
Decreased Platelet Aggregation in Patients with Decompensated Liver Cirrhosis and TIPS Implantation
 and
and
Abstract
:1. Introduction
2. Materials and Methods
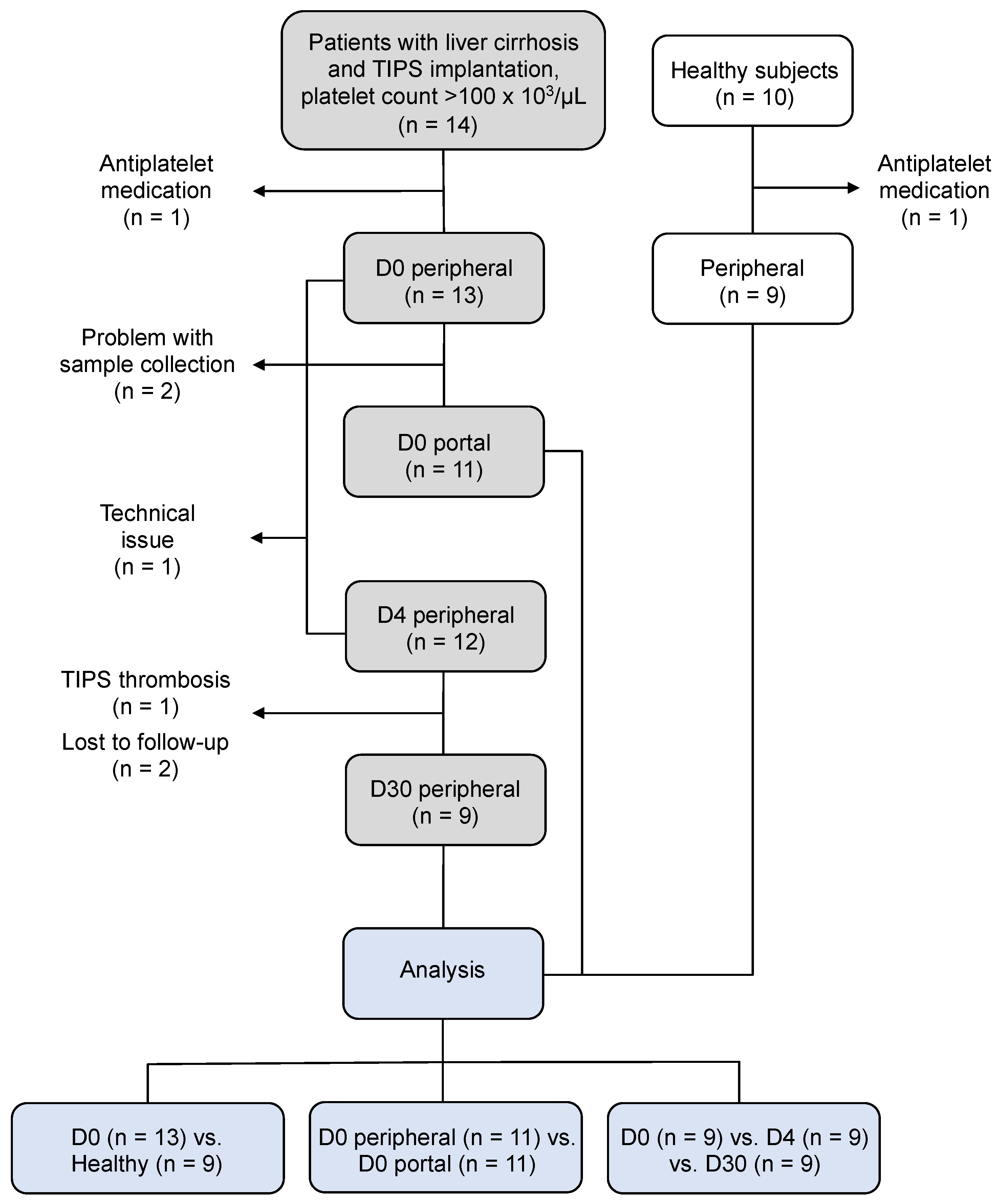
2.1. Study Design
2.2. Whole-Blood Impedance Aggregometry (WBIA)
2.3. Light Transmission Aggregometry (LTA)
2.4. Flow Cytometry
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
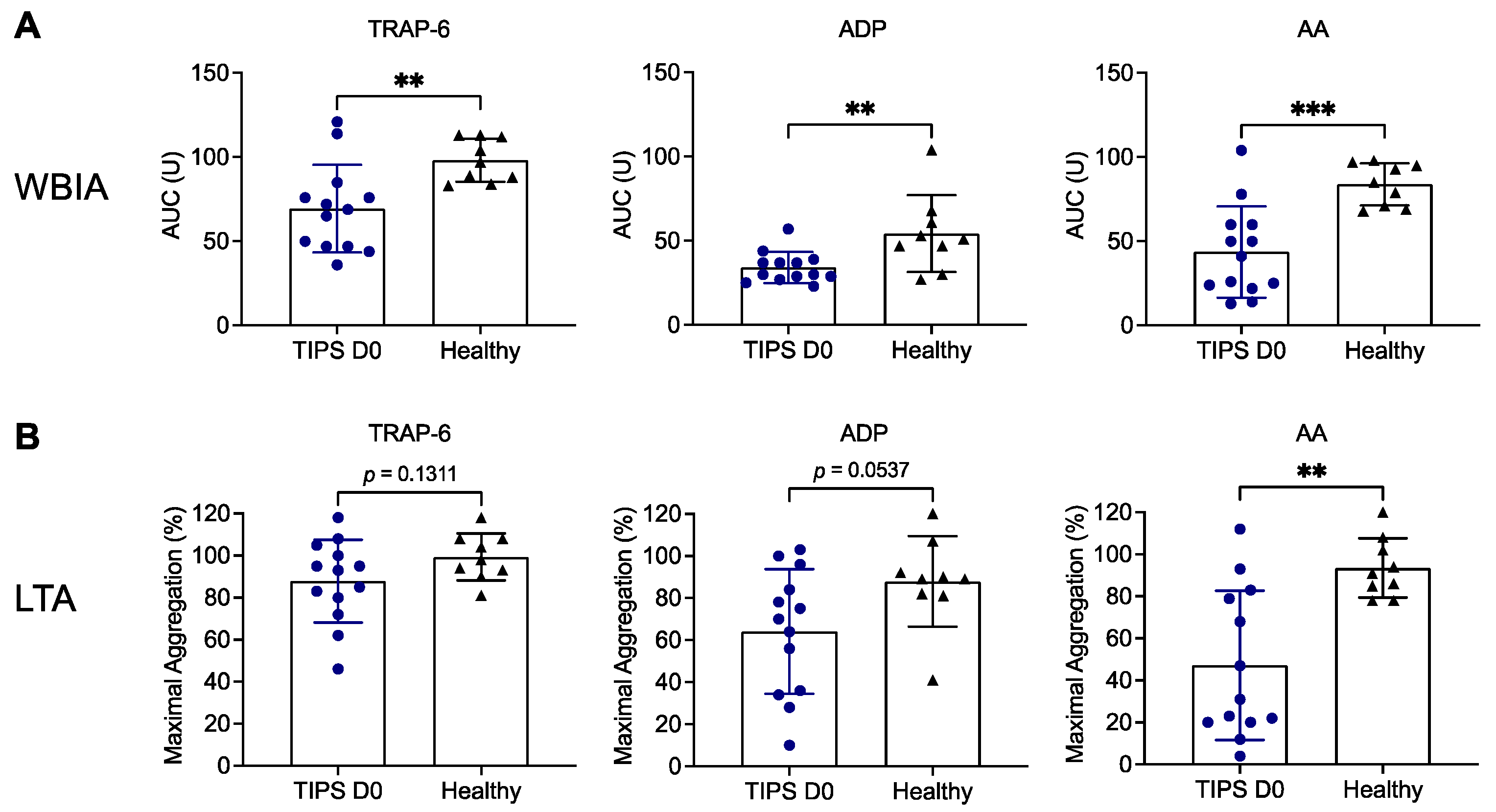
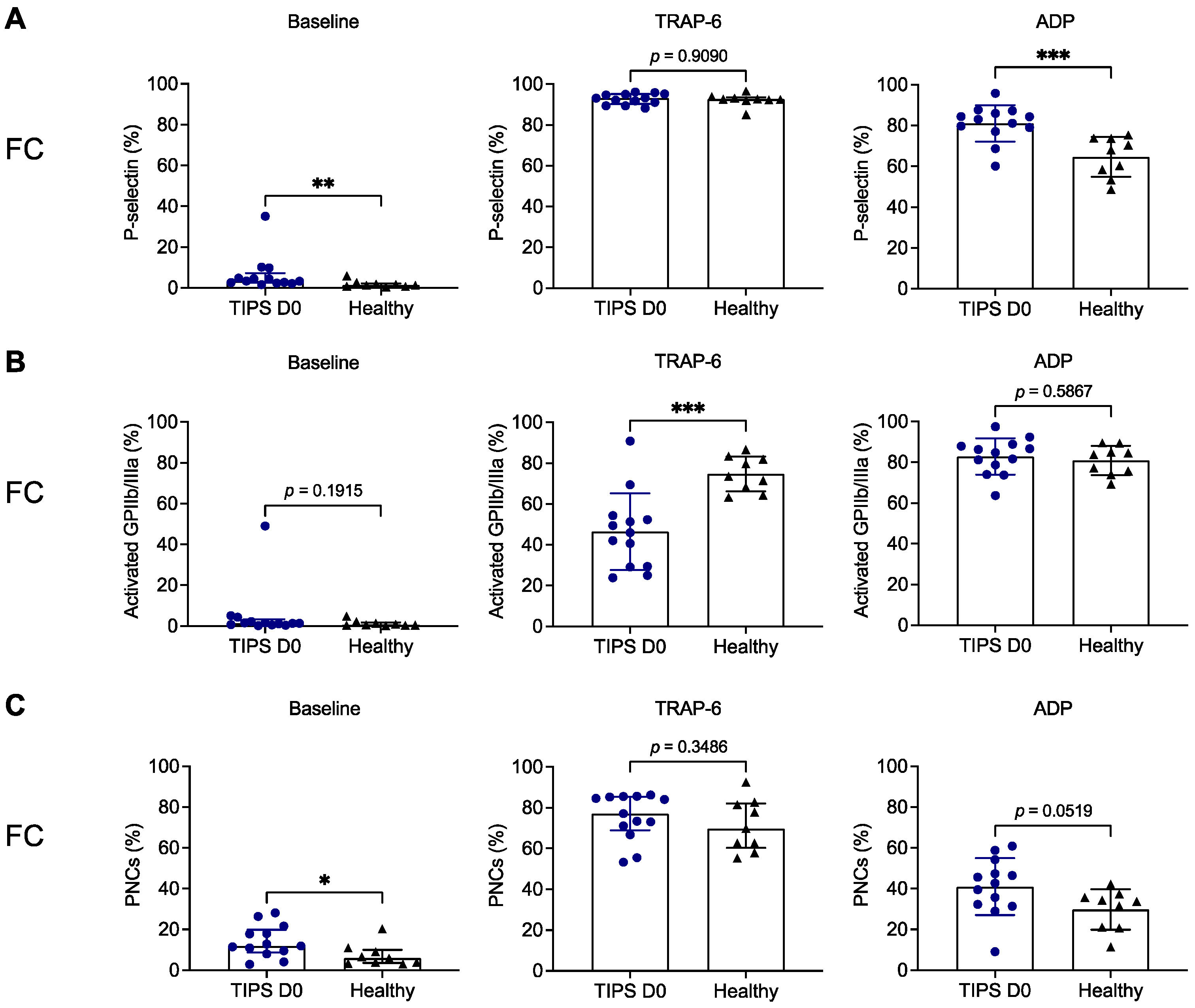
3.2. Platelet Aggregation Is Decreased in Patients with Liver Cirrhosis Prior to TIPS Implantation
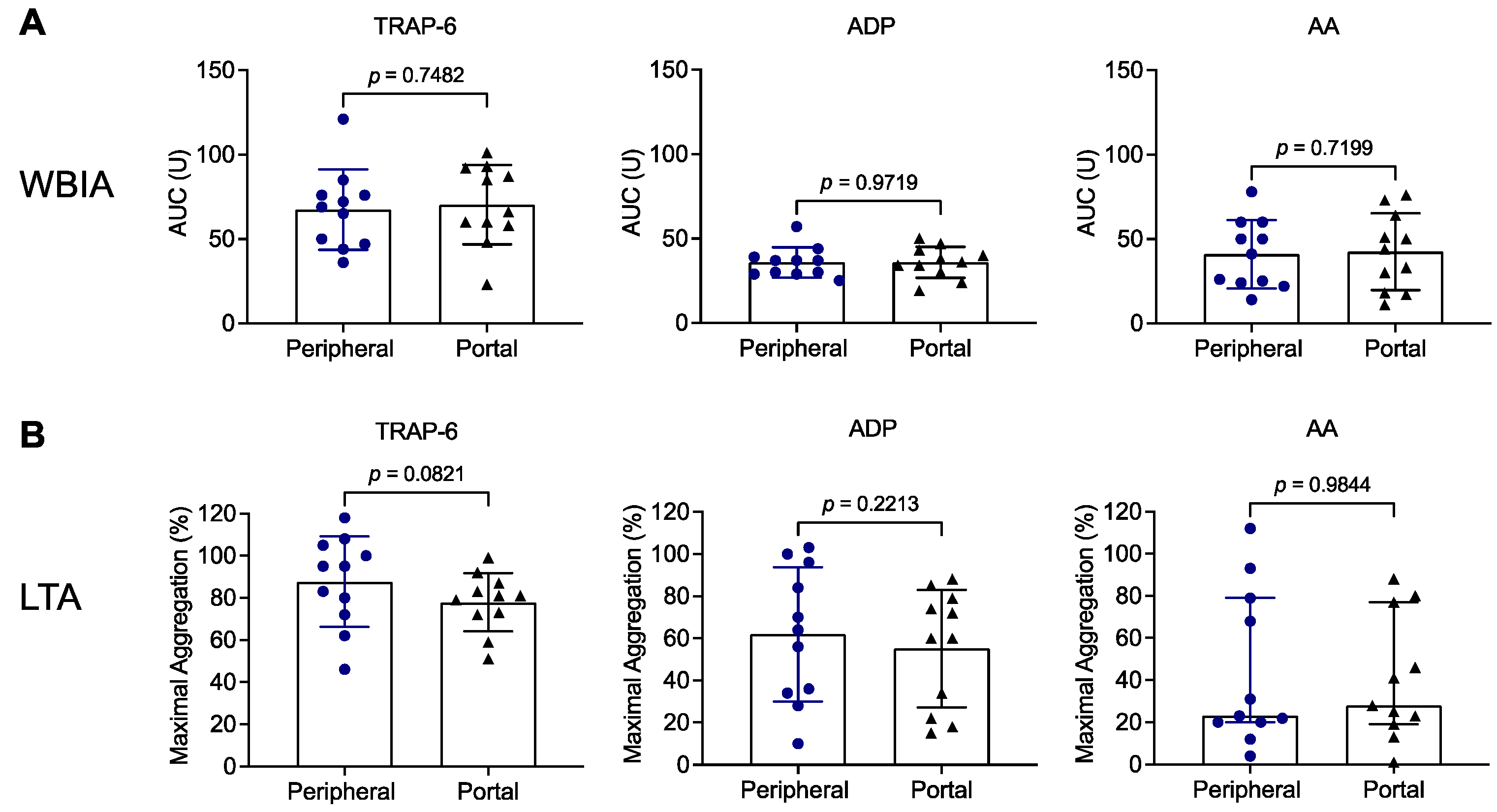
3.3. Results Do Not Differ between Peripheral and Portal-Vein Blood of Patients with Liver Cirrhosis Prior to TIPS Implantation
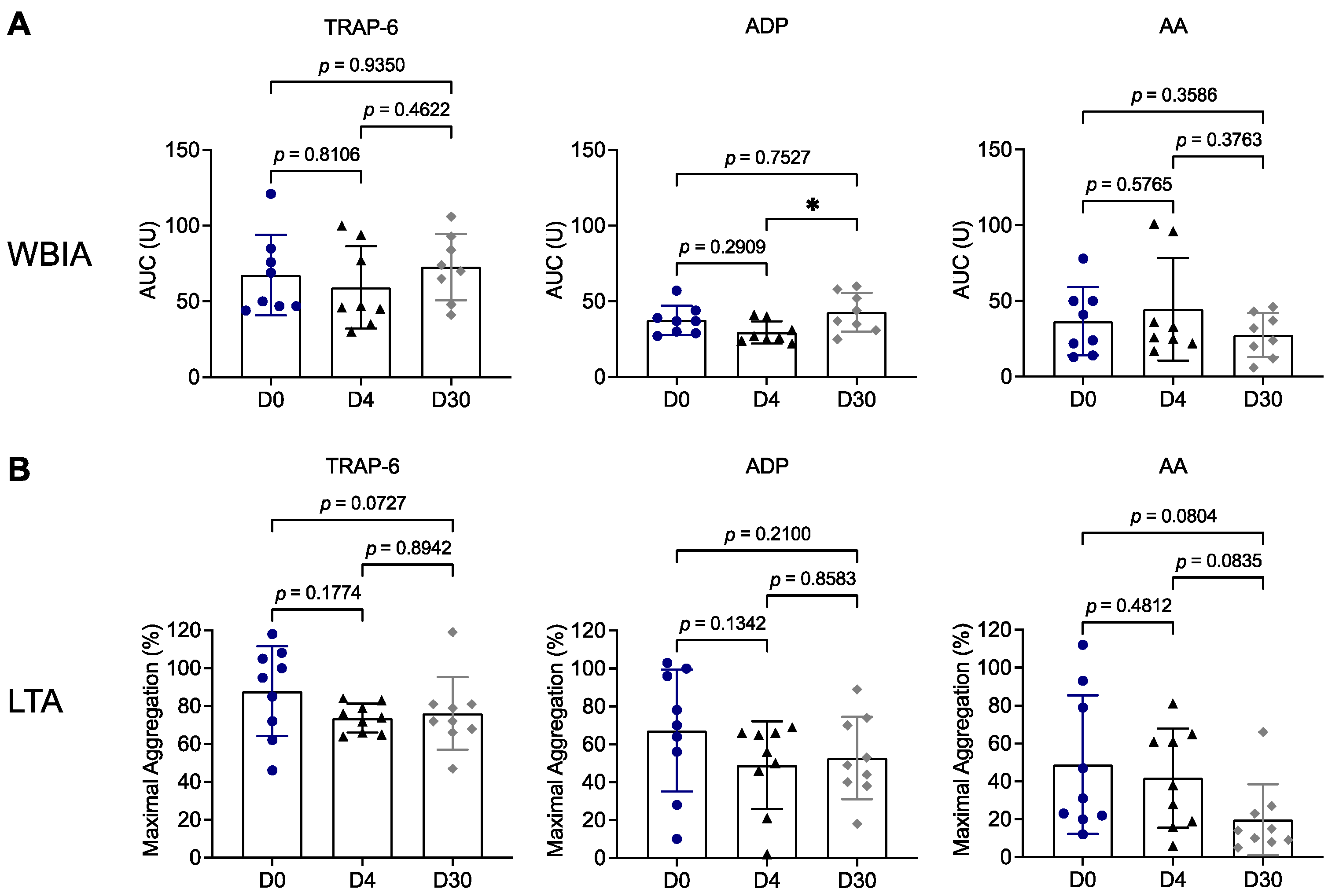
3.4. Platelet Aggregation Remains Impaired throughout the 30-Day Follow-Up after TIPS Implantation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Healthcare Access and Quality Collaborators. Assessing performance of the Healthcare Access and Quality Index, overall and by select age groups, for 204 countries and territories, 1990–2019: A systematic analysis from the Global Burden of Disease Study 2019. Lancet Glob. Health 2022, 10, e1715–e1743. [Google Scholar] [CrossRef] [PubMed]
- Gu, W.; Hortlik, H.; Erasmus, H.P.; Schaaf, L.; Zeleke, Y.; Uschner, F.E.; Ferstl, P.; Schulz, M.; Peiffer, K.H.; Queck, A.; et al. Trends and the course of liver cirrhosis and its complications in Germany: Nationwide population-based study (2005 to 2018). Lancet Reg. Health Eur. 2022, 12, 100240. [Google Scholar] [CrossRef] [PubMed]
- Iwakiri, Y.; Trebicka, J. Portal hypertension in cirrhosis: Pathophysiological mechanisms and therapy. JHEP Rep. 2021, 3, 100316. [Google Scholar] [CrossRef] [PubMed]
