
Cardiovascular Consequences of Acute Kidney Injury: Treatment Options

 ,
, 
Abstract
:1. Introduction
2. Scope of the Problem
2.1. The Co-Dependency of Heart and Kidneys
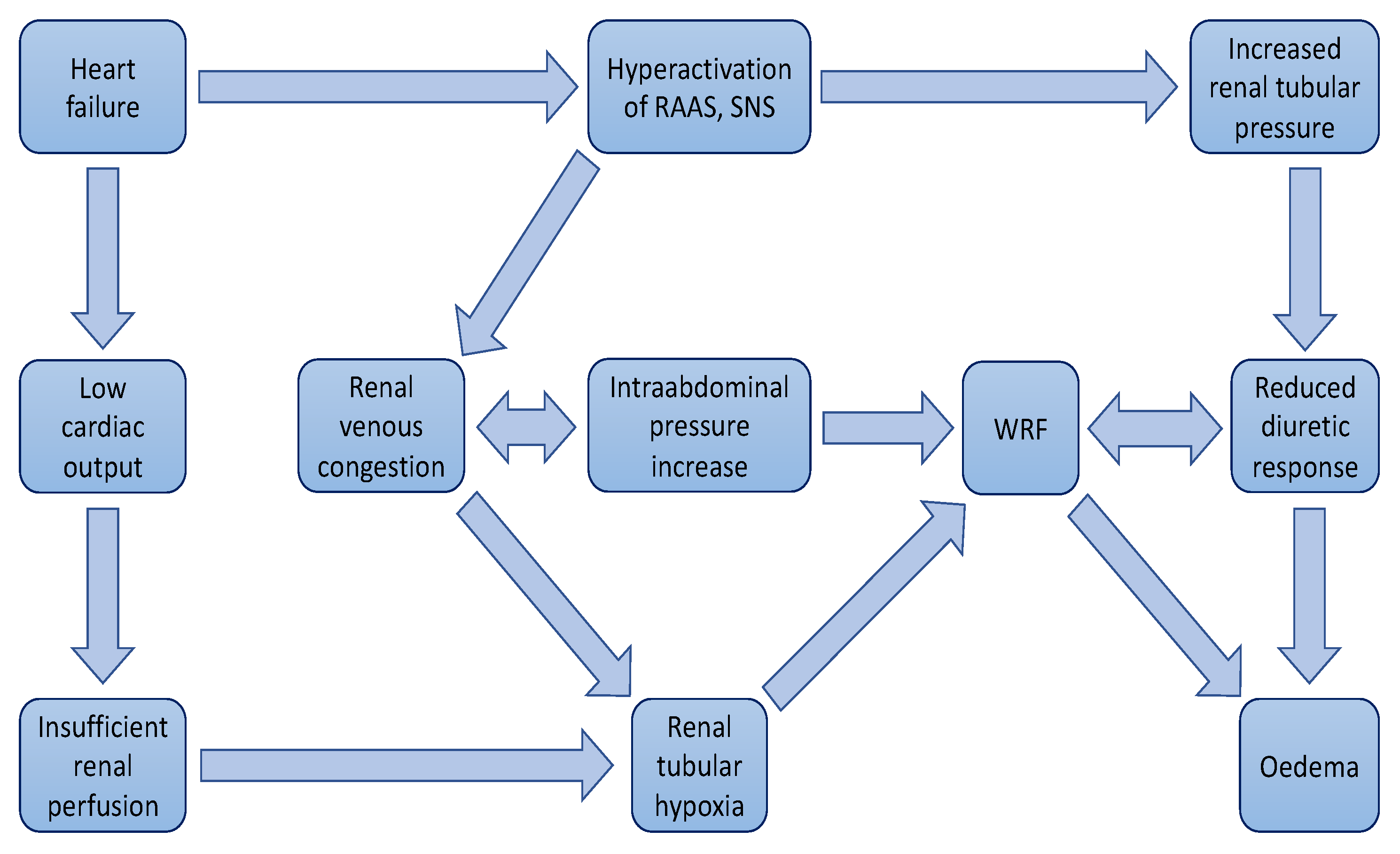
2.2. Understanding Fluid Retention and Resistance to Diuretics
2.3. Worsening of Renal Function and Cardiorenal Syndrome
2.4. Ultrafiltration
3. Clinical Studies
4. Conclusions
- In the case of congestion with volume overload consider loop diuretics, i/v root is preferable (at a dose of twice daily as an oral dose).
