
Tall Cell Carcinoma with Reversed Polarity: Case Report of a Rare Special Type of Breast Cancer and Review of the Literature

Abstract
:1. Introduction
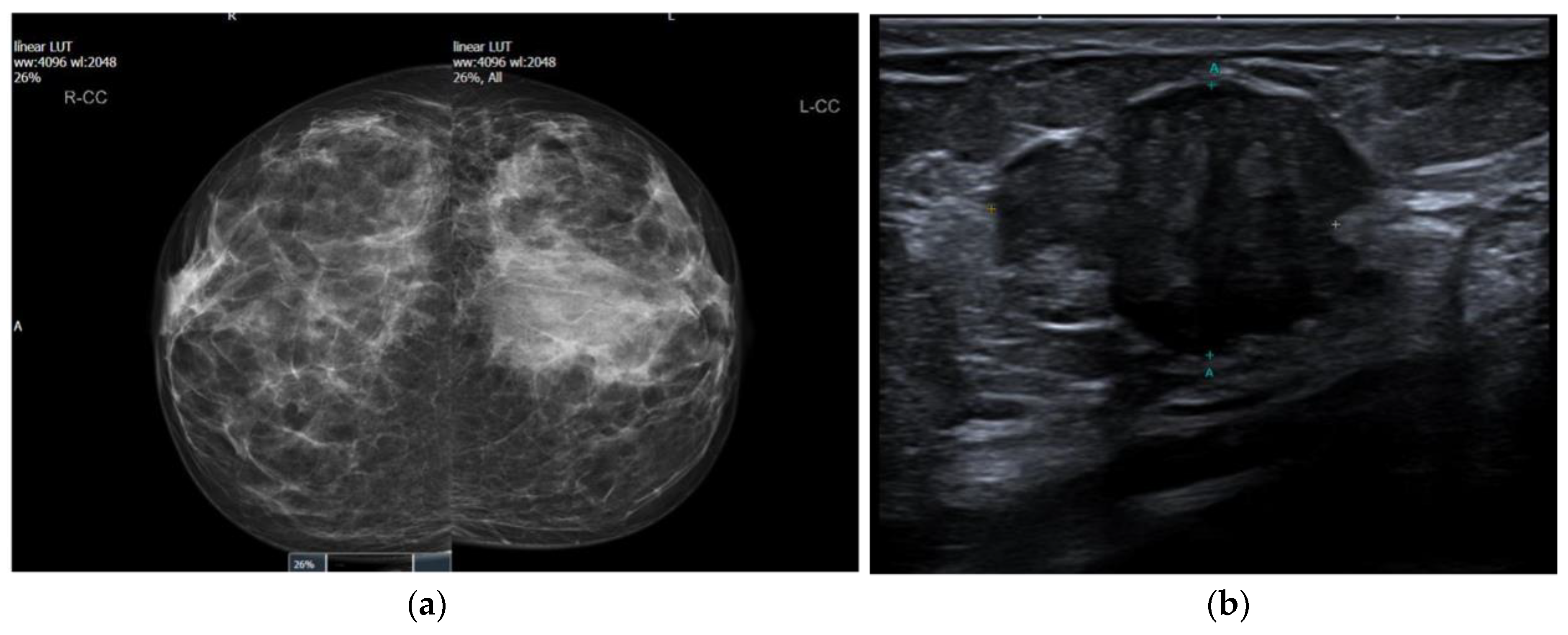