- Jalan, R.; D’Amico, G.; Trebicka, J.; Moreau, R.; Angeli, P.; Arroyo, V. New clinical and pathophysiological perspectives defining the trajectory of cirrhosis. J. Hepatol. 2021, 75 (Suppl. S1), S14–S26. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, G.; Bernardi, M.; Angeli, P. Towards a new definition of decompensated cirrhosis. J. Hepatol. 2022, 76, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Bettinger, D.; Thimme, R.; Schultheiss, M. Implantation of transjugular intrahepatic portosystemic shunt (TIPS): Indication and patient selection. Curr. Opin. Gastroenterol. 2022, 38, 221–229. [Google Scholar] [CrossRef]
- Buttner, L.; Aigner, A.; Pick, L.; Brittinger, J.; Steib, C.J.; Boning, G.; Streitparth, F. 25 years of experience with transjugular intrahepatic portosystemic shunt (TIPS): Changes in patient selection and procedural aspects. Insights Imaging 2022, 13, 73. [Google Scholar] [CrossRef]
- Meyer, C.; Paar Perez, A.M.; Chang, J.; Sprinkart, A.M.; Bohling, N.; Luu, A.M.; Kutting, D.; Jansen, C.; Luetkens, J.; Bischoff, L.M.; et al. Cranial stent position is independently associated with the development of TIPS dysfunction. Sci. Rep. 2022, 12, 3559. [Google Scholar] [CrossRef]
- Steib, C.J.; Li, H.; Zhang, J.; Mayerle, J.; Ricke, J.; Gerbes, A.L.; Meyer, C.; Zipprich, A.; Trebicka, J. Transjugular intrahepatic portosystemic shunt for patients with liver cirrhosis: Survey evaluating indications, standardization of procedures and anticoagulation in 43 German hospitals. Eur. J. Gastroenterol. Hepatol. 2020, 32, 1179–1185. [Google Scholar] [CrossRef]
- Violi, F.; Pignatelli, P.; Cammisotto, V. Platelet defetcts in cirrhosis: Fact or fiction? J. Hepatol. 2023, 76, 1291–1305. [Google Scholar] [CrossRef]