- Assess efficacy of diuretics by monitoring urine output and/or weight control.
- If no decongestive effect within the next 6 h—consider doubling the IV diuretic dose.
- If no decongestive effect within the next 6 h—UF should be considered.
5. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- O’Connor, C.M.; Stough, W.G.; Gallup, D.S.; Hasselblad, V.; Gheorghiade, M. Demographics, clinical characteristics, and outcomes of patients hospitalized for decompensated heart failure: Observations from the IMPACT-HF registry. J. Card. Fail. 2005, 11, 200–205. [Google Scholar] [CrossRef]
- Ambrosy, A.P.; Fonarow, G.C.; Butler, J.; Chioncel, O.; Greene, S.J.; Vaduganathan, M.; Nodari, S.; Lam, C.S.P.; Sato, N.; Shah, A.N.; et al. The global health and economic burden of hospitalizations for heart failure: Lessons learned from hospitalized heart failure registries. J. Am. Coll. Cardiol. 2014, 63, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Nieminen, M.S.; Brutsaert, D.; Dickstein, K.; Drexler, H.; Follath, F.; Harjola, V.P.; Hochadel, M.; Komajda, M.; Lassus, J.; Lopez-Sendon, J.L.; et al. EuroHeart Failure Survey II (EHFS II): A survey on hospitalized acute heart failure patients: Description of population. Eur. Heart J. 2006, 27, 2725–2736. [Google Scholar] [CrossRef]
- Setoguchi, S.; Stevenson, L.W.; Schneeweiss, S. Repeated hospitalizations predict mortality in the community population with heart failure. Am. Heart J. 2007, 154, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Crespo-Leiro, M.G.; Anker, S.D.; Maggioni, A.P.; Coats, A.J.; Filippatos, G.; Ruschitzka, F.; Ferrari, R.; Piepoli, M.F.; Delgado Jimenez, J.F.; Metra, M.; et al. European Society of Cardiology Heart Failure Long-Term Registry (ESC-HF-LT): 1-year follow-up outcomes and differences across regions. Eur. J. Heart Fail. 2016, 18, 613–625. [Google Scholar] [CrossRef]
- Opasich, C.; Rapezzi, C.; Lucci, D.; Gorini, M.; Pozzar, F.; Zanelli, E.; Tavazzi, L.; Maggioni, A.P.; Italian Network on Congestive Heart Failure (IN-CHF) Investigators. Precipitating factors and decision-making processes of short-term worsening heart failure despite “optimal” treatment (from the IN-CHF Registry). Am. J. Cardiol. 2001, 88, 382–387. [Google Scholar] [CrossRef]
- Lindner, A.; Charra, B.; Sherrard, D.J.; Scribner, B.H. Accelerated atherosclerosis in prolonged maintenance haemodialysis. N. Engl. J. Med. 1974, 290, 697–701. [Google Scholar] [CrossRef] [PubMed]
- Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; McCullough, P.A.; Kasiske, B.L.; Kelepouris, E.; Klag, M.J.; et al. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003, 108, 2154–2169. [Google Scholar] [CrossRef] [PubMed]
- McCullough, P.A.; Li, S.; Jurkovitz, C.T.; Stevens, L.A.; Wang, C.; Collins, A.J.; Chen, S.C.; Norris, K.C.; McFarlane, S.I.; Johnson, B.; et al. CKD and cardiovascular disease in screened high-risk volunteer and general populations: The Kidney Early Evaluation Program (KEEP) and National Health and Nutrition Examination Survey (NHANES) 1999–2004. Am. J. Kidney Dis. 2008, 51 (Suppl. 2), S38–S45. [Google Scholar] [CrossRef] [PubMed]
- Sarraf, M.; Masoumi, A.; Schrier, R.W. Cardiorenal syndrome in acute decompensated heart failure. Clin. J. Am. Soc. Nephrol. 2009, 4, 2013–2026. [Google Scholar] [CrossRef]