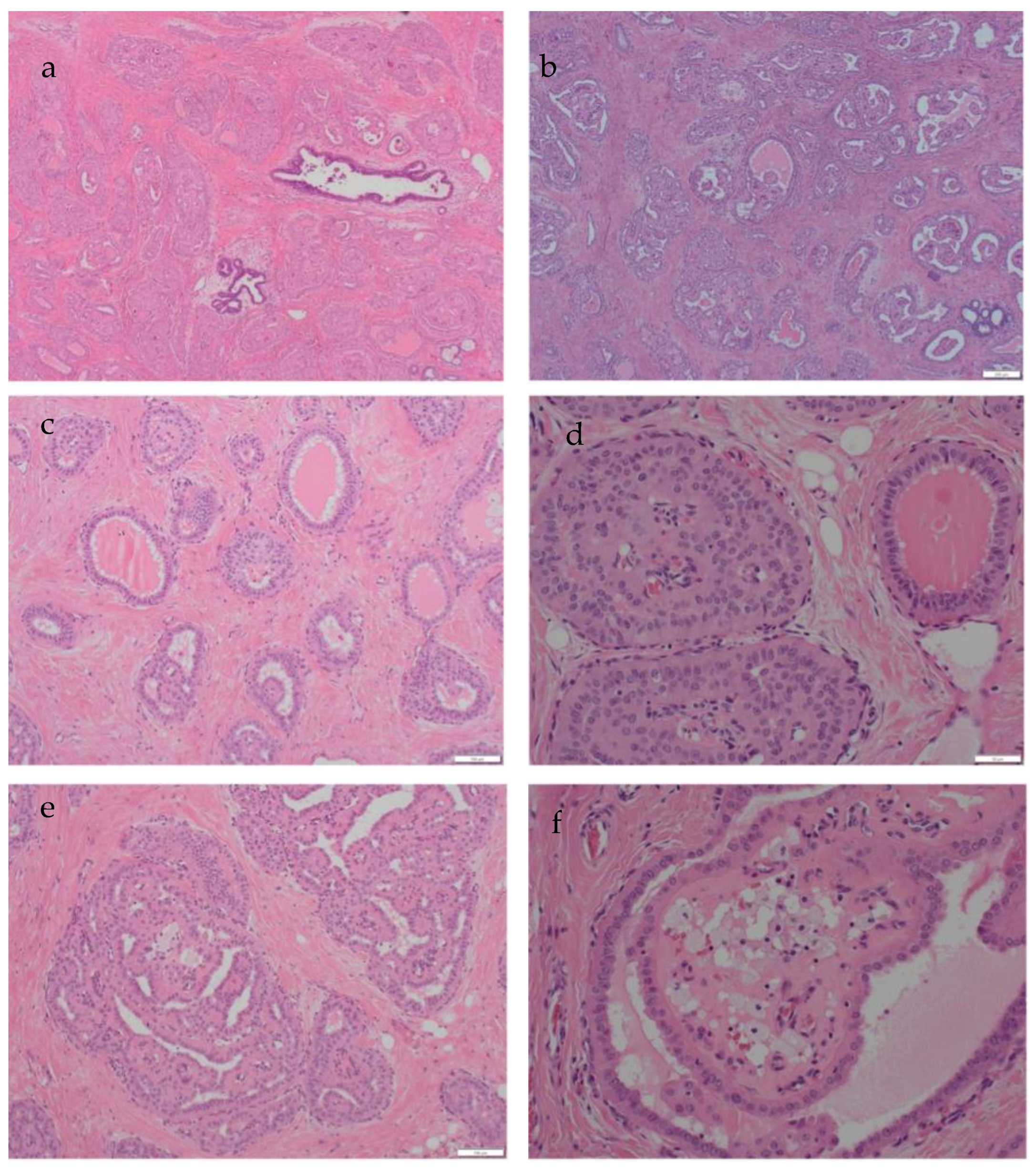
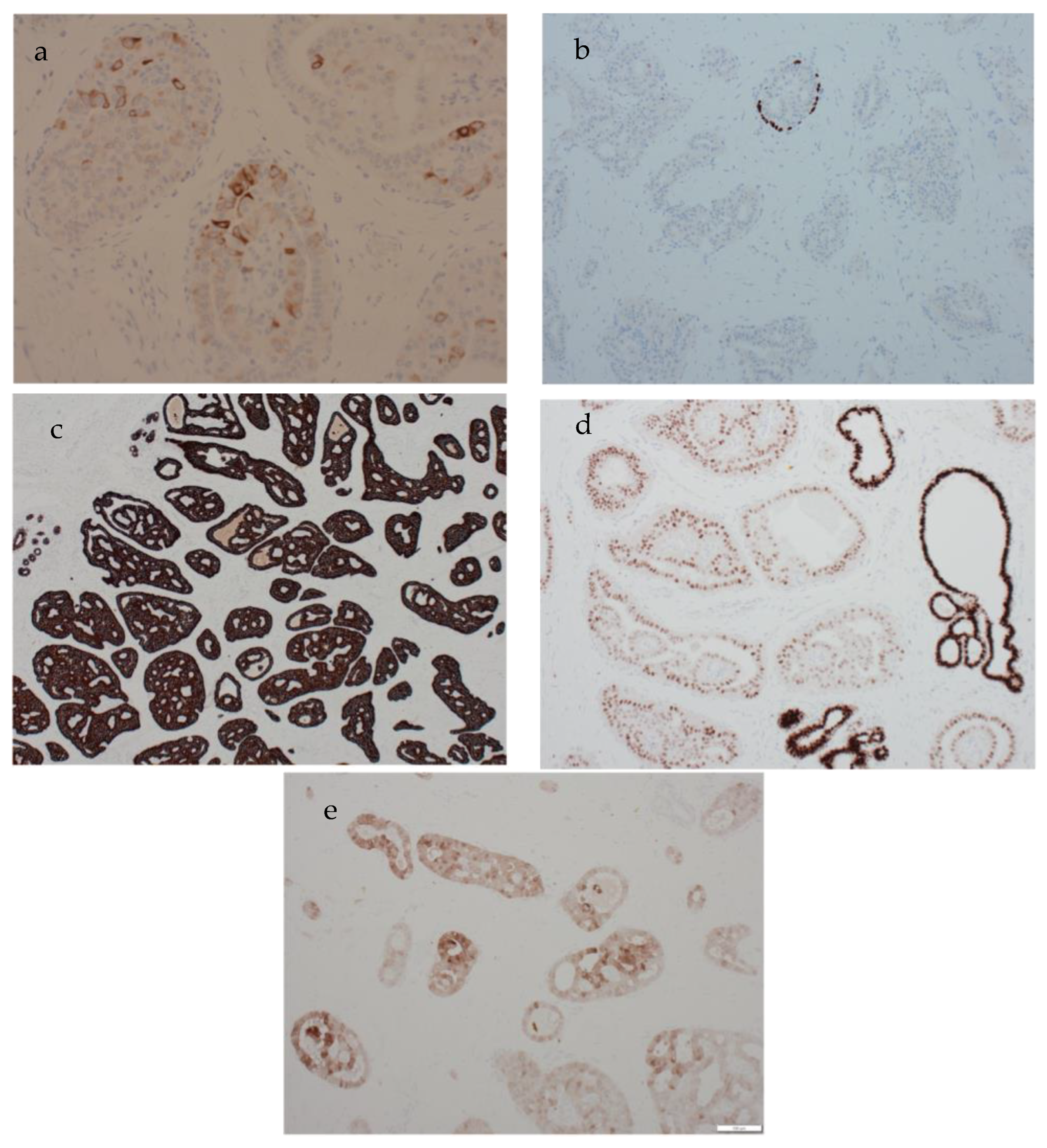
2. Clinical Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| TCCRP | Tall cell carcinoma of the breast with reversed polarity |
| ER | oestrogen receptor |
| HER2 | human epidermal growth factor receptor 2 |
| MDT | Multidisciplinary team |
References
- WHO (Ed.) WHO Classification of Breast Tumours, 5th ed.; World Health Organisation: Lyon, France, 2019.