- Zanetto, A.; Campello, E.; Bulato, C.; Gavasso, S.; Saggiorato, G.; Shalaby, S.; Burra, P.; Angeli, P.; Senzolo, M.; Simioni, P. Global hemostatic profiling in patients with decompensated cirrhosis and bacterial infections. JHEP Rep. 2022, 4, 100493. [Google Scholar] [CrossRef] [PubMed]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Bettinger, D.; Sturm, L.; Pfaff, L.; Hahn, F.; Kloeckner, R.; Volkwein, L.; Praktiknjo, M.; Lv, Y.; Han, G.; Huber, J.P.; et al. Refining prediction of survival after TIPS with the novel Freiburg index of post-TIPS survival. J. Hepatol. 2021, 74, 1362–1372. [Google Scholar] [CrossRef]
- Rossle, M. TIPS: 25 years later. J. Hepatol. 2013, 59, 1081–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scharf, R.E. Thrombocytopenia and Hemostatic Changes in Acute and Chronic Liver Disease: Pathophysiology, Clinical and Laboratory Features, and Management. J. Clin. Med. 2021, 10, 1530. [Google Scholar] [CrossRef] [PubMed]
- Violi, F.; Basili, S.; Raparelli, V.; Chowdary, P.; Gatt, A.; Burroughs, A.K. Patients with liver cirrhosis suffer from primary haemostatic defects? Fact or fiction? J. Hepatol. 2011, 55, 1415–1427. [Google Scholar] [CrossRef] [Green Version]
- Witters, P.; Freson, K.; Verslype, C.; Peerlinck, K.; Hoylaerts, M.; Nevens, F.; Van Geet, C.; Cassiman, D. Review article: Blood platelet number and function in chronic liver disease and cirrhosis. Aliment. Pharmacol. Ther. 2008, 27, 1017–1029. [Google Scholar] [CrossRef]
- Shalaby, S.; Zanetto, A.; Campello, E.; Gavasso, S.; Barbiero, G.; Battistel, M.; Feltracco, P.; Bizzaro, D.; Burra, P.; Simioni, P.; et al. Reply to “Peripheral versus central venous blood sampling does not influence the assessment of platelet activation in cirrhosis”. Platelets 2022, 33, 1104–1106. [Google Scholar] [CrossRef]