- Dries, D.L.; Exner, D.V.; Domanski, M.J.; Greenberg, B.; Stevenson, L.W. The prognostic implications of renal insufficiency in asymptomatic and symptomatic patients with left ventricular systolic dysfunction. J. Am. Coll. Cardiol. 2000, 35, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Testani, J.M.; McCauley, B.D.; Chen, J.; Shumski, M.; Shannon, R.P. Worsening renal function defined as an absolute increase in serum creatinine is a biased metric for the study of cardio-renal interactions. Cardiology 2010, 116, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Bongartz, L.G.; Cramer, M.J.; Doevendans, P.A.; Joles, J.A.; Braam, B. The severe cardiorenal syndrome: ‘Guyton revisited’. Eur. Heart J. 2005, 26, 11–17. [Google Scholar] [CrossRef]
- Brewster, U.C.; Setaro, J.F.; Perazella, M.A. The renin-angiotensin-aldosterone system: Cardiorenal effects and implications for renal and cardiovascular disease states. Am. J. Med. Sci. 2003, 326, 15–24. [Google Scholar] [CrossRef]
- Levin, A.; Thompson, C.R.; Ethier, J.; Carlisle, E.J.; Tobe, S.; Mendelssohn, D.; Burgess, E.; Jindal, K.; Barrett, B.; Singer, J.; et al. Left ventricular mass index increase in early renal disease: Impact of decline in hemoglobin. Am. J. Kidney Dis. 1999, 34, 125–134. [Google Scholar] [CrossRef]
- Silverberg, D.S.; Wexler, D.; Blum, M.; Keren, G.; Sheps, D.; Leibovitch, E.; Brosh, D.; Laniado, S.; Schwartz, D.; Yachnin, T.; et al. The use of subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe, resistant congestive heart failure improves cardiac and renal function and functional cardiac class, and markedly reduces hospitalizations. J. Am. Coll. Cardiol. 2000, 35, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Schrier, R.W. Body fluid volume regulation in health and disease: A unifying hypothesis. Ann. Intern. Med. 1990, 113, 155–159. [Google Scholar] [CrossRef]
- Ronco, C. Cardiorenal and renocardiac syndromes: Clinical disorders in search of a systematic definition. Int. J. Artif. Organs 2008, 31, 1–2. [Google Scholar] [CrossRef]
- Bekheirnia, M.R.; Schrier, R.W. Pathophysiology of water and sodium retention: Edematous states with normal kidney function. Curr. Opin. Pharmacol. 2006, 6, 202–207. [Google Scholar] [CrossRef]
- Verbrugge, F.H.; Grieten, L.; Mullens, W. Management of the cardiorenal syndrome in decompensated heart failure. Cardioren. Med. 2014, 4, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.L. Fluid Volume Overload and Congestion in Heart Failure: Time to Reconsider Pathophysiology and How Volume Is Assessed. Circ. Heart Fail. 2016, 9, e002922. [Google Scholar] [CrossRef] [PubMed]
- Burnett, J.C., Jr.; Opgenorth, T.J.; Granger, J.P. The renal action of atrial natriuretic peptide during control of glomerular filtration. Kidney Int. 1986, 30, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Richards, A.M. The renin-angiotensin-aldosterone system and the cardiac natriuretic peptides. Heart 1996, 76 (Suppl. 3), 36–44. [Google Scholar] [CrossRef]
- Melo, L.G.; Veress, A.T.; Ackermann, U.; Sonnenberg, H. Chronic regulation of arterial blood pressure by ANP: Role of endogenous vasoactive endothelial factors. Am. J. Physiol. 1998, 275, H1826–H1833. [Google Scholar] [CrossRef]