- Foschini, M.P.; Asioli, S.; Foreid, S.; Cserni, G.; Ellis, I.O.; Eusebi, V.; Juan, R. Solid Papillary Breast Carcinomas Resembling the Tall Cell Variant of Papillary Thyroid Neoplasms: A Unique Invasive Tumor with Indolent Behavior. Am. J. Surg. Pathol. 2017, 41, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Chiang, S.; Weigelt, B.; Wen, H.C.; Pareja, F.; Raghavendra, A.; Martelotto, L.G.; Burke, K.A.; Basili, T.; Li, A.; Geyer, F.C.; et al. IDH2 Mutations Define a Unique Subtype of Breast Cancer with Altered Nuclear Polarity. Cancer Res. 2016, 76, 7118–7129. [Google Scholar] [CrossRef] [PubMed]
- Shaaban, A.; Shaw, E. Bench to bedside: Research influencing clinical practice in breast cancer. Diagn. Histopathol. 2022, 28, 473–479. [Google Scholar] [CrossRef]
- Tsang, J.Y.; Tse, G.M. Update on triple-negative breast cancers-highlighting subtyping update and treatment implication. Histopathology 2023, 82, 17–35. [Google Scholar] [CrossRef] [PubMed]
- Eusebi, V.; Damiani, S.; Ellis, I.O.; Azzopardi, J.G.; Rosai, J. Breast tumor resembling the tall cell variant of papillary thyroid carcinoma: Report of 5 cases. Am. J. Surg. Pathol. 2003, 27, 1114–1118. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wu, H.; Wang, Z.; Zhou, Y.; Mao, F.; Lin, Y.; Shen, S.; Liang, Z.; Sun, Q. Tall cell carcinoma of the breast with reverse polarity: Case report with gene sequencing and literature review. Gland. Surg. 2021, 10, 837–843. [Google Scholar] [CrossRef]
- Trihia, H.J.; Lampropoulos, P.; Karelis, L.; Souka, E.; Galanopoulos, G.; Provatas, I. Tall cell carcinoma with reversed polarity: A case report of a very rare breast tumor entity and mini-review. Breast J. 2021, 27, 369–376. [Google Scholar] [CrossRef]
- Matute, G.; Barcenas, L.; Bautista, C.; Restrepo Ramirez, C.A.; Llinas Quintero, N. Tall Cell Carcinoma with Reversed Polarity of the Breast. Cureus 2021, 13, e16814. [Google Scholar] [CrossRef] [PubMed]
- Jassim, M.; Premalata, C.S.; Okaly, G.; Srinivas, C. Tall Cell Carcinoma with Reverse Polarity of Breast: Report of a Case with Unique Morphologic and Molecular Features. Turk. Patoloji. Derg. 2021, 37, 183–188. [Google Scholar] [CrossRef]
- Wei, Y.; Ding, L.; Song, X.; Tian, X.; Min, N.; Guan, Q.; Li, X.; Liu, M. Tall cell carcinoma with reversed polarity: Case report with gene sequencing and literature review. Gland. Surg. 2021, 10, 3147–3154. [Google Scholar] [CrossRef] [PubMed]
- Haefliger, S.; Muenst, S.; Went, P.; Bihl, M.; Dellas, S.; Weber, W.P.; Vlajnic, T. Tall cell carcinoma of the breast with reversed polarity (TCCRP) with mutations in the IDH2 and PIK3CA genes: A case report. Mol. Biol. Rep. 2020, 47, 4917–4921. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, R.; Florea, A.V.; Pelmus, M.; Jones, M.W.; Bonaventura, M.; Wald, A.; Nikiforova, M. Breast Tumor Resembling Tall Cell Variant of Papillary Thyroid Carcinoma: A Solid Papillary Neoplasm with Characteristic Immunohistochemical Profile and Few Recurrent Mutations. Am. J. Clin. Pathol. 2017, 147, 399–410. [Google Scholar] [CrossRef]
- Colella, R.; Guerriero, A.; Giansanti, M.; Sidoni, A.; Bellezza, G. An additional case of breast tumor resembling the tall cell variant of papillary thyroid carcinoma. Int. J. Surg. Pathol. 2015, 23, 217–220. [Google Scholar] [CrossRef]
- WHO Classification of Tumours Editorial Board. Endocrine and neuroendocrine tumours. In WHO Classification of Tumours Series, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2022; Volume 10. [Google Scholar]
- Betts, G.; Beckett, E.; Nonaka, D. GATA3 shows differential immunohistochemical expression across thyroid and parathyroid lesions. Histopathology 2014, 65, 288–290. [Google Scholar] [CrossRef]