- Zanetto, A.; Campello, E.; Bulato, C.; Gavasso, S.; Farinati, F.; Russo, F.P.; Tormene, D.; Burra, P.; Senzolo, M.; Simioni, P. Increased platelet aggregation in patients with decompensated cirrhosis indicates higher risk of further decompensation and death. J. Hepatol. 2022, 77, 660–669. [Google Scholar] [CrossRef]
- Cattaneo, M. Light transmission aggregometry and ATP release for the diagnostic assessment of platelet function. Semin. Thromb. Hemost. 2009, 35, 158–167. [Google Scholar] [CrossRef]
- Femia, E.A.; Scavone, M.; Lecchi, A.; Cattaneo, M. Effect of platelet count on platelet aggregation measured with impedance aggregometry (Multiplate analyzer) and with light transmission aggregometry. J. Thromb. Haemost. 2013, 11, 2193–2196. [Google Scholar] [CrossRef]
- Hanke, A.A.; Roberg, K.; Monaca, E.; Sellmann, T.; Weber, C.F.; Rahe-Meyer, N.; Gorlinger, K. Impact of platelet count on results obtained from multiple electrode platelet aggregometry (Multiplate). Eur. J. Med. Res. 2010, 15, 214–219. [Google Scholar] [CrossRef] [Green Version]
- Stissing, T.; Dridi, N.P.; Ostrowski, S.R.; Bochsen, L.; Johansson, P.I. The influence of low platelet count on whole blood aggregometry assessed by Multiplate. Clin. Appl. Thromb. Hemost. 2011, 17, E211–E217. [Google Scholar] [CrossRef] [PubMed]
- Scavone, M.; Podda, G.M.; Tripodi, A.; Cattaneo, M. Whole blood platelet aggregation measurement by Multiplate: Potential diagnostic inaccuracy of correcting the results for the sample platelet count. Platelets 2023, 34, 2156493. [Google Scholar] [CrossRef] [PubMed]
- Laffi, G.; Cominelli, F.; Ruggiero, M.; Fedi, S.; Chiarugi, V.P.; La Villa, G.; Pinzani, M.; Gentilini, P. Altered platelet function in cirrhosis of the liver: Impairment of inositol lipid and arachidonic acid metabolism in response to agonists. Hepatology 1988, 8, 1620–1626. [Google Scholar] [CrossRef]