- Greene, S.J.; Gheorghiade, M.; Borlaug, B.A.; Pieske, B.; Vaduganathan, M.; Burnett, J.C.; Roessig, L., Jr.; Stasch, J.P.; Solomon, S.D.; Paulus, W.J.; et al. The cGMP signaling pathway as a therapeutic target in heart failure with preserved ejection fraction. J. Am. Heart Assoc. 2013, 2, e000536. [Google Scholar] [CrossRef]
- Schrier, R.W.; Abraham, W.T. Hormones and hemodynamics in heart failure. N. Engl. J. Med. 1999, 341, 577–585. [Google Scholar] [CrossRef]
- Gheorghiade, M.; Filippatos, G.; De Luca, L.; Burnett, J. Congestion in acute heart failure syndromes: An essential target of evaluation and treatment. Am. J. Med. 2006, 119 (Suppl. S1), S3–S10. [Google Scholar] [CrossRef]
- Zile, M.R.; Bennett, T.D.; St John Sutton, M.; Cho, Y.K.; Adamson, P.B.; Aaron, M.F.; Aranda, J.M.; Abraham, W.T., Jr.; Smart, F.W.; Stevenson, L.W.; et al. Transition from chronic compensated to acute decompensated heart failure: Pathophysiological insights obtained from continuous monitoring of intracardiac pressures. Circulation 2008, 118, 1433–1441. [Google Scholar] [CrossRef]
- Nijst, P.; Verbrugge, F.H.; Grieten, L.; Dupont, M.; Steels, P.; Tang, W.H.W.; Mullens, W. The pathophysiological role of interstitial sodium in heart failure. J. Am. Coll. Cardiol. 2015, 65, 378–388. [Google Scholar] [CrossRef]
- Gelman, S.; Warner, D.S.; Warner, M.A. Venous function and central venous pressure: A physiologic story. Anesthesiology 2008, 108, 735–748. [Google Scholar] [CrossRef]
- Miller, W.L.; Mullan, B.P. Understanding the heterogeneity in volume overload and fluid distribution in decompensated heart failure is key to optimal volume management: Role for blood volume quantitation. JACC Heart Fail. 2014, 2, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.M.; Wang, L.; Chau, E.; Chan, R.H.; Kong, S.L.; Tang, M.O.; Christensen, J.; Stadler, R.W.; Lau, C.P. Intrathoracic impedance monitoring in patients with heart failure: Correlation with fluid status and feasibility of early warning preceding hospitalization. Circulation 2005, 112, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Mentz, R.J.; Stevens, S.R.; DeVore, A.D.; Lala, A.; Vader, J.M.; AbouEzzeddine, O.F.; Khazanie, P.; Redfield, M.M.; Stevenson, L.W.; O’Connor, C.M.; et al. Decongestion strategies and renin-angiotensin-aldosterone system activation in acute heart failure. JACC Heart Fail. 2015, 3, 97–107. [Google Scholar] [CrossRef]
- Dovancescu, S.; Pellicori, P.; Mabote, T.; Torabi, A.; Clark, A.L.; Cleland, J.G.F. The effects of short-term omission of daily medication on the pathophysiology of heart failure. Eur. J. Heart Fail. 2017, 19, 643–649. [Google Scholar] [CrossRef]
- Fallick, C.; Sobotka, P.A.; Dunlap, M.E. Sympathetically mediated changes in capacitance: Redistribution of the venous reservoir as a cause of decompensation. Circ. Heart Fail. 2011, 4, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Geisberg, C.; Butler, J. Addressing the challenges of cardiorenal syndrome. Clevel. Clin. J. Med. 2006, 73, 485–491. [Google Scholar] [CrossRef]
- Oster, J.R.; Epstein, M.; Smoller, S. Combined therapy with thiazide-type and loop diuretic agents for resistant sodium retention. Ann. Intern. Med. 1983, 99, 405–406. [Google Scholar] [CrossRef]
- Koniari, K.; Nikolaou, M.; Paraskevaidis, I.; Parissis, J. Therapeutic options for the management of the cardiorenal syndrome. Int. J. Nephrol. 2010, 2011, 194910. [Google Scholar] [CrossRef]