- Toss, M.S.; Billingham, K.; Egbuniwe, I.U.; Moreno, F.; Abass, A.; Rakha, E.A. Breast Tumours Resembling the Tall Cell Variant of Thyroid Papillary Carcinoma: Are They Part of the Papillary Carcinoma Spectrum or a Distinct Entity? Pathobiology 2019, 86, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Eberle, C.A.; Piscuoglio, S.; Rakha, E.A.; Ng, C.K.; Geyer, F.C.; Edelweiss, M.; Sakr, R.A.; Weigelt, B.; Reis-Filho, J.S.; Ellis, I.O. Infiltrating epitheliosis of the breast: Characterization of histological features, immunophenotype and genomic profile. Histopathology 2016, 68, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- Shaaban, A. Diagnostic pitfalls in needle core biopsy of the breast. Diagn. Histopathol. 2022, 28, 156–160. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | Age of Patient | Presenting Features | Radiological Features | Pathology Features | Immunohistochemistry |
|---|---|---|---|---|---|---|
| Elghobashy et al. (current study) | 2023 | 41 | Symptomatic lump | Ill-defined mass with normal axillary nodes | Proliferation of large, tall cells that exhibited solid nests with central fibrovascular cores and associated luminal histiocytes | +ve: CK5, CK7, GATA-3, calretinin −ve: ER, PR, HER2, TTF1, p63 |
| Trihia et al., 2021 [8] | 2021 | 70 | Incidental mammographic finding | Well-defined 9 mm lesion with normal axillary nodes | Nests of epithelial cells with focal solid papillary pattern. Tall columnar cells with reversed polarity | +ve: GATA3, Keratin 903, mammoglobin (focal) −ve: P63, SMA, CK5/6, ER/PR |
| Matute et al. [9] | 2021 | 63 | Identified via screening | Focal asymmetry, nodularity | Trabeculae, nests of columnar cells with histiocytes, wide granular cytoplasm | +ve: CK5/CK6, CK7, GCDFP-15, GATA-3 −ve: HER2, ER, PR, AR |
| Jassim et al. [10] | 2021 | 40 | Lump | BIRADS IV lesion | Nests of neoplastic cells, solid papillary pattern lined with columnar epithelial cells | +ve: CK5/CK6, GATA3, ER (weakly) −ve: HER2, BCL2 |
| Wei et al., 2021 [11] | 2021 | 72 | Palpable mass | Well circumscribed hypoechoic lesion | Papillary architecture, eosinophilic cytoplasm | +ve: ER, GATA-3 −ve: SMMHC, p63, PR |
| 70 | Palpable mass | Nodular density | Reversed polarity, eosinophilic cytoplasm, ovoid nuclei | +ve: CK5, calretinin, ER (weakly), SOX-10, GCDFP-15 −ve: SMMHC, p63, | ||
| Zhang et al. [7] | 2021 | 45 | Breast mass | Hypoechoic lesion | Circumscribed tumour cell nests with fibrovascular cores | +ve: CK5/CK6, GATA3, GCDFP-15, mammaglobin −ve: ER, PR, HER-2, S-100, p53 |
| Haefliger et al. [12] | 2020 | 60 | Breast nodule | BIRADS 4 lesion | Epithelial lesion with nests and solid papillary architecture | +ve: CK5/CK6, GATA3, E-cadherin −ve: ER, PR, HER-2, S-100, TTF1 |
| Foschini et al. [2] | 2017 | 13 cases ranging from 48 years to 85 years | 3 cases identified via screening 10 cases with palpable nodules | - | Multilobular architecture with neoplastic cells arranged in papillary, solid and follicular structures, fibrovascular cores | +ve: CK7 (in 10 out of 13 cases), CK14 (in 3 out of 13 cases), CK5/CK6 (in 7 out of 13 cases), GATA-3 (in 5 out of 13 cases) −ve: ER (in 10 out of 13 cases), PR (in 10 out of 13 cases), HER-2 (in all 13 cases) |
| Bhargava et al. [13] | 2017 | 65 | Breast mass | - | Nodular papillary lesion | +ve: CK5/CK6, S-100 −ve: SMMHC, p63, ER |
| 77 | Breast mass | - | Lobulated papillary lesion intersected by thick fibrous bands, eosinophilic secretions | +ve: CK5/CK6, ER (weakly), AE1/AE3, S-100, GATA-3 −ve: p63, SMMHC, TTF-1, thyroglobulin | ||