- Laffi, G.; Marra, F.; Gresele, P.; Romagnoli, P.; Palermo, A.; Bartolini, O.; Simoni, A.; Orlandi, L.; Selli, M.L.; Nenci, G.G.; et al. Evidence for a storage pool defect in platelets from cirrhotic patients with defective aggregation. Gastroenterology 1992, 103, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Vinholt, P.J.; Hvas, A.M.; Nielsen, C.; Soderstrom, A.C.; Sprogoe, U.; Fialla, A.D.; Nybo, M. Reduced platelet activation and platelet aggregation in patients with alcoholic liver cirrhosis. Platelets 2018, 29, 520–527. [Google Scholar] [CrossRef]
- Rieder, M.; Baldus, N.; Stallmann, D.; Jeserich, M.; Goller, I.; Wirth, L.; Pollmeier, L.; Hofmann, M.; Bode, C.; Busch, H.J.; et al. Early SARS-CoV-2 infection: Platelet-neutrophil complexes and platelet function. Res. Pract. Thromb. Haemost. 2023, 7, 100025. [Google Scholar] [CrossRef] [PubMed]
- Weiss, L.J.; Drayss, M.; Manukjan, G.; Zeitlhofler, M.; Kleiss, J.; Weigel, M.; Herrmann, J.; Mott, K.; Beck, S.; Burkard, P.; et al. Uncoupling of platelet granule release and integrin activation suggests GPIIb/IIIa as a therapeutic target in COVID-19. Blood Adv. 2023, 7, 2324–2338. [Google Scholar] [CrossRef]
- Weiss, L.J.; Manukjan, G.; Pflug, A.; Winter, N.; Weigel, M.; Nagler, N.; Kredel, M.; Lam, T.T.; Nieswandt, B.; Weismann, D.; et al. Acquired platelet GPVI receptor dysfunction in critically ill patients with sepsis. Blood 2021, 137, 3105–3115. [Google Scholar] [CrossRef]
- Queck, A.; Carnevale, R.; Uschner, F.E.; Schierwagen, R.; Klein, S.; Jansen, C.; Meyer, C.; Praktiknjo, M.; Thomas, D.; Strassburg, C.; et al. Role of portal venous platelet activation in patients with decompensated cirrhosis and TIPS. Gut 2020, 69, 1535–1536. [Google Scholar] [CrossRef] [Green Version]