- Salvador, D.R.; Rey, N.R.; Ramos, G.C.; Punzalan, F.E. Continuous infusion versus bolus injection of loop diuretics in congestive heart failure. Cochrane Database Syst. Rev. 2004, CD003178. [Google Scholar] [CrossRef]
- Brater, D.C. Diuretic therapy. N. Engl. J. Med. 1998, 339, 387–395. [Google Scholar] [CrossRef]
- Ronco, C.; Haapio, M.; House, A.A.; Anavekar, N.; Bellomo, R. Cardiorenal syndrome. J. Am. Coll. Cardiol. 2008, 52, 1527–1539. [Google Scholar] [CrossRef]
- Libetta, C.; Sepe, V.; Zucchi, M.; Pisacco, P.; Cosmai, L.; Meloni, F.; Campana, C.; Rampino, T.; Monti, C.; Tavazzi, L.; et al. Intermittent haemodiafiltration in refractory congestive heart failure: BNP and balance of inflammatory cytokines. Nephrol. Dial. Transplant. 2007, 22, 2013–2019. [Google Scholar] [CrossRef] [PubMed]
- Marenzi, G.; Lauri, G.; Grazi, M.; Assanelli, E.; Campodonico, J.; Agostoni, P. Circulatory response to fluid overload removal by extracorporeal ultrafiltration in refractory congestive heart failure. J. Am. Coll. Cardiol. 2001, 38, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Palevsky, P.M. Epidemiology of acute renal failure: The tip of the iceberg. Clin. J. Am. Soc. Nephrol. 2006, 1, 6–7. [Google Scholar] [CrossRef]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A.; Acute Kidney Injury Network. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P.; Acute Dialysis Quality Initiative workgroup. Acute renal failure—Definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [PubMed]
- Ledoux, P. Les cardio-rénaux [Cardiorenal syndrome]. Avenir Med. 1951, 48, 149–153. [Google Scholar]
- Silverberg, D. Outcomes of anaemia management in renal insufficiency and cardiac disease. Nephrol. Dial. Transplant. 2003, 18 (Suppl. 2), ii7–ii12. [Google Scholar]
- Dzau, V. The cardiovascular continuum and renin-angiotensin-aldosterone system blockade. J. Hypertens. 2005, 23, S9–S17. [Google Scholar] [CrossRef]
- Ronco, C.; Cicoira, M.; McCullough, P.A. Cardiorenal syndrome type 1: Pathophysiological crosstalk leading to combined heart and kidney dysfunction in the setting of acutely decompensated heart failure. J. Am. Coll. Cardiol. 2012, 60, 1031–1042. [Google Scholar] [CrossRef]
- Latchamsetty, R.; Fang, J.; Kline-Rogers, E.; Mukherjee, D.; Otten, R.F.; LaBounty, T.M.; Emery, M.S.; Eagle, K.A.; Froehlich, J.B. Prognostic value of transient and sustained increase in in-hospital creatinine on outcomes of patients admitted with acute coronary syndrome. Am. J. Cardiol. 2007, 99, 939–942. [Google Scholar] [CrossRef]
- Cowie, M.R.; Komajda, M.; Murray-Thomas, T.; Underwood, J.; Ticho, B.; POSH Investigators. Prevalence and impact of worsening renal function in patients hospitalized with decompensated heart failure: Results of the prospective outcomes study in heart failure (POSH). Eur. Heart J. 2006, 27, 1216–1222. [Google Scholar] [CrossRef]
- Ronco, C.; Bellomo, R.; McCullough, P.A. (Eds.) Cardiorenal Syndrome in Critical Care; Karger AG: Basel, Switzerland, 2010; p. 165. [Google Scholar] [CrossRef]