| 48 | Breast mass | - | Proliferative nodular lesion, nuclear grooves, reversed polarity | +ve: CK5/CK6, S-100 −ve: p63, SMMHC | ||
| Chiang et al. [3] | 2016 | 13 cases ranging from 51 years to 79 years | - | - | Circumscribed nodules of columnar epithelial cells with many containing fibrovascular cores and reverse polarity | +ve: CK5/CK6 (in 12 out of 13 cases), CK7(in 11 out of 13 cases) −ve: p63 (in all cases), SMMHC (in 12 out of 13 cases), ER (in 8 out of 13 cases), PR (in 11 out of 13 cases), HER-2 (in 10 out of 13 cases), TTF-1 (in 12 out of 13 cases) |
| Colella et al. [14] | 2014 | 79 | Breast mass, bloody nipple secretion | Lesion suspicious of malignancy | Cystic spaces containing eosinophilic material, epithelial cells with columnar configuration | +ve: GCDFP-15 −ve: TTF-1, thyroglobulin |
| Feature | Apocrine Carcinoma | Secretory Carcinoma | Solid Papillary Carcinoma | Encapsulated Papillary Carcinoma | Papillary Thyroid Carcinoma | TCCRP |
|---|---|---|---|---|---|---|
| Papillary architecture | Uncommon, may be focal | Uncommon | Common, solid papillary enclosing sinusoidal vessels | Common well developed papillary architecture with cystic change and haemorrhage | Common | Common |
| Secretion | Not a feature | Common including intra and extracellular PAS positive secretion | Extracellular mucin is common | Not a feature | Common, follicles with colloid | Common, colloid- like |
| Cells | Large with vesicular nuclei and ample granular eosinophilic cytoplasm. Can be low, intermediate of high grade | Usually low to intermediate grade nuclei, Inconspicuous nucleoli, prominent secretion | Low to intermediate grade nuclei, inconspicuous nucleoli | Low to intermediate grade nuclei, infrequent mitoses | Oval crowded pale nuclei with nuclear grooves and pseudo includsions | Pale cells, low to intermediate grade nuclei, inconspicuous nucleoli |
| Nuclear polarity | Normal | Normal | Normal | Normal | Normal | Reversed |
| Immunohistochemistry | GCDFP-15, GATA-3, AR positive. Often ER/PR negative, can be HER2 positive | Often triple negative, NTRK positive, alpha1 antitrypsin positive | Positive for neuroendocrine markers, usually lacking myoepithelial staining in and around lesion | Usually lacking myoepithelial staining in and around lesion. Negative for neuroendocrine markers | Positive for TTF1, Thyroglobulin, PAX8, CK7, AE1/3, CAM5.2 | Positive for low and high molecular weight cytokeratins, Often triple negative, GATA-3 positive, antimitochondrial antibody positive IDH2 positive |
| Molecular profile | Non-specific | ETV6-NTRK3 gene fusion | PIK3CA in 45% of cases | Nonspecific | BRAF, RET mutations | IDH2 p.Arg172 mutations |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elghobashy, M.; Jenkins, S.; Shulman, Z.; O’Neil, A.; Kouneli, S.; Shaaban, A.M. Tall Cell Carcinoma with Reversed Polarity: Case Report of a Rare Special Type of Breast Cancer and Review of the Literature. Biomedicines 2023, 11, 2376. https://doi.org/10.3390/biomedicines11092376
Elghobashy M, Jenkins S, Shulman Z, O’Neil A, Kouneli S, Shaaban AM. Tall Cell Carcinoma with Reversed Polarity: Case Report of a Rare Special Type of Breast Cancer and Review of the Literature. Biomedicines. 2023; 11(9):2376. https://doi.org/10.3390/biomedicines11092376
Chicago/Turabian StyleElghobashy, Maiar, Stephanie Jenkins, Zachary Shulman, Anne O’Neil, Sofia Kouneli, and Abeer M. Shaaban. 2023. "Tall Cell Carcinoma with Reversed Polarity: Case Report of a Rare Special Type of Breast Cancer and Review of the Literature" Biomedicines 11, no. 9: 2376. https://doi.org/10.3390/biomedicines11092376