- Raparelli, V.; Basili, S.; Carnevale, R.; Napoleone, L.; Del Ben, M.; Nocella, C.; Bartimoccia, S.; Lucidi, C.; Talerico, G.; Riggio, O.; et al. Low-grade endotoxemia and platelet activation in cirrhosis. Hepatology 2017, 65, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Ogasawara, F.; Fusegawa, H.; Haruki, Y.; Shiraishi, K.; Watanabe, N.; Matsuzaki, S. Platelet activation in patients with alcoholic liver disease. Tokai J. Exp. Clin. Med. 2005, 30, 41–48. [Google Scholar] [PubMed]
- Xianghong, G.; Guanping, C.; Fenghua, Y.; Jiayin, W. Changes in platelet functional parameters and CD62 P expression in liver cirrhosis. Afr. Health Sci. 2013, 13, 1079–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kannan, M.; Ahmad, F.; Saxena, R. Platelet activation markers in evaluation of thrombotic risk factors in various clinical settings. Blood Rev. 2019, 37, 100583. [Google Scholar] [CrossRef]
- Hassouna, M.M.; Mostafa, M.S.; Omar, H.M.; Mohammed, E.A.; Abdallah, H.M. Platelet transfusion in patients with liver cirrhosis cross-talk with neutrophil: Prospective study. Hematol. Transfus. Cell Ther. 2022. [Google Scholar] [CrossRef]
- Stoy, S.; Patel, V.C.; Sturgeon, J.P.; Manakkat Vijay, G.K.; Lisman, T.; Bernal, W.; Shawcross, D.L. Platelet-leucocyte aggregation is augmented in cirrhosis and further increased by platelet transfusion. Aliment. Pharmacol. Ther. 2018, 47, 1375–1386. [Google Scholar] [CrossRef] [Green Version]
- Brusilovskaya, K.; Simbrunner, B.; Lee, S.; Eichelberger, B.; Bauer, D.; Zinober, K.; Schwabl, P.; Mandorfer, M.; Panzer, S.; Reiberger, T.; et al. Peripheral versus central venous blood sampling does not influence the assessment of platelet activation in cirrhosis. Platelets 2022, 33, 879–886. [Google Scholar] [CrossRef]
- Nguyen, A.; Gemmell, C.H.; Yeo, E.L.; Packham, M.A.; Rand, M.L. Ethanol inhibits thrombin-induced secretion of the contents of human platelet dense and alpha-granules and lysosomes. Thromb. Haemost. 1998, 80, 662–667. [Google Scholar]