- Campbell, R.C.; Sui, X.; Filippatos, G.; Love, T.E.; Wahle, C.; Sanders, P.W.; Ahmed, A. Association of chronic kidney disease with outcomes in chronic heart failure: A propensity-matched study. Nephrol. Dial. Transplant. 2009, 24, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Roghi, A.; Savonitto, S.; Cavallini, C.; Arraiz, G.; Angoli, L.; Castriota, F.; Bernardi, G.; Sansa, M.; De Servi, S.; Pitscheider, W.; et al. Impact of acute renal failure following percutaneous coronary intervention on long-term mortality. J. Cardiovasc. Med. 2008, 9, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Kovesdy, C.P. Epidemiology of chronic kidney disease: An update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar] [CrossRef]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D.R. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef]
- Coresh, J.; Stevens, L.A.; Levey, A.S. Chronic kidney disease is common: What do we do next? Nephrol. Dial. Transplant. 2008, 23, 1122–1125. [Google Scholar] [CrossRef] [PubMed]
- Bagshaw, S.M.; Lapinsky, S.; Dial, S.; Arabi, Y.; Dodek, P.; Wood, G.; Ellis, P.; Guzman, J.; Marshall, J.; Parrillo, J.E.; et al. Acute kidney injury in septic shock: Clinical outcomes and impact of duration of hypotension prior to initiation of antimicrobial therapy. Intensive Care Med. 2009, 35, 871–881. [Google Scholar] [CrossRef]
- Bootsma, I.T.; Boerma, E.C.; Scheeren, T.W.L.; de Lange, F. The contemporary pulmonary artery catheter. Part 2: Measurements, limitations, and clinical applications. J. Clin. Monit. Comput. 2022, 36, 17–31. [Google Scholar] [CrossRef]
- Rodríguez-Espinosa, D.; Guzman-Bofarull, J.; De La Fuente-Mancera, J.C.; Maduell, F.; Broseta, J.J.; Farrero, M. Multimodal Strategies for the Diagnosis and Management of Refractory Congestion. An Integrated Cardiorenal Approach. Front. Physiol. 2022, 13, 913580. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- National Clinical Guideline Centre (UK). Acute Heart Failure: Diagnosing and Managing Acute Heart Failure in Adults; National Institute for Health and Care Excellence: London, UK, 2014; pp. 44,208–209. [Google Scholar]
- Writing Committee Members; ACC/AHA Joint Committee Members. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure. J. Card. Fail. 2022, 28, e1–e167. [Google Scholar] [CrossRef] [PubMed]
- Bart, B.A.; Goldsmith, S.R.; Lee, K.L.; Givertz, M.M.; O’Connor, C.M.; Bull, D.A.; Redfield, M.M.; Deswal, A.; Rouleau, J.L.; LeWinter, M.M.; et al. Ultrafiltration in decompensated heart failure with cardiorenal syndrome. N. Engl. J. Med. 2012, 367, 2296–2304. [Google Scholar] [CrossRef] [PubMed]
- Wobbe, B.; Wagner, J.; Szabó, D.K.; Rostás, I.; Farkas, N.; Garami, A.; Balaskó, M.; Hartmann, P.; Solymár, M.; Tenk, J.; et al. Ultrafiltration is better than diuretic therapy for volume-overloaded acute heart failure patients: A meta-analysis. Heart Fail. Rev. 2021, 26, 577–585. [Google Scholar] [CrossRef]
- Hu, J.; Wan, Q.; Zhang, Y.; Zhou, J.; Li, M.; Jiang, L.; Yuan, F. Efficacy and safety of early ultrafiltration in patients with acute decompensated heart failure with volume overload: A prospective, randomized, controlled clinical trial. BMC Cardiovasc. Disord. 2020, 20, 447. [Google Scholar] [CrossRef]
- Marenzi, G.; Muratori, M.; Cosentino, E.R.; Rinaldi, E.R.; Donghi, V.; Milazzo, V.; Ferramosca, E.; Borghi, C.; Santoro, A.; Agostoni, P. Continuous ultrafiltration for congestive heart failure: The CUORE trial. J. Card. Fail. 2014, 20, 9–17. [Google Scholar] [CrossRef]
- Costanzo, M.R.; Negoianu, D.; Jaski, B.E.; Bart, B.A.; Heywood, J.T.; Anand, I.S.; Smelser, J.M.; Kaneshige, A.M.; Chomsky, D.B.; Adler, E.D.; et al. Aquapheresis Versus Intravenous Diuretics and Hospitalizations for Heart Failure. JACC Heart Fail. 2016, 4, 95–105. [Google Scholar] [CrossRef]
