyssa, Ali Almuntashiri, Xiaoyun Wang, Sultan Almuntashiri, and Duo Zhang. 2023. "Circulating Surfactant Protein D: A Biomarker for Acute Lung Injury?" Biomedicines 11, no. 9: 2517. https://doi.org/10.3390/biomedicines11092517