- Renaud, S.C.; Ruf, J.C. Effects of alcohol on platelet functions. Clin. Chim. Acta 1996, 246, 77–89. [Google Scholar] [CrossRef]
- Scharf, R.E.; Aul, C. Alcohol-induced disorders of the hematopoietic system. Z. Gastroenterol. 1988, 26 (Suppl. S3), 75–83. [Google Scholar] [PubMed]
- Luo, S.H.; Chu, J.G.; Huang, H.; Yao, K.C. Effect of initial stent position on patency of transjugular intrahepatic portosystemic shunt. World J. Gastroenterol. 2017, 23, 4779–4787. [Google Scholar] [CrossRef] [PubMed]
- Buechter, M.; Manka, P.; Gerken, G.; Canbay, A.; Blomeyer, S.; Wetter, A.; Altenbernd, J.; Kahraman, A.; Theysohn, J.M. Transjugular Intrahepatic Portosystemic Shunt in Patients with Portal Hypertension: Patency Depends on Coverage and Interventionalist’s Experience. Dig. Dis. 2018, 36, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Bureau, C.; Garcia Pagan, J.C.; Layrargues, G.P.; Metivier, S.; Bellot, P.; Perreault, P.; Otal, P.; Abraldes, J.G.; Peron, J.M.; Rousseau, H.; et al. Patency of stents covered with polytetrafluoroethylene in patients treated by transjugular intrahepatic portosystemic shunts: Long-term results of a randomized multicentre study. Liver Int. 2007, 27, 742–747. [Google Scholar] [CrossRef]
- Gerbes, A.L.; Labenz, J.; Appenrodt, B.; Dollinger, M.; Gundling, F.; Gulberg, V.; Holstege, A.; Lynen-Jansen, P.; Steib, C.J.; Trebicka, J.; et al. Updated S2k-Guideline “Complications of liver cirrhosis”. German Society of Gastroenterology (DGVS). Z. Gastroenterol. 2019, 57, 611–680. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Patients D0 (n = 13) | Healthy Subjects (n = 9) |
|---|---|---|
| Male | 10 (76.9%) | 7 (77.8%) |
| Age (y) | 61 ± 13 | 40 ± 5 |
| Etiology | ||
| Alcoholic | 11 (84.6%) | |
| Hemochromatosis | 1 (7.7%) | |