- Costanzo, M.R.; Guglin, M.E.; Saltzberg, M.T.; Jessup, M.L.; Bart, B.A.; Teerlink, J.R.; Jaski, B.E.; Fang, J.C.; Feller, E.D.; Haas, G.J.; et al. Ultrafiltration versus intravenous diuretics for patients hospitalized for acute decompensated heart failure. J. Am. Coll. Cardiol. 2007, 49, 675–683. [Google Scholar] [CrossRef]
- Srivastava, M.; Harrison, N.; Caetano, A.F.S.; Tan, A.R.; Law, M. Ultrafiltration for acute heart failure. Cochrane Database Syst. Rev. 2022, 1, CD013593. [Google Scholar] [CrossRef]
- Shi, X.; Bao, J.; Zhang, H.; Wang, H.; Li, L.; Zhang, Y. Patients with high-dose diuretics should get ultrafiltration in the management of decompensated heart failure: A meta-analysis. Heart Fail. Rev. 2019, 24, 927–940. [Google Scholar] [CrossRef] [PubMed]
- Ong, L.T. Evidence based review of management of cardiorenal syndrome type 1. World J. Methodol. 2021, 11, 187–198. [Google Scholar] [CrossRef]
- Wang, M.J.; Zheng, Y.M.; Jin, H.X. Ultrafiltration for patients with acute decompensated heart failure: A systematic review and meta-analysis. Medicine 2021, 100, e28029. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Shen, C.; Lu, J.; Xu, F.; Tong, J.; Jiang, J.; Fu, G. Early continuous ultrafiltration in Chinese patients with congestive heart failure (EUC-CHF): Study protocol for an open-label registry-based prospective clinical trial. BMC Cardiovasc. Disord. 2019, 19, 249. [Google Scholar] [CrossRef] [PubMed]
- Grodin, J.L.; Carter, S.; Bart, B.A.; Goldsmith, S.R.; Drazner, M.H.; Tang, W.H.W. Direct comparison of ultrafiltration to pharmacological decongestion in heart failure: A per-protocol analysis of CARRESS-HF. Eur. J. Heart Fail. 2018, 20, 1148–1156. [Google Scholar] [CrossRef]
- Fudim, M.; Brooksbank, J.; Giczewska, A.; Greene, S.J.; Grodin, J.L.; Martens, P.; Ter Maaten, J.M.; Sharma, A.; Verbrugge, F.H.; Chakraborty, H.; et al. Ultrafiltration in Acute Heart Failure: Implications of Ejection Fraction and Early Response to Treatment From CARRESS-HF. J. Am. Heart Assoc. 2020, 9, e015752. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.; Douglas, H.; Wong, C. Cardio-nephrology MDT meetings play an important role in the management of cardiorenal syndrome. Br. J. Cardiol. 2020, 27, 26. [Google Scholar] [CrossRef]
- Joseph, M.S.; Palardy, M.; Bhave, N.M. Management of heart failure in patients with end-stage kidney disease on maintenance dialysis: A practical guide. Rev. Cardiovasc. Med. 2020, 21, 31–39. [Google Scholar] [CrossRef]
- Pickup, L.; Radhakrishnan, A.; Townend, J.N.; Ferro, C.J. Arterial stiffness in chronic kidney disease: A modifiable cardiovascular risk factor? Curr. Opin. Nephrol. Hypertens. 2019, 28, 527–536. [Google Scholar] [CrossRef]
- Voicehovska, J.G.; Bormane, E.; Grigane, A.; Moisejevs, G.; Moreino, E.; Trumpika, D.; Voicehovskis, V.V. Association of arterial stiffness with chronic kidney disease progression and mortality. Heart Lung Circ. 2021, 30, 1694–1701. [Google Scholar] [CrossRef]


{kind=link}
| First Author, Year | Study Type | Primary Outcomes | Results |
|---|---|---|---|
| Bart et al., 2012 [66] | Multicentred, prospective, RCT CARRESS-HF study | Change in serum creatinine level and change in weight. | UF is associated with more adverse events, WRF, and no change in weight. |
| Wobbe et al., 2021 [67] | Meta-analysis (PRISMA protocol) | Fluid removal, weight loss, all-cause mortality, heart failure-related rehospitalization, or adverse events. | UF increases fluid removal and weight loss and reduces rehospitalization. |
| Hu et al., 2020 [68] | RCT | Weight loss and an increase in urine output on days 4 and 8 of treatment. | Early UF is superior to diuretics for volume overload treatment initiation for ADHF patients. |
| Marenzi et al., 2014 [69] | RCT The CUORE trial | Rehospitalizations for congestive HF during a 1-year follow-up. | Clinical stabilization and less rehospitalization. |
| Costanzo et al., 2016 [70] | RCT The AVOID-HF | Time to first HF event within 90 days after discharge from index hospitalization. | UF group trended toward a longer time to first HF event within 90 days and had fewer HF and cardiovascular events. |
| Costanzo et al., 2007 [71] | RCT The UNLOAD trial | Weight loss and dyspnoea assessment at 48 h after randomization. | UF safely produces greater weight and fluid loss than intravenous diuretics. |
| Srivastava et al., 2022 [72] | Systematic search, RCT | Mortality and rehospitalisation rates. | UF probably reduces heart failure-related rehospitalisation in the long term. |
| Shi et al., 2019 [73] | RCT meta-analysis | Weight change, length of hospital stays, rehospitalization for HF, mortality, change in serum creatinine, dialysis dependence, and adverse outcomes. | UF was associated with significant reduction in the rate of rehospitalization. |
| Ong et al., 2021 [74] | Systematic search, RCT and observation studies | Changes in renal function tests. | Pharmacological therapy is recommended as the first-line therapy, and UF should only be reserved in cases of refractory congestion. |
| Wang et al., 2021 [75] | Systematic review and meta-analysis | Heart failure rehospitalization, all-cause rehospitalization, and mortality. | Although UF is more effective in removing fluids than diuretics and decrease rehospitalization due to HF and all causes, there is not enough evidence to prove that UF is superior because of adverse events and mortality in the UF group. |
| Yang et al., 2019 [76] | Open-label, registry-based, prospective study (EUC-CHF) | Changes of weight loss and dyspnoea severity score. | EUC-CHF is one of the first controlled trials tailored to determine the benefit of UF with 24 h from hospital admission. Results are pending. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Voicehovska, J.G.; Trumpika, D.; Voicehovskis, V.V.; Bormane, E.; Bušmane, I.; Grigane, A.; Moreino, E.; Lejnieks, A. Cardiovascular Consequences of Acute Kidney Injury: Treatment Options. Biomedicines 2023, 11, 2364. https://doi.org/10.3390/biomedicines11092364
Voicehovska JG, Trumpika D, Voicehovskis VV, Bormane E, Bušmane I, Grigane A, Moreino E, Lejnieks A. Cardiovascular Consequences of Acute Kidney Injury: Treatment Options. Biomedicines. 2023; 11(9):2364. https://doi.org/10.3390/biomedicines11092364
Chicago/Turabian StyleVoicehovska, Julija G., Dace Trumpika, Vladimirs V. Voicehovskis, Eva Bormane, Inara Bušmane, Anda Grigane, Eva Moreino, and Aivars Lejnieks. 2023. "Cardiovascular Consequences of Acute Kidney Injury: Treatment Options" Biomedicines 11, no. 9: 2364. https://doi.org/10.3390/biomedicines11092364