| Primary biliary cirrhosis | 1 (7.7%) | |
| Indication for TIPS implantation | ||
| Recurrent ascites | 8 (61.5%) | |
| Secondary prophylaxis of variceal bleeding | 5 (38.5%) | |
| Clinical scores | ||
| Child–Pugh Score | 7 (6–9) | |
| A | 5 (38.5%) | |
| B | 7 (53.8%) | |
| C | 1 (7.7%) | |
| FIPS 1 | 0.07 (−0.78–0.53) | |
| Low risk | 12 (92.3%) | |
| High risk | 1 (7.7%) | |
| Laboratory parameters | ||
| Hemoglobin (g/dL) | 10.8 ± 1.8 | |
| White blood cell count (×103/µL) | 7.9 ± 2.6 | |
| Platelets (×103/µL) | 173 ± 50 | |
| INR 2 | 1.26 ± 0.12 | |
| PTT 3 | 38 ± 6 | |
| Creatinine (mg/dL) | 0.9 (0.7–1.5) | |
| Bilirubin (mg/dL) | 1.4 (1.0–2.6) | |
| Albumin (g/L) | 30 (28–35) | |
| AST 4 (U/L) | 62 ± 24 | |
| ALT 5 (U/L) | 27 (22–54) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nassar, A.; Huber, J.P.; Stallmann, D.; Sharipova, D.; Hamad, M.A.; Schultheiss, M.; Thimme, R.; Duerschmied, D.; Scharf, R.E.; Bettinger, D.; et al. Decreased Platelet Aggregation in Patients with Decompensated Liver Cirrhosis and TIPS Implantation. Biomedicines 2023, 11, 2057. https://doi.org/10.3390/biomedicines11072057
Nassar A, Huber JP, Stallmann D, Sharipova D, Hamad MA, Schultheiss M, Thimme R, Duerschmied D, Scharf RE, Bettinger D, et al. Decreased Platelet Aggregation in Patients with Decompensated Liver Cirrhosis and TIPS Implantation. Biomedicines. 2023; 11(7):2057. https://doi.org/10.3390/biomedicines11072057
Chicago/Turabian StyleNassar, Asala, Jan Patrick Huber, Daniela Stallmann, Diana Sharipova, Muataz Ali Hamad, Michael Schultheiss, Robert Thimme, Daniel Duerschmied, Rüdiger Eberhard Scharf, Dominik Bettinger, and et al. 2023. "Decreased Platelet Aggregation in Patients with Decompensated Liver Cirrhosis and TIPS Implantation" Biomedicines 11, no. 7: 2057. https://doi.org/10.3390/biomedicines11072057